


Discover the crucial impact of pronation on your musculoskeletal well-being and explore preventative solutions to maintain the biomechanical balance of your feet
Introduction
Pronation is a natural movement of the foot that occurs when walking or running. It involves an inward rolling of the foot to absorb the impact of body weight. Normal pronation is an essential part of the gait cycle and contributes to the even distribution of forces across the foot.
However, excessive pronation can lead to biomechanical imbalances and cause various problems. In the context of what you call “foot pronation syndrome”, it can be assumed that this is a reference to pathological pronation, that is, pronation that exceeds normal limits and can lead to complications.
Symptoms associated with excessive pronation may include pain in the feet, ankles, knees, hips, or back. Complications such as plantar fasciitis, knee pain, and other musculoskeletal problems can also occur.
It is important to note that if you suspect problems with excessive pronation, it is recommended to consult a healthcare professional, such as a podiatrist, orthopedist or physiotherapist, for an accurate diagnosis and treatment recommendations tailored to your individual situation. .
Pronation
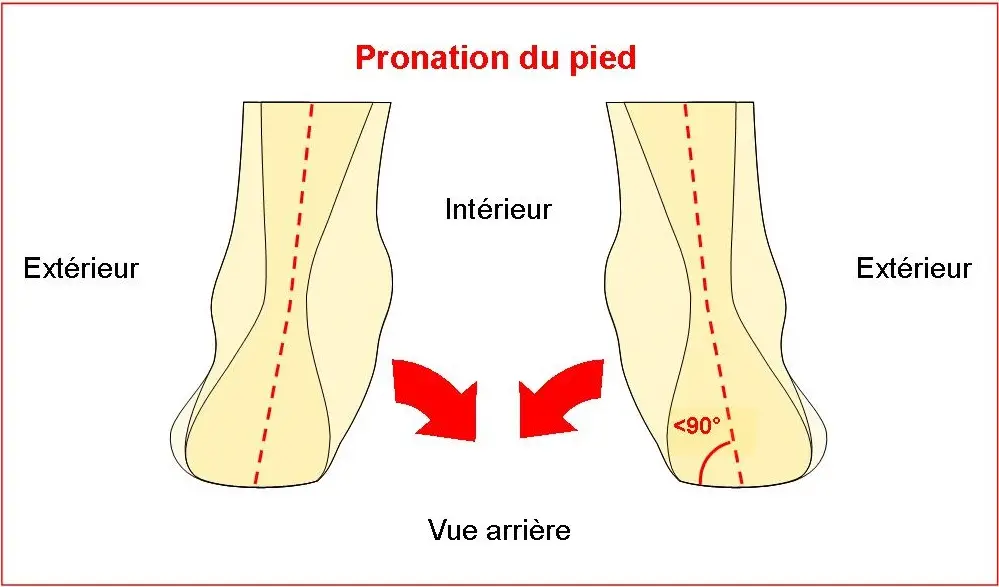
Pronation is a natural movement of the foot that occurs when walking or running. This is the inward rotational movement of the foot, particularly at the ankle. When pronating, the foot rolls inward, allowing the ball of the foot to adapt to the ground during the ground contact phase.
The pronation process begins when the heel hits the ground, and the foot then rolls inward, distributing the body’s weight. Pronation is essential for absorbing shock and allowing even force distribution when walking or running. It also contributes to the adaptability of the foot to different surfaces.
It is important to note that pronation is a normal and necessary movement for the biomechanics of the foot. However, overpronation or underpronation can sometimes lead to problems, including gait disturbances, foot pain, ankle pain, and even knee and hip problems. Proper pronation balance is therefore important to maintain efficient walking and running and minimize the risk of injury.

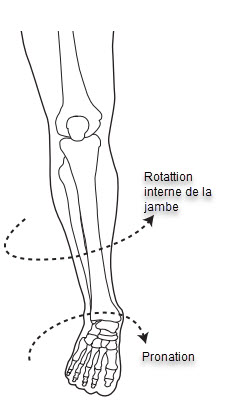
Internal rotation of the femur and tibia
Pronation, a natural movement of the human body, is often associated with internal rotation of the tibia and femur. These two essential leg bones play a crucial role in the stability and mobility of the body. When pronation occurs, it induces an inward rotation of these bones, creating a series of physiological and biomechanical responses.
This internal rotation of the tibia and femur can be seen during various physical activities, such as walking, running, or other functional movements. It occurs particularly at the knee joint, where coordination between these bones is essential to maintain balance and absorb shock during daily activities.
However, it is important to note that excessive levels of pronation can sometimes lead to orthopedic problems. Excessive internal rotation can place additional stress on joints and surrounding structures, increasing the risk of injury. People who play high-impact sports or have anatomical variations may be more likely to exhibit excessive pronation.

Mechanism of pronation syndrome

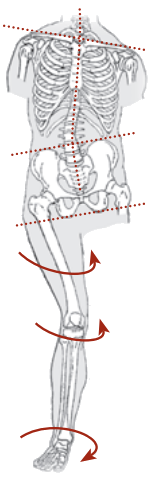
Repetitive overpronation when walking or running can have significant consequences on the biomechanics of the foot and the entire kinetic chain. By reducing shock absorption by the foot and compromising stability and propulsion efficiency, this anomaly can lead, over time, to compensatory muscle fatigue and poor biomechanics. The adverse effects of overpronation can propagate down the kinetic chain, affecting the foot, ankle, knee, hip, pelvis and spine.
Overpronation induces a functionally short leg and generates an increase in valgus forces at the knee and hip. These excessive forces cause repeated twisting and shearing on the lower limb, increasing wear and tear on the anatomical structures. Ligaments, cartilage and even bones can experience increased stress, promoting a process of premature wear.
This disruption in the natural biomechanics of walking or running can contribute to disorders such as osteoarthritis, ligament and cartilage injuries, and structural misalignments. Chronic overpronation may also be a risk factor for the development of various pathologies, including tendinitis, plantar fasciitis, and other musculoskeletal conditions.
It is imperative to take preventive and corrective measures to minimize the effects of overpronation, including wearing appropriate shoes, using orthopedic insoles, and adopting specific muscle strengthening exercises. A professional assessment by a podiatrist or orthopedist can guide these interventions to preserve the health and integrity of the kinetic chain.
Risk factors
- Individual biomechanics: The anatomical structure of the foot, such as the shape of the arch, can predispose to excessive pronation.
- Heredity: Genetic predispositions may play a role in the inheritance of certain biomechanical characteristics, including pronation.
- Weakened muscles: The muscles of the foot and leg play a crucial role in maintaining stability. Muscle weakness can promote excessive pronation.
- Inappropriate shoes: Frequently wearing shoes that do not provide adequate support can contribute to excessive pronation.
- Intensive physical activities: Certain sports or repetitive physical activities can put increased pressure on the feet, thus promoting excessive pronation.
- Age: Children and adolescents are sometimes more likely to exhibit excessive pronation due to the growth and development of the foot.
- Obesity: Excess weight can increase the load on the feet, leading to excessive pronation to compensate for this increased pressure.
- Pre-existing medical conditions: Certain conditions, such as congenital flatfoot, may be associated with excessive pronation.
- Previous trauma or injury: Previous injuries to the feet, ankles, or lower extremities can disrupt normal biomechanics, promoting excessive pronation.
- Walking Surface: Frequently walking or running on hard or uneven surfaces can influence pronation.
Inspection of the sole of a shoe as an indicator of excessive pronation
When examining the sole of a shoe worn regularly, several signs can suggest excessive pronation:
- Uneven sole wear: Greater wear on the inner side of the sole may indicate that the foot has a propensity to roll inward, which is characteristic of excessive pronation.
- Mid-section sagging: A noticeable deformity or sagging of the mid-sole can also be an indicator of pronation. This can result from excessive weight being placed on this area due to excessive inward rolling of the foot.
- Increased wear on the inner heel: More pronounced wear on the inner heel of the shoe can indicate excessive load on this region due to pronation, because the heel has a tendency to tilt inwards during this movement.
- Compression or deformation of the insole: Compression or deformation of the insole of the shoe, particularly on the inner side, may be related to the added pressure exerted by excessive pronation.

Arch inspection
When checking arch height, it is essential to note that having flat feet does not necessarily guarantee the presence of overpronation. Flat feet are characterized by a sagging medial arch, whether in a supportive position or not. This anatomical feature can be observed even when the foot is in a neutral position or at rest.
Contrary to this, individuals with overpronation syndrome have an arch that sags only when they are in a supportive position, i.e. standing or walking. In other words, the arches of those with overpronation appear normal when they are sitting or at rest, but they sag excessively when they support their body weight.


In the case of a normal foot that supports body weight when standing, it is usually possible for the fingers to slide under the arch of the foot. This anatomical feature indicates a natural curvature of the arch, allowing for effective support and balanced weight distribution.
However, in the presence of overpronation, the dynamics change significantly. Overpronation occurs when the foot has an excessive tendency to roll inward while walking or running. In this situation, the entire surface of the arch comes into contact with the ground, thereby losing the normal curvature of the arch.
This lack of support for the plantar arch can lead to biomechanical imbalances. Overpronation can put excessive pressure on parts of the foot, affect joint stability, and contribute to problems such as knee disease, hip pain, and other posture-related complications.
It is important to recognize normal variations in foot structure while being aware of the signs of overpronation. People experiencing symptoms associated with overpronation, such as persistent pain, unsteady gait, or joint problems, should see a healthcare professional, such as a podiatrist, for a thorough evaluation. Preventative measures, such as wearing supportive shoes or using orthotic insoles, can often help alleviate the harmful effects of overpronation and improve foot stability.
How to test pronation or supination yourself
A simple method to determine the shape of your arch is to perform a wet print test. To do this, open a wrapping paper bag or place newspaper on the ground, securing it firmly. Next, remove your shoes and socks, and lightly moisten the soles of your feet.
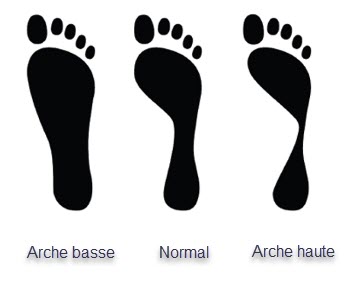
Then walk on the previously prepared paper. As you pass by, you will leave a characteristic wet imprint. By comparing this footprint to the standard drawings below, you will be able to determine the nature of your arch, whether it is high, medium or low.
This method of analyzing the footprint provides information on the structure of your foot. A high arch will result in an indentation where only the front of the foot and the heel are visible, with a thin strip connecting the two. An average arch will have a well-balanced footprint between the heel and the front of the foot. Finally, a low arch will be characterized by a wider footprint, with an extended connection between the heel and the front of the foot.
However, it is important to note that this test offers a general indication and does not replace a professional assessment. If you have specific concerns regarding your feet, it is recommended that you consult a healthcare professional, such as a podiatrist, for further analysis and personalized advice.

Conclusion
In conclusion, pronation, a natural movement of the foot, is crucial to the gait cycle by allowing an even distribution of forces across the foot. However, excessive pronation can lead to biomechanical imbalances, giving rise to various problems, such as pain in the feet, ankles, knees, hips, and even back. Foot pronation syndrome, characterized by pathological pronation, can cause musculoskeletal complications.
The mechanism of pronation syndrome involves internal rotation of the femur and tibia, inducing excessive forces and stresses that can lead to injuries and orthopedic disorders. Risk factors, such as individual biomechanics, heredity, weakened musculature, inappropriate footwear, intensive physical activities, age, obesity, pre-existing medical conditions, previous trauma, and walking surface , contribute to excessive pronation.
Inspection of the sole of a shoe and assessment of the arch of the foot provide visual clues to excessive pronation. Uneven sole wear and sagging of the midsection can be telltale signs. Additionally, simple tests, such as the wet print test, can give a general indication of the shape of the arch of the foot.
To prevent the harmful effects of excessive pronation, preventive and corrective measures, such as wearing appropriate shoes and using orthopedic insoles, are recommended. A professional assessment by a podiatrist or orthopedist will allow for an accurate diagnosis and treatment recommendations tailored to the individual situation. In summary, vigilance and appropriate interventions are essential to maintain the health and integrity of the kinetic chain in the context of foot pronation.
References
- Barnes A., Wheat J., Milner C. (2008). Association between foot type and tibial stress injuries: a systematic review. Br. J. Sports Med. 42 93–98. 10.1136/bjsm.2007.036533 [PubMed] [CrossRef] [Google Scholar]
- Bennett J. E., Reinking M. F., Pluemer B., Pentel A., Seaton M., Killian C. (2001). Factors contributing to the development of medial tibial stress syndrome in high school runners. J. Orthop. Sport Phys. Ther. 31 504–510. 10.2519/jospt.2001.31.9.504 [PubMed] [CrossRef] [Google Scholar]
- Bertelsen M. L., Hulme A., Petersen J., Brund R. K., Sørensen H., Finch C. F., et al. (2017). A framework for the etiology of running-related injuries. Scand. J. Med. Sci. Sport 27 1170–1180. 10.1111/sms.12883 [PubMed] [CrossRef] [Google Scholar]
- Bonacci J., Saunders P. U., Hicks A., Rantalainen T., Vicenzino B. G. T., Spratford W. (2013). Running in a minimalist and lightweight shoe is not the same as running barefoot: a biomechanical study. Br. J. Sports Med. 47 387–392. 10.1136/bjsports-2012-091837 [PubMed] [CrossRef] [Google Scholar]
- Bowser B. J., Fellin R., Milner C. E., Pohl M. B., Davis I. S. (2018). Reducing impact loading in runners. Med. Sci. Sport Exerc. 50 2500–2506. 10.1249/MSS.0000000000001710 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Brund R. B. K., Rasmussen S., Nielsen R. O., Kersting U. G., Laessoe U., Voigt M. (2017). Medial shoe-ground pressure and specific running injuries: A 1-year prospective cohort study. J. Sci. Med. Sport 20 1–5. 10.1016/j.jsams.2017.04.001 [PubMed] [CrossRef] [Google Scholar]
- Chan-Roper M., Hunter I., Myrer J. W., Eggett D. L., Seeley M. K. (2012). Kinematic changes during a marathon for fast and slow runners. J. Sport Sci. Med. 11 77–82. 10.1162/qjec.122.2.831 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Delp S. L., Anderson F. C., Arnold A. S., Loan P., Habib A., John C. T., et al. (2007). OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 54 1940–1950. 10.1109/TBME.2007.901024 [PubMed] [CrossRef] [Google Scholar]
- DeMers M. S., Pal S., Delp S. L. (2014). Changes in tibiofemoral forces due to variations in muscle activity during walking. J. Orthop. Res. 32 769–776. 10.1002/jor.22601 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Dugan S. A., Bhat K. P. (2005). Biomechanics and analysis of running gait. Phys. Med. Rehabil. Clin. N. Am. 16 603–621. 10.1016/j.pmr.2005.02.007 [PubMed] [CrossRef] [Google Scholar]
- Feng Y., Song Y. (2017). The Categories of AFO and its effect on patients with foot impair: a systemic review. Phys. Activ. Health 1 8–16. 10.5334/paah.3 [CrossRef] [Google Scholar]
- Fischer K. M., Willwacher S., Hamill J., Brüggemann G. P. (2017). Tibial rotation in running: does rearfoot adduction matter? Gait Posture 51 188–193. 10.1016/j.gaitpost.2016.10.015 [PubMed] [CrossRef] [Google Scholar]
- Fukano M., Inami T., Nakagawa K., Narita T., Iso S. (2018). Foot posture alteration and recovery following a full marathon run. Eur. J. Sport Sci. 18 1338–1345. 10.1080/17461391.2018.1499134 [PubMed] [CrossRef] [Google Scholar]
- Gerus P., Sartori M., Besier T. F., Fregly B. J., Delp S. L., Banks S. A., et al. (2013). Subject-specific knee joint geometry improves predictions of medial tibiofemoral contact forces. J. Biomech. 46 2778–2786. 10.1016/j.jbiomech.2013.09.005 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Giarmatzis G., Jonkers I., Wesseling M., Rossom S., Van Verschueren S. (2015). Loading of hip measured by hip contact forces at different speeds of walking and running. J. Bone Miner. Res. 30 1431–1440. 10.1146/annurev-bioeng-070909-105259 [PubMed] [CrossRef] [Google Scholar]









{kind=link}