



Introduction to Atlantoaxial Instability
Atlantoaxial instability (AAI) is a medical condition characterized by excessive movement at the junction between the atlas (C1) and axis (C2), the first two cervical vertebrae. This instability can result from bone or ligament abnormalities, compromising the stability of the upper cervical spine. Due to the complexity of this anatomical region, AAI can lead to neurological disorders when the spinal cord or adjacent nerve roots are affected.
Compared to other cervical segments, the atlantoaxial joint is particularly prone to subluxation, a partial displacement of the joint surfaces. The transverse and alar ligaments play a crucial role in maintaining the stability of this joint. When failure of these structures occurs, it can lead to significant instability, increasing the risk of neurological complications.
The clinical manifestations of AAI vary depending on the severity of the instability and the anatomic structures affected. Patients may experience symptoms such as neck pain, headache, dizziness and, in more severe cases, neurological disorders such as coordination problems, muscle weakness or sensory disturbances. These symptoms often result from compression of the spinal cord or nerve roots by unstable structures.
It is important to note that instability of the upper cervical spine can compromise the vascular structures, particularly the vertebral arteries, which pass through this region. Impaired blood flow can lead to serious complications, including stroke. In such circumstances, the use of spinal manipulation is contraindicated, as it could worsen instability and potentially cause neurovascular damage.
The diagnosis of AAI is based on imaging tests such as MRI or CT scan, allowing the bone structure and ligaments to be evaluated and any signs of instability to be identified. Treatment for AAI depends on the severity of the condition and may include conservative measures such as rest, physical therapy, and the use of neck braces to stabilize the area. In severe cases, surgery may be considered to stabilize the joint and relieve compression of the nerve structures.
Anatomy and Function of the Atlantoaxial Joint
The atlantoaxial joint (AAJ) is a crucial anatomical structure that plays a key role in the mobility and stability of the upper cervical spine. Located between the first cervical vertebra, the atlas (C1), and the second cervical vertebra, the axis (C2), this joint allows significant rotation of the head, making it vital for head and neck movements. Understanding the anatomy and function of the atlantoaxial joint is important for comprehending its contribution to cervical mobility and for diagnosing conditions like atlantoaxial instability (AAI).
Key Structures Involved in the Atlantoaxial Joint
The atlantoaxial joint is made up of three main articulations:
- One median atlantoaxial joint between the dens (odontoid process) of the axis and the anterior arch of the atlas
- Two lateral atlantoaxial joints located between the articular facets of C1 and C2.
Each of these articulations serves a unique function in enabling the rotation and stability of the joint.
- Atlas (C1): The first cervical vertebra, also known as the atlas, is a ring-like bone that supports the skull. It has no body and instead forms a circular structure that articulates with the skull’s occipital bone at the atlanto-occipital joint above and the axis below. The atlas serves as a base for skull movements, including nodding and turning.
- Axis (C2): The second cervical vertebra, or axis, has a unique projection called the dens or odontoid process. The dens extends upward through the atlas, creating a pivot that allows rotational movement. The axis serves as the structural foundation for the head’s rotation, and its articulation with the atlas is crucial for side-to-side movements of the head.
- Dens (Odontoid Process): The dens is a bony projection on the axis that extends upward into the atlas and is held in place by various ligaments. It acts as a pivot for rotation, allowing the atlas and the skull to rotate together around the axis. Damage to the dens can lead to significant instability in the cervical spine.
- Transverse Ligament: One of the most important stabilizing structures of the atlantoaxial joint is the transverse ligament, which extends across the ring of the atlas to hold the dens in place. This ligament prevents excessive anterior displacement of the atlas on the axis, which could compress the spinal cord. Without the transverse ligament’s support, the atlantoaxial joint would be prone to instability, leading to neurological issues.
- Alar Ligaments: These ligaments connect the sides of the dens to the skull and play a role in limiting excessive rotation and lateral flexion of the head and neck. Alar ligaments prevent over-rotation, which protects the spinal cord from injury during extreme movements.
- Facet Joints: The lateral atlantoaxial joints are synovial joints that allow gliding movements between the articular facets of C1 and C2. These joints facilitate smooth motion and play a role in stabilizing the joint during rotational movements.
- Anterior and Posterior Atlantoaxial Membranes: These membranes provide additional stability by connecting the atlas and axis. The posterior atlantoaxial membrane, in particular, helps to protect the spinal cord by preventing excessive motion of the vertebrae.
The Role of the Atlantoaxial Joint in Cervical Mobility
The atlantoaxial joint is essential for cervical mobility, especially in allowing rotation of the head. Nearly half of the total rotation in the cervical spine occurs at this joint, with approximately 45 degrees of rotation to either side. This enables activities like looking over the shoulder, shaking the head “no,” and turning the head from side to side. Without this joint’s contribution to mobility, the range of motion in the neck would be severely restricted.
- Rotational Movement: The atlantoaxial joint is primarily responsible for rotation of the head. The dens of the axis acts as a pivot, while the atlas rotates around it. This pivoting action enables a significant range of motion in the transverse plane, which is critical for head and neck movements. In healthy individuals, approximately 50% of cervical rotation occurs at this joint, underscoring its vital role in neck mobility.
- Stability vs. Mobility: While the atlantoaxial joint allows significant movement, it is also designed for stability, thanks to the support of the transverse ligament, alar ligaments, and surrounding muscles. These structures prevent excessive or abnormal motion that could threaten the spinal cord. However, conditions like atlantoaxial instability (AAI), caused by trauma, congenital anomalies, or degenerative changes, can lead to an excessive range of motion. This condition can compress the spinal cord and result in neurological symptoms such as pain, weakness, or even paralysis.
- Coordination with the Atlanto-occipital Joint: The atlantoaxial joint works in coordination with the atlanto-occipital joint (between the skull and the atlas), which is responsible for flexion and extension (nodding movements). Together, these two joints allow the full range of head movements, combining flexion, extension, and rotation to enable dynamic head positioning.
- Implications in Pathology: Atlantoaxial instability (AAI) is a condition where the joint becomes excessively mobile, often due to trauma, congenital abnormalities, or conditions like rheumatoid arthritis. AAI can lead to pain, limited range of motion, and, in severe cases, compression of the spinal cord. Diagnosis and treatment of AAI typically involve imaging studies like X-rays, MRIs, or CT scans, followed by immobilization or surgical stabilization if needed.
Primary Causes and Risk Factors for Atlantoaxial Instability (AAI)
Atlantoaxial instability (AAI) refers to excessive or abnormal movement between the first cervical vertebra (atlas, C1) and the second cervical vertebra (axis, C2). This instability can lead to significant neurological symptoms due to spinal cord compression, ranging from mild sensory disturbances to severe conditions such as cervical myelopathy or paralysis. AAI can arise from several causes, including congenital abnormalities, trauma, degenerative conditions, and genetic disorders. Understanding the primary causes and risk factors for AAI is essential for accurate diagnosis and timely intervention.

Congenital Anomalies and Developmental Issues
Congenital anomalies and developmental issues are significant causes of AAI, especially in children and young adults. These conditions can result in abnormal bone formation or ligament laxity, both of which can contribute to instability between the atlas and axis.
- Down Syndrome: One of the most well-known genetic conditions associated with AAI is Down syndrome. Up to 20% of individuals with Down syndrome may develop AAI due to laxity in the transverse ligament, which is responsible for stabilizing the atlas against the axis. Screening for AAI is crucial in this population, as undiagnosed instability can lead to sudden spinal cord compression, particularly during activities that stress the neck.
- Os Odontoideum: This is a condition in which the odontoid process, the bony projection from the axis that provides a pivot point for the atlas, is either underdeveloped or improperly fused. This malformation leads to an unstable connection between C1 and C2, increasing the risk of AAI.
- Klippel-Feil Syndrome: This congenital condition, characterized by the fusion of two or more cervical vertebrae, can also predispose individuals to AAI. Although the fusion occurs in other parts of the cervical spine, the altered biomechanics can place excessive stress on the C1-C2 junction, leading to instability.
These congenital and developmental abnormalities highlight the importance of early screening and monitoring in populations at risk for AAI.
Traumatic Events Leading to Instability
Trauma is another common cause of AAI, particularly in cases of high-impact injuries to the neck or cervical spine. Traumatic AAI can occur due to a variety of injuries:
- Motor Vehicle Accidents: Whiplash injuries from car accidents are a leading cause of traumatic AAI. The sudden, forceful movement of the head and neck can damage the ligaments that stabilize the C1-C2 junction, leading to instability. Even if there is no immediate fracture or dislocation, ligamentous damage can cause long-term instability.
- Sports Injuries: Contact sports such as football, wrestling, and gymnastics place athletes at risk for cervical spine injuries. A sudden blow to the head or a fall onto the neck can damage the ligaments, vertebrae, or intervertebral discs, resulting in AAI.
- Falls: In older adults, falls are a leading cause of cervical spine injuries, including AAI. Osteoporosis, common in the elderly, increases the likelihood of fractures and ligament damage, making the neck more vulnerable to instability after a fall.
In cases of trauma, early diagnosis and intervention are critical to prevent the progression of AAI and the development of spinal cord compression.
Rheumatologic and Degenerative Conditions
Rheumatologic and degenerative conditions are another significant category of risk factors for AAI. These conditions cause progressive damage to the joints and ligaments in the cervical spine, leading to instability over time.
- Rheumatoid Arthritis (RA): One of the most common rheumatologic conditions associated with AAI is rheumatoid arthritis. RA is an autoimmune disease that causes chronic inflammation of the joints, including those in the cervical spine. Over time, this inflammation can erode the cartilage and ligaments that support the atlantoaxial joint, leading to instability. RA-related AAI is most common in the later stages of the disease and can lead to severe neurological complications if left untreated.
- Degenerative Disc Disease: Degenerative changes in the intervertebral discs, common in older adults, can contribute to instability in the cervical spine. As the discs degenerate, the support they provide to the vertebrae diminishes, leading to increased movement between C1 and C2. This can eventually result in AAI, especially in individuals with pre-existing ligamentous laxity.
- Osteoarthritis: Osteoarthritis, another degenerative condition, can also contribute to AAI by causing joint space narrowing and ligament weakening. Over time, these changes can destabilize the atlantoaxial joint, particularly in elderly patients.
Genetic Conditions and Syndromes Predisposing to AAI
Several genetic conditions and syndromes predispose individuals to AAI due to their effects on bone and ligament development:
- Ehlers-Danlos Syndrome (EDS): This genetic connective tissue disorder is characterized by hypermobility and ligamentous laxity, which significantly increases the risk of AAI. Individuals with EDS may develop cervical spine instability due to the weakened connective tissue structures that fail to stabilize the atlantoaxial joint.
- Marfan Syndrome: Marfan syndrome, another genetic disorder affecting connective tissue, can lead to abnormal joint laxity, including in the cervical spine. Individuals with this condition may have a higher risk of AAI due to their predisposition to ligamentous weakness and abnormal joint movement.
- Achondroplasia: As a form of dwarfism that affects bone growth, achondroplasia can also increase the risk of AAI. The altered shape and structure of the cervical vertebrae can lead to instability at the C1-C2 junction.
These genetic conditions necessitate close monitoring for signs of AAI, as the risk of spinal cord compression and related complications is high.


Clinical Symptoms of Atlantoaxial Instability
The symptoms of Atlantoaxial instability (AAI) typically manifest in two broad categories: neurological and musculoskeletal. Additionally, cervical myelopathy is a severe complication that may arise if AAI is left untreated or becomes progressively worse.
Neurological Manifestations: From Numbness to Paralysis
The neurological symptoms of AAI arise primarily due to compression of the spinal cord or nerve roots at the cervical level. These symptoms can range in severity, from mild sensory disturbances to more debilitating neurological deficits. Patients often experience:
- Numbness and Tingling: The most common neurological manifestations include sensory disturbances like numbness, tingling, or “pins and needles” sensations in the extremities, particularly in the arms and hands. These symptoms result from irritation or compression of the cervical spinal cord or nerve roots.
- Weakness: As the condition progresses, patients may report muscle weakness, especially in the arms. In severe cases, this weakness can affect the legs, leading to difficulties with balance and gait.
- Loss of Coordination: AAI can interfere with fine motor skills, such as buttoning a shirt or writing, due to impaired hand coordination. Some individuals may also notice clumsiness or an increased likelihood of dropping objects.
- Paralysis: In severe cases, if left untreated, AAI can lead to partial or complete paralysis, often referred to as quadriparesis or quadriplegia. This is caused by significant compression of the spinal cord and may become life-threatening if the respiratory muscles are affected.
- Bladder and Bowel Dysfunction: Neurological involvement at the cervical level can also impair autonomic functions, leading to difficulties with bladder and bowel control.
These neurological symptoms often start subtly and may progress over time. Early identification and treatment are crucial to prevent permanent damage.
Musculoskeletal Symptoms and Neck Pain
The musculoskeletal symptoms of AAI are predominantly linked to the abnormal movement between the atlas and axis, which creates instability in the cervical spine. This can cause significant discomfort and affect day-to-day activities. Key musculoskeletal signs include:
- Chronic Neck Pain: Patients frequently report persistent or intermittent neck pain. The pain may worsen with neck movement, particularly during activities that involve looking up, turning the head, or prolonged periods of holding the head in one position.
- Headaches: Neck pain may radiate upwards, causing headaches, especially at the base of the skull. These headaches can be persistent and debilitating, often described as tension headaches or occipital neuralgia.
- Limited Range of Motion: Individuals with AAI often experience stiffness in their neck and a limited ability to move their head in certain directions. This limitation can affect daily activities such as driving or looking around.
- Muscle Spasms: The instability between the C1 and C2 vertebrae can lead to muscle tension and spasms in the surrounding muscles, further contributing to discomfort and limited movement.
While musculoskeletal symptoms may initially be mild, they can progressively worsen, especially if the underlying cause of AAI remains unaddressed.
Cervical Myelopathy: A Serious Complication of AAI
Cervical myelopathy is one of the most severe complications of atlantoaxial instability. It occurs when there is significant compression of the spinal cord, resulting in neurological dysfunction. The following are some of the hallmark features of cervical myelopathy:
- Gait Instability: Patients with cervical myelopathy may present with difficulty walking, characterized by an unsteady gait. This instability often worsens over time and may eventually lead to falls.
- Severe Muscle Weakness: As the spinal cord becomes more compressed, the motor deficits become more pronounced, resulting in profound weakness in the arms and legs. This can lead to difficulty performing basic tasks, such as dressing or feeding oneself.
- Hyperreflexia and Spasticity: In some cases, cervical myelopathy can cause overactive reflexes and increased muscle tone, leading to spasticity and abnormal movements.
- Breathing Difficulties: If the spinal cord compression affects the brainstem or high cervical levels, it can interfere with respiratory function, potentially becoming life-threatening.
Cervical myelopathy requires prompt medical intervention, often including surgical decompression, to prevent irreversible damage to the spinal cord. Without treatment, patients may experience permanent neurological deficits, including paralysis or even death.
Spencer’s rule
The atlantoaxial segment is made up of the atlas (C1) and the axis (C2) and forms a complex transitional structure connecting the occiput and the cervical spine.
The functional result of this joint is twofold: providing support for the occiput and providing the greatest possible range of motion and flexibility while maintaining stability.
Instability in this joint is usually congenital, but in adults it can result from an acute traumatic event or degenerative disease.
Atlantoaxial instability can be classified into three generalized categories: inflammatory, congenital, and traumatic.
“Spence’s Rule” classically determines the stability of C1 fractures by measuring the lateral spillover of C1 lateral masses onto C2 when examining an AP radiograph. If the sum of the two lateral masses of C1 over C2 is greater than 7 mm, the fracture is considered unstable. This measurement tool is also typically used to evaluate computed tomography (CT scan) images.
Treatment for atlantoaxial instability varies widely, and intervention is generally tailored to patients on an individualized basis. Asymptomatic patients can be monitored over time with dynamic images and MRI to track disease progression.
The prognosis in symptomatic patients treated early is good. Posterior spinal fusion can help restore function and reverse symptoms such as pain and myelopathy.
Diagnostic Approaches for Atlantoaxial Instability
Diagnosing AAI is critical to prevent potentially severe complications such as cervical myelopathy, paralysis, or even death. This article outlines the key clinical signs, the role of physical examination, and advanced imaging techniques used in the diagnostic process. Additionally, it discusses how to differentiate AAI from other cervical spine disorders to ensure accurate diagnosis and treatment.
Key Clinical Signs and Physical Examination
The initial diagnostic step for AAI involves a detailed patient history and thorough physical examination. Key clinical signs to watch for include:
- Neck Pain and Stiffness: Patients often report chronic neck pain that is exacerbated by movement, especially in activities requiring head rotation or prolonged stationary positions. Stiffness and limited range of motion in the neck are also common.
- Headaches: Occipital headaches (those at the base of the skull) can be a frequent symptom due to irritation of the upper cervical nerves. These headaches are often exacerbated by neck movements.
- Neurological Symptoms: Numbness, tingling, and weakness in the arms or hands may indicate nerve root compression. Severe cases may present with weakness in the legs, difficulty walking, or even signs of partial paralysis.
- Gait Instability: Patients may exhibit difficulty maintaining balance or walking properly, often described as a “wobbly” or unsteady gait. This is particularly concerning as it suggests spinal cord involvement, which could signal the development of cervical myelopathy.
During the physical examination, physicians may perform specific tests to evaluate the range of motion, muscle strength, and sensory function in the patient’s limbs:
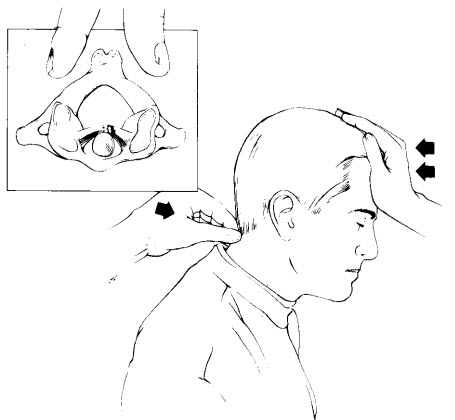
- Transverse Ligament Stress Test: This test evaluates the integrity of the transverse ligament, which stabilizes the atlas (C1) relative to the axis (C2). The patient lies in a supine position, and the examiner gently applies anterior pressure to the posterior arch of the atlas while stabilizing the occiput. If this maneuver produces neurological symptoms such as dizziness, tingling, or a feeling of instability, it suggests that the transverse ligament may be compromised, leading to atlantoaxial instability.
- Alar Ligament Stress Test: The alar ligaments are critical for stabilizing the skull on the cervical spine and limiting rotation and lateral bending. To perform this test, the examiner stabilizes the patient’s axis (C2) and gently rotates or side-bends the head. Limited motion or the reproduction of symptoms like dizziness, pain, or altered sensation can indicate damage to the alar ligaments, contributing to instability between the atlas and axis.
- Neck Flexion and Extension: The patient may be asked to move their neck forward and backward. In cases of AAI, this movement can elicit pain or neurological symptoms, such as numbness or a tingling sensation, indicating instability between the C1 and C2 vertebrae.
- Lhermitte’s Sign: This test, where the patient bends their neck forward, may produce an electric shock-like sensation down the spine or into the limbs. This finding strongly suggests spinal cord involvement, a potential complication of AAI.

If physical examination and clinical history indicate AAI, imaging studies are essential to confirm the diagnosis and assess the severity of instability.
Advanced Imaging: X-rays, CT, and MRI
Imaging is the cornerstone of diagnosing AAI. The most commonly used modalities include X-rays, computed tomography (CT), and magnetic resonance imaging (MRI). Each technique has its advantages and role in diagnosis:
- X-rays: Standard cervical spine X-rays are often the first-line imaging test in suspected AAI cases. Flexion and extension views are particularly valuable, as they allow clinicians to see how the C1 and C2 vertebrae move relative to one another during neck movement. If the distance between these vertebrae is abnormal or if there is excessive movement, it confirms instability. These dynamic X-rays help detect instability that may not be visible on neutral positioning alone.
- CT Scans: CT scans offer high-resolution images of bone structures and are especially helpful when there is suspicion of fractures, degenerative changes, or congenital anomalies contributing to AAI. This imaging modality provides detailed cross-sectional views of the cervical vertebrae and can identify structural defects that may not be apparent on X-rays.
- MRI: MRI is the gold standard for assessing the soft tissues and neural structures, including the spinal cord, ligaments, and intervertebral discs. It is crucial in determining whether AAI has caused spinal cord compression, a serious complication that could lead to myelopathy. MRI is also helpful for detecting inflammation or other soft tissue abnormalities that may contribute to the patient’s symptoms.
Each imaging modality complements the other, with X-rays helping to identify mechanical instability, CT scans providing detailed bone views, and MRI highlighting the effects of AAI on the spinal cord and surrounding soft tissues.
Differentiating AAI from Other Cervical Spine Disorders
While AAI has distinct characteristics, it can sometimes be confused with other cervical spine disorders such as degenerative disc disease, cervical stenosis, or cervical spondylosis. Proper diagnosis is essential, as the treatment for AAI differs significantly from these other conditions.
- Level of Instability: AAI specifically involves instability at the junction between C1 and C2, whereas other cervical spine disorders typically affect the lower cervical vertebrae (C3-C7). Recognizing this anatomical distinction is crucial for diagnosis.
- Imaging Features: X-ray and MRI findings are instrumental in distinguishing AAI from other conditions. For instance, cervical spondylosis usually presents with osteophyte formation and disc space narrowing, features that are absent in AAI. AAI, on the other hand, shows abnormal movement between C1 and C2, which is not seen in other disorders.
- Pattern of Neurological Involvement: While both AAI and cervical stenosis can cause neurological symptoms, AAI often results in more pronounced upper extremity weakness and sensory changes due to the higher location of instability in the cervical spine. Conversely, cervical stenosis and degenerative disc disease may cause symptoms lower down the spinal column, affecting both upper and lower extremities more equally.
Accurate differentiation ensures that AAI is not misdiagnosed as a less severe condition, allowing for timely intervention.
Potential Complications of Untreated AAI
Atlantoaxial Instability (AAI), if left untreated, can lead to serious and potentially life-threatening complications. These complications can vary in severity depending on the extent of the instability, the underlying causes, and how long the condition is left unmanaged. The following are the primary complications associated with untreated AAI:
Neurological Impairment and Progression
One of the most concerning complications of untreated AAI is neurological impairment. The atlantoaxial joint plays a crucial role in protecting the spinal cord, and instability in this area can lead to compression or irritation of the spinal cord. Over time, this pressure on the spinal cord can lead to a range of neurological symptoms. These symptoms often begin with mild issues like numbness or tingling in the extremities, but if left unchecked, they can progress to more severe neurological deficits such as weakness in the limbs, loss of motor control, and even paralysis.
In severe cases, AAI can lead to cervical myelopathy, a condition where the spinal cord becomes compressed. This can cause difficulty walking, loss of fine motor skills, and problems with bladder or bowel control. Early diagnosis and intervention are critical to preventing the progression of neurological damage, which may become irreversible if not treated in time.
Chronic Cervical Pain and Disability
Untreated AAI can also result in chronic neck pain, which significantly impacts a person’s quality of life. The instability of the atlantoaxial joint often leads to increased strain on the surrounding muscles and ligaments, causing muscle spasms and persistent discomfort. Over time, this can lead to chronic pain, which may be difficult to manage without medical intervention. Additionally, the constant tension on the neck can contribute to headaches, particularly cervicogenic headaches, which stem from issues in the cervical spine.
The chronic pain associated with untreated AAI can also lead to long-term disability. As pain increases and mobility decreases, patients may find it difficult to perform daily activities or maintain their usual level of physical activity. This can lead to muscle atrophy, reduced range of motion, and further complications, making the condition even more challenging to treat in the later stages.
Postural and Gait Abnormalities Stemming from AAI
Atlantoaxial instability can also affect a patient’s posture and gait. As the body attempts to compensate for the instability in the upper cervical spine, postural adjustments often occur. These compensations may manifest as a forward head posture, a hunched upper back, or an uneven gait. Over time, these postural abnormalities can lead to secondary musculoskeletal issues, such as pain in the lower back, hips, or legs.
Additionally, gait disturbances are common in individuals with untreated AAI. The instability at the top of the spine can impact balance and coordination, leading to an unsteady gait or an increased risk of falls. Patients may also experience difficulty with activities that require fine motor coordination or balance, such as climbing stairs or bending down.
Osteopathic Interventions for Atlantoaxial Instability
The primary goal of osteopathic treatment for AAI is to restore balance to the musculoskeletal and neurological systems while minimizing stress on the affected joint. Osteopaths utilize a variety of techniques, ranging from manual therapy to myofascial release, to address the symptoms of AAI. However, given the delicate nature of the cervical spine, certain precautions must be taken, particularly with manual manipulation.
Manual Techniques and Their Role in AAI Management
Manual techniques, which involve hands-on manipulation and assessment of the body’s structure, are a cornerstone of osteopathic care. In the case of AAI, manual techniques can be helpful in addressing compensatory tension patterns in the muscles and ligaments surrounding the atlantoaxial joint. Osteopaths may use soft tissue techniques to alleviate muscle spasms and reduce inflammation, which can improve overall neck mobility and decrease pain.
However, it’s crucial to emphasize that high-velocity cervical manipulation is contraindicated for patients with AAI. The instability in the atlantoaxial joint makes the upper cervical spine vulnerable to injury. Forceful manipulation could worsen the instability and, in severe cases, lead to spinal cord compression or neurological damage. Instead, osteopaths focus on gentle techniques that do not involve thrusts or sudden movements, ensuring the safety of the patient while still providing relief from symptoms.
For patients with AAI, osteopaths may instead employ low-force techniques, such as gentle mobilizations, to improve range of motion and support joint stability. These interventions are designed to work with the body’s natural healing mechanisms while avoiding any risk of exacerbating the condition.
Myofascial Release and Cranial Osteopathy
Myofascial release is another key technique in osteopathic care for AAI. The fascial system, which connects all parts of the body, can become tense or restricted in response to instability in the cervical spine. Osteopaths use myofascial release techniques to gently stretch and manipulate the fascia, relieving tension and improving circulation. This can help reduce pain and improve mobility, particularly in the muscles surrounding the atlantoaxial joint.
Cranial osteopathy, a more subtle form of manual therapy, focuses on the movement of the cranial bones and the flow of cerebrospinal fluid. For patients with AAI, cranial osteopathy can help address any imbalances in the cranium and upper cervical spine, promoting better overall function. This technique is especially useful for patients with neurological symptoms, as it aims to support the body’s inherent ability to self-regulate and heal.
Both myofascial release and cranial osteopathy are low-risk techniques that can provide relief without putting stress on the unstable atlantoaxial joint, making them ideal options for patients with AAI.
Addressing Whole-Body Compensation Patterns
When dealing with AAI, the body often compensates for the instability by creating tension in other areas, particularly in the thoracic and lumbar spine. These compensatory mechanisms can lead to pain and dysfunction in regions far from the site of the instability. Osteopathic treatment focuses not just on the cervical spine, but on the entire body, aiming to restore balance and reduce compensatory strain.
For example, a patient with AAI may develop tightness in the muscles of the upper back or even the lower back as the body tries to maintain stability. Osteopaths address these areas through gentle stretching, mobilization, and soft tissue techniques, relieving secondary pain and improving overall function. By treating the whole body, osteopaths can help patients manage their symptoms more effectively and reduce the likelihood of developing further complications.
Warning: Manual cervical manipulation, particularly high-velocity techniques, is extremely dangerous for individuals with Atlantoaxial Instability. Such manipulation can worsen the instability and cause serious damage, including spinal cord compression. Patients with AAI should only receive low-force, gentle osteopathic techniques that prioritize safety and do not involve thrusts or sudden movements. Always consult a healthcare professional familiar with AAI before undergoing any form of cervical manipulation.
Osteopathic interventions, when applied with care, can be a valuable part of managing AAI. By focusing on gentle manual techniques, myofascial release, and addressing whole-body compensation, osteopaths can provide symptom relief without endangering the patient’s health.
Non-Surgical Management Strategies
For individuals diagnosed with Atlantoaxial Instability (AAI), non-surgical management strategies play a crucial role in reducing symptoms, stabilizing the joint, and improving overall quality of life. These approaches are often preferred, especially in cases where the condition is mild or when surgery poses significant risks. The goal of non-surgical management is to provide stability to the cervical spine, alleviate pain, and support the body’s natural healing mechanisms without invasive intervention.
Use of Cervical Braces and Supports
One of the most common and effective non-surgical treatments for AAI is the use of cervical braces or collars. These devices help immobilize the cervical spine, reducing movement and allowing the affected area to stabilize. By limiting motion, cervical braces prevent further damage and give the joint time to heal. Patients often wear these supports for extended periods, particularly during activities that involve neck movement or strain.
There are various types of cervical braces, ranging from soft collars that provide minimal support to rigid braces that offer maximum immobilization. The choice of brace depends on the severity of the instability and the patient’s specific needs. Rigid braces are typically recommended for patients with more pronounced instability, as they provide greater protection against sudden or excessive movements.
Warning: It is crucial to consult a healthcare professional before using any cervical braces or supports. Improper use of these devices can lead to muscle atrophy, reduced range of motion, or even worsen the instability if not fitted correctly. A professional can assess your condition and prescribe the most suitable brace, ensuring that it provides the necessary support without causing unintended complications. This warning is essential because incorrect brace use can exacerbate the condition, leading to further complications, such as increased instability or muscle degeneration.
While cervical braces offer significant benefits, their use must be paired with a structured rehabilitation program to prevent muscle weakness and ensure long-term recovery.
Pain Control and Physical Rehabilitation
Managing pain is a top priority for patients with AAI, as chronic discomfort can significantly impact daily life. A combination of pain-relief medications, such as non-steroidal anti-inflammatory drugs (NSAIDs) or muscle relaxants, may be prescribed to reduce inflammation and manage acute pain. However, it’s important to consult a medical professional before using any medications, as incorrect dosages or prolonged use can lead to adverse side effects or dependency risks.
Warning: The use of medications without professional guidance can lead to complications such as gastrointestinal issues, addiction, or insufficient pain management. Consulting a healthcare provider is critical to ensure the correct medication, dosage, and duration are chosen to prevent these risks.
Physical rehabilitation, particularly through gentle exercises and stretches, is another cornerstone of non-surgical management. A physical therapist or osteopath may design a program tailored to the patient’s specific condition, focusing on improving range of motion, increasing strength, and addressing any compensatory muscle patterns that have developed due to the instability. Exercises often target the muscles surrounding the cervical spine, with an emphasis on enhancing neck stability and posture. Additionally, patients are often encouraged to engage in gentle aerobic activities like walking or swimming, which can improve overall fitness without placing undue strain on the neck.
The key to successful rehabilitation is gradual progression. Patients with AAI should avoid exercises or movements that put excessive stress on the cervical spine, as this could exacerbate the condition. Instead, the focus is on slow, controlled movements that promote healing and improve function over time.
Warning: Always consult a healthcare professional before using any cervical braces, supports, or medications. Improper use or unsupervised treatment can lead to worsening symptoms or complications. This warning is important to avoid the risk of further harm, such as increased instability or adverse reactions to treatments.
Surgical Solutions for Atlantoaxial Instability
In cases of severe Atlantoaxial Instability (AAI), where non-surgical management has proven insufficient or the risk of neurological damage is significant, surgical intervention may be necessary. The goal of surgery is to stabilize the atlantoaxial joint and prevent further damage to the spinal cord and surrounding structures. Surgical solutions are typically recommended when there is a high risk of spinal cord compression, progressive neurological deficits, or significant instability that cannot be managed conservatively.
Indications for Surgical Intervention
Surgical intervention for AAI is generally considered when conservative treatments, such as cervical bracing and rehabilitation, fail to alleviate symptoms or halt the progression of the condition. Some common indications for surgery include:
- Neurological deterioration: If a patient experiences worsening neurological symptoms, such as weakness, numbness, or loss of motor control, surgery may be required to prevent permanent damage.
- Severe instability: When the atlantoaxial joint is too unstable to be managed with external supports or braces, surgery is often necessary to provide internal stabilization.
- Risk of spinal cord compression: In cases where the instability has led to significant narrowing of the spinal canal, surgery is performed to decompress the spinal cord and prevent further injury.
- Congenital abnormalities or trauma: Patients with congenital conditions, such as Down syndrome, or those who have experienced trauma to the cervical spine may require surgical intervention to correct the instability.
Surgical decisions are typically made on a case-by-case basis, with the patient’s overall health, the severity of the condition, and the risk of complications being carefully considered by the surgeon.
Common Surgical Procedures: Fusion and Stabilization Techniques
Surgical stabilization of the atlantoaxial joint typically involves fusion procedures aimed at limiting motion between the C1 and C2 vertebrae. The most common surgical techniques used to treat AAI include:
- Posterior atlantoaxial fusion: This procedure involves fusing the C1 and C2 vertebrae from the back of the neck using screws, rods, or bone grafts. The goal is to create a stable connection between these two vertebrae, preventing further movement and reducing the risk of spinal cord compression. This is one of the most widely used techniques for managing AAI and has a high success rate in stabilizing the joint.
- Transarticular screw fixation: This method involves the placement of screws across the C1-C2 joint to achieve stabilization. It is often combined with posterior fusion to enhance stability and ensure that the bones fuse properly over time. This technique is highly effective in cases where severe instability is present.
- Occipitocervical fusion: In cases where instability extends beyond the atlantoaxial joint, occipitocervical fusion may be performed to stabilize the entire upper cervical spine. This procedure fuses the occiput (base of the skull) to the upper cervical vertebrae (C1-C2) using plates, screws, or rods. It is usually reserved for patients with complex or multi-level instability.
While these procedures are highly effective in stabilizing the cervical spine, they do limit motion between the affected vertebrae, which can result in a permanent reduction in neck mobility. However, the primary goal of surgery is to prevent neurological damage and improve quality of life, making the trade-off of reduced motion necessary in many cases.
Post-Surgical Rehabilitation and Recovery
After surgery, a comprehensive rehabilitation program is essential to ensure a successful recovery. The primary goals of post-surgical rehabilitation are to promote healing, restore strength and mobility, and prevent complications. The rehabilitation process is typically divided into two phases: early recovery and long-term rehabilitation.
Early Rehabilitation Protocols and Exercises
In the early stages of recovery, the focus is on protecting the surgical site and allowing the bones to fuse properly. Patients are often required to wear a cervical brace or collar for several weeks to support the neck and prevent excessive movement. During this time, physical activity is limited to gentle movements that do not strain the neck.
Physical therapists may introduce light stretching and range-of-motion exercises to prevent stiffness in the shoulders and upper back. These exercises are crucial in maintaining flexibility and preventing the development of compensatory patterns that could lead to pain in other areas of the body.
Long-Term Physical Therapy Goals
As the patient progresses in their recovery, the focus shifts to rebuilding strength in the neck and surrounding muscles. Physical therapy typically includes strengthening exercises that target the cervical and upper thoracic muscles, as well as exercises aimed at improving posture and body mechanics.
Patients are encouraged to gradually increase their physical activity, incorporating low-impact exercises such as walking or swimming. These activities help improve overall fitness without placing undue strain on the neck.
Monitoring and Preventing Recurrence After Surgery
Post-surgical follow-up is critical to ensure that the atlantoaxial joint has stabilized and that the bones have fused properly. Regular imaging studies, such as X-rays or CT scans, are often performed to monitor the progress of bone fusion and detect any signs of hardware failure or complications.
Patients are also educated on how to avoid movements or activities that could put excessive stress on the cervical spine. Preventive measures, such as maintaining good posture, avoiding heavy lifting, and engaging in regular physical therapy, can help prevent recurrence and ensure long-term success.
Prognosis and Long-Term Outlook for AAI Patients
The prognosis for patients with Atlantoaxial Instability (AAI) largely depends on the severity of the condition, the timing of diagnosis, and the effectiveness of the treatment. While some individuals can manage AAI with non-surgical interventions, others may require surgical stabilization to prevent neurological complications and ensure long-term stability. Understanding the factors that influence recovery and the potential long-term impacts of the condition is essential for both patients and healthcare providers.
Factors Affecting Recovery and Outcome
Several factors play a role in determining the prognosis for individuals with AAI:
- Severity of Instability: Patients with mild to moderate instability often have better outcomes, especially when the condition is identified early and managed effectively. Severe instability, particularly cases that involve spinal cord compression or progressive neurological symptoms, may require more aggressive treatment, including surgery.
- Timely Intervention: Early diagnosis and intervention are critical in preventing the progression of AAI. When left untreated, the instability can lead to irreversible neurological damage, including chronic pain, motor deficits, or even paralysis. The earlier the condition is diagnosed and treated, the better the prognosis for recovery and long-term function.
- Patient’s Overall Health: The overall health and physical condition of the patient also play a significant role in recovery. Patients who maintain a healthy lifestyle, including good posture and physical activity, are more likely to experience positive outcomes. On the other hand, individuals with underlying conditions such as rheumatoid arthritis, trauma, or congenital disorders like Down syndrome may face additional challenges in managing the condition.
- Adherence to Treatment Plans: The success of treatment, whether surgical or non-surgical, depends heavily on the patient’s adherence to the prescribed rehabilitation and follow-up care. Those who commit to a structured physical therapy program, follow medical advice, and take preventive measures to avoid exacerbating the condition typically have a more favorable long-term outlook.
- Surgical Success: For patients who undergo surgical treatment, the success of the surgery itself is a critical factor in prognosis. Most fusion and stabilization procedures for AAI are successful in providing long-term stability, but complications such as hardware failure, infection, or incomplete fusion can affect recovery. Regular monitoring and post-surgical care are essential to address any issues that arise.
[Long-Term Impact on Mobility and Daily Life]
While surgical and non-surgical interventions can stabilize the atlantoaxial joint, patients often experience some degree of lasting impact on their mobility and daily activities. The extent of these limitations varies depending on the severity of the instability and the type of treatment received.
- Reduced Neck Mobility: Patients who undergo fusion procedures typically experience a reduction in neck mobility, particularly between the C1 and C2 vertebrae. This loss of motion may affect activities such as turning the head while driving or looking over the shoulder. However, most patients adapt to these limitations over time and are able to resume a relatively normal lifestyle.
- Chronic Pain: Some individuals may continue to experience chronic neck pain or discomfort even after treatment, especially if the instability caused significant muscle tension or nerve irritation. Ongoing physical therapy and pain management strategies may be required to address these lingering symptoms.
- Neurological Function: In cases where AAI caused neurological damage prior to treatment, patients may experience long-term issues such as weakness, numbness, or impaired motor function. While surgery can prevent further damage, it may not reverse existing neurological deficits. Early intervention is key to preserving neurological function and preventing long-term disability.
- Impact on Quality of Life: Overall, the majority of patients with AAI who receive appropriate treatment can expect to return to normal activities, though some adjustments may be necessary to accommodate reduced mobility or lingering pain. Maintaining good posture, engaging in regular exercise, and following preventive measures are essential to minimizing the long-term impact of the condition.
Monitoring and Follow-up Care
Long-term prognosis for AAI also depends on regular monitoring and follow-up care. For surgical patients, imaging studies such as X-rays or CT scans are used to ensure that the bones are fusing properly and that the hardware remains stable. Non-surgical patients benefit from ongoing physical therapy and periodic assessments to ensure that the condition is not worsening.
Patients are also educated on lifestyle modifications that can help protect the cervical spine and prevent the recurrence of instability. This includes maintaining proper posture, avoiding high-impact activities, and engaging in exercises that strengthen the neck and upper back muscles.
Psychological and Emotional Considerations
Living with AAI can be emotionally challenging, particularly for individuals dealing with chronic pain, reduced mobility, or the uncertainty of surgical outcomes. It’s important for patients to receive emotional support throughout their treatment journey. Counseling, support groups, or even mindfulness practices can help patients cope with the mental strain that often accompanies physical limitations.
Prevention and Lifestyle Modifications
Preventing Atlantoaxial Instability (AAI) or minimizing its progression requires a proactive approach that incorporates both preventive strategies and lifestyle modifications. While some cases of AAI may be congenital or related to trauma or degenerative conditions, there are still several measures that can be taken to support cervical spine health and reduce the risk of further complications. Implementing these changes can be particularly beneficial for high-risk populations, such as those with certain genetic predispositions or pre-existing cervical conditions.
Prevention Strategies in High-Risk Populations
Individuals who are at higher risk for developing AAI, such as those with Down syndrome, rheumatoid arthritis, or a history of cervical trauma, should take specific precautions to protect their cervical spine. Early detection and intervention are critical for preventing the progression of the condition. Regular screening and diagnostic imaging are essential for identifying AAI in its early stages, particularly in children or adults with known risk factors.
- Screening and Monitoring: In high-risk populations, such as individuals with Down syndrome or those with inflammatory diseases, regular cervical spine evaluations are recommended. Pediatric patients with Down syndrome are typically screened for AAI between the ages of 3 to 5, as early detection can help prevent serious complications.
- Physical Activity Modifications: While staying active is important for maintaining overall health, high-risk individuals should avoid activities that involve excessive impact or stress on the cervical spine. This includes contact sports such as football or rugby, which can exacerbate instability or lead to trauma in the upper cervical region.
- Early Intervention for Trauma: Any trauma to the cervical spine, such as whiplash from a car accident or a sports injury, should be promptly evaluated by a healthcare professional. Delaying treatment or ignoring symptoms such as neck pain or stiffness can allow AAI to progress unnoticed, leading to more severe complications down the road.
Maintaining Cervical Spine Health Through Lifestyle Adjustments
For both high-risk individuals and those looking to prevent cervical spine issues, incorporating certain lifestyle modifications can help support long-term cervical spine health. These changes focus on reducing strain on the neck, improving posture, and strengthening the muscles that support the cervical region.
- Ergonomic Adjustments: One of the most effective ways to prevent strain on the cervical spine is by optimizing ergonomic setups at home and in the workplace. Proper desk and chair alignment, ensuring that the computer screen is at eye level, and using a supportive chair can help maintain neutral spine alignment and prevent forward head posture, which places stress on the upper cervical region. The use of ergonomic pillows during sleep can also help keep the neck in a neutral position and reduce strain overnight.
- Postural Awareness: Poor posture, particularly forward head posture or slouching, is a common contributor to cervical instability and pain. Individuals should be mindful of their posture throughout the day, especially during sedentary activities such as working at a computer or watching television. Exercises that promote postural awareness, such as yoga or Pilates, can be helpful in correcting poor posture and building strength in the muscles that support the cervical spine.
- Strengthening Exercises: Strengthening the muscles surrounding the cervical spine, particularly the deep neck flexors, can provide added stability to the atlantoaxial joint. Physical therapists or osteopaths often prescribe exercises that target these muscles, as well as those in the upper back and shoulders, to support proper neck alignment. Simple exercises such as chin tucks, shoulder blade squeezes, and neck stretches can be incorporated into a daily routine to prevent stiffness and promote strength.
- Weight Management: Maintaining a healthy weight is also important for reducing strain on the cervical spine. Excess weight, especially in the upper body, can place additional stress on the neck and exacerbate symptoms of AAI. Engaging in regular physical activity and following a balanced diet can help prevent weight gain and support overall spinal health.
- Stress Management and Relaxation Techniques: Stress can contribute to muscle tension, particularly in the neck and shoulders, which may worsen symptoms of AAI. Incorporating relaxation techniques such as deep breathing, meditation, or massage therapy can help alleviate tension and promote better posture.
Role of Education and Self-Care
Educating patients about the importance of proper neck care and posture is a key component of preventing AAI and managing its progression. Patients should be aware of the risks associated with cervical instability and be proactive in seeking medical evaluation if they experience symptoms such as neck pain, stiffness, or neurological changes. Additionally, maintaining a commitment to self-care, including regular physical activity and stress management, is essential for long-term spine health.
It’s important to note that while these lifestyle modifications can reduce the risk of exacerbating AAI or developing cervical spine issues, they are not a substitute for professional medical care. Individuals with AAI or those at high risk should work closely with healthcare providers to develop a personalized prevention and management plan.
Warning: Always consult a healthcare professional before starting any new exercise regimen, ergonomic changes, or lifestyle modifications, especially if you have a pre-existing condition such as AAI. Improper execution of exercises or activities may worsen symptoms or lead to additional complications.
Frequently Asked Questions (FAQ)
Managing Atlantoaxial Instability (AAI) can be a complex and overwhelming process, and many patients and their families have concerns about the condition, its treatment, and long-term outcomes. This FAQ section addresses some of the most common questions related to AAI, providing essential information to help patients make informed decisions about their care.
What is Atlantoaxial Instability (AAI)?
Atlantoaxial Instability (AAI) is a condition in which there is excessive movement or instability between the first (C1) and second (C2) cervical vertebrae. This instability can cause pressure on the spinal cord, leading to a variety of symptoms such as neck pain, headaches, and in severe cases, neurological deficits like numbness, weakness, or even paralysis. The condition can be congenital, related to trauma, or caused by degenerative diseases like rheumatoid arthritis.
How is AAI diagnosed?
AAI is typically diagnosed through a combination of clinical evaluation and imaging studies. After taking a thorough medical history and performing a physical examination, healthcare providers often order imaging tests such as X-rays, CT scans, or MRI scans to assess the alignment and stability of the C1 and C2 vertebrae. These tests help to confirm the diagnosis and evaluate the extent of instability.
What are the main symptoms of AAI?
The symptoms of AAI can vary depending on the severity of the condition. Common symptoms include:
- Neck pain or stiffness
- Headaches, especially at the base of the skull
- Reduced range of motion in the neck
- Numbness or tingling in the arms or legs
- Weakness in the limbs
- Difficulty walking or coordinating movements (in severe cases)
- Changes in bladder or bowel control (if spinal cord compression is present)
It is important to seek medical evaluation if you experience any of these symptoms, as untreated AAI can lead to serious complications.
Can AAI be treated without surgery?
Yes, many cases of AAI can be managed without surgery, especially if the instability is mild to moderate. Non-surgical treatments may include the use of cervical braces to stabilize the neck, physical therapy to strengthen the muscles supporting the cervical spine, and pain management strategies. These conservative approaches are often effective in controlling symptoms and preventing further progression of the instability.
However, it’s essential to consult a healthcare professional before starting any treatment to ensure that the chosen methods are appropriate and safe for your specific condition.
When is surgery necessary for AAI?
Surgery is typically considered when conservative treatments are not effective in managing symptoms or when there is a high risk of spinal cord compression. Common indications for surgery include:
- Worsening neurological symptoms (e.g., numbness, weakness, loss of motor control)
- Significant instability between the C1 and C2 vertebrae
- Failure of non-surgical treatments to provide relief
- Trauma-related AAI or congenital conditions that result in severe instability
The goal of surgery is to stabilize the cervical spine and prevent further damage to the spinal cord. The most common surgical procedures for AAI involve fusing the C1 and C2 vertebrae.
What are the risks of surgery for AAI?
Like any surgical procedure, surgery for AAI carries certain risks, including infection, bleeding, nerve damage, or failure of the fusion to heal properly. Additionally, patients who undergo cervical fusion may experience a permanent reduction in neck mobility. However, the primary benefit of surgery is the prevention of severe complications like spinal cord compression, which can lead to paralysis if left untreated.
It’s important to discuss the risks and benefits of surgery with your healthcare provider to determine if it’s the right option for you.
Will I lose neck mobility after surgery?
Yes, patients who undergo fusion of the C1 and C2 vertebrae will experience some loss of neck mobility, particularly in terms of rotation (turning the head). While this can be an adjustment, most patients are able to adapt to the reduced range of motion and continue with their daily activities. The trade-off between reduced mobility and the stabilization of the cervical spine is typically necessary to prevent further neurological damage and improve overall quality of life.
What is the recovery process like after surgery?
The recovery process after surgery for AAI typically involves wearing a cervical brace or collar for several weeks to support the neck and promote healing. Patients will gradually begin physical therapy to regain strength and mobility in the surrounding muscles. The initial recovery period usually lasts about 6 to 12 weeks, but full recovery, including the fusion of the bones, may take several months.
It’s important to follow your healthcare provider’s instructions carefully and attend all follow-up appointments to monitor your progress and ensure that the surgery was successful.
Can AAI recur after treatment?
In most cases, surgical fusion provides permanent stability to the atlantoaxial joint, significantly reducing the risk of recurrence. However, patients with underlying conditions such as rheumatoid arthritis or congenital disorders may need ongoing monitoring to ensure that the instability does not return or develop in other parts of the cervical spine. Regular follow-up appointments and imaging studies are essential to detect any changes early.
For patients who manage AAI non-surgically, recurrence of instability is possible if the underlying causes are not addressed or if the condition worsens over time. Adhering to preventive measures, such as maintaining good posture, engaging in strengthening exercises, and avoiding activities that strain the neck, can help reduce the risk of recurrence.
Red Flags: When to Seek Immediate Medical Attention
AAI can cause serious complications, particularly if it leads to spinal cord compression. It’s essential to seek immediate medical attention if you experience any of the following symptoms:
- Sudden onset of weakness or paralysis in the arms or legs
- Loss of bladder or bowel control
- Severe or worsening neck pain that does not respond to treatment
- Difficulty walking or maintaining balance
- Sudden loss of coordination or fine motor skills
These symptoms may indicate that the spinal cord is being compressed, and urgent treatment is necessary to prevent permanent neurological damage.
Conclusion: The Role of Early Management in AAI
Atlantoaxial Instability (AAI) is a serious condition that requires early diagnosis and prompt management to prevent complications such as spinal cord compression, chronic pain, or neurological damage. Early intervention is crucial, as it can prevent the progression of instability and improve overall patient outcomes.
Non-surgical management, including cervical braces, physical therapy, and osteopathic care, is often effective in mild to moderate cases, helping to stabilize the cervical spine and reduce symptoms. In more severe cases, surgical intervention, such as fusion or stabilization techniques, may be necessary to prevent further damage and ensure long-term stability. Post-surgical rehabilitation is vital for recovery, helping patients regain strength, mobility, and function.
Osteopathy plays a valuable role in addressing compensatory patterns and alleviating muscle tension that often arises due to AAI. However, it’s important to note that high-velocity cervical manipulation should be avoided in AAI patients due to the risk of worsening the instability.
Long-term success in managing AAI depends on patient education, regular follow-up, and adherence to preventive measures, such as proper posture, strengthening exercises, and lifestyle modifications. Individuals at higher risk, including those with congenital conditions or trauma-related AAI, should be especially proactive in monitoring their cervical spine health.
References
- Goel A. Indicators of atlantoaxial instability . J Craniovertebr Junction Spine. 2021 Apr-Jun;12(2):103-106. [ PMC free article ] [ PubMed ]2.
- Scholz C, Klingler JH, Scheiwe C, Naseri Y, Masalha W, Hubbe U. Atlantoaxial Instability in Patients Older Than 70 Years: What Is the Outcome When Further Conservative Treatment Is Not an Option? J Neurol Surg A Cent Eur Neurosurg. 2018 Sep;79(5):372-379. [ PubMed ]3.
- Cummings KR, Vilaplana Grosso F, Moore GE, Rochat M, Thomovsky SA, Bentley RT. Radiographic indices for the diagnosis of atlantoaxial instability in toy breed dogs [corrected]. Vet Radiol Ultrasound. 2018 Nov;59(6):667-676. [ PubMed ]4.
- Kothe R. [Rheumatoid instability in the cervical spine: Diagnostic and therapeutic strategies]. Orthopad. 2018 Jun;47(6):489-495. [ PubMed ]5.
- Yang SY, Boniello AJ, Poorman CE, Chang AL, Wang S, Passias PG. A review of the diagnosis and treatment of atlantoaxial dislocations. Global Spine J. 2014 Aug;4(3):197-210. [ PMC free article ] [ PubMed ]6.
- Macovei LA, Rezuş E. CERVICAL SPINE LESIONS IN RHEUMATOID ARTHRITIS PATIENTS. Rev Med Chir Soc Med Nat Iasi. 2016 Jan-Mar;120(1):70-6. [ PubMed ]7.
- Lyons C, Ross M, Elliott R, Tall M. Atlantoaxial Instability in a Patient with Neck Pain and Ankylosing Spondylitis. Mil Med. 2018 Sep 01;183(9-10):e654-e657. [ PubMed ]8.
- Goyal N, Bali S, Ahuja K, Chaudhary S, Barik S, Kandwal P. Posterior Arthrodesis of Atlantoaxial Joint in Congenital Atlantoaxial Instability Under 5 Years of Age: A Systematic Review. J Pediatr Neurosci. 2021 Apr-Jun;16(2):97-105. [ PMC free article ] [ PubMed ]9.
- Abou-Madawi AM, Ali SH, Alaswad M, Elkazaz MK, Abdelaziz MA, AlQazzaz MY, Al-Shatoury HA. Feasibility and Safety of Goel-Harms Posterior C1-C2 Fusion in the Management of Pediatric Reducible Atlantoaxial Instability . World Neurosurg. 2021 Nov;155:e592-e599. [ PubMed ]10.
- Burkhardt BW, Podolski W, Pitzen TR, Ruf M. The Feasibility of C1-C2 Screw-rod Fixation in the Children 5 Years of Age and Younger. J Pediatr Orthop. 2021 Sep 01;41(8):e651-e658. [ PubMed ]11.
- Raut S, Kundnani VG, Meena MK, Patel JY, Asati S, Patel A. Anthropometric evaluation for surgical feasibility of C1-C2 transarticular screw stabilization in Indian population. J Craniovertebr Junction Spine. 2021 Apr-Jun;12(2):129-135. [ PMC free article ] [ PubMed ]12.
- Su ML, Liu ZH, Tu PH, Huang YC. Dynamic cervical flexion/extension atlantodental interval and functional outcome of the Harms technique for posterior C1/2 fixation: A retrospective analysis of 16 atlantoaxial subluxation cases in a tertiary medical center. Neurosurgery. 2022 Feb;68(2):168-174. [ PubMed ]13.
- Kleinstück FS, Fekete TF, Loibl M, Jeszenszky D, Haschtmann D, Porchet F, Mannion AF. Patient-rated outcome after atlantoaxial (C1-C2) fusion: more than a decade of evaluation of 2-year outcomes in 126 patients. Eur Spine J. 2021 Dec;30(12):3620-3630. [ PubMed ]14.
- Tatter C, Fletcher-Sandersjöö A, Persson O, Burström G, Edström E, Elmi-Terander A. Fluoroscopy-Assisted C1-C2 Posterior Fixation for Atlantoaxial Instability : A Single-Center Case Series of 78 Patients. Medicine (Kaunas). 2022 Jan 12;58(1) [ PMC free article ] [ PubMed ]15.
- Malikov A, Secen AE, Divanlioglu D, Gunerhan G, Ocal O, Gunduz UK. The Feasibility of Creating Image-Based Patient-Specific Drill Guides for the Atlantoaxial Instabilities Using Open-Source CAD Software and Desktop 3D Printers. World Neurosurg. 2022 Jul;163:e377-e383. [ PubMed ]16.
- Jannelli G, Moiraghi A, Paun L, Cuvinciuc V, Bartoli A, Tessitore E. Atlantoaxial posterior screw fixation using intra-operative spinal navigation with three-dimensional isocentric C-arm fluoroscopy. Int Orthop. 2022 Feb;46(2):321-329. [ PubMed ]17.
- Du JY, Aichmair A, Kueper J, Wright T, Lebl DR. Biomechanical analysis of screw constructs for atlantoaxial fixation in cadaver: a systematic review and meta-analysis. J Neurosurg Spine. 2015 Feb;22(2):151-61. [ PubMed ]18.
- Zileli M, Akıntürk N. Complications of occipitocervical fixation: retrospective review of 128 patients with 5-year mean follow-up. Eur Spine J. 2022 Feb;31(2):311-326. [ PubMed ]19.
- Joaquim AF, Tedeschi H, Chandra PS. Controversies in the surgical management of congenital craniocervical junction disorders – A critical review. Neurol India. 2018 Jul-Aug;66(4):1003-1015. [ PubMed ]20.
- Robinson LC, Anderson RCE, Brockmeyer DL, Torok MR, Hankinson TC., Pediatric Craniocervical Society. Comparison of Fusion Rates Based on Graft Material Following Occipitocervical and Atlantoaxial Arthrodesis in Adults and Children. Opera Neurosurg (Hagerstown). 2018 Nov 01;15(5):530-537. [ PMC free article ] [ PubMed ]







")



{kind=link}