



Tommy John Ulnar Collateral Ligament Injury, a term now famous in the sports world, has its origins in the demanding field of professional baseball.
Introduction
This condition, named after baseball player Tommy John who was the first to undergo surgery for the injury in 1974, presents a significant challenge for athletes, particularly baseball pitchers.
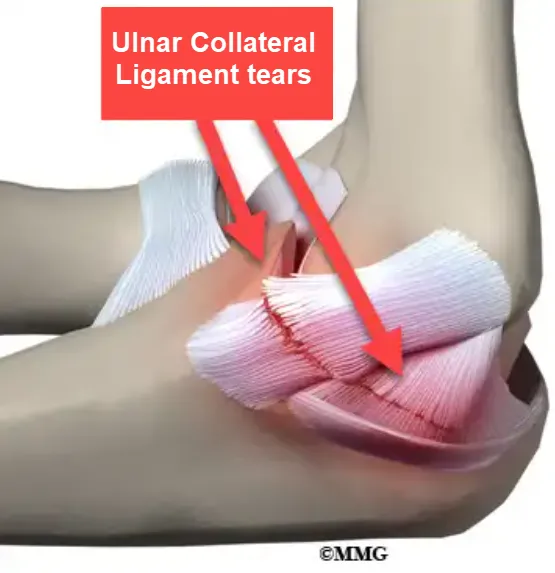
The ulnar collateral ligament (UCL) is a crucial structure for elbow stability, and it is subjected to extreme forces during the repetitive throwing movements characteristic of baseball. This injury is not limited to the world of professional sport; it also affects amateur athletes and individuals practicing activities involving repetitive arm movements.
Symptoms of UCL injury include persistent pain on the inside of the elbow, decreased grip strength, joint instability, and impaired performance during throwing. These aren’t just numbers in baseball statistics; these are athletes whose careers and passion are jeopardized by this debilitating injury.
However, there is hope for recovery through UCL reconstruction surgery, commonly known as Tommy John surgery. This intervention, which has evolved since its introduction, has enabled many athletes to return to competition after periods of intensive rehabilitation.
While Tommy John surgery has revolutionized the way athletes manage this injury, prevention remains an essential component. Understanding the underlying biomechanical mechanisms of this injury, as well as implementing appropriate training techniques, are crucial elements in minimizing the risk of UCL injuries.
This exploration of the Tommy John ulnar collateral ligament injury provides an in-depth look at the challenges faced by athletes and the medical advances that have transformed how we approach and treat this delicate condition.

Baseball pitchers are at high risk for ulnar collateral ligament (UCL) injuries due to the repetitive and forceful motions of throwing. The extreme stress placed on the elbow joint during pitching can cause tears or strains in the UCL, leading to pain, instability, and decreased throwing performance. Over time, this repetitive stress may result in chronic elbow pain and necessitate surgical intervention, such as Tommy John surgery, to repair or replace the damaged ligament. Proper throwing mechanics, strength training, and adequate rest are crucial in preventing UCL injuries and maintaining elbow health.
Anatomy of the ulnar collateral ligament (UCL)
The ulnar collateral ligament (UCL) is a crucial anatomical structure located in the elbow joint, playing a critical role in the stability and function of this complex joint. This detailed exploration of the anatomy of the UCL highlights its components, its attachment, and its fundamental role in maintaining the integrity of the elbow.
LCU Components
The ulnar collateral ligament consists of three main parts:
- Anterior bundle: Located on the anterior side of the elbow, it is the most important in terms of stability.
- Posterior bundle: Positioned on the posterior side, it provides additional support.
- Transverse band (transverse bundle): Connected to the other two bands, it contributes to the cohesion of the ligament.
Attachment of the LCU
The ulnar collateral ligament attaches to different parts of the ulnar bone, as well as to the inner part of the epitrochlea, a bony protrusion at the end of the femur.
Role of the LCU in the Elbow
- Joint Stability: The UCL plays a crucial role in elbow stability by preventing excessive lateral movement.
- Restriction of Extension: It helps to restrict excessive extension of the elbow, ensuring a controlled range of motion.
- Support during rotational movements: The UCL provides essential support during rotational movements of the elbow, such as pronation and supination.
Ulnar collateral ligament (UCL) injuries continue to be a major source of morbidity in baseball players. In fact, 25% of all professional pitchers have undergone at least one LUC reconstruction of the elbow. The throwing motion creates extreme levels of valgus stress on the medial elbow, putting these athletes at high risk for UCL injury. Incidence of injuries continues to rise at an alarming rate, particularly among adolescent baseball pitchers
Biomechanics of ulnar collateral ligament (UCL) injury
The biomechanics of an ulnar collateral ligament (UCL) injury of the elbow typically involves overloading or excessive stress on the ligament, leading to changes in the normal forces and motion of the elbow joint. Here is a biomechanical perspective of this injury:
- Elbow Movements: The elbow is a complex joint that allows for several types of movements, including flexion, extension, pronation and supination. These movements are controlled by the coordination of muscles, tendons and ligaments around the joint.
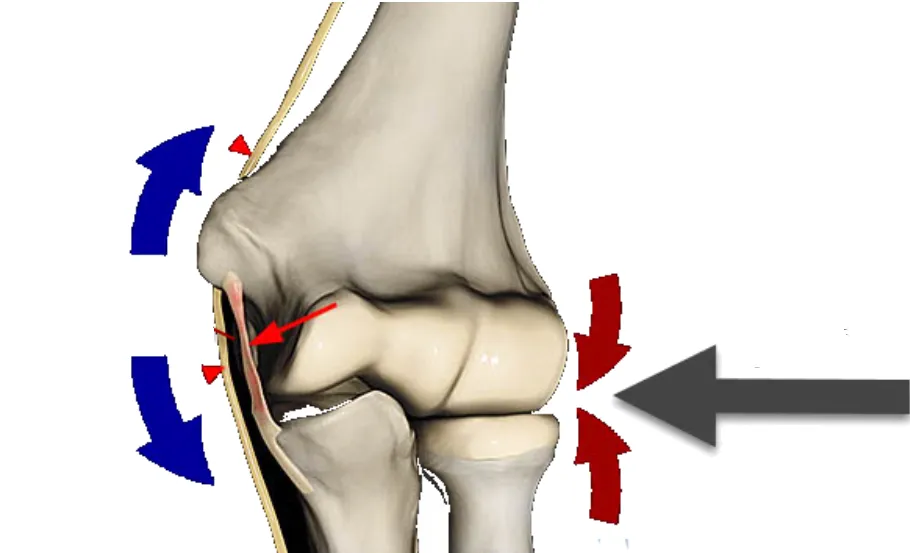
- Role of the ulnar collateral ligament (UCL): The ulnar collateral ligament is located on the inner side of the elbow and contributes to the stability of the joint. It resists the force that can push the elbow outward, helping to prevent excessive opening of the joint on the opposite side (valgus).
- Valgus stress: UCL injury is often associated with excessive valgus stress on the elbow. This typically occurs during activities that involve a throwing or striking motion, where the elbow is under significant load while being flexed.
- Change in joint dynamics: Injury to the UCL can lead to weakening or failure of the ligament, thereby altering normal joint dynamics. This can lead to elbow instability and increased opening on the medial side.
- Muscular compensation: In response to instability, the muscles around the elbow may attempt to compensate by providing increased muscular support. However, this can lead to muscle imbalances and increase the risk of injury.
- Impacts on pronation and supination: The UCL injury can also affect the pronation (inward rotation) and supination (outward rotation) movements of the forearm, as these movements are linked to the stability of the elbow joint.


Valgus elbow strain is a common injury mechanism among elite baseball pitchers like Clayton Kershaw of the Dodgers. The repetitive throwing motion, especially the rapid arm acceleration and deceleration, places significant stress on the ulnar collateral ligament (UCL) on the inside of the elbow. Over time, this strain can lead to microtears, ligament weakening, and ultimately UCL damage, causing pain, instability, and reduced performance. Preventive measures such as biomechanical analysis, targeted strength training, and proper pitching techniques are crucial in protecting the UCL from long-term damage and maintaining a successful pitching career.

Causes of Tommy John Injury
- Acute trauma: Direct trauma to the elbow, such as a fall on the inner side of the elbow or a violent impact, can cause tearing or distension of the ulnar collateral ligament.
- Repetitive stress: Repetitive activities that constantly strain the ligament, such as throwing movements in certain sports (baseball, softball) or repeated hitting movements (tennis, golf), can lead to progressive wear and tear of the ligament.
- Excessive stress: Repetitive movements associated with certain occupations or activities, such as hammering or screwdriving, can create excessive stress on the ulnar collateral ligament.
- Contact sports: Some contact sports, such as American football or rugby, increase the risk of elbow trauma, including UCL injuries.
- Biomechanical Changes: Anatomical abnormalities or biomechanical changes in the structure of the elbow can increase pressure on the ligament, contributing to its injury.
- Medial epicondylitis: Chronic inflammation of the medial epicondyle (medial epicondylitis) can weaken the ulnar collateral ligament, increasing the risk of injury.
- Age: With aging, the structure of ligaments can deteriorate, increasing the risk of injury.
- Genetic predisposition: Some individuals may have a genetic predisposition to develop ligament injuries, including those of the UCL.
Tommy John Injury Symptoms
- Pain: Pain is felt on the inner side of the elbow, often near the medial epicondyle. It may be acute upon initial impact or develop gradually over time.
- Tenderness to touch: The affected area may be tender to touch, and pain may intensify when palpating the medial epicondyle.
- Swelling: Swelling may develop around the UCL area, indicating inflammation associated with the injury.
- Weakness: Strength in the hand and wrist on the affected side may be reduced due to pain and ligament damage.
- Joint instability: A feeling of instability or looseness in the elbow may be present, especially when gripping or manipulating objects.
- Joint sounds: Some individuals may hear noises such as clicks or crackles during elbow movements, which may indicate instability.
- Limitation of movement: Pain and stiffness can cause limited movement of the elbow, especially during flexion and extension.
- Pronation and supination pain: Rotational movements of the forearm, such as pronation (inward rotation) and supination (outward rotation), can also cause pain.


Pathophysiology
- Overstrain: UCL injury usually occurs due to excessive stress on the ligament. This can result from acute trauma, such as a fall on the inner side of the elbow, or from repetitive strain linked to certain sporting or professional activities.
- Microtrauma: Excessive stress initially causes microtrauma to the ligament. These microtraumas may not be immediately noticeable, but they represent damage to the structure of the ligament.
- Inflammation: In response to microtrauma, an inflammatory reaction occurs. Inflammation is the body’s attempt to heal damage, but it can also contribute to symptoms such as pain and swelling.
- Degeneration: Repetitive microtrauma can lead to progressive degeneration of ligament tissue. This degeneration can weaken the ligament, making it more vulnerable to subsequent injury.
- Stretching or Rupture: As degeneration progresses, the ligament may experience excessive stretching or partial or complete rupture. This can occur during sudden stress or as a cumulative result of repeated stress.
- Joint instability: Once the ligament is weakened or ruptured, the elbow joint can become unstable. Instability may manifest as a feeling of looseness, an inability to bear loads, or increased lateral mobility of the elbow.
- Muscle response: In response to instability, the muscles surrounding the elbow may undergo changes in their activation and strength to compensate for the loss of stability. This can lead to muscle imbalances and contribute to symptoms.
Understanding the biomechanics of UCL injury is essential for developing effective treatment and rehabilitation approaches. Rehabilitation programs often focus on strengthening surrounding muscles, restoring joint stability, and improving movement coordination to promote optimal recovery.
Diagnosis and testing
Physical Exam
- Palpation:
- The healthcare professional palpates the elbow area looking for tenderness, swelling, or possible deformities.
- Mobility Assessment:
- Elbow movements, including flexion, extension, pronation, and supination, are assessed for limitations or unusual pain.
- Valgus and Varus Stress:
- Stress tests, such as the valgus test (to assess the UCL) and the varus test (to assess the radial collateral ligament), are performed to assess elbow stability.
Specialized Tests
- Rotator Cuff Test:
- Specific tests, such as the rotator cuff test, may be performed to rule out other possible causes of elbow pain.
Imaging Exams
- X-rays:
- Standard x-rays help rule out bone fractures and visualize the general structure of the elbow joint.
- Ultrasound:
- Ultrasound can be used to assess the real-time structure and movement of the ulnar collateral ligament.
- MRI (Magnetic Resonance Imaging):
- MRI provides detailed visualization of soft tissues and can detect tears, stretches or abnormalities in the ligament.
- Arthroscopy:
- In some cases, an arthroscopy may be performed, allowing direct visualization of the inside of the joint to confirm the diagnosis and make repairs if necessary.
Treatment
- Conservative treatment:
- Rest: Avoid activities that stress the elbow and ligament to allow healing.
- Ice: Apply ice to the affected area to reduce inflammation.
- Compression: Using a compression bandage can help control swelling.
- Drugs :
- Nonsteroidal anti-inflammatory drugs (NSAIDs): Medications such as ibuprofen may be prescribed to relieve pain and reduce inflammation.
- Osteopathy:
- Strengthening exercises: Exercise program targeting the muscles around the elbow to strengthen stability.
- Manual Therapy: Manipulative techniques to improve mobility and reduce tension in the elbow region.
- Orthotics and splints:
- Orthotics: Specific orthotics may be prescribed to stabilize the elbow and reduce the load on the ligament while it heals.
- Corticosteroid injections:
- Local injections: Corticosteroid injections can be used to reduce inflammation and relieve pain.
- Surgery :
- Surgical Repair: In cases of severe injury or complete ruptures of the UCL, surgery may be considered to repair or reconstruct the ligament.
- Rehabilitation:
- Rehabilitation Program: A rehabilitation plan supervised by a healthcare professional may be necessary to guide the patient through progressive stages of strengthening and recovery.
Tommy John Surgery
Tommy John surgery, also known as ulnar collateral ligament (UCL) reconstruction, is a surgical procedure frequently used to treat severe injuries to the ulnar collateral ligament of the elbow, often caused by overuse in athletes, especially baseball pitchers. Here is a detailed explanation of the surgical procedure and the post-operative recovery process:
Surgical Process
- Anesthesia:
- The patient is placed under general anesthesia to ensure a complete state of sleep during surgery.
- Incision:
- A small incision is made near the elbow to allow access to the damaged ulnar collateral ligament.
- Tendon sampling:
- A tendon is usually taken from another part of the patient’s body, often from the arm, forearm, or foot. This tendon will be used to reconstruct the ulnar collateral ligament.
- Preparation of the Bone Tunnel:
- Bone tunnels are drilled into the ulna (forearm bone) and humerus (upper arm bone) to secure the new tendon in place.
- Tendon fixation:
- The harvested tendon is then inserted into the bone tunnels and secured with screws or other fixation devices to rebuild the ligament.
- Closure of the Incision:
- Once the reconstruction is complete, the incision is closed using sutures.
Post-Operative Recovery
Recovery after Tommy John surgery is a gradual process, usually divided into several phases:
- Immediate Phase (Days to Weeks):
- The arm is usually placed in a splint to immobilize the elbow.
- Passive exercises are introduced to prevent joint stiffness.
- Intermediate Phase (Weeks to Months):
- Active exercises are gradually introduced to strengthen the muscles around the elbow.
- Osteopathy aims to restore range of motion.
- Advanced Phase (Months to Years):
- Muscle strengthening and stabilization activities are intensified.
- The gradual reintroduction of sporting activities is considered, generally after several months.
- Regular Medical Follow-up:
- Regular visits to the doctor or osteopath are necessary to assess progress and adjust the recovery plan.
- Back to Sports Activities:
- Full return to sports activities can take anywhere from six months to over a year, depending on individual recovery.
Conclusion
The ulnar collateral ligament (UCL) injury, popularly known as Tommy John injury, remains a significant challenge in the world of sports, particularly for baseball pitchers who are repeatedly exposed to high-stress throwing motions. This condition, named after the pioneering surgery of Tommy John, has necessitated advanced surgical and rehabilitative approaches to manage and mitigate its effects.
The complex anatomy and biomechanics of the UCL highlight its critical role in elbow stability, and understanding these aspects is key to both prevention and treatment. While Tommy John surgery has provided a pathway for many athletes to return to their sport, it underscores the importance of preventative measures, including proper throwing mechanics, strength training, and adequate rest.
The evolution of surgical techniques and rehabilitation strategies has offered hope for those affected, but it is essential to continue advancing our understanding of the injury’s underlying mechanisms. By combining biomechanical analysis, effective treatment options, and ongoing preventive strategies, we can work towards reducing the incidence of UCL injuries and supporting athletes in maintaining their careers and passion for their sport.
References
- Jobe, F. W., & Stark, H. (1986). “Reconstruction of the ulnar collateral ligament in athletes.” Journal of Bone and Joint Surgery, 68(2), 269-275.
- ElAttrache, N. S., & Andrews, J. R. (2009). “The role of Tommy John surgery in the prevention of elbow injuries in baseball players.” Journal of Shoulder and Elbow Surgery, 18(4), 640-646.
- Fleisig, G. S., & Andrews, J. R. (2009). “Biomechanics of baseball pitching and throwing injuries.” Sports Health, 1(4), 297-306.
- Wang, T. Y., & Dines, J. S. (2018). “The role of biomechanics in preventing ulnar collateral ligament injuries.” Sports Medicine and Arthroscopy Review, 26(1), 14-20.
- Reinold, M. M., & Wilk, K. E. (2014). “Rehabilitation of the ulnar collateral ligament injured elbow.” Journal of Orthopaedic & Sports Physical Therapy, 44(11), 904-915.
- Klein, S. K., & McAdams, T. R. (2019). “Long-term outcomes of ulnar collateral ligament reconstruction in baseball players.” Journal of Shoulder and Elbow Surgery, 28(6), 1093-1101.
- Wilk, K. E., & Reinold, M. M. (2011). “Current concepts in the rehabilitation of ulnar collateral ligament injuries in the overhead athlete.” International Journal of Sports Physical Therapy, 6(3), 199-217.
- Cain, E. L., & Dugas, J. R. (2008). “The role of ulnar collateral ligament reconstruction in the treatment of elbow instability.” Journal of Bone and Joint Surgery, 90(6), 1220-1230.
- Aune, K. T., & Schreiber, T. (2020). “Tommy John surgery: The evolving role of ulnar collateral ligament reconstruction.” Orthopaedic Journal of Sports Medicine, 8(1), 2325967119890531.
- Rosen, J. E., & Jacobson, R. J. (2017). “Outcome measures and return-to-play rates following ulnar collateral ligament reconstruction.” Sports Medicine, 47(4), 731-741.






")



{kind=link}