


Introduction
Scoliosis is a musculoskeletal disorder characterized by an abnormal curvature of the spine, typically in a sideways direction. This condition often develops during the growth spurt just before puberty. While scoliosis can be caused by conditions such as cerebral palsy and muscular dystrophy, the cause of most scoliosis is unknown.
Understanding Scoliosis
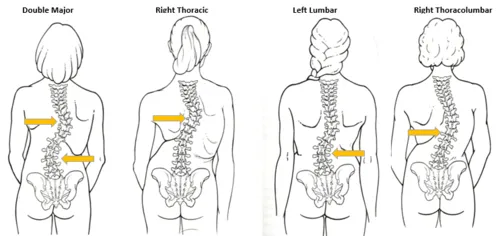
In scoliosis, the spine may curve to the left or right, forming an “S” or “C” shape. The severity of the curve can vary widely, and in some cases, it can worsen as the individual grows. The curvature can also cause the ribs to protrude on one side of the body more than the other, leading to an asymmetrical appearance of the torso.

Importance of Screening
Early detection of scoliosis is crucial for several reasons. First, identifying scoliosis early allows for early intervention, which can prevent the progression of the curvature. For most cases of scoliosis, especially those diagnosed during adolescence, the curvature can worsen as the child grows. Early intervention through bracing or other measures can potentially reduce the need for surgery later in life.
Second, scoliosis screening helps identify cases that require further evaluation and treatment. While many cases of scoliosis are mild and do not require treatment, some can progress and cause complications, such as pain, difficulty breathing, or heart problems if the curvature affects the chest cavity.
Third, screening for scoliosis helps to assess the risk factors and potential causes of the condition. While most cases of scoliosis are idiopathic, meaning there is no clear cause, some cases are linked to neuromuscular conditions such as cerebral palsy or muscular dystrophy. Identifying these risk factors can help in the early diagnosis and treatment of scoliosis.
Guidelines and Recommendations
National and International Guidelines
National and international organizations provide guidelines for scoliosis screening to ensure early detection and appropriate management. These guidelines are based on evidence-based practices and aim to optimize outcomes for individuals with scoliosis.
In the United States, the American Academy of Orthopaedic Surgeons (AAOS) and the Scoliosis Research Society (SRS) recommend screening programs for adolescents, particularly during growth spurts. The AAOS recommends screening for scoliosis in children and adolescents aged 10 to 14 years old, as this is when scoliosis most commonly develops. Screening should be performed annually or biennially during this period.
Internationally, guidelines vary by country but generally follow a similar approach. For example, the United Kingdom National Screening Committee (UK NSC) recommends against universal scoliosis screening due to the potential for false positives and overdiagnosis. Instead, they recommend selective screening for individuals at higher risk, such as those with family history, neuromuscular conditions, or previous spine abnormalities.
Age and Frequency Recommendations
- Age Recommendations:
- Screening for scoliosis typically begins around the age of 10 years, coinciding with the onset of puberty and the period of rapid growth.
- The screening process continues until the age of skeletal maturity, which is around 16-18 years for girls and 18-20 years for boys.
- Frequency Recommendations:
- Annual Screening: Many organizations recommend annual screening during the adolescent growth spurt, especially between ages 10 and 14 years.
- Biennial Screening: In some regions, screening may be performed every two years to balance early detection with minimizing unnecessary testing.
- Selective Screening: For individuals at higher risk or with certain risk factors, more frequent or targeted screening may be recommended.
These age and frequency recommendations aim to detect scoliosis early enough to intervene and prevent progression while minimizing unnecessary testing and potential harms associated with false positives. Regular screening ensures that healthcare providers can monitor spinal curvature and initiate appropriate treatments promptly when necessary.
Methods of Screening
Screening for scoliosis involves several methods to assess spinal curvature and identify individuals who may require further evaluation or treatment. These methods range from simple clinical examinations to more advanced radiographic evaluations.
Clinical Examination
Clinical examination is the initial step in screening for scoliosis and involves:
- Observation: The healthcare provider visually inspects the individual’s back while they stand and then bends forward. This helps to detect any asymmetry or abnormal curvature of the spine.
- Palpation: The healthcare provider may palpate (feel) the spine and surrounding muscles for any abnormalities or deviations from the normal spinal structure.
- Assessment of Trunk Symmetry: The provider assesses the alignment of the shoulders, scapulae (shoulder blades), and waistline to identify any signs of asymmetry that may indicate scoliosis.
- Measurement of Rib Hump: A rib hump can be palpated on forward bending in patients with scoliosis, indicating vertebral rotation.
Clinical examination is often used as the initial screening tool due to its simplicity and non-invasive nature. However, it may not be sufficient for confirming scoliosis diagnosis, especially in cases where the curvature is subtle or in younger children where spinal growth is ongoing.
Adam’s Forward Bend Test
The Adam’s Forward Bend Test is a specific maneuver used during clinical examination:

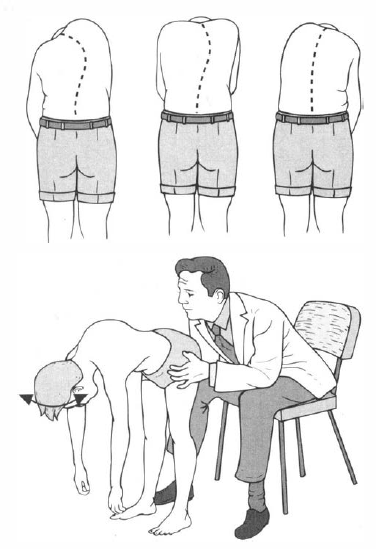
- Procedure: The individual stands with feet together and bends forward at the waist, allowing the arms to hang freely. The examiner observes the back for any asymmetry, rib prominence, or abnormal curvature.
- Detection of Scoliosis: A positive test is indicated by asymmetry, rib prominence (rib hump), or the appearance of a curve in the spine that may not be apparent when standing upright.


The Adam’s Forward Bend Test is a simple and effective screening tool that helps identify individuals who may have scoliosis and need further evaluation. It can be performed quickly and easily in a clinical setting.
Radiographic Evaluation
Scoliosis Radiographic Evaluation
Radiographic evaluation is considered the gold standard for confirming the diagnosis and assessing the severity of scoliosis.
Indications: Radiographic evaluation is typically recommended when clinical examination or other screening methods suggest the presence of scoliosis, or when monitoring the progression of scoliosis over time.
Imaging Techniques: X-rays are the most commonly used imaging modality for scoliosis evaluation. They provide detailed images of the spine, allowing healthcare providers to measure the degree of curvature and assess any associated vertebral rotation.
Assessment:
- Cobb Angle: One of the primary measurements obtained from radiographic images is the Cobb angle, which quantifies the degree of spinal curvature. To measure the Cobb angle, lines are drawn parallel to the top and bottom vertebrae of the curve. The angle between the intersecting perpendicular lines drawn from these parallel lines represents the Cobb angle. This measurement is critical for diagnosing scoliosis, determining its severity, and monitoring changes over time. A Cobb angle greater than 10 degrees typically indicates scoliosis.
- Location and Magnitude: Radiographs enable healthcare providers to pinpoint the location of the curvature (thoracic, lumbar, or thoracolumbar) and determine its magnitude. The Cobb angle provides a numerical value to classify the severity: mild (10-20 degrees), moderate (20-40 degrees), or severe (greater than 40 degrees).
- Pattern of Curvature: Radiographs help identify the pattern of the spinal curve, whether it is a single curve (C-shaped) or a double curve (S-shaped), which is essential for developing a tailored treatment plan.


While radiographic evaluation provides valuable information for scoliosis diagnosis and management, it involves exposure to ionizing radiation. Therefore, its use is generally reserved for cases where clinical or other screening methods suggest significant spinal deformity or progression of scoliosis.
Considerations in Screening
Screening for scoliosis involves several important considerations to ensure effective and ethical practice. These considerations include understanding the benefits and limitations of screening, the implications of false positives and false negatives, and the ethical principles surrounding informed consent.
Benefits and Limitations
Benefits:
- Early Detection: Screening allows for early detection of scoliosis, which can facilitate timely intervention and treatment.
- Prevent Progression: Early intervention can prevent the progression of spinal curvature and reduce the likelihood of needing surgery.
- Improved Outcomes: Early detection and treatment can lead to better outcomes and improved quality of life for individuals with scoliosis.
Limitations:
- Overdiagnosis: Screening can lead to the identification of mild cases that may not progress or require treatment.
- False Positives: Some individuals may be incorrectly identified as having scoliosis (false positives), leading to unnecessary anxiety and additional testing.
- Resource Intensive: Screening programs can be resource-intensive in terms of time, manpower, and healthcare costs.
False Positives and False Negatives
False Positives:
- Definition: A false positive occurs when screening identifies a condition that is not actually present.
- Implications: False positives can lead to unnecessary follow-up tests, anxiety for the individual and their family, and unnecessary treatment interventions.
False Negatives:
- Definition: A false negative occurs when screening fails to identify a condition that is actually present.
- Implications: False negatives can delay diagnosis and treatment, allowing the condition to progress unchecked, potentially leading to worse outcomes.
Ethics and Informed Consent
Ethical Considerations:
- Informed Consent: Individuals and their guardians must be informed about the purpose, risks, benefits, and limitations of scoliosis screening.
- Privacy: Screening procedures should respect patient privacy and confidentiality.
- Voluntary Participation: Participation in screening programs should be voluntary, and individuals should have the right to decline or withdraw at any time.
- Equity: Screening programs should be accessible to all individuals, regardless of socioeconomic status or other factors.
Informed Consent:
- Purpose: Clearly communicate the purpose of screening, including the potential benefits and limitations.
- Risks: Discuss the risks associated with screening, including false positives, false negatives, and the potential need for follow-up testing.
- Alternative Options: Provide information about alternative screening methods or options for those who decline screening.
- Decision Making: Ensure that individuals and their guardians have the information necessary to make informed decisions about participation.
Osteopathic management
Osteopathic management of scoliosis involves a comprehensive approach that includes assessment, treatment, and monitoring. This approach aims to improve spinal alignment, reduce symptoms, and prevent progression.
Referral Criteria
Referral criteria for scoliosis are important to ensure that patients receive appropriate care based on the severity and progression of their condition:
- Degree of Curvature: Referral may be indicated based on the degree of spinal curvature measured on radiographs. Generally, referral is considered for curvatures greater than 25-30 degrees.
- Progression of Curvature: Patients with scoliosis that is progressing despite conservative measures may require referral to a specialist for further evaluation and management.
- Presence of Symptoms: Referral may be necessary for patients experiencing symptoms such as pain, breathing difficulties, or other functional impairments related to scoliosis.
- Age of Patient: Referral criteria may vary based on the age of the patient and the potential for progression as the skeleton matures.
- Other Risk Factors: Referral may also be considered for patients with underlying conditions that contribute to scoliosis or complicate its management.
Treatment Options
Osteopathic treatment options for scoliosis focus on improving spinal alignment, reducing muscle tension, and enhancing overall musculoskeletal function:
- Osteopathic Manipulative Treatment (OMT): OMT techniques such as myofascial release, muscle energy techniques, and indirect techniques are used to address musculoskeletal imbalances and promote spinal alignment.
- Exercise Therapy: Specific exercises and stretches can help strengthen muscles and improve flexibility, which can support spinal alignment and function.
- Bracing: In cases of moderate to severe scoliosis, bracing may be recommended to prevent further progression of the curvature, especially in growing children and adolescents.
- Patient Education: Educating patients and their families about scoliosis, proper posture, and lifestyle modifications can empower them to manage the condition effectively.
Monitoring and Follow-Up
Monitoring and follow-up are essential components of osteopathic management to track progression and adjust treatment as needed:
- Regular Clinical Assessment: Clinical assessments, including observation of posture and spinal alignment, are performed regularly to monitor changes in the curvature.
- Periodic Imaging: Radiographic imaging may be performed periodically to assess the degree of curvature and monitor progression.
- Adjustment of Treatment Plan: Based on clinical assessments and imaging results, the treatment plan may be adjusted to address changes in the curvature or symptoms.
- Patient Education: Continued education about scoliosis management, including exercises, posture awareness, and bracing compliance, is important for long-term outcomes.
Conclusion
Summary of Key Points
In conclusion, osteopathic management of scoliosis encompasses a holistic approach that includes assessment, treatment, and monitoring. Key points to consider include:
- Screening and Assessment: Early detection through clinical examination, Adam’s Forward Bend Test, and radiographic evaluation is crucial for identifying scoliosis and determining the severity of spinal curvature.
- Referral Criteria: Referral to specialists is based on the degree of curvature, progression of the condition, presence of symptoms, and other risk factors.
- Treatment Options: Osteopathic treatment options such as OMT, exercise therapy, bracing, and patient education aim to improve spinal alignment, reduce muscle tension, and enhance musculoskeletal function.
- Monitoring and Follow-Up: Regular clinical assessments and periodic imaging help monitor progression and adjust treatment plans as necessary.
Future Directions
Looking ahead, several areas warrant further exploration and development in the field of osteopathic management of scoliosis:
- Research: Continued research into the effectiveness of osteopathic treatments for scoliosis, including larger clinical trials and longitudinal studies, is needed to establish evidence-based guidelines.
- Advanced Techniques: Exploration of advanced osteopathic techniques and their impact on spinal alignment and patient outcomes.
- Patient-Centered Care: Emphasis on patient-centered care, including shared decision-making and patient education, to improve treatment adherence and outcomes.
- Interdisciplinary Collaboration: Strengthening interdisciplinary collaboration between osteopaths, orthopedic surgeons, physical therapists, and other healthcare providers to optimize care pathways for patients with scoliosis.
- Healthcare Policies: Advocacy for healthcare policies that support early screening programs, access to osteopathic care, and reimbursement for osteopathic treatments.
Final Thoughts
Osteopathic management of scoliosis offers a comprehensive approach that addresses the complex needs of patients with spinal curvature. By focusing on early detection, conservative treatments, and regular monitoring, osteopaths play a crucial role in improving outcomes and quality of life for individuals affected by scoliosis. Continued advancements in research and practice will further enhance our understanding and treatment of this challenging musculoskeletal condition.
References:
- Negrini, S., Donzelli, S., Aulisa, A. G., Czaprowski, D., Schreiber, S., De Mauroy, J. C., … & Zaina, F. (2018). 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders, 13, 3. doi:10.1186/s13013-017-0145-8.
- U.S. Preventive Services Task Force. (2018). Screening for adolescent idiopathic scoliosis: US Preventive Services Task Force recommendation statement. JAMA, 319(2), 165-172. doi:10.1001/jama.2017.19342.
- Hresko, M. T., Talwalkar, V., & Schwend, R. M. (2013). Early detection of idiopathic scoliosis in adolescents. The Journal of Bone and Joint Surgery, 95(14), e98(1-8). doi:10.2106/JBJS.L.01160.
- Bunnell, W. P. (2005). Selective screening for scoliosis. Clinical Orthopaedics and Related Research, 434, 40-45. doi:10.1097/01.blo.0000160050.06365.60.
- Grivas, T. B., Wade, M. H., Negrini, S., O’Brien, J. P., Maruyama, T., Rigo, M., & Kotwicki, T. (2007). SOSORT consensus paper: School screening for scoliosis. Where are we today? Scoliosis, 2, 17. doi:10.1186/1748-7161-2-17.
- Labelle, H., Richards, S. B., De Kleuver, M., Grivas, T. B., Luk, K. D., Wong, H. K., … & Kotwicki, T. (2013). Screening for adolescent idiopathic scoliosis: An information statement by the Scoliosis Research Society International Task Force. Scoliosis, 8, 17. doi:10.1186/s13013-014-0007-7.
- The Scoliosis Research Society. (n.d.). Adolescent Idiopathic Scoliosis Screening. Retrieved from Scoliosis Research Society Website.
- Konieczny, M. R., Senyurt, H., & Krauspe, R. (2013). Epidemiology of adolescent idiopathic scoliosis. Journal of Children’s Orthopaedics, 7(1), 3-9. doi:10.1007/s11832-012-0457-4.
- Rowe, D. E., Feise, R. J., & Crowther, E. R. (1997). The effect of chiropractic treatment on adolescent idiopathic scoliosis: A pilot study. Journal of Manipulative and Physiological Therapeutics, 20, 535-539. doi:10.1016/S0161-4754(97)90095-8.
- Weinstein, S. L., Dolan, L. A., Wright, J. G., & Dobbs, M. B. (2013). Effects of bracing in adolescents with idiopathic scoliosis. New England Journal of Medicine, 369(16), 1512-1521. doi:10.1056/NEJMoa1307337.
- Dunn, J., Henrikson, N. B., Morrison, C. C., Blasi, P. R., Nguyen, M., & Lin, J. S. (2018). Screening for adolescent idiopathic scoliosis: Evidence report and systematic review for the US Preventive Services Task Force. JAMA, 319(2), 173-187. doi:10.1001/jama.2017.11669.
- Kotwicki, T., Negrini, S., Rigo, M., Maruyama, T., Weiss, H. R., & Chêneau, J. (2008). Methodology of evaluation of morphology of scoliosis and other spinal deformities: 6th SOSORT consensus paper. Scoliosis, 4, 26. doi:10.1186/1748-7161-4-26.
- Negrini, S., & Donzelli, S. (2019). Aetiology of adolescent idiopathic scoliosis: Current trends and relevance to scoliosis clinical practice. Vertebral Column, 27, 217-232. doi:10.1097/BRS.0000000000002953.
- Goldberg, C. J., Dowling, F. E., Fogarty, E. E., & Moore, D. P. (1995). School scoliosis screening and the clinical visit. Spine, 20(12), 1368-1374. doi:10.1097/00007632-199506150-00014.
- Lonstein, J. E. (1994). Adolescent idiopathic scoliosis. The Lancet, 344(8934), 1407-1412. doi:10.1016/S0140-6736(94)90572-X.
- Scoliosis Research Society. (n.d.). Screening for Scoliosis: An Information Statement by the Scoliosis Research Society (SRS) International Task Force. Retrieved from Scoliosis Research Society.
- Wong, H. K., Hui, J. H., Rajan, U., & Chia, H. P. (2005). Idiopathic scoliosis in Singapore schoolchildren: A prevalence study 15 years into the screening program. Spine, 30(10), 1188-1196. doi:10.1097/01.brs.0000164286.93233.63.
- Reamy, B. V., & Slakey, J. B. (2001). Adolescent idiopathic scoliosis: Review and current concepts. American Family Physician, 64(1), 111-116.
- Nachemson, A. L., & Peterson, L. E. (1995). Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. New England Journal of Medicine, 333(11), 726-731. doi:10.1056/NEJM199509143331101.
- Goldberg, C. J., Fogarty, E. E., Moore, D. P., & Dowling, F. E. (1995). Scoliosis school screening: Two decades of experience in Ireland. Annals of the Royal College of Surgeons of England, 77(4), 209-212.








{kind=link}