


Introduction
A meniscal tear in the knee marks the beginning of a physical and emotional transformation. This little pad, the meniscus, usually discreet in its role of stability and shock absorption, becomes the involuntary protagonist of a healing story.
When an extreme rotational movement causes the meniscus to give way, each step becomes a painful encounter with reality. Symptoms, such as pain, swelling and joint locking, may seem discouraging, but they become signals that guide you toward appropriate care.
The key to recovery is a combination of rest, physical therapy, and sometimes medical procedures. Just as the meniscus repairs itself, patience and perseverance become essential allies on the path to healing.
Emotional support also plays a crucial role. The frustrations of limiting daily activities can be overwhelming, but support from healthcare professionals, friends and family helps ease the burden.
Every small step forward in this journey to healing becomes a significant victory. A meniscal tear is not simply an obstacle, but an opportunity to strengthen understanding of our own bodies and cultivate a more conscious relationship with our well-being.
Beyond the pain, the meniscal tear in the knee becomes an invitation to resilience, to deep self-understanding and to a recovery full of learning about the inner strength that resides in each of us. Each step in this healing process offers the opportunity to not only restore functionality to the knee but also to develop a deeper connection with our body and our ability to overcome challenges. Thus, the meniscal tear becomes a chapter in the book of our resilience, a story where patience, perseverance and support come together to open the door to a new understanding of the inner strength and healing capacity of the human body.
Warning: The information provided in this article is intended for general informational purposes only and should not be considered as medical advice. It is not a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Warning: The information provided in this article is intended for general informational purposes only and should not be considered as medical advice. It is not a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Summary
The menisci are made of crescent-shaped bands of fibrocartilage that provide the structural integrity of the knee. When the doctor tells his patient that he has diagnosed a “ cartilage tear ,” he is really saying that he has found a “ meniscus tear .” The medial meniscus is C-shaped and the lateral is U-shaped. They perform many functions for the knee, including load-bearing, shock absorption, joint lubrication, joint stability and proprioceptive feedback.

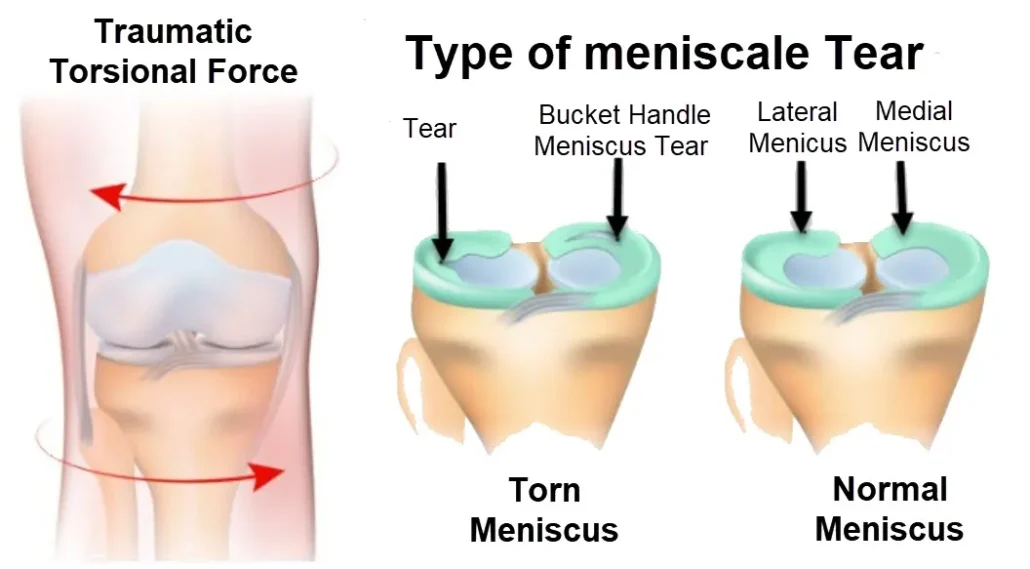
The image illustrates the mechanisms and types of meniscal tears, a common knee injury caused by excessive force or torsional stress on the joint. The meniscus is a crescent-shaped cartilage structure located between the femur (thighbone) and tibia (shinbone), serving as a cushion and stabilizer for the knee.
On the left, the image depicts a traumatic torsional force, a frequent cause of meniscal tears. This force typically occurs during activities involving sudden twisting, pivoting, or deceleration movements, such as in sports like football, basketball, or skiing.
On the right, different types of meniscal tears are shown:
Tear: A simple tear in the cartilage, causing pain and swelling in the knee.
Bucket Handle Tear: A severe tear where a fragment of the meniscus becomes displaced, leading to locking or restricted movement in the knee.
Lateral and Medial Tears: These occur on either side of the meniscus (lateral or medial), often associated with instability and pain during motion.
The image also contrasts a normal meniscus, which is intact and functional, with the damaged structures, highlighting the importance of early diagnosis and appropriate treatment to prevent further joint damage and maintain knee function.
When the knee is in extension, the meniscus is capable of transmitting up to 50% of the total load placed on the knee and approximately 90% of the load when the knee is in flexion. Only a small segment of the meniscus is vascular and responds well to surgery or heals without intervention (see below).
The remaining meniscus cannot heal with conservative measures and may need surgical resection, but this depends on the severity and type of tear.
Any degree of trauma to the menisci can lead to knee instability, loss of articular cartilage, and ultimately degenerative arthritis or re-injury. Meniscal tears can be traumatic or degenerative, depending on the mechanism of injury and the patient’s age and activity level.
Functions of the meniscus
The menisci are crescent-shaped structures located in the knee joints, between the femur (thigh bone) and the tibia (lower leg bone). They play a crucial role in joint function by providing stability, pressure distribution and lubrication of the joint. Here are some of the main functions of the menisci:
- Cushioning: The menisci act as natural shock absorbers, absorbing shock and reducing pressure on the joint surfaces of the femur and tibia. This helps prevent premature wear of the cartilage.
- Stability: They reinforce the stability of the joint by improving the fit between the femur and the tibia. By acting as wedges, the menisci help maintain proper alignment of joint surfaces during movement.
- Load Distribution: The menisci contribute to uniform load distribution on the joint surfaces. This helps prevent excessive pressure points and minimize the risk of cartilage damage.
- Lubrication: They play a role in lubricating the joint by promoting the production of synovial fluid, a fluid that reduces friction between joint surfaces, thus facilitating movement.
- Reduced Friction: The menisci reduce friction between the femur and tibia during movement, contributing to a smoother joint and making flexion and extension of the knee easier.
- Support in Lateral Stability: The menisci help stabilize the knee joint laterally, helping to prevent excessive side-to-side rocking movements.
- Proprioception: They play a role in proprioception, which is the body’s ability to perceive its position in space. This contributes to coordination of movements and body awareness.
Mechanism of meniscal tear injury
- Knee Rotation: Sudden rotation of the knee while bearing weight, such as during rapid pivoting during sporting activity, can cause the meniscus to twist, resulting in a tear.
- Flexion and Extension: Extreme flexion and extension movements, especially when combined with compressive forces, can place excessive pressure on the meniscus, leading to a tear.
- Squatting with Rotation: When a person performs a squat while rotating the knee, it can create significant stress on the meniscus, increasing the risk of tearing.
- Axial Compression: A large load applied directly to the top of the knee, such as during a fall with a bent knee, can cause axial compression, leading to a meniscal tear.
- Direct Trauma: A direct blow to the knee, for example, during a sporting accident or violent impact, can damage the meniscus and cause a tear.
- Aging and Wear: In some cases, especially in older people, gradual wear and tear from aging can weaken the meniscus, making it more likely to tear even during normal activities.
It is important to note that meniscal tears can occur as a result of a combination of these mechanisms, and each person may have specific risk factors based on their anatomy, activity level, and other factors.
Causes of a meniscal tear
- Acute trauma: Sudden trauma, such as violent twisting or direct impact to the knee, can cause a meniscal tear. This can happen during sporting activities, accidents or falls.
- Aging: With age, the meniscus can undergo a natural process of wear. Age-related changes, including reduced cartilage quality, can increase the risk of a meniscal tear, even with normal movement.
- Repetitive movements: Repetitive movements of the knee, especially with frequent twisting, can contribute to progressive wear of the meniscus, increasing the risk of tearing.
- Sports Activities: Certain sports activities that involve rotational movements, pivoting, or rapid changes of direction may increase the risk of a meniscal tear. This particularly concerns sports such as football, basketball and skiing.
- Anatomical defects: Anatomical abnormalities of the knee, such as a particular shape of the meniscus or poor alignment of the lower extremities, can increase vulnerability to meniscal tears.
- Excessive loading: Excessive loading on the knee, such as lifting heavy objects incorrectly, can cause significant stress on the meniscus and contribute to a tear.
- Joint Diseases: Certain medical conditions, such as arthritis, can weaken the cartilage in the knee, increasing the risk of a meniscal tear.
- Previous injuries: People with previous knee injuries, such as sprains or ligament damage, may be more likely to develop meniscal tears.
Symptoms of a meniscal tear
- Pain: Knee pain is one of the most common symptoms. The pain may be felt on the inside or outside of the knee, depending on the location of the tear.
- Swelling: Swelling of the knee can occur due to joint fluid buildup. This can make you feel full or stiff.
- Locking or stuck feeling: Some individuals may experience a stuck or numb feeling in the knee, which may be caused by the displacement of a torn piece of the meniscus.
- Clicks or crackles: Noises such as clicks, crackles, or squeaks may accompany knee movements. This may be due to friction of irregular surfaces caused by tearing.
- Difficulty extending the knee: Some individuals may have difficulty fully extending the knee due to the meniscal tear.
- Tenderness to touch: The knee may be tender to touch, especially around the area of the tear.
- Limitation of movement: A meniscal tear can cause limitation of movement, especially twisting or rotating movements of the knee.
- Increased pain during certain activities: Pain may intensify during certain activities, such as walking, running, or movements that involve pivoting.
A Day in the Life of Someone Suffering from Having a Meniscal Tear
6:30 AM: The Painful Awakening
Samantha, a 42-year-old graphic designer, starts her day with a familiar ache in her right knee. A meniscal tear, which she sustained during a recent soccer game, has been a persistent source of discomfort. The pain is often sharp and localized, and she struggles to get out of bed, favoring her injured knee. Mornings are particularly challenging as stiffness and swelling are at their peak. She takes a moment to apply an ice pack to her knee, hoping to reduce inflammation and ease the pain before beginning her day.
7:00 AM: Morning Routine with Caution
Samantha’s morning routine has become a careful balancing act. Simple tasks like showering and dressing require adjustments. She uses a shower chair and has installed grab bars to avoid putting weight on her injured knee. Choosing clothes that are easy to put on while seated is a must. The pain and stiffness make standing and moving around difficult, so she relies heavily on a cane for support. Despite these modifications, the process is slow and often frustrating.
8:00 AM: The Commute
Getting to work is another challenge. Samantha drives to the office, but the short commute is uncomfortable due to prolonged sitting and limited leg movement. She uses a cushion to reduce pressure on her knee and makes frequent stops to stretch and move her leg. At the office, she has a special ergonomic chair with added knee support to make sitting more bearable. The commute is a reminder of how everyday activities are now influenced by her injury.
9:00 AM: Work Adjustments
At work, Samantha’s tasks are adapted to her current limitations. She uses a height-adjustable desk so she can alternate between sitting and standing, which helps reduce the strain on her knee. Her colleagues are supportive, often helping with tasks that require more mobility. Samantha also keeps her workspace organized to minimize the need for frequent movements. Despite these adaptations, focusing on work is challenging when dealing with constant pain and the need for occasional breaks to stretch or elevate her leg.
12:00 PM: Lunch Break
Lunchtime offers a brief respite. Samantha uses this time to elevate her knee and apply ice if needed. She usually opts for a short walk, but even this can be painful. Her colleagues often join her for lunch, and she appreciates their company and support. However, she remains cautious about her movements, avoiding any activity that could exacerbate her symptoms. The break is both a physical and mental relief, providing a momentary escape from the discomfort of her injury.
2:00 PM: Managing Pain and Discomfort
By the afternoon, Samantha’s knee pain often intensifies. She periodically takes prescribed pain medication and performs gentle stretching exercises to maintain mobility and reduce stiffness. Using a small heating pad during breaks helps with muscle relaxation. These strategies are part of her daily routine, designed to manage the pain and prevent further injury. Despite her efforts, fatigue from dealing with constant discomfort sets in, making it difficult to stay focused.
5:00 PM: Heading Home
The journey home is a slow and careful process. Samantha uses her cane for support and is mindful of every step to avoid aggravating her knee. She takes frequent breaks and avoids carrying heavy bags. At home, she immediately puts her leg up on a stack of pillows and applies ice to help with swelling. The end of the day is often a relief, but Samantha knows that managing her meniscal tear requires ongoing attention and care.
7:00 PM: Evening Routine
In the evening, Samantha takes time for physical therapy exercises recommended by her doctor. These exercises are crucial for strengthening the muscles around her knee and improving her range of motion. Though sometimes painful, they are essential for her recovery. After her exercises, she enjoys a quiet dinner and spends time relaxing with a book or watching TV, all while keeping her knee elevated and supported.
10:00 PM: Preparing for Rest
As bedtime approaches, Samantha carefully prepares for sleep. She applies a final layer of ice to her knee and performs some relaxation techniques to ease any remaining discomfort. She arranges her pillows to support her knee and attempts to get comfortable despite the pain. The day ends with a sense of accomplishment for having managed the challenges of living with a meniscal tear, but also with a hope for healing and improvement.
11:00 PM: Reflecting on the Day
Before falling asleep, Samantha reflects on her day. Managing a meniscal tear requires constant vigilance and adaptation, but she remains hopeful and resilient. Each day is a testament to her strength and determination to navigate life with her injury while working towards recovery and a return to normalcy.
Classification of the red zone and the white zone of the knee
The classification of red zone and white zone refers to the vascularity of the meniscus of the knee. These areas determine the ability of the meniscus to regenerate and heal after injury.
- Zone Rouge :
- Characteristics: The red zone is the outer part of the meniscus, near the periphery.
- Vascularization: This area is well vascularized, which means that it has an adequate blood supply.
- Healing Ability: Due to the presence of blood vessels, the red area has relatively better healing ability compared to the white area.
- Zone Blanche :
- Characteristics: The white area is the interior part of the meniscus, further from the periphery.
- Vascularization: Unlike the red zone, the white zone is poorly vascularized, or even avascular in certain regions.
- Healing Ability: Due to lack of blood supply, the healing ability of the white area is limited. Lesions in this area often have difficulty healing spontaneously.
When a meniscal tear occurs, the location of the tear in relation to these areas can influence treatment options and prognosis. Tears in the red zone tend to respond better to surgical repair due to better vascularity, while tears in the white zone may require more careful treatment approaches.
It is essential to consider these vascular characteristics when making decisions about the treatment of meniscus injuries to optimize the healing process. Surgical procedures, such as arthroscopy, may be considered depending on the location of the tear and the specific needs of the patient. However, each case is unique, and the final decision will depend on several factors, including the severity of the injury and the patient’s overall health.
Menisci are classified based on the blood supply to the area (Poulsen M, Johnson 2011)

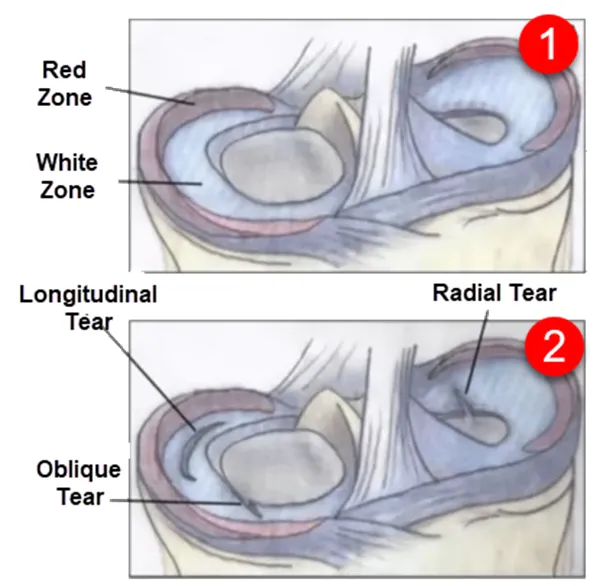
This image illustrates the structural zones of the meniscus and the various types of meniscal tears that can occur. The meniscus is a critical cartilage structure within the knee, providing cushioning, stability, and load distribution.
Meniscal Zones
Red Zone: The outer region of the meniscus, rich in blood supply. Tears in this zone have a higher potential to heal naturally or with surgical repair due to the abundant vascularization.
White Zone: The inner region of the meniscus, with little to no blood supply. Tears in this area are less likely to heal on their own and often require surgical intervention.
Types of Meniscal Tears
Longitudinal Tear: A tear that runs along the length of the meniscus. These are often repairable, especially if they occur in the red zone.
Oblique Tear: A diagonal tear that can destabilize the meniscus.
Radial Tear: A tear extending outward from the inner edge of the meniscus. These often impair the meniscus’s ability to absorb shock and distribute load, requiring surgical management.
- The “red-red” zone is located at the very outer edge of the meniscus and receives the most blood. Damage to the meniscus is repairable
- The “red-white” zone is located in the middle 1/3 of the meniscus at the junction between the vascular and avascular parts of the meniscus. Damage to the meniscus is partially repairable
- The “white-white” zone is the innermost aspect of the meniscus and includes the avascular portion. Damage to the meniscus is irreparable
Type of Meniscal Knee Tear
Meniscal tear of the knee is a common injury that affects the meniscus, a crescent-shaped piece of cartilage located between the femur (thigh bone) and the tibia (shin bone) in the knee joint. There are different types of meniscal tears, generally classified based on the nature of the tear and its location. Here are some common types of meniscal tears:
- Radial Tear: It occurs when the tear extends from the outer edge of the meniscus towards the center. Radial tears can sometimes heal on their own, but they may also require surgery, depending on the location and severity.
- Longitudinal Tear: This type of tear generally follows the direction of the meniscus fibers. The severity of the tear can vary, and treatment will depend on the size and location of the tear.
- Complex Tears: These often involve several types of tears combined. Complex tears may require surgery to repair or remove the damaged portion of the meniscus.
- Flap Tear: This type of tear creates a flap-like portion that can hang in the knee joint, causing symptoms such as locking or locking of the knee. Surgery is often necessary to resolve this problem.
- Displaced Tear: When part of the meniscus is displaced from its normal position in the knee joint, it can lead to severe symptoms. Surgery is usually recommended to put the displaced part back in place.


(A) Longitudinal tear, (B) Radial tear, (C) Horizontal tear, (D) Bucket handle tear, (E) Parrot’s beak tear and (F) Segmental tear
Meniscus assessment
- Joint line tenderness
- Posterior knee pain may be present
- Joint effusion (may be difficult to find and occur several hours after injury)
- Lameness
- A displaced tear can prevent the knee from reaching full extension, as well as impaired flexion.
- A mechanical blockage of movement is called a locked knee.
McMurray test
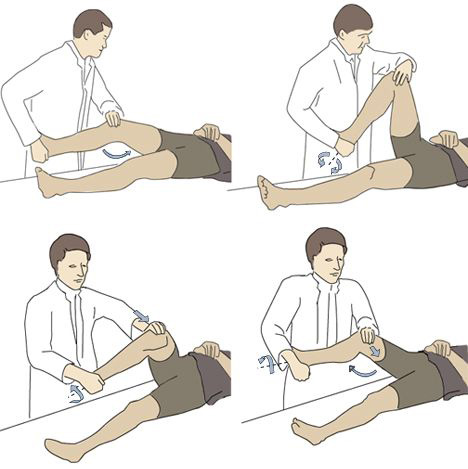
The McMurray test is an orthopedic test that is used to evaluate the presence of a meniscal tear in the knee. It is named after the British orthopedic surgeon Thomas Porter McMurray, who first described it in the early 20th century. Here is how the McMurray test is generally performed:
Objective: Detect a meniscal tear in the knee.
Procedure :
- The patient lies supine on an examination table, with the feet hanging off the edge.
- The healthcare professional flexes the patient’s knee, then places one hand on the knee while grasping the end of the foot with the other hand.
- Maintaining external rotation of the tibia, the knee is gently flexed and extended.
- During this movement, the practitioner listens and looks for signs of clicks, pops, or pops that could indicate a meniscal tear.
Interpretation:
- A clicking or palpable sensation when rotating the knee may indicate a meniscal tear.
- The location of the click can provide insight into the position of the tear (e.g., inside or outside the knee).
It is important to note that the McMurray test is a preliminary diagnostic tool and confirmation by other methods, such as medical imaging (MRI or X-ray), is often necessary.

The McMurray Test is a clinical examination used in osteopathy, orthopedics, and physical therapy to assess the integrity of the menisci in the knee joint, specifically to detect tears. It is commonly performed when a patient reports knee pain, clicking, or a feeling of instability.
How the McMurray Test is Performed
- Positioning: The patient lies supine on an examination table.
- Flexion and Rotation: The examiner holds the patient’s heel and places their other hand on the knee joint. The knee is flexed fully while the examiner rotates the tibia internally and externally.
- Extension and Compression: As the leg is extended, the examiner applies varus (inward) or valgus (outward) stress to the knee while maintaining rotation to stress specific parts of the meniscus.
- Medial Meniscus: Tested with external rotation and varus stress.
- Lateral Meniscus: Tested with internal rotation and valgus stress.
Positive Test
- A clicking sound, pain, or a sensation of “catching” during the movement indicates a possible tear in the medial or lateral meniscus.
Differential diagnoses of a meniscal tear
Differential diagnoses for a meniscal tear include other conditions and injuries that may present with similar symptoms. It is important to consider these possibilities when evaluating a person with knee pain. Here are some possible differential diagnoses:
- Osteoarthritis of the knee: Osteoarthritis is a degenerative joint condition that can cause pain, stiffness, and decreased range of motion, symptoms also present in meniscal tears.
- Anterior Cruciate Ligament (ACL) Sprain: An ACL sprain can cause knee pain, a “giving” feeling or instability, symptoms similar to those of a meniscal tear.
- Patellar tendonitis: Inflammation of the patellar tendon can cause pain and swelling in the knee, which may be confused with symptoms of a meniscal tear.
- Knee bursitis: Inflammation of the bursae around the knee can lead to pain, swelling and tenderness, symptoms shared with a meniscal tear.
- Tibial plateau fracture: A fracture at the tibial plateau can cause knee pain and limitation of movement, resembling some symptoms of a meniscal tear.
- Iliotibial band syndrome: Irritation of the iliotibial band can cause knee pain, especially during physical activity, which may be confused with symptoms of a meniscal tear.
- Baker’s Cyst: A Baker’s cyst, which is a buildup of synovial fluid at the back of the knee, can cause pain and swelling, resembling some symptoms of a meniscal tear.
Treatment of a meniscal tear in the knee?
- Surgical treatment is recommended for most meniscal tears, except those causing minor symptoms in less active patients.
- If nonoperative management is chosen, treatment aims to minimize symptoms of pain and swelling
- Inflammatory medications are warranted until symptoms subside.
- It is safe to wear a knee brace
References
- Dejour D, Pungitore M, Valluy J, Nover L, Saffarini M, Demey G. Tibial slope and medial meniscectomy significantly influence short-term knee laxity following ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019 Nov;27(11):3481-3489. [PubMed]2.
- van de Graaf VA, Willigenburg NW, Poolman RW. Arthroscopic Partial Meniscectomy vs Physical Therapy for Nonobstructive Meniscal Tears-Reply. JAMA. 2019 Feb 26;321(8):806. [PubMed]3.
- Liebs TR. Arthroscopic Partial Meniscectomy vs Physical Therapy for Nonobstructive Meniscal Tears. JAMA. 2019 Feb 26;321(8):805-806. [PubMed]4.
- Donohue MA, Zhou L, Haley CA. Meniscus Injuries in the Military Athlete. J Knee Surg. 2019 Feb;32(2):123-126. [PubMed]5.
- Fuchs A, Kloos F, Bode G, Izadpanah K, Südkamp NP, Feucht MJ. Isolated revision meniscal repair – failure rates, clinical outcome, and patient satisfaction. BMC Musculoskelet Disord. 2018 Dec 21;19(1):446. [PMC free article] [PubMed]6.
- Wilson PL, Wyatt CW, Romero J, Sabatino MJ, Ellis HB. Incidence, Presentation, and Treatment of Pediatric and Adolescent Meniscal Root Injuries. Orthop J Sports Med. 2018 Nov;6(11):2325967118803888. [PMC free article] [PubMed]7.
- Kurzweil PR, Cannon WD, DeHaven KE. Meniscus Repair and Replacement. Sports Med Arthrosc Rev. 2018 Dec;26(4):160-164. [PubMed]8.
- Karia M, Ghaly Y, Al-Hadithy N, Mordecai S, Gupte C. Current concepts in the techniques, indications and outcomes of meniscal repairs. Eur J Orthop Surg Traumatol. 2019 Apr;29(3):509-520. [PMC free article] [PubMed]9.
- Hollier J, Leonardi C, Igbokwe L, Dasa V. Knee Range of Motion as a Discriminatory Tool Indicating Potential Meniscal Tears. Ochsner J. 2018 Summer;18(2):126-130. [PMC free article] [PubMed]10.
- Chirichella PS, Jow S, Iacono S, Wey HE, Malanga GA. Treatment of Knee Meniscus Pathology: Rehabilitation, Surgery, and Orthobiologics. PM R. 2019 Mar;11(3):292-308. [PubMed]11.
- Ferrari MB, Murphy CP, Gomes JLE. Meniscus Repair in Children and Adolescents: A Systematic Review of Treatment Approaches, Meniscal Healing, and Outcomes. J Knee Surg. 2019 Jun;32(6):490-498. [PubMed]12.
- Rathcke MW, Lind M, Boesen MI, Nissen N, Boesen AP, Mygind-Klavsen B, Hölmich P. [Treatment of meniscal pathology]. Weekly Laeger. 2017 Sep 18;179(38) [ PubMed ]13.
- Beaufils P, Becker R, Kopf S, Matthieu O, Pujol N. The knee meniscus: management of traumatic tears and degenerative lesions. EFORT Open Rev. 2017 May;2(5):195-203. [PMC free article] [PubMed]14.
- Hagmeijer MH, Kennedy NI, Tagliero AJ, Levy BA, Stuart MJ, Saris DBF, Dahm DL, Krych AJ. Long-term Results After Repair of Isolated Meniscal Tears Among Patients Aged 18 Years and Younger: An 18-Year Follow-up Study. Am J Sports Med. 2019 Mar;47(4):799-806. [PubMed]



 Weakness: Causes, Implications, and Solutions")




{kind=link}