



Introduction
The Q angle, also known as the quadriceps angle, is a critical biomechanical factor influencing knee health and function. It represents the angle formed between two lines: one drawn from the anterior superior iliac spine (ASIS) to the center of the patella, and another from the center of the patella to the tibial tuberosity. This angle offers insight into the alignment of the knee joint and the forces exerted on the patella during movement.
Understanding the Q angle is essential for both practitioners and individuals, as a larger Q angle can increase the risk of several musculoskeletal conditions, including patellar subluxation, patellofemoral pain syndrome, and anterior cruciate ligament (ACL) injuries. In both men and women, deviations from the normal Q angle may signal biomechanical imbalances that could predispose individuals to knee pain and dysfunction.
While the Q angle is present in both men and women, it tends to be larger in females, owing to differences in pelvic anatomy that develop during puberty. This larger Q angle is associated with a greater predisposition to knee injuries, particularly in women who engage in high-impact sports or activities that place a significant load on the knee joint. Understanding this distinction is vital for developing effective preventive strategies, as well as for treatment and rehabilitation in cases of injury.
The Q angle can provide valuable information regarding the alignment of the lower limbs and the distribution of forces through the knee joint. A normal Q angle in men is generally around 14 degrees, while in women, it tends to be around 17 degrees due to the wider pelvis. However, these values can vary depending on factors such as posture, muscle imbalances, and previous injuries. An increased Q angle can place more stress on the patella, leading to conditions such as patellar tracking disorders, where the patella deviates from its normal path during movement.
In addition to its relevance in injury prevention, the Q angle is a crucial factor in rehabilitation programs for those recovering from knee injuries. Correcting or compensating for an increased Q angle through strengthening exercises, stretching, and proper alignment can significantly reduce the risk of recurrence and improve long-term outcomes. For athletes, especially female athletes who are more prone to ACL injuries, paying attention to the Q angle and adopting strategies to maintain healthy knee biomechanics is essential for performance and injury prevention.
This article delves into the details of the Q angle, exploring its anatomical basis, biomechanical implications, and its significance in both injury development and prevention. We will also look at how this angle differs in men and women, why these differences exist, and what can be done to minimize the risk of damage from an increased Q angle.
Anatomy of the Q Angle
The Q angle, short for quadriceps angle, is a biomechanical measurement used to evaluate knee alignment and the forces acting on the knee joint, particularly on the patella. It is essential for understanding how the knee functions during movement and how imbalances can lead to injury. This section will explore the anatomical foundations of the Q angle, its significance in biomechanics, and how deviations from the normal range can impact knee health.
Defining the Q Angle
The Q angle is formed by the intersection of two lines. The first line extends from the anterior superior iliac spine (ASIS) of the pelvis to the center of the patella. This line represents the pull of the quadriceps muscle, which plays a critical role in knee extension and stabilization. The second line extends from the center of the patella to the tibial tuberosity, a bony prominence on the front of the tibia (shin bone) where the patellar tendon attaches. The angle formed by these two lines is the Q angle, and it serves as an indicator of the alignment between the pelvis, knee, and lower leg.

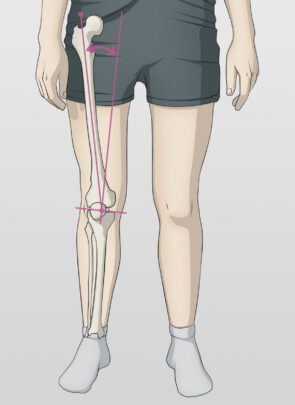
In a typical, healthy individual, the Q angle ranges from 14 to 17 degrees. For men, a normal Q angle is around 14 degrees, while for women, it is slightly larger, averaging around 17 degrees. The difference in Q angle between men and women is primarily due to anatomical variations, such as a wider pelvis in females, which affects the angle at which the quadriceps muscle pulls on the patella.
Key Landmarks in Measuring the Q Angle
To measure the Q angle, three key anatomical landmarks must be considered:
- Anterior Superior Iliac Spine (ASIS): This is the bony prominence at the front of the pelvis, which serves as the origin point for the first line of the Q angle. The ASIS is an important reference in biomechanics, as it reflects the alignment of the pelvis and the pull of the quadriceps muscle.
- Center of the Patella: The patella, or kneecap, is a sesamoid bone that sits within the quadriceps tendon and articulates with the femur. Its position is crucial in knee movement, as it helps distribute forces and protects the knee joint. The center of the patella is the point where the two lines of the Q angle intersect.
- Tibial Tuberosity: This is the attachment site for the patellar tendon on the tibia. The second line of the Q angle runs from the center of the patella to this point. The tibial tuberosity’s position indicates the alignment of the lower leg in relation to the knee.
The Q angle provides insight into the alignment and functioning of the lower limb. A smaller or larger Q angle can indicate potential imbalances that may predispose an individual to knee injuries, such as patellar maltracking, where the patella does not move smoothly in its groove during knee flexion and extension.
The Role of the Q Angle in Biomechanics
The Q angle influences how forces are distributed across the knee joint, particularly on the patella. A larger Q angle creates more lateral pull on the patella, which can increase the risk of patellar dislocation or subluxation. This lateral pull can also lead to conditions like patellofemoral pain syndrome, where the cartilage on the underside of the patella wears down due to abnormal stress.
Conversely, a smaller Q angle can reduce the lateral forces on the patella but may also lead to other biomechanical issues, such as improper alignment of the knee joint during movement. For example, a reduced Q angle may contribute to a higher risk of medial (inner) knee injuries or issues with knee stability.
How Deviations from Normal Affect Knee Health
Deviations from the normal Q angle range can have significant implications for knee health. An increased Q angle, common in women, is associated with a higher risk of knee injuries, particularly those related to the patella. Women with a larger Q angle are more susceptible to patellar subluxation, where the patella partially dislocates from its normal position. This condition can cause pain, instability, and an increased risk of recurrent knee injuries.
An increased Q angle is also linked to a higher incidence of anterior cruciate ligament (ACL) injuries. The ACL is one of the major ligaments in the knee that stabilizes the joint, and its integrity is crucial for activities that involve cutting, pivoting, or jumping. A larger Q angle can place more stress on the ACL, making it more prone to tearing, particularly in female athletes.
In contrast, a reduced Q angle, while less common, can also present challenges. It may lead to abnormal alignment of the knee joint, increasing the risk of medial knee pain or degenerative conditions like osteoarthritis. Proper alignment and muscle balance are critical in maintaining knee health, and any deviation from the normal Q angle can disrupt these factors.
Biomechanical Differences in Women
Biomechanical differences between men and women have profound effects on the function and alignment of the knee joint, particularly through the influence of the Q angle. These anatomical and physiological variations often result in women having a wider Q angle, which predisposes them to specific knee-related issues. Understanding these differences is crucial for both prevention and treatment, as they can significantly affect performance in sports, daily activities, and the risk of injury.
Influence of Pelvic Anatomy on the Q Angle
One of the primary reasons for the difference in Q angle between men and women is the structure of the pelvis. Women naturally have a wider pelvis, a feature that develops during puberty to accommodate childbirth. This wider pelvis affects the alignment of the femur (thigh bone) in relation to the knee. As the femur angles inward to align with the knee, the Q angle increases. While a typical Q angle in men is around 14 degrees, in women it averages around 17 degrees, though this can vary depending on individual anatomy.
This increase in the Q angle can lead to a number of biomechanical changes that place more stress on the knee joint. One of the most notable is the lateral (outward) pull on the patella, or kneecap, which increases the risk of patellar subluxation (partial dislocation) or dislocation. In women with a significantly higher Q angle, the patella may not track properly within the femoral groove, resulting in pain, instability, and a higher likelihood of injury.
The increased Q angle in women also predisposes them to other knee issues, including patellofemoral pain syndrome (PFPS), which is characterized by pain around or behind the kneecap. This condition is particularly common in female athletes and those who engage in activities that involve running, jumping, or squatting. The combination of a wider pelvis and an increased Q angle alters the mechanics of how the knee absorbs and distributes forces, making women more vulnerable to such injuries.
The Impact of Hormonal Differences
Hormonal differences between men and women further exacerbate the biomechanical challenges associated with a higher Q angle. The hormone relaxin, which is present in higher levels during pregnancy but also in lower levels throughout the menstrual cycle, affects the laxity of ligaments and connective tissues. This increased laxity can reduce joint stability, particularly in the knees, where the alignment is already compromised by the wider Q angle.
During certain phases of the menstrual cycle, hormonal fluctuations may increase the risk of injury due to decreased joint stability. This is especially relevant in sports that require quick changes in direction, jumping, or pivoting, as these movements place significant stress on the knee ligaments, including the anterior cruciate ligament (ACL). Studies have shown that women are more likely to suffer ACL injuries than men, and the combination of a wider Q angle, hormonal influences, and decreased joint stability plays a significant role in this increased risk.
Common Biomechanical Tendencies in Women
The wider pelvis and increased Q angle in women often lead to a series of compensatory postural changes that affect the entire kinetic chain, from the hips down to the feet. These biomechanical tendencies include:
- Cervical and Lumbar Hyperlordosis: The natural curvature of the spine tends to be more pronounced in women, particularly in the cervical (neck) and lumbar (lower back) regions. Hyperlordosis, or an exaggerated inward curve, can shift the body’s center of gravity, affecting knee alignment and increasing the strain on the knee joint during movement.
- Dorsal Hyperkyphosis: This refers to an excessive outward curvature of the upper back, which often occurs in combination with lumbar hyperlordosis. Dorsal hyperkyphosis can alter posture and gait, further contributing to misalignment in the lower limbs and increasing the risk of knee pain or injury.
- Anterior Pelvic Tilt: Women often exhibit an anterior pelvic tilt, where the pelvis is tilted forward. This posture shifts the body’s weight toward the front of the knee, placing additional strain on the quadriceps muscles and increasing the load on the patella. Over time, this can exacerbate issues related to the Q angle, leading to patellofemoral pain or other knee disorders.
- Genu Valgum (Knock-Knees): Genu valgum is a condition where the knees angle inward and touch when the legs are straightened. This is more common in women and is directly related to the increased Q angle. Genu valgum places abnormal stress on the medial (inner) side of the knee joint, increasing the risk of cartilage damage, meniscal tears, and osteoarthritis.
- Femoral Internal Rotation: As a result of the wider pelvis, women are more likely to exhibit internal rotation of the femur. This inward rotation shifts the alignment of the knee and lower leg, contributing to poor patellar tracking and increasing the risk of knee pain.
- External Rotation of the Tibia: To compensate for the inward rotation of the femur, women may also display external rotation of the tibia (shin bone). This misalignment can place undue stress on the knee joint and increase the likelihood of developing knee pain, particularly in the patellofemoral region.
- Hyperpronation of the Foot: Hyperpronation, or excessive inward rolling of the foot during walking or running, is more common in women due to the biomechanical chain initiated by the increased Q angle. Hyperpronation can exacerbate knee pain by altering the alignment and function of the lower limbs.
Addressing Biomechanical Imbalances
Understanding these biomechanical tendencies is crucial for preventing and managing knee injuries in women. Strengthening key muscle groups, particularly the hip abductors, quadriceps, and hamstrings, can help improve alignment and reduce the strain on the knee joint. Additionally, proper footwear, orthotics, and targeted stretching exercises can help correct issues such as hyperpronation and improve overall knee function.
Conditions Associated with an Increased Q Angle
An increased Q angle significantly affects the biomechanics of the knee joint, particularly the patellofemoral region. When the Q angle deviates from the normal range, it can lead to several musculoskeletal issues, primarily centered around the misalignment of the patella and the abnormal distribution of forces through the knee joint. This section will explore the various conditions associated with an increased Q angle, emphasizing how these conditions arise and the role of proper knee alignment in preventing them.
Patellofemoral Pain Syndrome (PFPS)
Patellofemoral pain syndrome, often referred to as “runner’s knee,” is one of the most common conditions associated with an increased Q angle. The patella (kneecap) sits within the patellar groove of the femur, and during movement—especially activities involving knee flexion such as running, squatting, or climbing—the patella should glide smoothly within this groove. However, when the Q angle is increased, there is a greater lateral pull on the patella, causing it to deviate from its normal path.
This lateral misalignment of the patella creates abnormal stress on the cartilage beneath the kneecap, leading to pain and inflammation in the anterior knee. Individuals with PFPS often report pain when sitting for prolonged periods (known as “theater sign”), climbing stairs, or engaging in activities that involve knee flexion and extension.
PFPS is particularly prevalent in women due to their naturally larger Q angle. In women, the wider pelvis and subsequent increase in Q angle exacerbate the lateral pull on the patella, making proper patellar tracking more difficult. Over time, if left untreated, PFPS can lead to more severe issues, including cartilage degradation and chronic knee pain.
Patellar Subluxation and Dislocation
An increased Q angle not only predisposes individuals to patellofemoral pain but also increases the risk of patellar subluxation or dislocation. Patellar subluxation refers to the partial displacement of the kneecap from its groove, while patellar dislocation occurs when the kneecap is completely dislocated from its normal position. Both conditions result in knee instability, pain, and, in the case of dislocation, a visibly displaced kneecap.
The lateral pull caused by a larger Q angle contributes directly to patellar subluxation. As the Q angle increases, the patella is subjected to greater forces pulling it laterally, which can cause it to “pop out” of its groove during movement. Patellar dislocation is often associated with trauma, such as a sudden twisting motion or a direct blow to the knee, but individuals with an increased Q angle are more susceptible to this condition due to the weakened alignment of the joint.
Both subluxation and dislocation can lead to significant pain, swelling, and long-term instability of the knee. Rehabilitation often involves strengthening the quadriceps, particularly the vastus medialis obliquus (VMO), to improve patellar tracking and reduce the risk of recurrence. In more severe cases, surgery may be required to realign the patella or repair damaged ligaments.
Anterior Cruciate Ligament (ACL) Injuries
ACL injuries are another common consequence of an increased Q angle, particularly in women. The ACL is one of the major stabilizing ligaments in the knee, preventing the tibia from sliding out in front of the femur and providing rotational stability. However, when the Q angle is larger, as is often the case in women, it alters the biomechanics of the knee, placing greater stress on the ACL during activities that involve pivoting, jumping, or rapid changes in direction.
Studies have shown that women are significantly more likely to suffer ACL injuries than men, with some estimates suggesting they are up to 8 times more likely to experience this type of injury. The combination of a wider pelvis, increased Q angle, and hormonal factors (such as ligament laxity influenced by estrogen) contribute to this heightened risk. ACL injuries often occur during sports like basketball, soccer, and skiing, where the knee is subjected to sudden directional changes or deceleration forces.
In addition to an increased Q angle, weak or imbalanced muscles, particularly in the hips and thighs, can exacerbate the risk of ACL injuries. Strengthening the surrounding musculature, particularly the hamstrings and quadriceps, is crucial for stabilizing the knee and reducing the risk of ligament damage.
Plantar Fasciitis
While plantar fasciitis is a condition typically associated with foot biomechanics, an increased Q angle can indirectly contribute to its development. When the Q angle is larger, it affects the alignment and function of the entire lower kinetic chain, including the foot. Individuals with a larger Q angle often display compensatory patterns, such as hyperpronation (excessive inward rolling of the foot), which places additional strain on the plantar fascia, the thick band of tissue that runs along the bottom of the foot.
Over time, the increased strain on the plantar fascia can lead to inflammation, microtears, and chronic pain in the heel or arch of the foot. This condition is particularly common in individuals who engage in activities that involve prolonged standing, walking, or running, especially on hard surfaces. In women, the combination of a wider Q angle, hyperpronation, and poor footwear choices (such as high heels) can exacerbate the risk of developing plantar fasciitis.
Genu Valgum (Knock Knees)
Genu valgum, commonly known as “knock knees,” is a condition where the knees angle inward and touch each other while the feet remain apart. This alignment issue is often linked to an increased Q angle, as the wider pelvis in women predisposes them to this condition. Genu valgum places abnormal stress on both the medial (inner) and lateral (outer) aspects of the knee, which can accelerate the wear and tear of cartilage and increase the risk of degenerative joint diseases like osteoarthritis.
In individuals with genu valgum, the altered alignment can lead to a range of knee problems, including patellofemoral pain, meniscal tears, and ligament instability. The increased Q angle contributes to this misalignment, and addressing the underlying biomechanical issues through strengthening exercises, orthotics, and proper footwear can help prevent further damage.
Postural and Biomechanical Factors
Posture and biomechanics play a crucial role in determining the alignment of the body, particularly the knees, hips, and lower back. When the Q angle of the knee is increased, it can have widespread effects on the rest of the body’s posture and movement patterns. These biomechanical factors often lead to compensatory changes in posture, which can exacerbate musculoskeletal issues and increase the risk of injury. This section will explore how postural and biomechanical factors interact with the Q angle and contribute to the development of pain and dysfunction in the body.
Cervical and Lumbar Hyperlordosis
Hyperlordosis refers to an exaggerated inward curve of the spine, most commonly seen in the cervical (neck) and lumbar (lower back) regions. In women, cervical and lumbar hyperlordosis are often more pronounced due to the structural differences in pelvic alignment and wider Q angle. The relationship between the spine and lower body alignment is crucial in understanding how the Q angle can influence overall posture.
Lumbar hyperlordosis, for instance, shifts the body’s center of gravity forward, which places added stress on the lower limbs, particularly the knees. This anterior shift increases the load on the quadriceps, further pulling on the patella and aggravating issues related to an increased Q angle, such as patellofemoral pain and patellar tracking disorders. When the lower back curves excessively inward, it changes the way forces are transmitted through the body, altering the alignment of the pelvis, hips, and knees.
Cervical hyperlordosis, though less directly related to knee function, can also have indirect effects. Poor neck posture often leads to compensatory changes in the thoracic and lumbar spine, further disrupting the alignment of the lower limbs. These postural imbalances can increase the strain on the lower body, contributing to knee pain and injury.
Dorsal Hyperkyphosis
Dorsal hyperkyphosis, also known as an exaggerated outward curvature of the upper back (thoracic spine), is another common postural issue that affects individuals with an increased Q angle. Hyperkyphosis often develops as a compensation for lumbar hyperlordosis, as the body tries to balance the excessive curvature of the lower back by curving the upper back in the opposite direction.
This postural imbalance can further shift the body’s center of gravity, causing the pelvis to tilt anteriorly (forward) and placing even more strain on the knees. Dorsal hyperkyphosis is often associated with a “hunched” posture, where the shoulders round forward, and the head juts out. This forward shift of the upper body alters the biomechanics of walking and running, leading to abnormal loading on the knees and increasing the likelihood of knee pain, particularly in those with a larger Q angle.
In addition to its effects on knee biomechanics, dorsal hyperkyphosis can also lead to compensatory changes in the lower back, hips, and feet, exacerbating issues related to lower limb alignment. The combination of lumbar hyperlordosis, dorsal hyperkyphosis, and an increased Q angle creates a biomechanical chain that places undue stress on the knee joints, often leading to chronic pain and dysfunction.
Anterior Pelvic Tilt
The anterior pelvic tilt is a common postural issue that occurs when the pelvis tilts forward, causing the lower back to arch excessively. This posture is often associated with an increased Q angle, particularly in women, due to the wider pelvis and the subsequent inward angling of the femur (thigh bone). When the pelvis tilts forward, it alters the alignment of the hips, knees, and ankles, placing greater stress on the knee joint.
In individuals with an anterior pelvic tilt, the quadriceps muscles become overactive, while the hamstrings and gluteal muscles are often weak or underactive. This muscle imbalance increases the pull on the patella, contributing to patellar tracking issues and exacerbating the effects of an increased Q angle. The excessive anterior tilt of the pelvis also shifts the body’s weight forward, increasing the load on the knees during activities such as walking, running, or standing for prolonged periods.
Anterior pelvic tilt can also lead to lower back pain, as the exaggerated lumbar curve compresses the vertebrae and places additional strain on the lower spine. This condition is commonly seen in individuals with poor posture or those who spend extended periods sitting, as prolonged sitting often weakens the muscles responsible for stabilizing the pelvis and lower back.
Genu Valgum (Knock Knees)
Genu valgum, or knock knees, is a condition in which the knees angle inward and touch each other when the legs are straightened. This postural misalignment is often seen in individuals with a larger Q angle, as the inward angling of the femur leads to an abnormal alignment of the knees. Genu valgum places significant stress on both the medial (inner) and lateral (outer) aspects of the knee joint, increasing the risk of injuries such as meniscal tears, cartilage damage, and osteoarthritis.
In individuals with knock knees, the abnormal alignment can also affect the function of the ankles and feet, leading to issues such as hyperpronation (excessive inward rolling of the foot) and plantar fasciitis. The increased Q angle contributes to this misalignment, and addressing the underlying biomechanical issues through strengthening exercises, orthotics, and proper footwear can help reduce the risk of further damage.
Femoral Internal Rotation and Tibial External Rotation
Femoral internal rotation and tibial external rotation are two compensatory movements often seen in individuals with an increased Q angle. When the femur rotates inward (toward the midline of the body), it alters the alignment of the knee and contributes to patellar tracking issues. This inward rotation of the femur is common in individuals with a wider pelvis, as seen in women, and it can lead to an increased risk of patellofemoral pain and knee instability.
Tibial external rotation, on the other hand, occurs when the tibia (shin bone) rotates outward. This rotation is often a compensation for the inward rotation of the femur and can further exacerbate knee misalignment. When the tibia is externally rotated, it places additional stress on the knee joint, particularly on the lateral side, increasing the risk of injury and dysfunction.
These rotational imbalances can also affect the alignment and function of the hip and ankle joints, leading to a chain of compensatory movements that increase the likelihood of pain and injury. Correcting these rotational imbalances through targeted strengthening and stretching exercises can help improve knee alignment and reduce the risk of injury.
Hyperpronation of the Foot
Hyperpronation, or excessive inward rolling of the foot during walking or running, is a common compensatory mechanism in individuals with an increased Q angle. The misalignment of the knee joint caused by the larger Q angle affects the biomechanics of the entire lower limb, including the foot. When the foot rolls inward excessively, it places additional stress on the knee joint, particularly on the medial side.
Hyperpronation can lead to a variety of lower limb issues, including plantar fasciitis, shin splints, and knee pain. In individuals with an increased Q angle, addressing hyperpronation is essential for improving knee alignment and reducing the risk of injury. This can be achieved through the use of orthotics, proper footwear, and exercises that strengthen the muscles of the foot and lower leg.
Preventing Knee Damage
Preventing knee damage, particularly in individuals with an increased Q angle, requires a multifaceted approach that includes proper alignment, strength training, flexibility, and maintaining a healthy weight. The Q angle, by itself, can predispose individuals to a variety of knee injuries, but proactive measures can minimize the risk of long-term damage. This section will cover strategies to prevent knee damage, with a focus on postural alignment, muscle conditioning, and lifestyle modifications.
Maintaining a Healthy Weight
One of the most effective ways to reduce the risk of knee damage is by maintaining a healthy weight. Excess body weight increases the load on the knees, placing additional strain on the patella and other knee structures. For every pound of extra weight, there is a fourfold increase in the force exerted on the knee during walking or running. This added stress can exacerbate issues related to an increased Q angle, such as patellofemoral pain syndrome and patellar subluxation.
In individuals with an increased Q angle, managing weight is particularly important as the lateral pull on the patella is already heightened. Maintaining a healthy weight can reduce the strain on the quadriceps and patellar tendon, minimizing the risk of overloading the knee joint.
Adopting Proper Posture
Proper posture is critical for minimizing knee damage, especially in individuals with postural imbalances such as anterior pelvic tilt or lumbar hyperlordosis. By addressing these issues, individuals can realign the lower limbs, reduce the strain on the knees, and prevent excessive lateral forces on the patella.
For example, correcting anterior pelvic tilt by strengthening the gluteal and abdominal muscles can reduce the forward pull on the pelvis, alleviating the strain on the knees. Similarly, improving spinal posture can redistribute weight more evenly across the lower body, reducing stress on the knees and improving overall alignment.
Avoiding High Heels
High heels can significantly exacerbate the problems associated with an increased Q angle. Wearing high heels shifts the body’s weight forward, increasing the load on the front of the knees and heightening the risk of patellofemoral pain and knee instability. In addition, high heels can alter the biomechanics of the lower limb, increasing the strain on the quadriceps and patellar tendon.
For individuals with a larger Q angle, it is especially important to wear supportive, flat shoes or shoes with minimal heels. These types of footwear help to maintain proper alignment of the lower limbs and reduce the risk of knee pain.
Strengthening the Abdominal and Hamstring Muscles
Strengthening the muscles around the knee joint, particularly the hamstrings and abdominal muscles, is essential for maintaining proper alignment and reducing the strain on the knee. The hamstrings play a critical role in stabilizing the knee by balancing the forces exerted by the quadriceps. Strengthening these muscles can help to counteract the lateral pull caused by an increased Q angle, reducing the risk of patellar subluxation or dislocation.
In addition to the hamstrings, the abdominal muscles are essential for stabilizing the pelvis and spine, which in turn influences the alignment of the lower limbs. A strong core can help maintain proper posture, reducing the risk of anterior pelvic tilt and lumbar hyperlordosis, both of which contribute to knee pain.
Stretching the Quadriceps and Gluteal Muscles
Flexibility is another critical factor in preventing knee damage. Tight quadriceps and gluteal muscles can pull on the patella, increasing the strain on the knee joint and exacerbating issues related to an increased Q angle. Regular stretching of these muscle groups can improve flexibility, reduce tension on the patella, and prevent imbalances in the lower limb.
Stretching should be incorporated into any fitness routine, particularly for individuals with an increased Q angle. Dynamic stretches before activity and static stretches after activity can help maintain muscle flexibility and reduce the risk of knee injuries.
Maintaining Physical Fitness During Pregnancy
Pregnancy can increase the Q angle as the pelvis widens to accommodate childbirth. This widening, combined with weight gain, can place additional strain on the knees, increasing the risk of patellofemoral pain and knee instability. Maintaining physical fitness during pregnancy is essential for minimizing these risks.
Exercises that strengthen the quadriceps, hamstrings, and core muscles are particularly important for pregnant women, as these muscle groups help stabilize the pelvis and knee joint. Low-impact activities, such as swimming or walking, are also beneficial for maintaining joint health and reducing the strain on the knees during pregnancy.
Exercises to Strengthen the Vastus Medialis
The vastus medialis obliquus (VMO) is a key muscle in the quadriceps group responsible for stabilizing the patella and ensuring proper knee alignment. Strengthening the VMO is particularly important for individuals with an increased Q angle, as it helps to counteract the lateral pull on the patella and improves patellar tracking. In this section, we will explore specific exercises designed to strengthen the vastus medialis and enhance knee stability.
Knee Extension with Lateral Foot Deviation
One of the most effective exercises for targeting the vastus medialis is the knee extension with lateral foot deviation. This exercise helps isolate the VMO by emphasizing the medial side of the quadriceps, where the vastus medialis is located. Here’s how to perform it:
- Starting Position: Sit on the floor or a bench with your back straight and one leg extended in front of you. Place the other leg in a bent position with the foot flat on the ground.
- Foot Positioning: Rotate the foot of the extended leg slightly outward. This lateral foot deviation emphasizes the medial portion of the quadriceps, including the vastus medialis.
- Execution: Slowly lift the extended leg off the ground, keeping the foot rotated outward. Hold the leg in this position for 5 to 10 seconds, then lower it back down.
- Repetitions: Perform 5 to 10 repetitions before switching to the other leg.
This exercise strengthens the vastus medialis and helps improve knee stability by correcting patellar tracking. It is particularly beneficial for individuals with an increased Q angle, as it reduces the lateral pull on the patella.
Terminal Knee Extensions (TKEs)
Terminal knee extensions are another effective exercise for strengthening the vastus medialis and improving knee alignment. This exercise can be performed with a resistance band to provide additional resistance:
- Starting Position: Secure a resistance band around a sturdy object and loop the other end around the back of your knee. Stand facing away from the anchor point with the band taut.
- Execution: Slowly extend your knee, pushing against the resistance of the band. As you straighten your leg, focus on contracting the vastus medialis to control the movement.
- Repetitions: Perform 10 to 15 repetitions on each leg.
TKEs help strengthen the muscles responsible for knee extension, particularly the vastus medialis, and improve knee stability. This exercise is ideal for individuals recovering from patellofemoral pain syndrome or patellar subluxation.
Step-Ups
Step-ups are a functional exercise that targets the quadriceps and improves overall knee strength. By focusing on the upward motion, step-ups engage the vastus medialis and help stabilize the knee during weight-bearing activities:
- Starting Position: Stand in front of a step or bench with one foot placed on the step.
- Execution: Push through the foot on the step to lift your body up, straightening the leg fully at the top. Focus on engaging the vastus medialis during the upward motion.
- Repetitions: Perform 10 to 15 repetitions on each leg.
Step-ups are a versatile exercise that can be modified with added weights or higher steps to increase intensity. They are particularly effective for improving knee strength and stability in individuals with an increased Q angle.
Wall Sits with Squeeze
Wall sits are an excellent isometric exercise for strengthening the quadriceps, and by adding a squeeze (e.g., placing a ball between the knees), you can specifically target the vastus medialis:
- Starting Position: Stand with your back against a wall and your feet about shoulder-width apart. Place a small ball or rolled-up towel between your knees.
- Execution: Slide down the wall until your thighs are parallel to the floor, as if sitting in an invisible chair. Squeeze the ball or towel between your knees to engage the vastus medialis. Hold this position for 20 to 30 seconds.
- Repetitions: Perform 3 to 5 repetitions.
Wall sits with a squeeze help strengthen the vastus medialis and improve knee stability by training the muscles in an isometric hold. This exercise is particularly beneficial for individuals with patellar tracking issues.
Squats with Focus on VMO Activation
Traditional squats can be modified to place greater emphasis on the vastus medialis by adjusting foot positioning and focusing on VMO activation:
- Starting Position: Stand with your feet shoulder-width apart and your toes slightly turned out.
- Execution: Slowly lower yourself into a squat position, keeping your knees aligned with your toes. Focus on contracting the vastus medialis as you rise back to the starting position
- Repetitions: Perform 10 to 15 repetitions.
Squats are a fundamental exercise for overall lower body strength, and by emphasizing VMO activation, they can improve knee stability and prevent issues related to an increased Q angle.
Conclusion
Understanding the Q angle and its implications for knee health is essential for both clinicians and individuals looking to prevent injury and maintain optimal biomechanics. The Q angle provides insight into the alignment of the knee joint and the forces acting upon it during movement. When the Q angle deviates from the norm—especially in individuals with a larger Q angle, such as women—it can lead to various musculoskeletal issues, including patellofemoral pain syndrome, patellar subluxation, and even more serious injuries like ACL tears.
Key anatomical and biomechanical factors, including the natural widening of the pelvis in women and the subsequent increase in the Q angle, can predispose individuals to these conditions. By understanding the mechanics of the Q angle and the effects of postural and muscular imbalances, individuals can take proactive steps to protect their knee health.
Preventing knee damage involves a multifaceted approach that includes maintaining a healthy weight, adopting proper posture, avoiding high heels, and incorporating targeted exercises to strengthen the vastus medialis and other key muscle groups. These strategies can help counteract the negative effects of an increased Q angle, ensuring proper knee alignment and minimizing the risk of injury.
Exercises such as knee extensions with lateral foot deviation, step-ups, and wall sits with a squeeze are particularly beneficial for strengthening the vastus medialis obliquus (VMO), which plays a crucial role in stabilizing the patella and preventing issues such as patellar tracking disorder. Additionally, addressing postural problems such as lumbar hyperlordosis, anterior pelvic tilt, and hyperpronation of the feet can further reduce the strain on the knee joint and improve overall biomechanics.
References
- Emami, M.J., Ghahramani, M.H., Abdinejad, F., & Namazi, H. (2007). “Q-angle: An invaluable parameter for evaluation of anterior knee pain.” Archives of Iranian Medicine, 10(1), 24-26.
- This study discusses the role of the Q angle in anterior knee pain and its relevance in clinical evaluation.
- Herrington, L., & Nester, C. (2004). “Q-angle undervalued? The relationship between Q-angle and its components.” Clinical Biomechanics, 19(8), 867-871.
- This article examines the Q angle and its components, providing insights into its significance in knee biomechanics.
- Fisher, R.L., & Canales, M.B. (2020). “Q-angle measurement: Reliability and validity in diagnosing patellofemoral pain syndrome.” Journal of Orthopaedic Research, 38(6), 1341-1346.
- This research focuses on the reliability of Q angle measurements in diagnosing patellofemoral pain syndrome.
- Woodland, L.H., & Francis, R.S. (1992). “Parameters and comparisons of the quadriceps angle in teenage males and females.” Clinical Orthopaedics and Related Research, 279, 179-183.
- A comparative study highlighting the differences in Q angle between males and females, particularly during adolescence.
- Myer, G.D., Ford, K.R., & Hewett, T.E. (2004). “Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes.” Journal of Athletic Training, 39(4), 352-364.
- This paper discusses ACL injury prevention strategies in female athletes, emphasizing the role of Q angle and biomechanics.
- Barton, C.J., Menz, H.B., Crossley, K.M. (2011). “The relationship between Q-angle and lower limb kinematics during gait.” Gait & Posture, 34(3), 370-374.
- A study on how the Q angle affects lower limb kinematics during movement, with implications for gait analysis and injury risk.
- Livingston, L.A., & Mandigo, J.L. (1999). “Bilateral Q angle asymmetry and anterior knee pain syndrome.” Clinical Biomechanics, 14(1), 7-13.
- This research explores the relationship between Q angle asymmetry and anterior knee pain syndrome.
- Smith, T.O., Hunt, N.J., & Donell, S.T. (2008). “The reliability and validity of the Q-angle: A systematic review.” Knee Surgery, Sports Traumatology, Arthroscopy, 16(12), 1068-1079.
- A systematic review assessing the validity and reliability of the Q angle as a clinical measurement.
- Post, W.R. (1999). “Patellofemoral pain: What does it really mean?” Sports Medicine and Arthroscopy Review, 7(2), 75-83.
- A comprehensive review of patellofemoral pain syndrome, with a focus on the biomechanical role of the Q angle.
- Powers, C.M. (2010). “The influence of abnormal hip mechanics on knee injury: A biomechanical perspective.” Journal of Orthopaedic & Sports Physical Therapy, 40(2), 42-51.


 Weakness: Causes, Implications, and Solutions")





{kind=link}