



Introduction
Lumbar lordosis is a term used to describe the natural inward curvature of the lumbar spine, which is the lower portion of the vertebral column located in the lower back. This curvature is essential for maintaining balance, absorbing shock, and allowing for flexibility and movement in the lower back region. Lumbar lordosis helps distribute body weight evenly along the spine, reducing the risk of injury and strain.
The lumbar spine normally has a slight lordotic curve, which is more pronounced in some individuals than in others. This curvature is formed by the shape of the vertebrae, the intervertebral discs, and the surrounding ligaments and muscles. In a healthy spine, the lordotic curve is balanced and aligned, providing stability and support for the upper body and pelvis.
However, abnormalities or excessive curvature of the lumbar lordosis can lead to various issues and discomfort. Hyperlordosis, or excessive inward curvature of the lumbar spine, can result in lower back pain, muscle tightness, and postural problems. It may be caused by factors such as poor posture, muscle imbalances, obesity, pregnancy, or certain medical conditions such as spondylolisthesis or osteoporosis.
Conversely, hypolordosis, or a reduction in the normal lumbar curvature, can also cause problems. It may lead to decreased flexibility, limited range of motion, and increased pressure on the spinal discs and joints. Hypolordosis is often associated with conditions such as flatback syndrome, ankylosing spondylitis, or degenerative disc disease.
Treatment for abnormal lumbar lordosis depends on the underlying cause and severity of the condition. For hyperlordosis caused by muscle imbalances or poor posture, physical therapy exercises focusing on strengthening the core muscles and stretching tight muscles can help correct the curvature and alleviate symptoms. Weight management, ergonomic adjustments, and lifestyle modifications may also be recommended to reduce strain on the lower back.
The Evolution of Lumbar Lordosis: Key to Human Bipedalism
Lumbar lordosis, this natural curve of the spine, played a fundamental role in the evolution of humans towards bipedalism. Even before hyperlordosis was a concern, lumbar lordosis was crucial to our ability to walk upright.

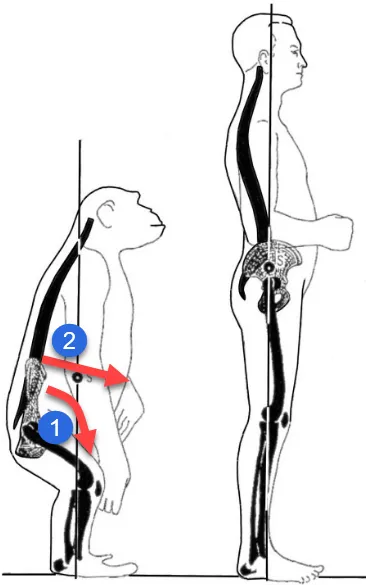
When our ancestors evolved to adopt a bipedal posture, the spine underwent notable adaptations to support this new way of moving. The natural curve in the lumbar region was essential for maintaining balance, distributing body weight efficiently, and enabling stable bipedal locomotion.
This curvature allowed the spine to act as a spring, absorbing shock while walking and contributing to the agility needed for hunting and avoiding predators. Lumbar lordosis has therefore been an evolutionary advantage, favoring the survival and success of our species.
However, in our modern lifestyle this curvature can sometimes become excessive, leading to problems such as hyperlordosis. It is essential to understand the line between healthy and excessive curvature, because too much lumbar lordosis can lead to orthopedic complications.
By exploring the evolution of lumbar lordosis, we can better understand how our anatomy adapted to allow us to become agile bipeds. At the same time, it highlights the importance of maintaining balance in our posture to prevent spine-related health problems in our modern life.
The Evolution of lumbar lordosis: Impact of Sedentary Lifestyle on Human Posture
The appearance of hyperlordosis, excessive curvature of the spine in the lumbar region, could be attributed to significant changes in the lifestyle of modern man. If we go back in time, our ancestors adopted a natural bipedal posture, with a lumbar lordosis adapted to walking and running.
However, with the advent of an increasingly sedentary society, marked by a reduction in physical activities, the impact on human posture has been significant. Less effort when running, excess weight and a less active lifestyle can contribute to an increase in lumbar curvature.
Reducing physical activity weakens the muscles that support the spine, especially those in the lumbar region. At the same time, excess weight placed on the spine can accentuate the natural curvature, possibly leading to hyperlordosis.
This change in muscle dynamics and imbalance caused by a sedentary lifestyle can create excessive strain on the spine. Weakened lower back muscles and excess weight can contribute to increased curvature, creating the conditions for hyperlordosis.
Thus, by examining the implications of sedentary lifestyle on human posture, we can better understand how modern factors may contribute to orthopedic problems such as hyperlordosis.
Before lumbar lordosis
Lumbar lordosis is a normal curvature of the spine found in the lower back region, at the level of the lumbar vertebrae. This curvature has several important functions for the human body:
- Shock absorption: Lumbar lordosis acts as a natural shock absorber, absorbing shock and forces placed on the spine during movement, walking or other physical activities.
- Stability and support: The lumbar curvature contributes to the stability of the spine by evenly distributing the weight of the body across the vertebrae. This helps maintain balance while providing structural support.
- Facilitation of movements: Lumbar lordosis promotes mobility of the trunk and hips, thus allowing a greater range of movement. This is essential for activities such as flexion, extension and rotation of the body.
- Alignment with Gravity: The lumbar curvature helps align the spine with gravity, which is crucial for maintaining an effective standing posture.
Lumbar lordosis is present in early childhood and develops further as the child learns to stand and walk. It is generally considered a normal feature of the spine. However, conditions such as hyperlordosis (an excessive inward curvature) or hypolordosis (a reduced curvature) can sometimes cause problems and require special attention, especially if pain or functional limitations are present.
Causes of lumbar lordosis
- Poor Postures: Improper postural habits, such as sitting or standing incorrectly, can contribute to excessive lordosis over time.
- Obesity: Excess weight, especially around the abdominal region, can cause the body’s center of gravity to shift, thereby influencing the curvature of the spine.
- Pregnancy: During pregnancy, extra weight in the abdominal area can lead to increased lordosis in some women. Hormonal changes associated with pregnancy can also influence joint stability.
- Muscle Imbalance: An imbalance between the abdominal muscles and the back muscles can lead to excessive lordosis. Weak abdominal muscles and tight back muscles can contribute to this condition.
- Genetic Conditions: Some individuals may be genetically predisposed to developing excessive lordosis due to specific anatomical characteristics of their spine.
- Neurological Diseases: Conditions such as polio, muscular dystrophy or other neurological diseases can affect muscles and nerves, leading to excessive lordosis.
- Trauma: Injuries or trauma to the spine can alter the natural curvature of the spine, leading to excessive lordosis.
- Myopathies: Certain muscular diseases can affect the tone of the muscles that support the spine, thus contributing to excessive lordosis.
- Congenital Anomalies: Congenital anomalies of the spine can cause excessive curvature. These conditions can be present from birth.
- Spondylolisthesis: This is a condition where one vertebra slips forward relative to the vertebra below it, which can contribute to excessive lordosis.
- Spinal Arthritis: Inflammatory conditions such as ankylosing spondylitis can affect the joints of the spine, leading to postural changes including excessive lordosis.
Symptoms of lumbar hyperlordosis
The symptoms of lumbar hyperlordosis are diverse and may include pain in the lumbar region, accompanied by discomfort or pain in the hip area due to the anterior tilt of the pelvis. This condition can also influence posture, manifesting itself as an accentuated curvature and sometimes leading to muscle stiffness. Mobility may be reduced, and muscle fatigue may occur due to the constant effort required to maintain proper posture. In more severe cases, hyperlordosis can even lead to respiratory complications, highlighting the importance of early management and treatment of this condition. A consultation with a healthcare professional, such as an osteopath, is recommended for a thorough assessment and recommendations tailored to each specific case.
- Lower Back Pain: Pain in the lumbar region is one of the most common symptoms of hyperlordosis. This pain can be chronic and increase with physical activity.
- Discomfort: People with hyperlordosis may experience general discomfort in the lumbar region due to excessive curvature of the spine.
- Muscle Fatigue: Back muscles can fatigue more quickly due to increased tension caused by excessive lordosis.
- Limited Movements: Some individuals may have difficulty performing certain movements, such as bending forward, due to excessive curvature of the spine.
- Respiratory Problems: In severe cases of hyperlordosis, excessive curvature can affect the chest space, potentially lead to compression of internal organs, and cause breathing problems.
- Posture Alterations: Excessive lordosis can lead to noticeable changes in posture, such as a protruding buttocks or an accentuated curvature of the lower back.
- Neuralgia Sensations: In some cases, excessive lordosis can put pressure on the nerves in the spine, causing neuralgia sensations in the legs.
- Digestive Problems: In severe cases, hyperlordosis can affect the abdominal area, potentially leading to digestive problems.
Pathophysiology of lumbar lordosis
Lumbar hyperlordosis is a condition characterized by excessive curvature of the lumbar region of the spine. Its pathophysiology involves a series of factors. Most of the time, it is linked to a muscular imbalance between the hip flexor muscles and the trunk extensor muscles.
Weakening of the abdominal muscles, combined with shortening of the hip flexors and lumbar muscles, can contribute to an anterior tilt of the pelvis, thereby accentuating the lumbar curvature. Postural imbalances and inappropriate movement habits can also play a crucial role.
Underlying causes of hyperlordosis include genetic factors, previous injuries, medical conditions such as spondylolisthesis, and sometimes neurological disorders. Pregnancy in women may also be associated with temporary hyperlordosis due to hormonal changes and weight redistribution.
- Abnormal Curvature: Hyperlordosis manifests as excessive curvature of the spine in an anterior (forward) direction. Under normal circumstances, the spine has natural curvatures that contribute to stability and mobility.
- Muscle Imbalance: An imbalance between the muscles of the back, abdominals and hips can contribute to hyperlordosis. Weak abdominal muscles combined with tight back muscles can lead to excessive pelvic tilt, contributing to increased lumbar curvature.
- Ligament Tension: The ligaments that support the spine can experience excessive strain due to increased curvature. This can lead to spinal instability and contribute to the progression of hyperlordosis.
- Modification of Natural Curvatures: Normal curvatures of the spine include lumbar lordosis and thoracic kyphosis (backwards curvature). Hyperlordosis can alter these natural curvatures, leading to abnormal posture.
- Genetic Factors: Some people may be genetically predisposed to developing excessive lordosis due to specific anatomical characteristics of their spine.
- Obesity: Excess weight, especially around the abdominal region, can shift the body’s center of gravity and contribute to increased lordosis.
- Pregnancy: During pregnancy, extra weight in the abdominal area can lead to increased lordosis in some women. Hormonal changes associated with pregnancy can also influence joint stability.
- Trauma or Injuries: Trauma, injuries, or previous surgeries can change the structure of the spine, contributing to hyperlordosis.
- Neurological Conditions: Certain neurological conditions, such as polio, muscular dystrophy, or other diseases affecting the muscles and nerves, may contribute to excessive lordosis.
Biomechanics
The muscle biomechanics of hyperlordosis involve changes in spinal alignment and changes in the forces exerted on muscle and joint structures. Here is a detailed explanation of the biomechanics associated with hyperlordosis:
- Psoas and Pelvic Tilt: Hyperlordosis is often associated with an anterior tilt of the pelvis. The psoas muscle, located in the lumbar region and attached to the femur, can play a key role in this shift. A tight psoas can pull the pelvis forward, contributing to excessive curvature of the lumbar spine.
- Piriformis and Pelvic Rotation: The piriformis, a deep muscle in the pelvic region, may also be involved. Its action on hip rotation can influence the position of the pelvis. Excessive rotation of the pelvis can worsen hyperlordosis.
- Change in Point of Gravity: Hyperlordosis shifts the body’s center of gravity forward. This can create increased load on the lower back muscles and joints of the spine, increasing stress on these structures.
- Formation of Dorsal Kyphosis: To compensate for the increased curvature in the lumbar region, some people with hyperlordosis develop dorsal kyphosis (backwards curvature) at the thoracic level. This helps maintain postural balance.
- Lumbar Facets and Premature Wear: The facet joints between the lumbar vertebrae may be subjected to uneven pressure due to hyperlordosis. This can lead to premature wear of joint surfaces, increasing the risk of degenerative spinal disorders.
- Disc Compression: Hyperlordosis can lead to compression of the intervertebral discs. Constant compression can contribute to disc degeneration and, in some cases, disc herniation.
- Nerve Root Compression: Advanced disc degeneration associated with hyperlordosis can compress the nerve roots emerging from the spine. This can lead to symptoms such as radicular pain, numbness, or weakness in the lower extremities.
- Discomfort in the Legs: Due to compression of the nerve roots, feelings of discomfort, pain or numbness may spread down the lower extremities.
Lumbar lordosis prevention
Prevention of hyperlordosis is essential to maintaining optimal spinal health. Here are some tips and preventive practices:
- Maintaining Good Posture: Encourage patients to use correct posture when sitting, standing, and even walking. This includes maintaining the natural curvature of the spine.
- Muscle-strengthening exercises: Targeted exercises to strengthen the core muscles, particularly the abdominals and lower back muscles, can help stabilize the spine and prevent hyperlordosis.
- Regular stretching: Encourage regular stretching to maintain muscle and joint flexibility. This can help prevent stiffness and muscle imbalances.
- Weight Management: Maintaining a healthy body weight is crucial, as excess weight can put additional strain on the spine, contributing to the development of hyperlordosis.
- Ergonomics at work: Advise on the importance of good ergonomics at work to avoid prolonged sitting and encourage regular breaks to move.
Case studies :
Case study: Isabelle, 40 years old
Journey: Isabelle, a teacher in Quebec, consulted an osteopath due to persistent lower back pain and difficulty maintaining a comfortable posture in class.
Treatment methods: After a thorough assessment, the osteopath identified imbalances in Isabelle’s lumbar region, contributing to her hyperlordosis. The osteopathic-exclusive treatment plan included gentle mobilizations to restore spinal alignment, myofascial release techniques to release muscle tension, and advice on daily postural adjustments.
Results: Over the course of the osteopathy sessions, Isabelle felt a gradual improvement in her lower back pain. The manipulations and release techniques helped reduce pressure on his spine, improving his posture. Isabelle also learned specific exercises recommended by the osteopath to strengthen her muscles and maintain the gains obtained.
Isabelle’s story highlights osteopathy’s ability to successfully treat hyperlordosis using specific manual techniques and a personalized approach. The collaboration between the osteopath and the patient played a crucial role in obtaining positive results.
Self-management tips
- Abdominal strengthening exercises: Regularly practice exercises targeting the abdominal muscles, such as crunches and planks, to strengthen the core region and stabilize the spine.
- Lower back muscle stretches: Incorporate specific stretches for the lower back muscles, such as psoas muscle stretches, to promote flexibility and relieve tension.
- Strengthening the back muscles: Include strengthening exercises for the back muscles, such as back extensions, to balance muscle strength between the front and back of the trunk.
- Maintaining a good sitting posture: Adopt a correct sitting posture by maintaining the natural curvature of the spine. Use a lumbar cushion if necessary to support the lumbar region.
- Break and Stretch at Work: Take regular breaks at work to stand, stretch, and change positions. This helps prevent muscle fatigue and improve circulation.
- Using lumbar support: If you spend a lot of time sitting, use appropriate lumbar support on your chair to maintain the natural curvature of the spine.
- Maintaining a healthy body weight: Adopt a healthy lifestyle with a balanced diet and regular exercise to maintain an optimal body weight, thereby reducing pressure on the spine.
- Postural education: Learn about good postural practices in different daily activities, such as lifting objects, to avoid excessive pressure on the spine.
- Relaxation exercises: Practice relaxation exercises, such as meditation or deep breathing, to reduce stress and muscle tension.
- Regular consultations with a healthcare professional: Schedule regular consultations with an osteopath to assess your posture and receive personalized advice on managing hyperlordosis.
Stretches and exercises
Stretching
- Stretching the psoas muscle:
- Get on your knees on the floor.
- Step one leg forward while keeping the other bent behind you.
- Tilt your pelvis slightly forward until you feel a stretch in your hip area.
- Hip flexor stretch:
- Sit on the floor with your legs extended.
- Bend one leg and place the foot on the inner thigh of the other leg.
- Lean your upper body slightly forward, keeping your back straight.
- Étirement du quadratus lumborum :
- Sit in a chair with your back straight.
- Lean slightly to one side, bringing the ear towards the shoulder, to stretch the muscles on the side of the spine.
Strengthening exercises
- Plank :
- Assume a push-up position with your arms straight.
- Maintain the position by contracting your abdominal muscles and keeping your back straight. Start with short intervals and gradually increase the duration.
- Extensions two:
- Lie face down on the floor.
- Gently lift your chest off the floor using your lower back muscles. Hold the position for a few seconds.
- Lying leg raises:
- Lie on your back with your arms at your sides.
- Raise both legs toward the ceiling, contracting your abdominal muscles, then slowly lower back down.
- Reverse crunches:
- Lie on your back with your legs bent at 90 degrees.
- Lift your lower back off the floor by contracting your abs, bringing your knees closer to your chest.
- Candle exercise (against a wall):
- Lie on your back with your buttocks against the wall.
- Raise your legs along the wall, keeping your lower back flat on the floor. This strengthens the abdominal and back muscles.
Postural assessment
- Slight plantar flexion of the ankle possible.
- Slight hyperextension of the knee possible.
- Hip flexion
- Bilateral anterior pelvic tilt in hyperlordosis is greater than 10 degrees in women and greater than 5 degrees in men.
- Lumbar lordotic curve is increased.
- Compensatory hyperkyphosis
- Forward head posture.


Questionnaire 1
- What is hyperlordosis and how is it characterized?
- a) An accentuated curvature of the cervical region
- b) An accentuated curvature of the thoracic region
- c) An accentuated curvature of the lumbar region
- d) An accentuated curvature of the sacral region
- How important is lumbar lordosis in human evolution?
- a) She did not play a significant role
- b) It contributed to human bipedalism
- c) It caused posture problems
- d) It caused lower back pain
- How did lumbar lordosis benefit our ancestors?
- a) By making walking difficult
- b) By absorbing shocks while walking
- c) By limiting trunk mobility
- d) By causing respiratory problems
- What modern factors can contribute to hyperlordosis?
- a) A natural bipedal posture
- b) An increase in physical activity
- c) A sedentary lifestyle and being overweight
- d) Adaptation to natural conditions
- What are the possible causes of hyperlordosis?
- a) Correct posture
- b) Strong abdominal muscles
- c) Genetic conditions, trauma, and muscular imbalances
- d) Regular physical activity
Symptoms and Pathophysiology
- What are the common symptoms of lumbar hyperlordosis?
- a) Pain in the cervical region
- b) Pain in the shoulders
- c) Pain in the lumbar region, discomfort, muscle fatigue, alterations in posture
- d) Abdominal pain
- What primarily contributes to anterior pelvic tilt in hyperlordosis?
- a) Weakening of the back muscles
- b) Contracture du muscle psoas
- c) Atrophy of the abdominal muscles
- d) Stiffness of the muscles of the lower limbs
- How can hyperlordosis affect the intervertebral discs?
- a) By strengthening them
- b) By compressing them, contributing to degeneration
- c) By isolating them from the rest of the spine
- d) By making them more flexible
Prevention and Self-management Tips
- What tips are recommended for the prevention of hyperlordosis?
- a) Maintaining poor posture
- b) Avoidance of stretching
- c) Weight management, muscle strengthening exercises, and maintaining good posture
- d) Ignoring early signs
Case Study and Conclusion
- What treatment method was used successfully in Isabelle’s case study?
- a) Surgery
- b) Medication
- c) Exclusive approach to osteopathy
- d) No treatment was applied
Answers:
- c) An accentuated curvature of the lumbar region
- b) It contributed to human bipedalism
- b) By absorbing shocks while walking
- c) A sedentary lifestyle and being overweight
- c) Genetic conditions, trauma, and muscular imbalances
- c) Pain in the lumbar region, discomfort, muscle fatigue, alterations in posture
- b) Contracture du muscle psoas
- b) By compressing them, contributing to degeneration
- c) Weight management, muscle strengthening exercises, and maintaining good posture
- c) Exclusive approach to osteopathy
References
- Been E, Kalichman L. Lumbar lordosis. Spine J. 2014; 14(1): 87–97. 10.1016/j.spinee.2013.07.464 [PubMed] [CrossRef] [Google Scholar]
- Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am . 2005; 87: 260–267. [ PubMed ] [ Google Scholar
- Vrtovec T, Likar B, Pernus F. Quantitative analysis of spinal curvature in 3D: Application to CT images of normal spine. Phys Med Biol. 2008; 53: 1895–1908. 10.1088/0031-9155/53/7/006 [PubMed] [CrossRef] [Google Scholar]
- Cobb J. Outline for the study of scoliosis. Amer Acad Orthop Surg Instructional Course Lectures. 1948; 5:261–275. [Google Scholar]
- Harrison DE, Harrison DD, Cailliet R, Janik T, Holland B. Radiographic analysis of lumbar lordosis: Centroid, Cobb, TRALL, and Harrison posterior tangent methods. Spine. 2001; 26: E235–E242. [PubMed] [Google Scholar]
- Voutsinas S, MacEwen G. Sagittal profiles of the spine. Clin Orthopaed Related Res. 1986; 210: 235–242. [PubMed] [Google Scholar]
- Hicks G, George S, Nevitt M, Cauley J, Vogt M. Measurement of lumbar lordosis: Inter-rater reliability, minimum detectable change and longitudinal variation. J Spinal Disord. 2006; 19: 501–506. [PubMed] [Google Scholar]
- Polly D, Kilkelly F, McHale K, Asplund L, Mulligan M, Chang A. Measurement of lumbar lordosis: Evaluation of intraobserver, interobserver, and technique variability. Spine. 1996; 21:1530–1535. [PubMed] [Google Scholar]
- Norton BJ, Sahrmann SA, Van Dillen LR. Differences in measurements of lumbar curvature related to gender and low back pain. J Orthopaed Sports Phys Therapy. 2004; 34: 524–534. [PubMed] [Google Scholar]
- Korovessis PG, Stamatakis MV, Baikousis AG. Reciprocal angulation of vertebral bodies in the sagittal plane in an asymptomatic Greek population Spine. 1998; 23: 700–704. [PubMed] [Google Scholar]
- Janssen MM, Drevelle X, Humbert L, Skalli W, Castelein RM. Differences in male and female spino-pelvic alignment in asymptomatic young adults: a three-dimensional analysis using upright low-dose digital biplanar X-rays. Spine. 2009; 34: E826–E832. 10.1097/BRS.0b013e3181a9fd85 [PubMed] [CrossRef] [Google Scholar]
- Kim H, Kim HS, Moon ES, Yoon CS, Chung TS, Song HT, et al. Scoliosis imaging: what radiologists should know. Radiographics. 2010; 30: 1823–42. 10.1148/rg.307105061 [PubMed] [CrossRef] [Google Scholar]
- Rangayyan RM, Deglint HJ, Boag GS. Method for the automatic detection and segmentation of the spinal canal in CT images. J Electron Imaging. 2006; 15: 033007 10.1117/1.2234770 [CrossRef] [Google Scholar]
- Klinder T, Ostermann J, Ehm M, Franz A, Kneser R, Lorenz C. Automated model-based vertebra detection, identification, and segmentation in CT images. Med Image Anal. 2009; 13: 471–482. 10.1016/j.media.2009.02.004 [PubMed] [CrossRef] [Google Scholar]
- McInerney T, Terzopoulos D. Deformable models in medical image analysis: A survey. Med Image Anal. 1996; 1: 91–108. [PubMed] [Google Scholar]
- Andrews J, Sethian J. Fast marching methods for the continuous traveling salesman problem. Proc Nat Acad Sci 2007; 104: 1118–1123. [PMC free article] [PubMed] [Google Scholar]
- Perneger TV. What is wrong with Bonferroni adjustments. Br Med J. 1998; 136: 1236–1238. [PMC free article] [PubMed] [Google Scholar]
- Sankoh AJ, Huque MF, Dubey SD. Some comments on frequently used multiple endpoint adjustments methods in clinical trials. Stat Med. 1997; 16: 2529–2542. [PubMed] [Google Scholar]







{kind=link}