


Introduction
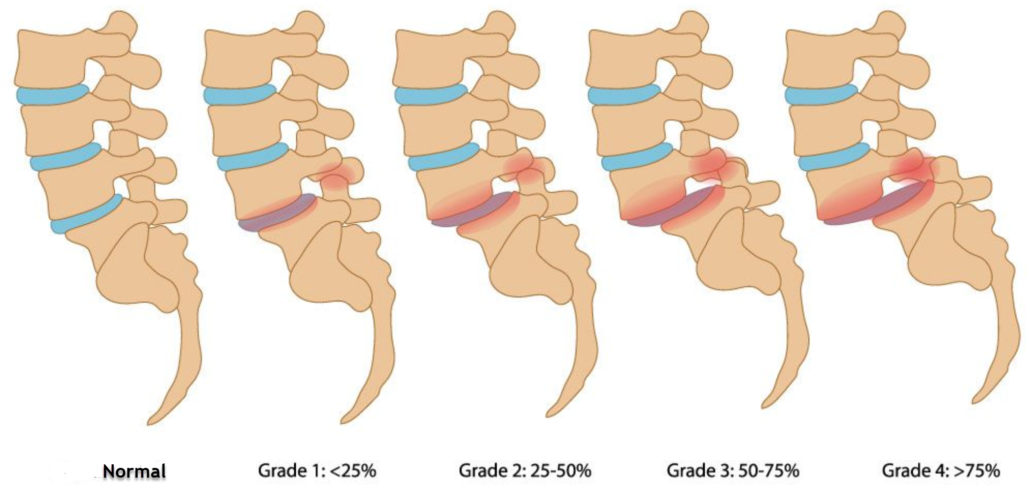
Spondylolisthesis is a medical condition where one vertebra slips forward relative to the underlying vertebra. This condition can be the result of a variety of factors, including birth defects, injuries, or spinal degeneration. For people who participate in gymnastics, spondylolisthesis can present particular challenges and requires a careful approach to avoid worsening the condition.
One of the main concerns when doing gymnastics with spondylolisthesis is maintaining good posture and avoiding movements that could further stress the spine. This generally means avoiding movements that involve hyperextension or excessive flexion of the spine. Gymnastic exercises that put excessive strain on the back, such as jumps, flips, or back arches, can be particularly problematic for people with spondylolisthesis.
Instead, people with spondylolisthesis may benefit from muscle-strengthening exercises that target the core muscles, particularly the abdominal muscles and back muscles. Strengthening these muscles can help stabilize the spine and reduce pressure on the affected vertebrae. Strengthening exercises can include planks, sit-ups, hip bridges, and spinal stabilization exercises.
It is also important for people with spondylolisthesis to maintain good flexibility and mobility in the spine and surrounding joints. However, this must be done with caution to avoid overstraining the spinal structures. Gentle, controlled stretches can be beneficial, but it is essential to perform them with proper technique and without force.
In addition to exercise, pain management and injury prevention are also important aspects to consider for gymnasts with spondylolisthesis. This may involve relaxation techniques, osteopathy sessions, as well as paying close attention to posture and technique when practicing gymnastics.


Causes of Spondylolisthesis
Spondylolisthesis, a condition characterized by the forward movement of one vertebra relative to another, can result from a variety of causes, each contributing to the destabilization of the spine. A main cause is congenital defects, where individuals are born with abnormalities of the vertebrae. These defects, such as dysplastic or elongated facets, predispose individuals to spondylolisthesis at a young age, which can lead to progressive displacement over time.
Degenerative changes in the spine also play a significant role in the development of spondylolisthesis, especially in older people. Wear and tear of spinal structures, such as degenerative disc disease or arthritis of the joints, can weaken the integrity of the spine, allowing the vertebrae to shift. Traumatic injuries, such as fractures or serious accidents, can also lead to spondylolisthesis by causing the vertebrae to suddenly shift, disrupting the stability of the spine.
Repetitive stress on the spine is another common cause, especially among athletes or people engaged in activities involving repetitive hyperextension. Sports like gymnastics, soccer, or weightlifting, which require frequent extension of the spine, can increase the risk of spondylolisthesis, especially in the lumbar region where hyperextension is most common.
Genetic factors can also contribute to spondylolisthesis, with some cases showing a familial predisposition to the condition. Although the precise genetic mechanisms remain unclear, family history may be a significant risk factor.
Specifically, isthmic spondylolisthesis results from defects or fractures in the pars interarticularis, the bony bridge connecting the facet joints at the back of the spine. These defects can be congenital or acquired and are often associated with activities involving repetitive hyperextension, such as gymnastics or football.
Additionally, pathological conditions such as tumors or infections can weaken spinal structures, increasing the risk of spondylolisthesis. These conditions compromise spinal stability and can lead to abnormal vertebral displacement.
Here are some of the most common causes:
- Isthmic spondylolisthesis: This form of spondylolisthesis is often caused by spondylolysis, which is a fracture or weakness in the isthmus of the vertebra. Repetitive activities that put stress on the spine, such as lifting weights or gymnastics, can contribute to this condition.
- Degenerative spondylolisthesis: This form of spondylolisthesis is usually caused by aging and degeneration of the intervertebral discs. With age, the discs become less elastic and can cause the vertebrae to slip.
- Traumatic spondylolisthesis: A traumatic injury, such as a car accident or fall, can result in a fracture or displacement of the vertebrae, causing spondylolisthesis.
- Congenital Spondylolisthesis: In some cases, spondylolisthesis may be present from birth due to congenital abnormalities in the formation of the vertebrae.
- Pathological spondylolisthesis: This form of spondylolisthesis is caused by underlying medical conditions such as osteoporosis, infections or tumors, which weaken the bones and can lead to slippage of the vertebrae.
Symptoms of spondylolisthesis
Lower back pain is often the predominant symptom, characterized by a feeling of pain in the lower back region. This pain may intensify with physical activity or sitting for long periods of time. Sometimes it can radiate along affected nerves, causing pain, tingling, or numbness in the buttocks, thighs, and legs. Sufferers may also experience decreased spinal flexibility, making certain movements difficult to perform. A feeling of muscle weakness in the lower extremities may accompany compression of the spinal nerves, affecting the ability to walk or stand. General mobility of the spine may be reduced, and pain may be exacerbated when standing or during physical activities. Finally, in severe cases, spinal instability may occur, making it difficult to maintain a stable position. Early recognition of these symptoms is crucial to obtaining effective treatment and preventing long-term complications associated with spondylolisthesis.
- Lower back pain: Pain in the lower back region is one of the most common symptoms of spondylolisthesis. This pain may be localized in the lower back region and may worsen with physical activity or prolonged sitting.
- Radicular pain: If the spinal nerves are compressed due to the sliding of the vertebrae, this can lead to pain that travels along the affected nerve. This pain can radiate to the buttocks, thighs, and even legs, and is often described as a burning or shooting pain.
- Numbness and tingling: Compression of the spinal nerves can also cause abnormal sensations such as numbness, tingling, or muscle weakness in the lower extremities.
- Difficulty walking or standing: In severe cases of spondylolisthesis, where slippage of the vertebrae is significant, there may be an impairment in the ability to walk or stand properly due to pain and weakness muscular.
- Reduced spinal flexibility: Due to slippage of the vertebrae, there may be a decrease in spinal flexibility, which may make it difficult to perform certain movements, such as bending forward or twisting. on the coast.
- Decreased mobility: Due to pain and stiffness in the lumbar region, people with spondylolisthesis may experience a decrease in overall spinal mobility.
- Feeling of muscle weakness: Compression of the spinal nerves can cause a feeling of weakness in the muscles of the lower extremities, which can make daily activities more difficult to perform.
- Increased pain when standing: Pressure on the spine when standing can worsen the pain associated with spondylolisthesis, which may lead to a preference for sitting or lying down.
- Pain during physical activities: Movements that involve bending forward, lifting heavy objects, or twisting the spine can worsen pain in people with spondylolisthesis.
- Spinal Instability: In severe cases of spondylolisthesis, where there is significant slippage of the vertebrae, there may be spinal instability, which can lead to difficulty maintaining a stable standing or sitting position.


Gymnasts often perform complex movements that require both flexibility and strength, leading to substantial rotational forces that can challenge the integrity of the spinal structure. Over time, repeated exposure to such torsion can increase the risk of developing spinal conditions, including disc herniation, stress fractures, and chronic back pain.
This image serves as a critical reminder of the importance of proper technique, conditioning, and awareness in gymnastics training to minimize the risk of injury from spinal torsion. It also underscores the need for ongoing research and education in sports medicine to support the health and well-being of athletes exposed to such intense physical demands.
Spondylolisthesis can happen at any age, but children and adolescents are more prone to the disease because their spines are still in development. This is why gymnasts are at risk. In fact, gymnasts are reportedly four times more likely to develop spondylolysis due to repetitive hyperflexion-hyperextension maneuvers such as turning, stooping, dismounting and flexion exercises.1-3
Pathophysiology of spondylolisthesis
The pathophysiology of spondylolisthesis involves several complex mechanisms related to the spine and surrounding structures. In the isthmic form of spondylolisthesis, a condition often associated with repetitive activities, microfractures develop in the isthmus of the vertebra, weakening its structure. These microfractures can result from excessive stress placed on the spine, such as lifting weights or participating in strenuous sporting activities. Over time, these fractures can lead to one vertebra slipping over another, exacerbating symptoms and increasing the risk of complications.
Degenerative spondylolisthesis, on the other hand, is often attributed to aging and degeneration of the intervertebral discs. As we age, the discs lose their elasticity and ability to absorb shock, leading to decreased disc height and increased spinal instability. This disc degeneration can contribute to slippage of the vertebrae by weakening the supporting structures of the spine, thereby increasing pressure on the surrounding vertebrae and joints.
In some cases, spondylolisthesis can be congenital, resulting from spinal malformations present from birth. These birth defects can affect the structure and stability of the spine, increasing the risk of vertebrae slipping as the individual ages.
The pathophysiology of traumatic spondylolisthesis is usually related to acute injuries, such as vertebral fractures caused by car accidents or falls. These traumatic injuries can cause the vertebrae to suddenly shift, disrupting the normal alignment of the spine and leading to symptoms of spondylolisthesis.
Finally, pathological spondylolisthesis can result from underlying medical conditions such as osteoporosis, infections, or tumors. These conditions weaken the bones and supporting structures of the spine, increasing the risk of vertebrae slipping and symptoms associated with spondylolisthesis.
Treatment of spondylolisthesis
Treatment for spondylolisthesis varies depending on the severity of symptoms and each patient’s individual factors. In less serious cases, conservative approaches are often favored. This may include rest and modifying activities to avoid movements that make the pain worse. Medications such as pain relievers, nonsteroidal anti-inflammatory drugs (NSAIDs), or muscle relaxants may be prescribed to relieve pain and inflammation. Physical therapy also plays an important role, with specific exercises aimed at strengthening the muscles around the spine, improving its stability. In some cases, wearing a lumbar brace may also be recommended to provide additional support to the lumbar region and relieve pain.
For more severe cases or those that do not respond to conservative treatments, surgical options may be considered. Surgery may be recommended to decompress the spinal nerves if slipping vertebrae causes severe compression and neurological symptoms, such as numbness, tingling, or muscle weakness. Another surgical option involves a spinal fusion, where unstable vertebrae are stabilized by fusing them together using bone grafts and fixation devices such as plates and screws. This procedure aims to reduce abnormal movement between the vertebrae and relieve pain associated with spondylolisthesis.
The choice of treatment will depend on several factors, including the severity of symptoms, the underlying cause of the spondylolisthesis, the age and general health of the patient. It is essential to consult a doctor or spine specialist to evaluate the available treatment options and develop a personalized treatment plan based on each patient’s specific needs.
Treatment for spondylolisthesis depends on several factors, including the severity of symptoms, the degree of slippage of the vertebrae, and the underlying cause of the condition. Here is an overview of common treatment options:
Conservative approaches
- Rest and activity modification: Avoiding activities that exacerbate pain and prioritizing rest can help relieve symptoms.
- Medications: Pain relievers, nonsteroidal anti-inflammatory drugs (NSAIDs), or muscle relaxants may be prescribed to relieve pain and inflammation.
- Physical therapy: Muscle strengthening, stretching, and spinal stabilization exercises may be recommended to strengthen the muscles around the spine and improve stability.
- Orthotics: Lumbar orthotics or support belts can help reduce pressure on the spine and relieve pain.
Corticosteroid injections
In some cases, corticosteroid injections may be given directly to the affected area to reduce inflammation and relieve pain.
Surgery
- Nerve decompression: If sliding vertebrae compress the spinal nerves and cause severe neurological symptoms, surgery to decompress the nerves may be necessary.
- Spinal Fusion: In severe cases of spondylolisthesis, where slippage of the vertebrae is significant and results in spinal instability, a spinal fusion may be recommended. This procedure involves stabilizing the spine by fusing the affected vertebrae using bone grafts and fixation devices such as plates and screws.
The choice of treatment will depend on several factors, including the severity of symptoms, the underlying cause of the spondylolisthesis, the age and general health of the patient. It is important to consult a doctor or spine specialist to obtain an accurate diagnosis and a treatment plan tailored to each individual case.
The Impact of Gymnastics on Spondylolisthesis
Gymnastics, with its graceful yet demanding movements, poses a multifaceted impact on individuals grappling with spondylolisthesis, a condition characterized by the forward displacement of one vertebra over another. In navigating this intricate relationship, gymnasts and healthcare professionals alike confront a delicate balance between the sport’s potential benefits and inherent risks. At its core, gymnastics serves as a crucible for cultivating core strength, flexibility, and overall physical fitness. Through meticulously choreographed routines and disciplined training, gymnasts harness the power of their bodies to execute feats of agility, balance, and precision. In doing so, they engage a myriad of muscles, including those supporting the spine, thus laying the groundwork for enhanced spinal stability and resilience. However, amidst the backdrop of these athletic achievements lies the looming specter of spondylolisthesis, a condition that can cast a shadow over gymnasts’ aspirations and well-being. The repetitive strain and biomechanical stresses inherent in gymnastics movements, particularly those involving spinal extension or hyperflexion, can exacerbate spondylolisthesis-related symptoms and potentially precipitate further vertebral displacement. Consequently, gymnasts with spondylolisthesis find themselves navigating a precarious terrain, where the pursuit of athletic excellence intersects with the imperative of spinal health preservation.
For gymnasts with spondylolisthesis, the journey towards balancing athletic pursuits with spinal health necessitates a nuanced and individualized approach. Collaborative partnerships between gymnasts, coaches, and healthcare professionals form the cornerstone of this endeavor, facilitating tailored training regimens and informed decision-making. Coaches assume the role of mentors and guides, imparting wisdom gleaned from years of experience while fostering an environment of open communication and mutual trust. Through their guidance, gymnasts learn to honor the signals of their bodies, discerning between discomfort borne of exertion and warning signs indicative of underlying spinal pathology. In parallel, healthcare professionals serve as vigilant guardians of gymnasts’ spinal health, offering clinical expertise, diagnostic insights, and evidence-based interventions aimed at optimizing performance while minimizing risk. Together, these stakeholders form an interconnected web of support, united in their shared commitment to nurturing the holistic well-being of gymnasts with spondylolisthesis.
In navigating the complex interplay between gymnastics and spondylolisthesis, education emerges as a potent tool for empowerment and risk mitigation. By fostering awareness of spondylolisthesis among gymnasts, coaches, and parents, educational initiatives can catalyze early detection, facilitate informed decision-making, and foster a culture of proactive spinal health management within gymnastics communities. Moreover, educational efforts extend beyond mere awareness-raising, encompassing strategies for injury prevention, proper technique execution, and adaptive training modifications tailored to the unique needs of gymnasts with spondylolisthesis. Through a combination of knowledge dissemination, skill-building, and ongoing support, educational initiatives serve as linchpins of resilience, equipping gymnasts with the tools and resources needed to navigate the challenges of their athletic journey with confidence and fortitude.
Ultimately, the impact of gymnastics on spondylolisthesis transcends the realm of physicality, extending into the realms of resilience, determination, and self-discovery. In confronting the dual imperatives of athletic excellence and spinal health preservation, gymnasts with spondylolisthesis embark on a journey fraught with challenges yet ripe with opportunity. Through unwavering commitment, collaborative partnership, and a steadfast dedication to holistic well-being, gymnasts chart a course towards realizing their full potential, embodying the indomitable spirit of the human endeavor.
Gymnastics, with its rigorous demands on the spine, can have both positive and negative impacts on individuals with spondylolisthesis, a condition characterized by the forward displacement of one vertebra over another. Here’s an overview of the potential effects:
- Strengthening and Flexibility:
- Gymnastics involves various movements that require strength, flexibility, and control of the spine and core muscles.
- Properly executed gymnastics exercises can help strengthen the muscles supporting the spine, including the abdominals, erector spinae, and deep stabilizers.
- Improved muscle strength and flexibility can potentially alleviate some of the symptoms associated with spondylolisthesis and provide better support for the spine.
- Risk of Aggravation:
- Despite the potential benefits, certain gymnastics movements may exacerbate spondylolisthesis symptoms.
- Movements that involve hyperextension or excessive loading of the lumbar spine, such as backbends, somersaults, or high-impact landings, can increase stress on the vertebrae and surrounding structures.
- Repetitive or forceful spinal movements in gymnastics routines may contribute to further vertebral slippage, spinal instability, and pain.
- Individualized Approach:
- The impact of gymnastics on spondylolisthesis varies depending on factors such as the severity of the condition, the degree of vertebral slippage, and the individual’s overall musculoskeletal health.
- It’s essential for gymnasts with spondylolisthesis to work closely with healthcare professionals, including orthopedic specialists, physical therapists, and coaches, to develop personalized training plans that accommodate their condition.
- Modifications to gymnastics routines may be necessary to minimize risk and avoid activities that exacerbate symptoms or compromise spinal stability.
- Focus on Technique and Alignment:
- Proper technique and alignment are critical for gymnasts with spondylolisthesis to reduce strain on the spine and prevent injury.
- Emphasizing core stability, neutral spine alignment, and controlled movement execution can help minimize excessive stress on the vertebrae and surrounding tissues.
- Coaches and instructors play a crucial role in providing guidance and supervision to ensure that gymnasts with spondylolisthesis perform exercises safely and effectively.
- Monitoring and Management:
- Regular monitoring of spondylolisthesis symptoms and periodic evaluation of spinal stability are essential for gymnasts participating in the sport.
- Healthcare professionals can recommend appropriate interventions, such as targeted exercises, manual therapy, bracing, or, in severe cases, surgical intervention, to manage spondylolisthesis and mitigate its impact on gymnastics performance.
- Early Detection and Prevention:
- Early detection of spondylolisthesis in gymnasts is crucial for implementing preventive measures and minimizing the risk of progression.
- Regular screening by healthcare professionals, including orthopedic specialists or sports medicine physicians, can help identify potential spinal abnormalities and address them proactively.
- Education and Awareness:
- Educating gymnasts, coaches, and parents about the signs and symptoms of spondylolisthesis is essential for promoting early recognition and appropriate management.
- Increasing awareness of the potential risks associated with certain gymnastics movements can empower athletes to communicate any discomfort or concerns to their healthcare providers promptly.
- Cross-Training and Injury Prevention:
- Incorporating cross-training activities into gymnastics programs can help reduce overuse injuries and provide opportunities for rest and recovery.
- Low-impact exercises such as swimming, cycling, or Pilates can complement gymnastics training while minimizing stress on the spine and supporting overall musculoskeletal health.
- Individualized Rehabilitation:
- For gymnasts who develop spondylolisthesis-related symptoms or injuries, individualized rehabilitation programs are essential for promoting recovery and minimizing recurrence.
- Physical therapy interventions focusing on core stabilization, flexibility, and proprioception can help address muscle imbalances, improve spinal alignment, and enhance overall functional performance.
- Psychosocial Support:
- Coping with a spinal condition such as spondylolisthesis can have psychosocial implications for gymnasts, including stress, anxiety, or fear of reinjury.
- Providing psychosocial support and resources, such as counseling or peer support groups, can help gymnasts navigate the emotional challenges associated with managing a chronic musculoskeletal condition.
- Long-Term Monitoring and Management:
- Spondylolisthesis is a chronic condition that requires long-term monitoring and management, especially for athletes engaged in high-impact sports like gymnastics.
- Regular follow-up appointments with healthcare providers and periodic imaging studies may be necessary to track the progression of spondylolisthesis and adjust treatment plans accordingly.
Safe Practices and Considerations for Gymnastics with Spondylolisthesis
Safe practices and considerations are paramount for gymnasts with spondylolisthesis to ensure their well-being and longevity in the sport. Prior to engaging in gymnastics, comprehensive medical evaluation and clearance by a healthcare professional, preferably an orthopedic specialist or sports medicine physician, are essential to assess the severity of the condition, degree of vertebral slippage, presence of symptoms, and overall spinal health. Individualized training programs must be developed, tailored to the specific needs and limitations of gymnasts with spondylolisthesis, with modifications to routines to avoid movements that exacerbate spinal stress or risk further vertebral displacement. Emphasizing proper technique and alignment is crucial, prioritizing neutral spine alignment, avoiding excessive spinal extension or flexion, and engaging core muscles for stability and support. A gradual progression of gymnastics skills and exercises, along with close monitoring for signs of discomfort, pain, or worsening symptoms during training sessions, is imperative. Thorough warm-up and cool-down routines should be incorporated, including dynamic stretching, mobility exercises, and foam rolling, to prepare the body for exercise and promote recovery. Cross-training activities, such as swimming, yoga, or Pilates, should complement gymnastics training to reduce the risk of overuse injuries, and regular rest days should be scheduled to allow for recovery and prevent excessive fatigue or strain on the spine. Open communication between gymnasts, coaches, parents, and healthcare providers is essential to address concerns or changes in symptoms related to spondylolisthesis, empowering gymnasts to advocate for their own health and well-being. Regular follow-up appointments with healthcare providers are necessary to monitor the progression of spondylolisthesis and evaluate the effectiveness of treatment and management strategies, adjusting training programs and interventions as needed based on changes in symptoms or imaging findings. By adhering to these safe practices and considerations, gymnasts with spondylolisthesis can enjoy the physical and mental benefits of gymnastics while minimizing the risk of exacerbating their condition and promoting long-term spinal health and athletic success.
Here are key guidelines and recommendations:
- Medical Evaluation and Clearance:
- Before engaging in gymnastics, gymnasts with spondylolisthesis should undergo a comprehensive medical evaluation by a healthcare professional, preferably an orthopedic specialist or sports medicine physician.
- Clearance for participation should be based on the severity of the condition, degree of vertebral slippage, presence of symptoms, and overall spinal health.
- Individualized Training Programs:
- Develop individualized training programs tailored to the specific needs and limitations of gymnasts with spondylolisthesis.
- Modify gymnastics routines to avoid movements that exacerbate spinal stress or risk further vertebral displacement.
- Focus on strengthening core muscles, improving flexibility, and promoting proper body mechanics to support spinal stability.
- Emphasis on Proper Technique:
- Prioritize proper technique and alignment in gymnastics movements to minimize strain on the spine.
- Educate gymnasts on the importance of maintaining neutral spine alignment, avoiding excessive spinal extension or flexion, and engaging core muscles for stability and support.
- Gradual Progression and Monitoring:
- Implement a gradual progression of gymnastics skills and exercises, allowing gymnasts to build strength, flexibility, and skill proficiency over time.
- Monitor gymnasts closely for signs of discomfort, pain, or worsening symptoms during training sessions, and adjust activities accordingly.
- Warm-up and Cool-down Routines:
- Incorporate thorough warm-up and cool-down routines into gymnastics sessions to prepare the body for exercise and promote recovery.
- Include dynamic stretching, mobility exercises, and foam rolling to enhance flexibility, circulation, and muscle relaxation.
- Cross-Training and Rest Days:
- Encourage cross-training activities, such as swimming, yoga, or Pilates, to complement gymnastics training and reduce the risk of overuse injuries.
- Schedule regular rest days to allow for recovery and prevent excessive fatigue or strain on the spine.
- Open Communication and Advocacy:
- Foster open communication between gymnasts, coaches, parents, and healthcare providers regarding any concerns or changes in symptoms related to spondylolisthesis.
- Empower gymnasts to advocate for their own health and well-being by communicating their needs and limitations to coaches and teammates.
- Regular Follow-up and Evaluation:
- Schedule regular follow-up appointments with healthcare providers to monitor the progression of spondylolisthesis and evaluate the effectiveness of treatment and management strategies.
- Adjust training programs and interventions as needed based on changes in symptoms or imaging findings.
Conclusion
In conclusion, treatment of spondylolisthesis is an individualized approach based on symptom severity, underlying cause, and patient preference. Treatment options range from conservative approaches such as rest, physical therapy and medication, to surgical interventions such as nerve decompression and spinal fusion. The primary goal of treatment is to relieve pain, restore functionality, and improve the patient’s quality of life. It is crucial to consult a healthcare professional for an accurate diagnosis and a treatment plan tailored to each individual case. With proper treatment and management, many patients with spondylolisthesis can regain significant relief from their symptoms and return to daily activities with greater comfort and mobility.
Reference
- Cohen M, Abdalla J.R. Lesões nos esportes. Diagnóstico prevenção e tratamento. Revinter; São Paulo: 2002. Ginástica olímpica; pp. 776–784. [Google Scholar]
- Garcés GL, González-Montoro I, Rasines L.J., Santoja F. Early diagnosis of stress facture of the lumbar spine in athletes. Int Orthop. 1999;23(4):213–215. [PMC free article] [PubMed] [Google Scholar]
- Kolt GS, Kirkby RJ. Epidemiology of injury in elite and subelite female gymnasts: a comparison of retrospective and prospective findings. Br J Sports Med. 1999;33(5):312–318. [PMC free article] [PubMed] [Google Scholar]
- Tertti M, Paajanen H, Kujala UM, Alanen A, Salmi TT, Kormano M. Disc degeneration in young gymnasts. A magnetic resonance imaging study. Am J Sports Med. 1990;18(2):206–208. [PubMed] [Google Scholar]
- Dixon M, Fricker P. Injuries to elite gymnasts over 10 yr. Med Sci Sports Exerc. 1993;25(12):1322–1329. [PubMed] [Google Scholar]
- Garrick James G, Requa Ralph K. Epidemiology of women’s gymnastics injuries. Am J Sports Med. 1980;8(4):261–264. [PubMed] [Google Scholar]
- Pettrone FA, Ricciardelli E. Gymnastic injuries: the Virginia experience 19821983. Am J Sports Med. 1987;15(1):59–62. [PubMed] [Google Scholar]
- Snook GA. Injuries in women’s gimnastics. Am J Sports Med. 1979;7(4):242–244. [PubMed] [Google Scholar]
- Bozdech Z, Dufek P. Spondylolisthesis in young gymnasts. Acta Univ Carol Med (Praha) 1986;32(5-6):405–409. [PubMed] [Google Scholar]
- Ibarra AG, Miñarro PAL. Espondilolisis y espondilolistesis en la práctica físico-deportiva. Revista digital- Buenos Aires [periódico na internet] 2003 [citado Jan 2003; 8(56)]. Disponível em
- Cassidy RC, Shaffer WO, Johnson DL. Spondylolysis and spondylolisthesis in the athlete. Orthopedics. 2005;28(11):1331–1333. [PubMed] [Google Scholar]
- Standaert CJ. Spondylolysis in the adolescent athlete. Clin J Sports Med. 2002;12(2):119–122. [PubMed] [Google Scholar]
- Lowry C Benton, Leveau Barney F. A retrospective study of gymnastics injuries to competitors and noncompetitors in private clubs. Am J Sports Med. 1982;10(4):237–239. [PubMed] [Google Scholar]
- Baker DR, McHollick W. Spondylolysis and spondylolisthesis in children. J Bone Joint Surg Am. 1978;38:933–934. [Google Scholar]
- Frederickson BE, Baker D, McHolick WJ, Hansen AY, Luubicky JP. The natural history of spondylolysis and spondylolistesis. J Bone Joint Surg. 1984;66(5):699707. [PubMed] [Google Scholar]
- Stewart TD. The age incidence of neural arch defects in Alaska natives, considered from standpoint of etiology. J Bone Joint Surg Am. 1953;35(4):935–950. [PubMed] [Google Scholar]







{kind=link}