


What is Lumbar Radiculopathy?
Lumbar radiculopathy is a condition that results from compression or irritation of one or more lumbar nerve roots, representing a group of nerve disorders associated with these roots. Lumbar nerve roots are branches of nerves that emerge from the lumbar spine, located in the lower back. These roots contribute to the formation of the sciatic nerve, a major nerve that runs down the leg. Radiculopathy is also known by terms such as nerve root avulsion, nerve root compression, radicular inflammation, radiculitis, and radiculoneuritis.
Characteristic symptoms of lumbar radiculopathy include low back pain, often severe, with radiating pain along the lower limb. This pain may follow the course of a specific nerve root and is often described as burning, tingling, or numbness. Patients may also experience muscle weakness in the affected lower limb. These symptoms can vary in intensity and duration, and their severity depends on the location and extent of nerve compression.
Lumbar radiculopathy is most common in men over the age of 40, although it can also affect women, particularly in their 50s and 60s. Risk factors include age, degenerative spinal disorders such as herniated discs and spinal stenosis, and trauma or injury to the lumbar spine.
Common causes of lumbar radiculopathy include a herniated disc, where the intervertebral disc bulges and puts pressure on the nerve root, and spinal stenosis, which is a narrowing of the spinal canal that compresses the nerve roots. Other causes can include tumors, infections, and inflammation related to conditions such as ankylosing spondylitis.
Diagnosis of lumbar radiculopathy is based on a patient’s medical history, a thorough physical examination, neurological testing, and imaging studies such as magnetic resonance imaging (MRI) or computed tomography (CT) scans. Treatment of radiculopathy may involve conservative approaches such as physical therapy, analgesic and anti-inflammatory medications, and corticosteroid injections to reduce inflammation. In some severe cases or those resistant to conservative treatment, surgery may be considered to relieve nerve compression.
Causes of Lumbar Radiculopathy
Lumbar radiculopathy, or sciatica, can have several causes. The most common causes include problems affecting the lumbar (lower back) spine and associated nerve roots. Some of the main causes of lumbar radiculopathy include:
- Herniated disc: A herniated disc occurs when the jelly-like material inside an intervertebral disc protrudes through the outer wall of the disc, compressing a nerve root.
- Spinal stenosis: Spinal stenosis is a narrowing of the spinal canal, the part of the spine that houses the spinal cord. This narrowing can put pressure on nerve roots.
- Spondylolisthesis: This is an abnormal slippage of one vertebra over another. This can compress the nerve roots and cause radiculopathy.
- Lumbar Arthritis: Arthritis, especially osteoarthritis, can cause inflammation of the joints in the spine, which can lead to compression of the nerve roots.
- Tumors: Tumors in the lumbar region can compress nerve roots and cause symptoms of radiculopathy.
- Infections: Spinal infections, although less common, can also lead to irritation of the nerve roots.
- Trauma: Injuries to the spine, such as fractures or dislocations, can damage structures and cause compression of nerves.
- Degenerative Factors: Natural aging can lead to degeneration of the intervertebral discs, joints, and other structures of the spine, contributing to radiculopathy.
It is important to note that some people may be more predisposed to developing radiculopathy due to factors such as genetics, lifestyle, being overweight, and other risk factors. Accurately diagnosing the underlying cause of radiculopathy requires a thorough medical evaluation, often with imaging tests such as X-rays, MRI (magnetic resonance imaging), or CT (computed tomography) scans. Treatment will depend on the specific cause and may include conservative approaches or, in some cases, surgery.
Symptoms of Lumbar Radiculopathy
Lumbar radiculopathy, more commonly referred to as “sciatica” when it affects the sciatic nerve, is a painful condition caused by compression of a nerve in the lumbar spine. This compression can cause a variety of symptoms in the lower back, buttocks, legs, and sometimes even the feet. Recognizing these symptoms is essential to effectively diagnosing and treating the condition.
1. Severe Lower Back Pain
One of the first signs of lumbar radiculopathy is localized pain in the lower back. This pain can range in intensity from mild discomfort to a throbbing, burning pain. It is often made worse by movements such as bending, sitting, or lifting. The pain may also be worse with daily activities, such as walking or standing for long periods of time.
Low back pain is distinguished from general back pain because it is often associated with radiating pain that follows the path of nerves in the leg. It is this specific type of pain that helps healthcare professionals differentiate radiculopathy from other back conditions.
2. Radiated Pain (Sciatica)
Another characteristic symptom of lumbar radiculopathy is radiating pain, which follows the path of the affected nerve from the lumbar region to the leg or even to the foot. This pain, commonly called “sciatica,” is usually felt on one side of the body, although it can affect both sides in rare cases.
Sciatica pain is often described as a sharp, electric shock-like pain that travels down the leg. It can also feel like a burning or shooting sensation, making it difficult to move the affected leg. Sciatica is often triggered or made worse by movements such as coughing, sneezing, or getting up after sitting for a long time.
3. Numbness and Tingling
Numbness and tingling are common symptoms of lumbar radiculopathy, particularly along the affected leg. These sensations, also known as paresthesias, occur when nerve signals are disrupted due to compression or irritation of the nerve.
Numbness can occur in the leg, foot, or even the toes, giving the sensation that the area is “asleep.” Tingling, on the other hand, often feels like “ants” or “pins” invading the leg. These symptoms can be intermittent, sometimes occurring with pain or independently, and can seriously impair patients’ mobility and quality of life.
4. Muscle Weakness
Muscle weakness is another common sign of lumbar radiculopathy, and it results from the inability of the nerve to properly transmit signals to the muscles. This weakness can affect the legs and feet, making it difficult to perform simple tasks such as walking, climbing stairs, or even getting up from a chair.
In severe cases, weakness may be accompanied by loss of muscle control, especially those needed to maintain a stable position. For example, some people with lumbar radiculopathy may have difficulty standing on tiptoes or heels. Prolonged weakness can lead to muscle atrophy if left untreated.
5. Decreased Reflexes
Decreased reflexes in the lower extremities are a sometimes less obvious but telltale symptom of lumbar radiculopathy. During a physical exam, a healthcare professional may test the reflexes in the affected leg to see if they are normal. Decreased reflexes, such as a decreased knee jerk or Achilles jerk, often indicate lumbar nerve damage and are an important sign in the evaluation of radiculopathy.
6. Pain that varies depending on the position
A distinct aspect of lumbar radiculopathy is that pain and discomfort can vary depending on the position of the body. Certain postures, such as bending forward or rising from a sitting position, can make the pain worse. In contrast, some people experience relief by lying down or adopting a posture that decreases pressure on the nerves.
Positional pain can also be influenced by the type of nerve compression. For example, patients with foraminal stenosis (narrowing of the nerve openings) may experience relief by leaning their back forward, as this position slightly opens up the space around the nerves.
7. Changes in Sensitivity
Lumbar radiculopathy can also cause changes in the sensitivity of the lower limbs. Patients may notice reduced sensitivity in certain parts of the leg or foot, or conversely, hypersensitivity where the slightest touch causes intense pain. This alteration in perception can make it difficult to walk or even wear certain types of shoes, increasing discomfort in daily life.
- Radicular pain: Pain is the main symptom. It can manifest as a shooting, burning, or tingling pain along the course of the sciatic nerve, usually from the lower back to the buttock and leg. The pain can vary in intensity.
- Numbness and tingling: You may feel sensations of numbness, tingling, or weakness in your lower back, buttocks, leg, or foot.
- Muscle weakness: Compression of the nerve roots can cause muscle weakness in the affected leg or foot.
- Worse when sitting: The pain may be worse when sitting, coughing or sneezing, as this can increase pressure on the nerve roots.
- Difficulty standing: Some individuals may have difficulty standing or walking normally due to pain and weakness.
- Lower back pain: Pain may also be present in the lower back where nerve roots are compressed.
- Unilateral pain: Pain and other symptoms are usually present on the side where the nerve root is compressed.
- rhymed. However, it is possible to have bilateral symptoms if both sides are affected.


Diagnosis of Lumbar Radiculopathy
Lumbar radiculopathy is a condition characterized by compression or irritation of a spinal nerve in the lower back, resulting in pain radiating to the legs, numbness, tingling, and sometimes muscle weakness. An accurate diagnosis is essential to identify the cause of this compression and provide appropriate treatment. The diagnostic process is based on a combination of physical examination, the patient’s medical history, and additional tests, including imaging and neurological examinations.
Clinical Examination and Medical History of the Patient
The evaluation of a patient suspected of having lumbar radiculopathy begins with a detailed medical history and a thorough physical examination. This initial contact with the patient provides important information to guide diagnostic hypotheses and assess the severity of symptoms.
a. Collection of medical history
The medical history helps to better understand the evolution of pain and other symptoms, as well as the circumstances of their appearance. The practitioner questions the patient about:
- Characteristics of the pain : location, intensity, type of pain (burning, electric shock, stabbing), and possible radiation to the legs.
- Triggers and aggravating factors : Certain movements or positions can aggravate symptoms, which provides clues as to the origin of the nerve compression.
- Associated neurological symptoms : The practitioner looks for signs of muscle weakness, loss of sensation, numbness, or loss of reflexes in the legs.
- Medical history : Pre-existing conditions such as herniated discs, lumbar injuries or fractures, and disc degeneration problems are taken into account.
By combining reported symptoms and the patient’s history, the healthcare professional can identify useful clues to determine the area of nerve compression, often in the L4, L5 or S1 vertebrae, where lumbar radiculopathies are most common.
b. Physical examination
Physical examination can confirm or rule out certain characteristic signs of radiculopathy. The following tests are often performed:
- Lasègue test : lying on the back, the patient raises his right or left leg; if the pain is reproduced during elevation, this often indicates compression of the sciatic nerve.
- Deep tendon reflexes : The doctor tests the reflexes in the knee and ankle. Decreased reflexes may indicate nerve damage.
- Gait and muscle strength test : The patient is asked to walk on the heels or tiptoes. Weakness during these movements may suggest specific damage to the affected nerve.
- Sensory examination : the practitioner examines the sensitivity of the leg and foot to detect possible numbness or insensitive areas.
All of these assessments make it possible to identify clinical signs of nerve compression and to direct additional examinations to confirm the diagnosis.
Diagnostic Tools: Neurological Imaging and Tests
After the clinical examination, the practitioner may recommend imaging studies and neurological tests to visualize the structure of the spine, locate nerve compression, and assess the impact on the nerves.
a. Medical Imaging
Imaging is essential to observe spinal structures and confirm the site and cause of nerve compression. The main imaging techniques used are:
- X-ray : Although limited in observing soft tissues, X-rays can detect bone abnormalities such as fractures, osteoarthritis or osteophytes. They are useful in ruling out some causes of lower back pain of bone origin.
- MRI (Magnetic Resonance Imaging) : MRI is the imaging tool of choice for diagnosing lumbar radiculopathy. It provides detailed images of the soft tissues, intervertebral discs, ligaments, and nerves, helping to identify a herniated disc, foraminal stenosis, or disc degeneration that may be compressing the nerves. In addition, MRI helps detect signs of local inflammation or other abnormalities.
- CT scan (computed tomography) : Although less accurate than MRI for soft tissues, CT can be useful in some cases to visualize bone structures in detail. It is sometimes used in addition to MRI, particularly for patients with contraindications to MRI.
b. Tests Neurophysiologiques
Neurophysiological tests are performed to assess nerve functionality and detect signs of nerve damage:
- Electromyogram (EMG) : This test measures the electrical activity of muscles in response to nerve stimulation. It is particularly useful for confirming nerve damage and for identifying the level of the spine where compression is located.
- Nerve conduction study : This test measures the speed of transmission of nerve signals in peripheral nerves. In cases of lumbar radiculopathy, nerve conduction may be slowed in the affected nerve. This test is often used in conjunction with EMG to assess the extent and severity of nerve compression.
These tests are essential to confirm the presence of lumbar radiculopathy, assess its impact on the nervous system and help guide treatment choices.
Pathophysiology of lumbar radiculopathy
Here is a step-by-step explanation of the pathophysiology of lumbar radiculopathy:
- Herniated Disc or Spinal Stenosis:
- Most cases of lumbar radiculopathy are associated with a herniated disc or spinal stenosis. A herniated disc occurs when part of the intervertebral disc moves out of its normal position and puts pressure on the lumbar nerve roots. Spinal stenosis is the narrowing of the spinal canal, which can compress the nerve roots.
- Compression of Nerve Roots:
- A herniated disc or spinal stenosis can cause direct compression or irritation of the lumbar nerve roots. This usually occurs at the lumbar vertebrae, particularly between the fourth and fifth lumbar vertebrae (L4-L5) or between the fifth lumbar vertebra and the first sacral vertebra (L5-S1).
- Nervous Irritation:
- Compression of nerve roots results in local nerve irritation. This can cause symptoms such as shooting pain, tingling, numbness, and muscle weakness along the path of the affected nerves.
- Inflammatory Response:
- Irritation of the nerve roots triggers a local inflammatory response, resulting in increased blood flow to the affected area. Inflammation can worsen symptoms and contribute to the pain associated with radiculopathy.
- Radicular Pain:
- The pain resulting from radiculopathy is often described as radicular pain that follows the path of the affected nerve. For example, a herniated disc at the L4-L5 level can cause pain along the sciatic nerve, which runs down the back of the leg to the foot.
- Sensory and Motor Alterations:
- In addition to pain, nerve root compression can cause sensory alterations, such as numbness or tingling, as well as motor alterations, such as muscle weakness in the muscles innervated by the affected nerves.
- Aggravation by Movements:
- Symptoms of radiculopathy may be exacerbated by certain movements, such as bending or rotating the lumbar spine. These movements can increase pressure on the irritated nerve roots.
- Risk Factors:
- Certain risk factors, such as aging, a sedentary lifestyle, obesity, excessive physical activity, and certain anatomical disorders of the spine, can increase the likelihood of developing lumbar radiculopathy.
Decrease in intervertebral space
Lumbar radiculopathy, a painful neurological condition that can cause symptoms throughout the lower extremities, often results from structural changes in the spine. One of these major changes is the narrowing of the intervertebral space, which directly affects the intervertebral foramen, or foramen conjugation, through which spinal nerve roots pass. In this article, we explore the role of this space, its changes with aging or disease, and the implications for nerve health, particularly in patients with chronic low back pain.
Role of the Nucleus Pulposus and the Intervertebral Space
Intervertebral discs play a fundamental role in maintaining the intervertebral space. Each disc is composed of two essential parts: the annulus fibrosus, which forms the tough outer layer, and the nucleus pulposus, a gelatinous, hydrophilic substance in the center. This nucleus, rich in proteoglycans, attracts water to maintain hydration and allow the disc to resist compression. The function of the nucleus pulposus is therefore not limited to shock absorption; it also ensures the maintenance of intervertebral height and evenly distributes pressure on the annulus fibrosus and the vertebral endplates.
When the nucleus pulposus dries out or the annulus fibrosus deteriorates, the height of the disc decreases, causing the vertebrae to move closer together. This reduces the intervertebral space and affects the intervertebral foramen, or foramen conjugation, the essential passage for nerve roots exiting the spine. The reduction of this space often leads to nerve compression, the main cause of lumbar radiculopathy.
Consequences of Intervertebral Space Reduction
The reduction of the intervertebral space has serious consequences for the surrounding nerve structures:
- Nerve compression : With the decrease in space in the foramen, the nerve roots are compressed, which results in radiating pain, numbness, tingling, and sometimes muscle weakness in the lower limbs. This type of compression is common in patients with sciatica.
- Inflammation : Prolonged compression can lead to local inflammation, exacerbating pain and causing muscle spasms.
- Loss of mobility : As the space between the vertebrae decreases, the spine loses flexibility, and movement becomes more painful. This stiffness can impair quality of life, making it difficult to perform daily activities such as walking or standing.
Causes of Intervertebral Space Decrease
Narrowing of intervertebral space can result from several factors:
- Aging : Over the years, intervertebral discs naturally lose their elasticity and their ability to retain water, which reduces disc height.
- Disc degeneration : With age and due to certain risk factors such as obesity or repeated trauma, the discs become thinner, leading to a loss of intervertebral space and greater proximity of the foramens.
- Mechanical and postural factors : Poor posture, repetitive mechanical stress and certain prolonged static positions also promote the reduction of intervertebral space.
Management and Prevention of Intervertebral Space Decrease
For osteopaths and other health professionals, a good understanding of the techniques for managing this decrease in intervertebral space is crucial:
Spinal decompression techniques : Certain techniques, such as traction, can temporarily widen the intervertebral space, relieving pressure on the nerves.
Manual therapy : Osteopathic techniques, including gentle spinal manipulation, can help improve mobility, release muscle tension and, in some cases, relieve nerve compressions.
Hydration : It is important to remind patients of the importance of good hydration, as it helps maintain the elasticity and hydration of the intervertebral discs.
Strengthening and stretching : Specific muscle strengthening exercises and appropriate stretches help keep the spine stable, which can reduce disc compression.


Differential diagnoses of lumbar radiculopathy
- Herniated disc: A herniated disc occurs when the jelly-like core inside an intervertebral disc moves out of its normal position and can compress nerve roots.
- Spinal stenosis: Spinal stenosis is the narrowing of the spinal canal, which can lead to compression of the nerve roots. This can cause symptoms similar to those of lumbar radiculopathy.
- Spondylolisthesis: This is a condition where one vertebra slips forward relative to the vertebra below it, which can cause compression of the nerve roots.
- Piriformis syndrome: The sciatic nerve can pass through or under the piriformis muscle, and if this muscle is tight or inflamed, it can compress the nerve and cause symptoms similar to lumbar radiculopathy.
- Lumbar Arthritis: Arthritis in the lumbar spine can lead to irritation of the nerves and cause symptoms similar to those of radiculopathy.
- Lumbar plexus injuries: Injuries to the lumbar plexus, a network of nerves in the lower back, can cause symptoms similar to those of radiculopathy.
- Infections: Infections of the spine, although less common, can cause similar neurological symptoms.
Posture
Lumbar radiculopathy, a condition characterized by irritation or compression of the nerve roots of the lumbar spine, can result in a variety of adaptive responses in patients. One common response is adopting an unnatural posture in an attempt to relieve pressure on the affected nerve root and alleviate associated pain.
Patients with lumbar radiculopathy often experience shooting pain, tingling, or numbness along the affected nerve, which can radiate to the lower extremities. Faced with this debilitating pain, it is common for individuals to alter their natural posture to find a more comfortable position, even if it is considered “unnatural” from a biomechanical perspective.
The primary goal of postural adjustment in patients with lumbar radiculopathy is to reduce pressure on the compromised nerve root. These adjustments may include lateral trunk tilt, forward trunk bending, or even body twists. These altered postures may provide temporary relief by minimizing compression on the nerves, but they may also contribute to other postural and musculoskeletal problems in the long term.
It is important to note that these unnatural postures adopted by patients can lead to harmful consequences in the long term. Prolonged changes in posture can lead to muscle imbalances, joint tension and mobility limitations, thus aggravating existing problems. In addition, these adjustments can negatively influence the quality of daily life of patients, affecting their ability to perform simple activities and maintain a normal life.
The use of altered postures can also influence the gait pattern of individuals with lumbar radiculopathy. Some patients may develop compensatory walking habits to minimize pain, which can lead to muscle imbalances and postural abnormalities. These changes in gait can make the condition worse by placing increased pressure on other parts of the body, creating a vicious cycle of musculoskeletal problems.
Treatment for lumbar radiculopathy is not limited to symptom management alone, but should also include a holistic approach aimed at restoring normal spinal function. This may involve interventions such as physical therapy, therapeutic exercise, pain management, and in some cases, medical or surgical procedures.


Exercise and Stretching to Help Those Suffering from Lumbar Radiculopathy
Here are some stretches that might be considered under the supervision of your healthcare professional or a physical therapist:
- Psoas Stretch:
- Kneel on the floor.
- Step one foot forward so that your knee is bent 90 degrees.
- Gently tilt your pelvis forward, keeping your back straight, until you feel a stretch in the front of the hip on the stretched side.
- Hold the position for 15 to 30 seconds and repeat on the other side.
- Piriformis Stretch:
- Sit on the floor with the affected leg bent and the other leg extended.
- Place the foot of the bent leg on the thigh of the other leg.
- Lean forward slightly while keeping your back straight until you feel a stretch in the buttock on the stretched side.
- Hold the position for 15 to 30 seconds and repeat on the other side.
- Core Stretch:
- Sit on the floor with your legs extended in front of you.
- Gently rotate your torso to one side, using your arms to help you reach a little further.
- Hold the position for 15 to 30 seconds and repeat on the other side.
- Standing Quadriceps Stretch:
- Stand with one hand on a stable support.
- Bend one leg and grab your ankle with the hand on the same side.
- Bring your heel toward your buttock until you feel a stretch in the front of your thigh.
- Hold the position for 15 to 30 seconds and repeat on the other side.
Be sure to do these stretches slowly and gently, without forcing the movement. If you feel sharp pain or if symptoms worsen, stop immediately and consult your healthcare professional. A specific exercise program can be developed based on your individual condition and the underlying cause of radiculopathy.
Preventing Lumbar Radiculopathy
Although it is not always possible to completely prevent lumbar radiculopathy, there are several lifestyle measures and habits that can help reduce the risk or minimize the likelihood of developing lumbar radiculopathy. Here are some tips:
- Maintain a Healthy Weight :
- Excess weight can put additional stress on the spine. Maintaining a healthy weight through a balanced diet and regular physical activity can help reduce the risk of lumbar radiculopathy.
- Regular Exercise :
- Get regular physical activity to strengthen the muscles that support your spine. Focus on exercises that improve core strength, flexibility, and overall spinal health.
- Proper Lifting Techniques :
- When lifting heavy objects, use proper lifting techniques. Bend at the knees rather than the waist, and lift with your legs rather than your back. Avoid twisting your spine while lifting.
- Good Posture :
- Maintain good posture, whether sitting or standing. Use ergonomically designed furniture and workstations to support healthy spinal alignment.
- Avoid Prolonged Sitting :
- Take breaks and avoid sitting for long periods of time. If your job requires long periods of sitting, consider using a standing desk or taking short breaks to stretch and move around.
- Regular Stretching :
- Incorporate regular stretching exercises into your routine, focusing on the muscles in your lower back, hips, and legs. This can help maintain flexibility and reduce muscle tension.
- Stop Smoking :
- Smoking has been linked to an increased risk of degenerative disc disease. Quitting smoking can help with overall spinal health.
- Suitable Shoes:
- Wear comfortable, supportive shoes. High heels or poorly designed shoes can affect your posture and spinal alignment.
- Stay Hydrated :
- Drink adequate amounts of water to keep the discs in your spine well hydrated, which contributes to their shock-absorbing properties.
- Regular Consultations :
- Schedule regular visits with your healthcare professional to monitor and promptly treat any developing problems.
It is important to note that while these lifestyle measures can contribute to spinal health, some causes of lumbar radiculopathy are related to factors beyond lifestyle choices, such as herniated discs, spinal stenosis, or other degenerative conditions. If you experience persistent back pain or symptoms suggestive of lumbar radiculopathy, it is crucial to consult a healthcare professional for appropriate treatment.
FAQ about Lumbar Radiculopathy
What is lumbar radiculopathy?
Lumbar radiculopathy is a painful condition that results from compression or irritation of a spinal nerve in the lumbar region, that is, the lower back. This compression causes pain that often radiates to the buttocks, legs, and sometimes to the feet. This condition is often called “sciatica” when the sciatic nerve is involved.
What are the main causes of lumbar radiculopathy?
Causes of lumbar radiculopathy include:
- Herniated disc : When the intervertebral disc shifts or ruptures, it puts pressure on the nerve root.
- Foraminal stenosis : Narrowing of the spaces through which nerves exit the spine, causing compression.
- Osteoarthritis and osteophytes : Wear and tear on the vertebral joints generates bony growths that can compress the nerves.
- Disc degeneration : With age, the discs lose height and hydration, bringing the vertebrae closer together and increasing the risk of nerve compression.
What are the typical symptoms of lumbar radiculopathy?
The most common symptoms include:
- Lower back pain radiating down the leg : Often felt as a sharp, burning or electric shock type pain.
- Numbness and tingling : Mainly in the leg or foot, often along the path of the affected nerve.
- Muscle weakness : Difficulty lifting the leg, walking, or standing on tiptoe.
- Decreased reflexes : Particularly at the knee or ankle.
How is lumbar radiculopathy diagnosed?
Diagnosis begins with a physical examination and evaluation of the patient’s medical history. Imaging tests such as MRI or CT scan are often used to visualize the spine and identify the source of nerve compression. In some cases, an electromyogram (EMG) may be performed to assess nerve function and detect possible nerve damage.
What treatments are recommended for lumbar radiculopathy?
Treatment depends on the severity of symptoms and underlying causes:
- Conservative treatments : Include rest, physical therapy, stretching, and anti-inflammatory medications to relieve pain.
- Corticosteroid injections : Given directly into the spine to reduce local inflammation.
- Surgical interventions : In severe or persistent cases, surgery may be necessary to release the nerve compression.
- Complementary approaches : Osteopathy, acupuncture, and chiropractic can provide significant relief in addition to medical treatments.
Can lumbar radiculopathy be prevented?
Prevention involves several good practices, including:
- Adopt good posture : Sit and lift ergonomically to reduce pressure on the spine.
- Regular exercise : Strengthening the core muscles helps stabilize the spine.
- Avoid carrying heavy loads : Especially by adopting appropriate lifting techniques.
- Hydration and nutrition : Maintaining good hydration promotes the elasticity of the intervertebral discs.
Is lumbar radiculopathy a chronic condition?
It can be temporary or become chronic depending on the cause and management. With appropriate treatment, many people manage to relieve their symptoms and prevent recurrences. However, if the compressive factors persist without treatment, the symptoms can become recurrent or chronic.
When to consult an osteopath for lumbar radiculopathy?
It is advisable to consult an osteopath or other health professional if:
- The pain has persisted for more than two weeks with no improvement.
- The pain is intense and limits daily mobility.
- Neurological symptoms, such as numbness or muscle weakness, occur.
- You have difficulty walking or maintaining balance.
What is the difference between lumbar radiculopathy and simple lower back pain?
Simple lower back pain is often caused by muscle strains, sprains, or poor posture, and is usually limited to the lower back. Lumbar radiculopathy, on the other hand, involves compression of a nerve, causing pain that radiates to the legs, numbness, tingling, and sometimes muscle weakness. These distinctive symptoms help differentiate radiculopathy from simple lower back pain.
Can exercises help with lumbar radiculopathy?
Yes, there are exercises that can help relieve symptoms of lumbar radiculopathy. Core strengthening exercises, hamstring stretches, and gentle spinal mobilization can reduce pressure on nerves and improve spinal stability. However, it is important to consult a healthcare professional or osteopath to ensure that the exercises are appropriate and will not worsen symptoms.
Can lumbar radiculopathy be treated without surgery?
In many cases, lumbar radiculopathy can be managed without surgery. Conservative approaches such as physical therapy, osteopathic adjustments, anti-inflammatory medications, and postural modifications can help reduce nerve compression and relieve symptoms. Surgery is usually considered as a last resort, when symptoms are severe, persist despite treatment, or result in loss of function.
Can lumbar radiculopathy recur?
Yes, lumbar radiculopathy can recur, especially if risk factors such as poor posture, lack of physical activity, or repetitive movements are not corrected. A prevention program including regular exercise, good posture hygiene, and regular visits to an osteopath to monitor the condition of the spine can help reduce the risk of recurrence and maintain good lumbar health.
Osteopathy
Osteopathic techniques for treating lumbar radiculopathy may include:
- Soft tissue manipulation:
- Osteopathic practitioners often use soft tissue manipulation to release tension in the muscles, tendons, and ligaments surrounding the lumbar spine. This can help improve blood circulation, reduce inflammation, and relieve pressure on affected nerves.
- Joint mobilization:
- Gentle joint mobilization techniques can be applied to the lumbar spine to improve joint function and reduce stiffness. This can help improve range of motion and relieve pressure on affected nerve roots.
- Muscle Energy Techniques (MET)
- MET involves the active and controlled contraction of muscles against a defined resistance. In lumbar radiculopathy, the
- MET can be used to improve muscle strength and flexibility, promoting better spinal support.
- Counter-stress technique:
- This technique involves the practitioner finding a position that relieves tension in the affected muscles and tissues, promoting relaxation and reducing pain associated with lumbar radiculopathy.
- Myofascial release:
- Osteopaths can use myofascial release techniques to treat restrictions and adhesions in the fascia, the connective tissue that surrounds muscles and nerves. This can help improve mobility and reduce pain.
- Lumbar traction:
- Traction can be used to gently stretch the spine and create space between the vertebrae, reducing pressure on the nerve roots. This can help relieve pain in cases of lumbar radiculopathy.
The Benefits of Osteopathic Treatment for Lumbar Radiculopathy”
Here is a curated list of scientific articles demonstrating the effectiveness of osteopathic treatment for lumbar radiculopathy. Each study is summarized for clarity and includes a direct link for further reading.
Title: Prevalence and Recovery Rate of Low Back Pain and Leg Pain in Osteopathic Practice
Summary: This study explores the recovery rates of patients undergoing osteopathic treatments for low back and leg pain, highlighting its effectiveness in mitigating symptoms associated with lumbar radiculopathy.
Read Here
Title: Outcomes of Osteopathic Manual Treatment for Chronic Low Back Pain
Summary: The OSTEOPATHIC trial investigates osteopathic manual therapy (OMT) as a non-invasive intervention for chronic back pain and potential radiculopathy. Results show significant improvements in pain severity and functional outcomes.
Read Here
Title: Osteopathic Manipulative Treatment for the Management of Adjacent Segment Pathology
Summary: This study evaluates the role of osteopathic manipulative treatment (OMT) in managing lumbar radiculopathy caused by adjacent segment pathology. Significant functional improvements were noted post-treatment.
Read Here
Title: Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review
Summary: A systematic review that consolidates evidence on the efficacy of manual therapy techniques, including osteopathy, in treating lumbar radiculopathy.
Read Here
Title: Spinal Manipulation for Subacute and Chronic Lumbar Radiculopathy
Summary: This randomized controlled trial highlights the positive outcomes of spinal manipulation therapy on patients with lumbar radiculopathy, with significant improvements in mobility and pain relief.
Read Here
Title: Efficiency of Physical Therapy and Osteopathic Techniques in Recurrent Lumbar Disc Herniation
Summary: Case report demonstrating the combined effectiveness of osteopathic and physical therapy techniques in treating recurrent lumbar disc herniation with associated radiculopathy.
Read Here
Title: Short-Term Study on Risk-Benefit Outcomes of Spinal Manipulative Therapies
Summary: Focuses on spinal manipulative therapies, including osteopathic techniques, for acute radiculopathy caused by lumbar disc herniation, showing favorable outcomes.
Read Here
Title: Osteopathic Manipulative Treatment for Chronic Low Back Pain
Summary: A systematic review analyzing multiple randomized controlled trials to determine the effectiveness of OMT for chronic low back pain with and without radiculopathy.
Read Here
Title: An Osteopathic Approach to Degenerative and Herniated Discs
Summary: The study emphasizes the osteopathic approach to managing degenerative and herniated discs, often causing lumbar radiculopathy, and discusses significant symptom relief.
Read Here
Title: Two Manual Therapy Techniques for Lumbar Radiculopathy: A Randomized Clinical Trial
Summary: Compares two osteopathic manual therapy techniques for lumbar radiculopathy, demonstrating their effectiveness in pain and mobility improvements.
Read Here
Title: Osteopathic Manipulative Treatment in Lumbar Disc Pathologies
Summary: This paper highlights the advantages of OMT for lumbar disc pathologies, demonstrating symptom improvement and reduced radiculopathy severity.
Read Here
Title: Effectiveness of Manual Therapy in Treating Lumbar Radiculopathy
Summary: A clinical review consolidating evidence for manual therapy techniques, including osteopathy, in alleviating radiculopathy symptoms.
Read Here
Title: Comparative Outcomes of Spinal Manipulation and Osteopathy for Radiculopathy
Summary: This comparative study evaluates the outcomes of spinal manipulation and osteopathic techniques, reporting significant improvement in pain relief and function.
Read Here
Title: Adjunctive Osteopathic Techniques in Chronic Lumbar Radiculopathy
Summary: This study focuses on the role of adjunctive osteopathic techniques in chronic cases, demonstrating enhanced recovery rates.
Read Here
Title: Longitudinal Benefits of OMT in Lumbar Disc-Related Radiculopathy
Summary: Explores long-term outcomes of OMT in managing lumbar disc herniation and radiculopathy, showing sustained benefits.
Read Here
Title: Evidence-Based Osteopathic Treatment for Lumbar Radiculopathy
Summary: A review discussing evidence-based approaches to OMT, highlighting its role in conservative management strategies for lumbar radiculopathy.
Read Here
Title: Osteopathic Manual Therapy and Neurological Symptoms in Radiculopathy
Summary: This research investigates the neurological benefits of OMT in patients with radiculopathy, noting improved nerve function and reduced pain.
Read Here
Title: Multimodal Therapy with Osteopathy in Lumbar Pain Syndromes
Summary: Evaluates the effectiveness of combining osteopathic techniques with other modalities, finding superior results for lumbar radiculopathy treatment.
Read Here
Title: Randomized Controlled Trials of OMT for Lumbar Disc Herniation
Summary: Highlights randomized controlled trials demonstrating OMT’s efficacy in managing lumbar disc herniation and associated radiculopathy.
Read Here
Title: Patient Outcomes Following Osteopathic Intervention in Lumbar Radiculopathy
Summary: Analyzes patient-reported outcomes post-osteopathic treatment, showing improved quality of life and decreased pain levels.
Read Here
Osteopathy
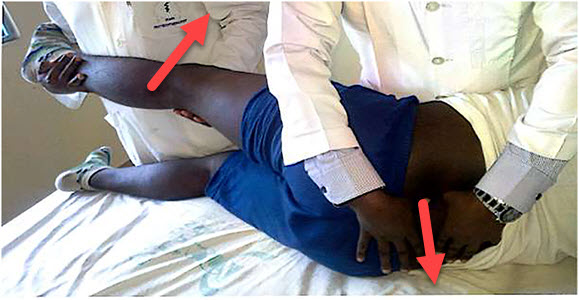
Mobilization of the spine with leg movement
Synonyme : Mobilisation vertébrale avec mouvement des jambes
Indication: Leg pain and other symptoms that extend below the knee induced by the SLR test.
Technique:
- This technique requires a therapist and an assistant.
- The patient is in a side-lying position with the affected leg on top near the edge of the treatment table. The affected leg is extended with a slight abduction at the hip and held by the assistant. The therapist applies and maintains a transverse glide from the spinous process to the floor of the cranial vertebra at the affected segment.
- The patient actively moves the leg in SLR with the help of the assistant.
- This position is maintained for 30 seconds
- The treating therapist releases the pressure on the spinous process and the patient lowers the supported leg onto the treatment table.
- Three rehearsals during the first visit.
- However, when the patient has improved during subsequent visits, the therapist should apply overpressure to the supported leg while the assistant performs the SLR.
- This pressure was also maintained for 30 seconds, after which the leg must be lowered onto the treatment table. This procedure was repeated six times on subsequent visits.
- At the end of a session, always reassess the SLR in the supine position.

Progressive inhibition of neuromuscular structures (PNMS)
Definition: A form of inhibition technique developed by Dennis Dowling, DO. The practitioner locates two related points and sequentially applies pressure along a series of related points:
Technique:
- Two connected points, called primary and end points, must be found. These points are the most and least sensitive areas, respectively, along a neuromuscular structure.
- When an area of reduced tenderness (end point) was found, moderate ischemic compression was applied with the index finger of one hand without releasing the pressure until the treatment was completed.
- When an area of greater sensitivity was found (primary point), moderate ischemic compression was also applied with the index finger of the other hand for 30 s, after which another sensitive point was identified with the middle finger of the same hand in the vicinity of the final point without releasing the index finger pressure.
- When the middle finger pressure was judged to be more sensitive than the index finger, pressure, the index finger, pressure was released and the middle finger pressure was held without releasing the end point pressure. This was maintained for 30 s before the third point was identified. Similar patterns for all identified tender points were followed continuously along the neuromuscular continuum until the last point, approximately 2 cm from the end point, was found. Pressure was held for 30 seconds simultaneously on both points (the last and the end point) and then released.


Conclusion
In conclusion, lumbar radiculopathy is a neurological condition that can significantly impair individuals’ quality of life due to compression or irritation of the lumbar nerve roots. The varied symptoms, such as pain, numbness, muscle weakness, and tingling sensations, can lead to functional limitations and daily discomfort.
This condition, which is more common in men over 40 and also affects women, requires a thorough diagnostic approach that includes medical history, physical examinations, and imaging investigations. Treatment for lumbar radiculopathy varies depending on the severity of symptoms, ranging from conservative approaches such as physiotherapy and medications to more interventional options, including surgery, in more severe cases.
Management of lumbar radiculopathy should be personalized, taking into account the specific characteristics of each patient. Close collaboration between healthcare professionals and patients is essential to determine the optimal treatment plan and optimize outcomes.
Although lumbar radiculopathy can present significant challenges, advances in the medical field offer diverse options to relieve symptoms and restore functionality. Current approaches aim to improve the quality of life of those affected, adapting to their individual needs and minimizing the disruptions caused by this neurological condition.
References
- Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010 Dec;24(6):769-81. [PubMed]2.
- Urits I, Burshtein A, Sharma M, Testa L, Gold PA, Orhurhu V, Viswanath O, Jones MR, Sidransky MA, Spektor B, Kaye AD. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Curr Pain Headache Rep. 2019 Mar 11;23(3):23. [PubMed]3.
- Tarulli AW, Raynor EM. Lumbosacral radiculopathy. Neurol Clin. 2007 May;25(2):387-405. [PubMed]4.
- van der Windt DA, Simons E, Riphagen II, Ammendolia C, Verhagen AP, Laslett M, Devillé W, Deyo RA, Bouter LM, de Vet HC, Aertgeerts B. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 2010 Feb 17;(2):CD007431. [PubMed]5.
- Al Nezari NH, Schneiders AG, Hendrick PA. Neurological examination of the peripheral nervous system to diagnose lumbar spinal disc herniation with suspected radiculopathy: a systematic review and meta-analysis. Spine J. 2013 Jun;13(6):657-74. [PubMed]6.
- Nguyen HS, Doan N, Shabani S, Baisden J, Wolfla C, Paskoff G, Shender B, Stemper B. Upright magnetic resonance imaging of the lumbar spine: Back pain and radiculopathy. J Craniovertebr Junction Spine. 2016 Jan-Mar;7(1):31-7. [PMC free article] [PubMed]7.
- Kennedy DJ, Noh MY. The role of core stabilization in lumbosacral radiculopathy. Phys Med Rehabil Clin N Am. 2011 Feb;22(1):91-103. [PubMed]8.
- Tang S, Mo Z, Zhang R. Acupuncture for lumbar disc herniation: a systematic review and meta-analysis. Acupunct Med. 2018 Apr;36(2):62-70. [PubMed]9.
- Wenger HC, Cifu AS. Treatment of Low Back Pain. JAMA. 2017 Aug 22;318(8):743-744. [PubMed]







{kind=link}