



Sacroiliac syndrome, also called sacroiliac dysfunction (SID), refers to a condition in which there is joint dysfunction or instability at the sacroiliac (SI) joint, which is located between the the sacrum bone and the ilium (pelvic bone).
Introduction
Sacroiliac syndrome (SSI) is a condition characterized by pain in the region of the sacroiliac (SI) joint, which is located between the sacrum (the triangular bone at the base of the spine) and the ilium (the pelvic bone). This joint has an important role in transmitting weight from the lower trunk to the lower limbs.
Bernard Albinus (1697-1770)

Bernard Albinus (1697-1770): A renowned Dutch anatomist, Albinus did significant work in the field of anatomy in the 18th century, including studies on the sacroiliac joint.
Albinus is famous for his anatomical atlas “Tabulae Sceleti et Musculorum Corporis Humani” (1747), which has become an essential reference work in the field of human anatomy. In this and other publications, Albinus described in detail the structure and anatomical relationships of many parts of the human body, including the sacroiliac joint.
Through his meticulous dissections and precise illustrations, Albinus contributed to a better understanding of the anatomy of the sacroiliac joint, highlighting its ligaments, joint surfaces and anatomical variations. His work was widely used by medical students and anatomists of the time, and continued to be a source of inspiration for researchers in subsequent centuries.
In addition to his work in anatomy, Albinus was also a renowned educator, teaching at the University of Leiden in the Netherlands. His innovative teaching methods and contributions to anatomical research have left a lasting legacy in the field of medicine and anatomy.
Giovanni Battista Morgagni (1682-1771)
Giovanni Battista Morgagni (1682-1771): Morgagni, an eminent Italian anatomist, is indeed considered one of the fathers of pathological anatomy. His contributions to medicine were broad, and his studies included various aspects of human anatomy, including the sacroiliac joint, in the 18th century.

Morgagni is famous for his monumental work “De Sedibus et Causis Morborum per Anatomen Indagatis” (On the Seats and Causes of Diseases, Researched Through Anatomy), published in 1761. In this work, Morgagni examined more than 600 autopsies and established correlations between the anatomical lesions observed and the clinical symptoms of patients of his time. This revolutionary approach laid the foundation for modern pathological anatomy.
Although Morgagni’s main focus was on pathological anatomy, his observations also covered various aspects of normal anatomy, including the sacroiliac joint. His precise dissections and detailed descriptions have contributed to a better understanding of the structure and function of this joint, as well as its anatomical variations and associated pathologies.
Morgagni’s work has been widely recognized for its precision and methodological rigor. His scientific approach significantly influenced the development of medicine and anatomy, laying the foundation for evidence-based medicine and modern pathological anatomy.
Domenico Felice Antonio Cotugno (1736-1822)
He was one of the first anatomists to study the anatomy of the sacroiliac joint in the 18th century.
Cotugno, an Italian physician and anatomist, is best known for his contributions to neuroanatomy and forensic medicine, but he also made significant contributions to the understanding of the general anatomy of the human body, including that of the sacro joint. -iliac.


At a time when anatomy techniques were rudimentary and knowledge limited, Cotugno undertook careful dissections to explore the structures of the sacroiliac joint. His observations documented the anatomical features of this complex joint, laying the foundation for our modern understanding of its structure and function.
Although the dissection methods and observational tools of the time did not allow for analyzes as detailed as those carried out today, Cotugno’s work nevertheless helped lay the foundation for future research into the sacroiliac joint. His observations were valuable to anatomists and physicians of his day, providing essential information about the structure and function of this crucial joint.
By recognizing the importance of the sacroiliac joint and documenting its anatomical features in a systematic manner, Cotugno laid the foundation for subsequent anatomical and biomechanical studies of this joint. His work has helped inform the understanding of this complex structure, paving the way for future discoveries in the field of anatomy and orthopedic medicine.
Antoine Louis (1723-1792)
Antoine Louis (1723-1792): Famous French anatomist, Louis greatly contributed to the study of the anatomy of the sacroiliac joint during the 18th century.

Known for his groundbreaking work in anatomy, Antoine Louis played a central role in the advancement of medical science of his time. Among his many contributions, his study of the sacroiliac joint was particularly significant.
As a renowned anatomist, Louis performed extensive dissections to explore the structures of the sacroiliac joint. His detailed observations made it possible to identify the ligaments, joint surfaces and anatomical variations of this essential joint of the pelvis.
Antoine Louis’s work was characterized by its precision and methodological rigor, thereby establishing new standards for descriptive anatomy. His detailed anatomical descriptions of the sacroiliac joint enriched the medical literature of the time and provided a solid basis for subsequent research in this area.
In addition to his contributions to anatomy, Antoine Louis was also an influential educator, training many medical students in anatomy and surgery. His influence extended far beyond his time, his work continuing to inspire and guide anatomists and surgeons in their exploration of human anatomy.
Thus, thanks to the research of Antoine Louis, the anatomy of the sacroiliac joint was documented with remarkable precision, laying the foundation for our modern understanding of this complex anatomical structure. His legacy lives on in the field of medical anatomy, testifying to his lasting contribution to science and medicine.
Jean Cruveilhier (1791-1874)
A French physician and anatomist, Cruveilhier was a prominent figure in the field of human anatomy in the 19th century. His research has encompassed various aspects of anatomy, including the study of the sacroiliac joint.


Cruveilhier was renowned for his precision and attention to detail in his anatomical dissections. His work on the sacroiliac joint has deepened our understanding of this complex structure of the pelvis. Through careful dissections, he identified ligaments, joint surfaces and anatomical variations of the joint, thereby helping to enrich the medical literature of his time.

In addition to his research on anatomy, Cruveilhier also published several anatomical works which became essential references for medical students and anatomists of the time. His work helped establish a solid foundation for modern anatomy and influenced many researchers and practitioners in the field of medicine.
Thanks to the contributions of Jean Cruveilhier, the sacroiliac joint has been studied with increased precision, which has provided a better understanding of its structure and functioning. His legacy lives on in the field of medical anatomy, testifying to his significant contribution to science and medicine.
François Magendie (1783-1855)
A renowned French physiologist, Magendie carried out pioneering work in neurology and physiology in the 19th century. Although he is not primarily known for his contributions to the anatomy or specific study of the sacroiliac joint, his research laid the foundation for understanding the nervous system and the physiological mechanisms underlying functions of the human body, including aspects of pain and mobility.
As a physiologist, Magendie contributed to a better understanding of nerve pathways and reflexes, as well as the mechanisms of pain and sensation. Although this work was not specifically focused on the sacroiliac joint, it provided a broader conceptual framework for understanding the neurological mechanisms involved in pain and movement perception, which are relevant to all joints of the body, including the sacroiliac joint.
Additionally, Magendie’s research laid the foundation for the experimental method in physiology, encouraging a more systematic and empirical approach to the study of biological processes. This laid the foundation for subsequent research that contributed to a better understanding of the anatomy and physiology of various parts of the body, including the sacroiliac joint.
Although Magendie is not directly associated with specific studies of the sacroiliac joint, his work has influenced the development of medical science as a whole, paving the way for new discoveries and advances in many fields, including understanding joints and how they work.
Charles Bell (1774-1842)
A prominent Scottish surgeon, Bell indeed made significant contributions to anatomy and physiology in the 19th century. Among his most important works are his studies of nerves and joints.


Bell is best known for his discoveries about the nervous system, particularly for his description of the functional difference between sensory and motor nerves, known as the “Bell-Magendie law”. His work laid the foundation for modern neurology and profoundly influenced our understanding of the peripheral nervous system.

Regarding joints, Bell also carried out important studies. He has contributed to the understanding of the anatomy and function of joints, including the sacroiliac joint. His detailed observations expanded our understanding of joint structure and physiology, laying the foundation for further research in this area.
As a distinguished surgeon and anatomist, Bell also shared his knowledge through teaching and writing. His works were widely used as references in medical schools and helped train many generations of doctors and surgeons.
William Jason Mixter
In 1905, William Jason Mixter made a significant advance in our understanding of back pain by highlighting the importance of the sacroiliac joint. His article published in the Journal of Bone and Joint Surgery marked a milestone by establishing a link between mechanical damage to this joint and lower back pain.


Mixter’s groundbreaking research represented a turning point in understanding the causes of back pain by highlighting the relevance of the sacroiliac joint. Before this publication, the specific links between dysfunctions of this joint and pain referred to the buttocks and the hind leg were unclear. Mixter’s observations and conclusions have helped broaden our perspective on back disorders.
The 1905 article was instrumental in recognizing the sacroiliac joint as a potential contributor to back pain and related pain. This advance has had significant repercussions in the medical field, directing future research into pelvic and lower back problems. Thus, the year 1905 remains a crucial milestone in the history of medicine, thanks to the light shed on the sacroiliac joint and its involvement in lower back pain.
Jean-Pierre Barral, DO
He played an essential role in the exploration and understanding of visceral dysfunctions and their link to the sacroiliac joint, beginning his work in the 1970s.
The sacroiliac (SI) joint is often considered to be solely involved in musculoskeletal disorders, but Jean-Pierre Barral’s groundbreaking research has revealed a fascinating link between this joint and visceral dysfunction.
In the 1970s, Barral began to explore the complex interactions between internal organs and the musculoskeletal system, focusing particularly on the SI joint. He observed that visceral dysfunctions, such as adhesions or tensions in the abdominal organs, could exert indirect influences on the sacroiliac joint, leading to imbalances and pain in the pelvic and lumbar region.
Barral’s pioneering work opened new avenues in the practice of osteopathy, highlighting the importance of considering the body as a whole when evaluating and treating musculoskeletal disorders. Its holistic approach has allowed a better understanding of the underlying mechanisms of lower back and pelvic pain, and has opened new perspectives for patient care.
Over the decades, Barral continued to deepen his research into the interactions between the viscera and the SI joint, developing specific treatment techniques to restore balance between these systems. His contributions have had a significant impact on the practice of osteopathy, expanding our understanding of the complex connections between the different systems of the human body.
In addition to his research, Barral has shared his knowledge through training and publications, influencing generations of osteopathic practitioners. His commitment to continued exploration and dissemination of his discoveries has helped advance the field of manual medicine and improve the care of patients suffering from pelvic and lower back pain of visceral origin.
Vladimir Andrysek, MD
Vladimir Andrysek, MD: His involvement in research into musculoskeletal dysfunctions and disorders, including those involving the sacroiliac joint, began in the 1970s and continued throughout the following decades.
Musculoskeletal dysfunctions, particularly those affecting the sacroiliac (SI) joint, are common problems that can have a significant impact on patients’ quality of life. Vladimir Andrysek, through his ongoing research, has sought to better understand these disorders and develop effective treatment approaches.
In the 1970s, Andrysek began his first studies of the sacroiliac joint, exploring its mechanisms of operation and its interactions with other structures in the body. At that time, techniques for diagnosing and treating SI joint dysfunction were still developing, and Andrysek’s research helped shed light on these areas.
Over the next decades, Andrysek continued to deepen his research, exploring new aspects of musculoskeletal dysfunction and related disorders. He used a multidisciplinary approach, combining advanced imaging techniques, biomechanical studies and innovative treatment methods to study and treat sacroiliac joint problems.
Andrysek’s contributions have been significant in the field of management of musculoskeletal disorders, particularly those involving the sacroiliac joint. His research has contributed to the development of more accurate diagnostic protocols and more effective treatment strategies, thereby improving outcomes for patients suffering from these conditions.
André K. Vleeming, Ph.D.
His research in the 1980s and 1990s greatly enriched our understanding of the biomechanics and stability of the sacroiliac (SI) joint.
The sacroiliac (SI) joint plays a crucial role in the stability and mobility of the pelvis, but its anatomical complexity has long made it a difficult subject of study. However, thanks to the innovative work of André K. Vleeming, our understanding of this essential articulation has progressed considerably.
In the 1980s and 1990s, Vleeming focused on the detailed anatomy of the SI joint, using advanced dissection techniques and imaging methods to explore its structures and relationships with surrounding tissues. His research has shed light on the unique characteristics of the SI joint, including its anatomical variations and biomechanical adaptations in response to forces exerted on the pelvis.
Alongside his work on anatomy, Vleeming became interested in the biomechanics of the SI joint, seeking to understand how it functions in different movement and loading situations. His studies used advanced techniques such as cinematography and computer analysis to study the forces, stresses and movements applied to the joint during various physical activities.
Vleeming’s research also addressed the question of SI joint stability, examining the role of ligaments, muscles and external forces in maintaining it. His work has contributed to a better understanding of the mechanisms of joint stabilization, as well as the identification of risk factors for associated dysfunction and pain.
In addition to his academic contributions, Vleeming has played a crucial role in disseminating his knowledge through scientific publications, conferences and clinical training. His commitment to sharing his findings with the medical community has had a significant impact on clinical practice, helping clinicians better diagnose and treat SI joint disorders.
Fred L. Mitchell, Sr. and Fred L. Mitchell, Jr.
Their work in the 1970s and 1980s contributed significantly to the understanding of the anatomy and biomechanics of the sacroiliac (SI) joint.
The sacroiliac (SI) joint is an essential component of the human musculoskeletal system, playing a crucial role in load transmission and movement between the pelvis and spine. The work of Fred L. Mitchell, Sr. and Fred L. Mitchell, Jr. laid the foundation for our current understanding of this complex structure.
In the 1970s, their research explored the detailed anatomy of the SI joint, highlighting its unique features and relationship to surrounding structures. Their careful dissections identified the ligaments, muscles and joint surfaces involved in joint stability and function.
During the 1980s, the Mitchells expanded their scope of study to include the biomechanics of the SI joint. Their experiments used sophisticated methods such as high-speed cinematography and computer analysis to study the forces, movements and stresses applied to the joint during various activities.
Through their innovative work, the Mitchells have helped enlighten clinicians about the underlying mechanisms of SI joint disorders, such as sacroiliac dysfunction and associated lower back pain. Their research has also guided the development of more precise assessment and treatment techniques for these conditions.
In addition to their academic contributions, the Mitchells have played a crucial role in the training and education of health professionals, disseminating their knowledge through publications, conferences and workshops. Their dedication to research and teaching has influenced generations of health care practitioners and helped improve the care of patients with SI joint disorders.
Michael TW Piek, MD
Dr. Piek’s research on the clinical anatomy and biomechanics of the sacroiliac joint extends from the late 20th century to more recent years. He is recognized for his research on the clinical anatomy and biomechanics of the sacroiliac joint.
The sacroiliac (SI) joint is a complex structure that connects the sacrum to the ilium, playing a crucial role in the stability and mobility of the pelvis. Dr. Piek’s work focuses on understanding this essential joint and its role in musculoskeletal disorders.
As an orthopedic surgeon and anatomist, Dr. Piek has conducted extensive studies on the detailed anatomy of the SI joint, identifying its bony, ligamentous, and muscular structures. His research has provided a better understanding of the anatomical variations and biomechanical adaptations of the joint, which is essential for the diagnosis and treatment of associated pathologies.
Alongside his work on anatomy, Dr. Piek has also explored the biomechanics of the SI joint, using advanced techniques such as medical imaging analysis and computer modeling. His studies have examined the forces, movements and stresses applied to the joint in various clinical settings, providing crucial information to optimize treatment strategies.
Dr. Piek’s research has also had a significant impact on clinical practice, helping clinicians better understand the mechanisms underlying SI joint disorders such as sacroiliac dysfunction and low back pain. His contributions have influenced diagnostic and treatment protocols, allowing for more accurate and effective management of these common conditions.
Don T. Kirkaldy-Willis, MD, and Howard SA Bernstein, MD
Their research, spanning several decades, has made significant contributions to the understanding of spinal disorders, with notable advances made in the second half of the 20th century and continuing into the 21st century.
The work of Kirkaldy-Willis and Bernstein revolutionized our understanding of spinal conditions, focusing on biomechanics, pathology and treatment strategies. Their collaboration gave rise to innovative theories that have influenced clinical practice and research in the field of orthopedics and neurosurgery.
In the second half of the 20th century, Kirkaldy-Willis and Bernstein introduced the concept of segmental spinal degeneration, highlighting specific pathological changes seen in the intervertebral discs and facet joints. Their multidisciplinary approach, combining anatomy, radiology and pathology, has allowed a more in-depth understanding of the underlying mechanisms of lumbar and cervical disorders.
In the 21st century, their work has continued to influence clinical practice and research, with a particular emphasis on the conservative management of spinal conditions. Kirkaldy-Willis and Bernstein developed treatment protocols focused on restoring spinal function and preventing recurrence, emphasizing physical therapy, spinal manipulation, and functional rehabilitation.
Their research also explored the psychosocial aspects of spinal disorders, recognizing the importance of psychological and social factors in patients’ pain perception and recovery. Their holistic approach to the management of spinal conditions has contributed to a better understanding of the mechanisms of chronic pain and the development of more integrative treatment strategies.
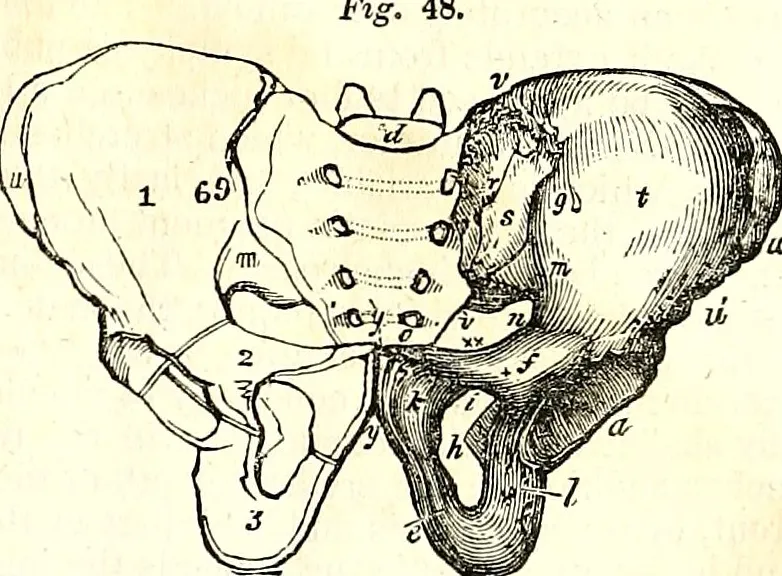
Anatomy of the sacroiliac joint
The sacroiliac (SI) joints represent an essential component of the pelvic girdle, playing a crucial role in upper body stability and facilitating the harmonious transfer of forces generated by the lower limbs during walking. The anatomical complexity of these joints deserves particular attention to understand their functioning and their evolution over time.
The sacroiliac joints form from an initially flat, round joint, evolving over time into an inverted “L” shaped structure. This transformation occurs with aging, creating a rearward-facing configuration, characterized by a short upper arm and a longer lower arm. This structural adaptation makes it possible to optimize the transmission of forces and effectively support body movements.
These joints are located between the articular surfaces of the sacrum and the ilium, located on the lateral aspect of the sacrum. They are an integral part of the synovial joint, where the anterior and lower third constitutes the synovial portion, with the presence of hyaline cartilage on the sacral side and fibrocartilage on the iliac side. This unique configuration contributes to shock absorption and the balanced distribution of stresses exerted on these joints.
Although sacroiliac joint movements are not directly regulated by dedicated muscles, many surrounding muscles exert an indirect influence on their function. It is important to note that the anatomical and functional complexity of these joints makes them an essential area of study for healthcare professionals, particularly in the context of musculoskeletal disorders and lower back pain.


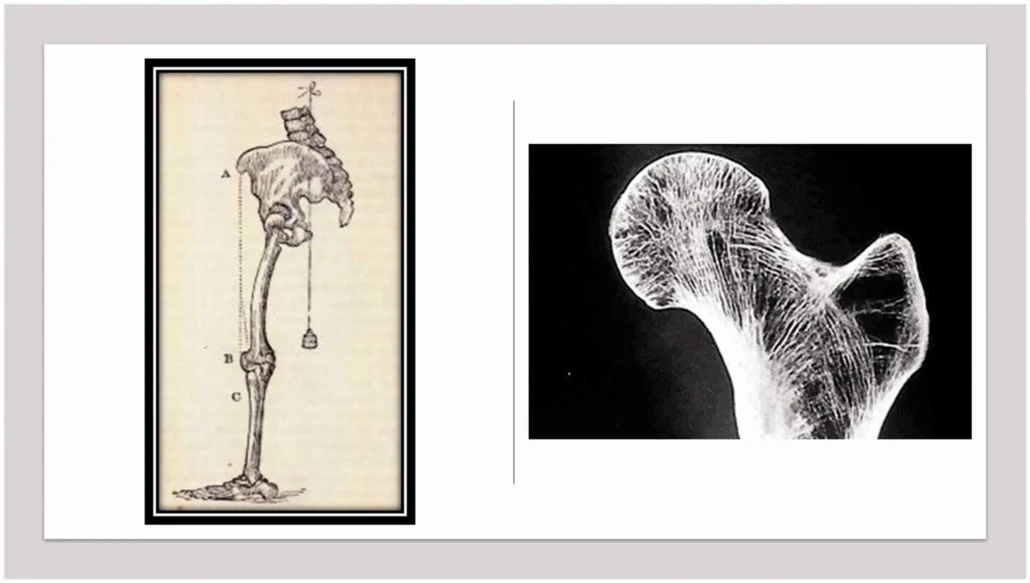
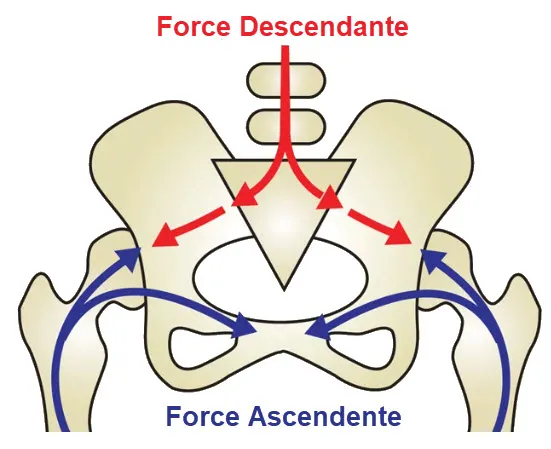
Up and down force
When we talk about upward and downward forces at the sacroiliac joint, we are generally referring to the way in which forces are transmitted through this joint based on body movements. However, there is no purely upward or downward force in this joint; rather, there is a complex combination of forces that depend on muscular movements and actions.
- Descending Forces:
- When the body supports a load, such as when walking, running or standing, there is a transmission of forces downward through the spine and ASI to the lower extremities.
- Ascending Forces:
- Upward forces can be associated with movements where the body straightens, such as when pushing up from a seated position or bending forward to a standing position.
- Muscles and Stabilization:
- The surrounding muscles, including the gluteal muscles, core muscles, and pelvic muscles, play a crucial role in stabilizing the ASI. They help balance and distribute the forces that pass through this joint.
- Physiological Constraints:
- During pregnancy, for example, hormones such as relaxin can influence the stability of the ASI to allow greater elasticity, preparing the body for childbirth.
- Pain and Dysfunction:
- Muscle imbalances, incorrect movements, injuries, or postural problems can contribute to pain or dysfunction in the ASI. Certain disorders, such as sacroiliac syndrome, may be associated with problems in this area.

Sacroiliac movement
The sacroiliac (SI) joint is a joint located between the sacrum (the lower part of the spine) and the ilium (the pelvic bone). Movements of the sacroiliac are generally sliding, rotating, and slight tilting movements. These movements may be limited or altered if the joint is dysfunctional, such as in sacroiliac syndrome.
Movements of the sacroiliac joint include:
- Anterior and posterior tilt of the pelvis: During anterior tilt, the pelvis tilts forward, while during posterior tilt, it tilts backward. These movements are associated with the flexion and extension movements of the spine.
- Rotation: The sacroiliac joint can undergo rotational movements, meaning the sacrum can rotate slightly in relation to the ilium.
- Gliding: Sliding movements may occur, allowing the articular surfaces of the sacroiliac joint to move relative to each other.
- Compression and relaxation: Compression and relaxation forces can also play a role, particularly when transmitting loads between the spine and lower extremities.
Movement of the sacroiliac joint is generally relatively limited compared to other joints such as the hip or shoulder. However, they are essential for pelvic stability, the transmission of forces during walking and other activities, and for adapting to changes in body position.
Causes of Sacroiliac Syndrome
Let’s explore some of the possible causes of SSI in more detail:
- Trauma: Trauma, such as a fall, car accident, or sports injury, can cause damage to the sacroiliac joint. Significant forces exerted on the pelvic region can lead to instability or injury.
- Ligament instability: The ligaments surrounding the sacroiliac joint play a crucial role in its stability. Distension, overstretching, or weakness of the ligaments can lead to instability, thereby causing symptoms of SSI.
- Pregnancy: Hormonal changes during pregnancy, such as increased relaxin, can affect ligaments, softening them to make childbirth easier. However, it can also lead to instability of the sacroiliac joint, causing pain in some pregnant women.
- Arthritis: Forms of inflammatory arthritis, such as ankylosing spondylitis, can affect joints, including the sacroiliac joint. The resulting inflammation may contribute to the development of SSI.
- Leg asymmetry: Unequal leg length can create asymmetric stress on the sacroiliac joint, disrupting its balance. This asymmetry can result from a variety of conditions, including growth disorders or injuries.
- Repetitive movements: Certain occupations or activities that involve repetitive movements, such as lifting heavy objects incorrectly, can overstrain the sacroiliac joint, contributing to its dysfunction.
- Muscle dysfunction: Muscle imbalances in the pelvic region can disrupt the normal mechanics of the sacroiliac joint. Muscle weakness or uneven tension can negatively influence this joint.
- Postural stress: Poor posture, especially from prolonged periods of sitting in an inappropriate position, can place excessive pressure on the sacroiliac joint. This can lead to premature wear or imbalances.
Symptoms of Sacroiliac Syndrome
Symptoms of sacroiliac syndrome (SSI) can vary from person to person, but they generally include:
- Lower back pain: Pain is often felt in the lumbar region, usually on one side of the lower back. The pain may be localized or spread to the buttocks, hips, thigh or leg.
- Pain in the buttocks or hips: Pain may be felt in the buttocks or hips area, often on one side.
- Pain worse with certain movements: Symptoms may worsen with certain movements, such as getting up from a chair, climbing stairs, or turning the body.
- Stiffness or stuck feeling: Some individuals may feel stiffness in the sacroiliac joint, or feel like something is blocking.
- Difficulty standing or walking: Pain can make it difficult to stand for long periods of time or walk.
- Radiation of pain to the leg: In some cases, pain may radiate down the thigh or leg, sometimes mimicking symptoms similar to sciatica.
- Pain during pregnancy: In some women, SSI may be associated with pregnancy due to hormonal changes that affect the ligaments around the sacroiliac joint.
It is important to note that the symptoms of SSI can sometimes be similar to other conditions, such as a herniated disc or sciatica.
Osteopathy and treatment of sacroiliac syndrome
Here are some techniques commonly used by osteopaths to treat SSI:
- Muscle release techniques: Muscle tension around the sacroiliac joint can contribute to SSI. The osteopath uses muscle release techniques to relax tense muscles, thus promoting better mobility of the joint.
- Specific stretches: Targeted stretches may be prescribed to loosen the muscles associated with the sacroiliac joint. These stretches can be taught to the patient so that they can practice them at home.
- Mobilization techniques: The osteopath can use mobilization techniques to improve joint mobility without performing direct joint manipulation. This may be particularly beneficial for patients preferring less direct approaches.
- Postural Correction: Postural adjustments may be recommended to correct imbalances that contribute to SSI. This may include advice on posture when sitting, standing and walking.
- Specific exercises: The osteopath can prescribe specific exercises aimed at strengthening the stabilizing muscles of the sacroiliac joint. These exercises help maintain stability and prevent recurrence.
- Ergonomic advice: Lifestyle and ergonomic advice can be provided to minimize SSI risk factors. This may include recommendations on posture at work, carrying loads, etc.
It is important to note that osteopathic treatment is tailored to each patient based on their specific condition and needs.
Exercise and stretching
Here are some general exercises and stretches that may be helpful in managing SSI:
Strengthening Exercises
- Pelvic elevations:
- Lie on your back with your knees bent.
- Contract your gluteal muscles and slowly lift your hips toward the ceiling.
- Hold the position for a few seconds, then slowly lower back down.
- Repeat several times.
- Unilateral bridges:
- In the same starting position as the pelvic raises, lift one leg toward the ceiling while keeping your hips raised.
- Alternate between legs while keeping hips elevated.
- This strengthens the gluteal and stabilizer muscles.
- Knee to chest:
- Lie on your back and bring one knee toward your chest, holding it with your hands.
- Hold the position for 15-30 seconds, then release.
- Alternate between legs.
Stretching
- Stretching the piriformis muscle:
- In a seated position, cross one ankle over the opposite knee.
- Tilt your torso slightly forward while keeping your back straight.
- You should feel the stretch in the buttock of the crossed leg.
- Adductor stretch:
- Sitting with your legs apart, slowly lean forward, keeping your back straight.
- Stretch your hands forward, toward your feet.
- This stretch targets the adductors.
- Hip flexor stretch:
- From your knees, bring one leg forward, keeping your foot flat on the floor.
- Lean your pelvis forward while keeping your back straight.
- You should feel the stretch in the front of the hip.
These exercises and stretches aim to strengthen the stabilizing muscles and improve flexibility around the sacroiliac joint.
Clinical assessment of sacroiliac syndrome
Posterior pelvic pain provocation test (Östgaard):
The Posterior Pelvic Pain Provocation Test, also known as the Östgaard Test, is a clinical assessment used to assess posterior pelvic pain in individuals, particularly pregnant women. This test was developed by Norwegian researcher Stuge Östgaard.
The Posterior Pelvic Pain Provocation Test procedure generally consists of several steps:
- Patient positioning: The patient usually lies supine on an examination table.
- Hip flexion: The practitioner asks the patient to flex the hips, usually by drawing the knees toward the chest. This can be done while sitting or lying down.
- Pain assessment: During hip flexion, the practitioner observes and asks the patient about the presence of pain, particularly in the pelvis or posterior pelvic region.
- External rotation of the hips: Next, the practitioner can apply slight external rotation to the patient’s hips to see if this causes an increase in posterior pelvic pain.
- Reproducing symptoms: If the movement or position reproduces the symptoms of posterior pelvic pain, it may indicate tenderness or dysfunction at the sacroiliac joint.
The Östgaard Test is often used in the context of managing pelvic pain, particularly during pregnancy. It aims to assess the sensitivity of the sacroiliac joint and identify specific movements that may trigger or worsen pain in the patient. It is important to note that the test results should be interpreted by a qualified healthcare professional, who can then recommend appropriate interventions or treatments based on the assessment results.


Flexion, abduction and external rotation test (FABER test)
The Flexion, Abduction, and External Rotation Test, commonly known as the FABER test, is a clinical examination used to evaluate hip joint function and mobility, particularly at the hip joint and of the sacroiliac joint. This test is also known as the Patrick test or Patrick-FABER test.
Here is how the FABER test generally takes place:
- Patient positioning: The patient lies supine on an examination table.
- Flexion, abduction and external rotation of the hip: The practitioner positions the lower limb to be tested in a specific position. The knee and hip of the side to be tested are bent at a right angle, with the foot placed against the opposite knee. This position forms a figure similar to the letter “4”. The practitioner then applies light downward pressure to the knee on the side being tested, causing flexion, abduction and external rotation of the hip.
- Symptom Assessment: The patient is asked to report any discomfort, pain, or restriction of movement during application of pressure.
- Comparison with the other side: The test is often performed on both sides to allow a comparison between the right and left sides.
The FABER test is commonly used to assess hip joint and sacroiliac joint mobility. Pain or restriction of movement during the test may indicate potential problems, such as joint disorders, muscle strains, or sacroiliac joint dysfunction.
It is important to note that the FABER test is part of a comprehensive assessment and should be interpreted by a qualified healthcare professional based on the clinical context and other relevant medical information. This test is often used in the field of osteopathy, orthopedics and sports medicine.


The Flexion, Abduction, and External Rotation Test, commonly known as the FABER test, is a clinical examination used to evaluate hip joint function and mobility, particularly at the hip joint and of the sacroiliac joint. This test is also known as the Patrick test or Patrick-FABER test.
relevant medical information. This test is often used in the field of osteopathy, orthopedics and sports medicine.
Sacroiliac Compression Test
Test positioning: the subject lies on their side. The examiner stands next to the subject and places both hands directly on the subject’s iliac crest. Repeat bilaterally.
Action: Examiner applies downward pressure.
Positive result: Increased pain or pressure indicates SI joint dysfunction.


Gaenslen test
Test Positioning: The subject lies on the side of the uninvolved leg. With the involved leg in slight hyperextension, the subject then flexes the knee on the uninvolved side toward the chest.
Action: The examiner stabilizes the subject’s pelvis and further extends the affected leg.
Positive Finding: Pain in the SI region is a positive finding and may be associated with SI joint dysfunction.


Bilateral Straight Leg Raise Test
Test Positioning: The subject lies supine with hips and knees extended. The examiner stands with the distal hand or forearm around or under the subject’s heels and the proximal hand on the subject’s distal thighs to maintain knee extension.
Action: With the subject relaxed, slowly raise the legs until you notice pain or tightness.
Positive result: Low back pain occurring at hip flexion angles less than 70 degrees indicates SI joint damage. Low back pain occurring at hip flexion angles greater than 70 degrees indicates damage to the lumbar spine.
SI Joint Distraction Test


Test positioning: the subject lies on their back. The examiner stands next to the subject with arms crossed, places the heel of both hands on the subject’s anterior superior iliac spines.
Action: The examiner applies outward and downward pressure with the heel of the hands.
Positive result: Unilateral pain in the SI joint or gluteal ligament region indicates a SI ligament sprain or SI joint dysfunction.
References
- Cohen SP. Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. Anesth Analg. 2005 Nov;101(5):1440-1453. [ PubMed ]
- Chuang CW, Hung SK, Pan PT, Kao MC. Diagnosis and interventional pain management options for sacroiliac joint pain. Ci Ji Yi Xue Za Zhi. 2019 Oct-Dec;31(4):207-210. [ PMC free article ] [ PubMed ]
- Slipman CW, Whyte WS, Chow DW, Chou L, Lenrow D, Ellen M. Sacroiliac joint syndrome. Pain Physician. 2001 Apr;4(2):143-52. [ PubMed ]
- Fortin JD. Sacroiliac Joint DysfunctionA New Perspective. J Back Musculoskelet Rehabil. 1993 Jan 01;3(3):31-43. [ PubMed ]
- Ivanov AA, Kiapour A, Ebraheim NA, Goel V. Lumbar fusion leads to increases in angular motion and stress across sacroiliac joint: a finite element study. Spine (Phila Pa 1976). 2009 Mar 01;34(5):E162-9. [ PubMed ]
- Ha KY, Lee JS, Kim KW. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up. Spine (Phila Pa 1976). 2008 May 15;33(11):1192-8. [ PubMed ]
- Simopoulos TT, Manchikanti L, Gupta S, Aydin SM, Kim CH, Solanki D, Nampiaparampil DE, Singh V, Staats PS, Hirsch JA. Systematic Review of the Diagnostic Accuracy and Therapeutic Effectiveness of Sacroiliac Joint Interventions. Pain Physician. 2015 Sep-Oct;18(5):E713-56. [ PubMed ]
- Kiapour A, Joukar A, Elgafy H, Erbulut DU, Agarwal AK, Goel VK. Biomechanics of the Sacroiliac Joint: Anatomy, Function, Biomechanics, Sexual Dimorphism, and Causes of Pain. Int J Spine Surg. 2020 Feb;14(Suppl 1):3-13. [ PMC free article ] [ PubMed ]
- Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012 Dec;221(6):537-67. [ PMC free article ] [ PubMed ]
- Poilliot AJ, Zwirner J, Doyle T, Hammer N. A Systematic Review of the Normal Sacroiliac Joint Anatomy and Adjacent Tissues for Pain Physicians. Pain Physician. 2019 Jul;22(4):E247-E274. [ PubMed ]









{kind=link}