



Introduction
Piriformis syndrome, a delicate and sometimes overlooked condition, is characterized by compression or irritation of the sciatic nerve by the piriformis muscle. This pear-shaped muscle, which extends from the sacrum to the upper part of the femur, plays a crucial role in external rotation of the hip. Despite its small size, the piriformis can have a significant impact on the quality of life of individuals when it is involved in the development of the syndrome.
Symptoms of piriformis syndrome are diverse and may include localized pain in the gluteal region, numbness or tingling down the leg, and muscle weakness in the affected area. These manifestations can disrupt daily activities and limit mobility, creating an often painful experience for those who suffer from them.
The underlying causes of piriformis syndrome are varied. They can result from muscle tension from prolonged sitting, injuries, muscle spasms, or even repetitive activities that overuse the piriformis muscle. Diagnosing this condition can sometimes be complex due to the similarity of its symptoms to other lower back conditions, emphasizing the importance of a thorough medical evaluation.
Among the different therapeutic approaches aimed at relieving the symptoms of piriformis syndrome, osteopathy stands out as a holistic approach that seeks to restore the structural balance of the body. Osteopathic practitioners take a personalized approach, taking into account the severity of the situation, the patient’s medical history and underlying factors.
Osteopathy is based on a thorough understanding of the anatomy and mechanisms of piriformis syndrome. Osteopathy sessions may involve gentle joint manipulation, muscle stretching, and other techniques aimed at reducing tension and restoring mobility. By working on the entire body, osteopaths seek to identify and correct structural imbalances that could contribute to piriformis syndrome.
Historically, piriformis syndrome was introduced into medical terminology by British surgeon Sir Herbert William Ralston Yeoman in 1928. Since then, osteopathy has positioned itself as an effective complementary approach to relieving the symptoms associated with this condition.
Consulting a competent osteopath can provide several benefits, including an accurate diagnosis, designing a treatment plan tailored to the patient’s individual needs, and improving overall well-being. Collaboration between patient and osteopath plays an essential role in the healing process, allowing a better understanding of the triggering factors and contributing to an integrated approach to the management of piriformis syndrome. By choosing osteopathy, individuals can explore a holistic therapeutic pathway to alleviate the symptoms of this delicate condition.
Warning: This article discusses Piriformis Syndrome and provides techniques specifically intended for use by trained osteopaths. The information presented is not meant for self-treatment or use by unqualified individuals. It is crucial not to attempt osteopathic techniques or any form of manual therapy on yourself or others without proper training and certification. Always consult a licensed osteopath or healthcare professional for appropriate assessment and treatment. Attempting untrained interventions may result in harm or exacerbate existing conditions.
Anatomy of the piriformis
The piriformis is a small muscle located deep in the pelvic region. It originates on the anterior surface of the sacrum, at the level of the S2 to S4 vertebrae, as well as on the sacrotuberal ligament. From there, it extends diagonally toward the upper portion of the greater trochanter of the femur, where it inserts.

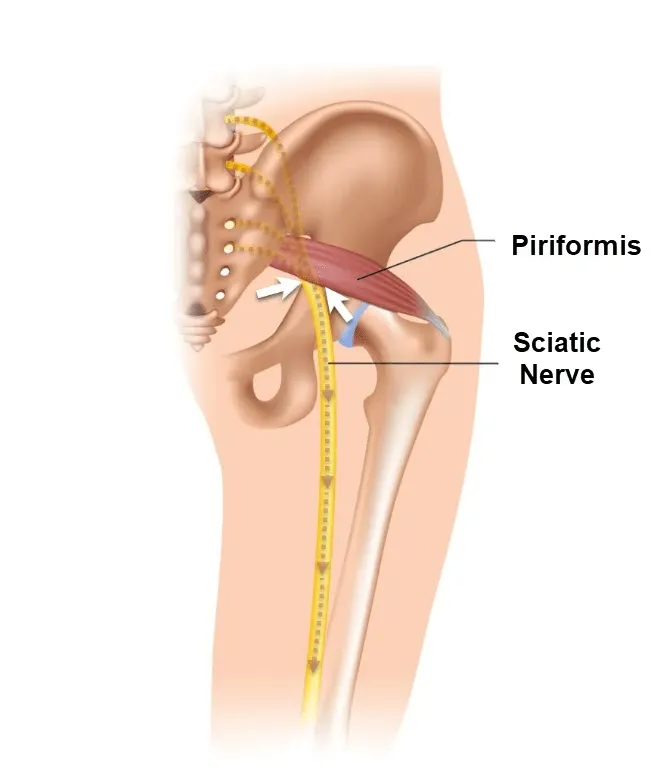
The main function of the piriformis is to participate in the external rotation of the hip, thereby contributing to the stability of the hip joint. It is primarily innervated by the sciatic nerve, which may pass through or underneath the muscle in some people. Notably, due to its proximity to the sciatic nerve, excessive tension or contraction of the piriformis can sometimes lead to piriformis syndrome, causing pain and numbness along the path of the sciatic nerve.
The Crossing of the Sciatic Nerve by the Piriformis Muscle: Anatomical Variations
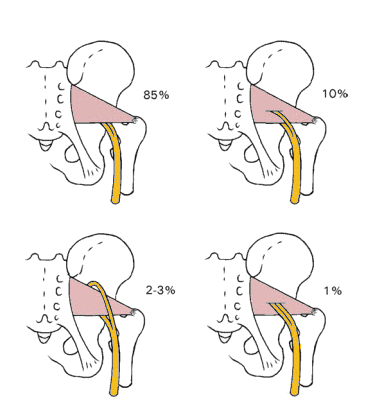
The sciatic nerve, an essential component of the peripheral nervous system, plays a crucial role in transmitting signals between the spinal cord and lower extremities. Its complex route through the human body can be subject to various anatomical variations, one of them being the crossing of the piriformis muscle. The piriformis, a small pear-shaped muscle located in the pelvic region, can sometimes become an unwitting player in sciatic nerve problems. In 10 to 20% of the population, the sciatic nerve passes through the piriformis muscle, creating a situation conducive to specific clinical manifestations. The interaction between the sciatic nerve and the piriformis muscle can result in symptoms such as sciatic pain, muscle stiffness, and even numbness in the lower extremities. Researchers have studied this condition to better understand its underlying mechanisms and improve treatment approaches.
Some studies, notably those carried out by Pecina et al. (1991), Szabo (1989) and Travel, Simons (1992), examined the prevalence of sciatic nerve crossing by the piriformis muscle. This work made it possible to determine that this anatomical variant is not rare, affecting a significant part of the population. When the sciatic nerve passes through the piriformis, it can be exposed to increased pressure, leading to unpleasant symptoms. Compression of the nerve can cause shooting pain along its path, often felt in the buttocks, lower back, and leg. Patients sometimes report a tingling or numbness sensation, which can compromise their daily quality of life.
- Pecina et al. (1991) : Pecina, M. (1991). “Contribution to the etiological explanation of the piriformis syndrome.” Acta Anatomica, 142(3), 261-263.
- Szabo (1989) : Szabo, R. M. (1989). “Piriformis syndrome: a cause of nondiscogenic sciatica.” Orthopedics, 12(2), 231-233.
- Travell, Simons (1992) : Travell, J. G., & Simons, D. G. (1992). Myofascial Pain and Dysfunction: The Trigger Point Manual. Volume 2: The Lower Extremities. Baltimore: Williams & Wilkins.
Health professionals, particularly osteopaths, play an essential role in managing problems related to the crossing of the sciatic nerve through the piriformis. Treatment approaches may include manual techniques to release muscle tension, improve nerve mobility, and relieve associated pain.

Pain cycle
Vicious cycle where excessive muscle contraction leads to compression of the sciatic nerve, causing impaired nerve transmission, which in turn can further influence muscle contraction.

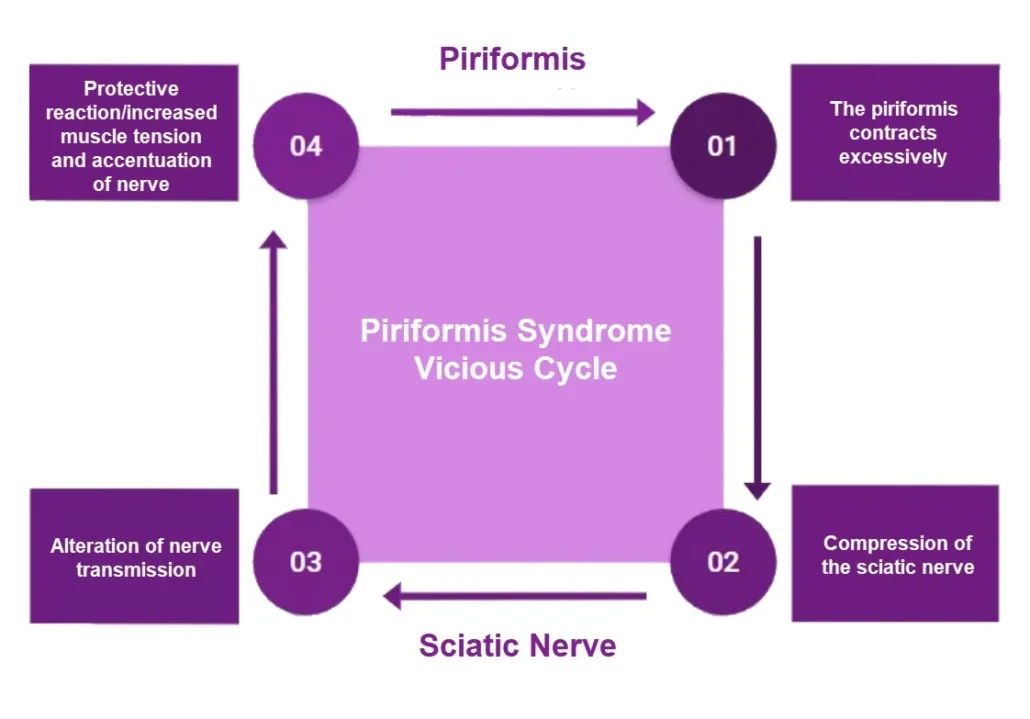
In the specific context of the piriformis and sciatic nerve, this interaction may contribute to piriformis syndrome. When the piriformis muscle contracts excessively, it can compress the sciatic nerve, causing symptoms such as pain and numbness. These symptoms can in turn lead to a protective response, inducing an increase in muscle tension, which worsens the compression of the nerve and intensifies the symptoms. This cycle continues, creating a complex interrelationship between muscle contraction and impaired nerve transmission.
Mechanism of sciatic nerve compression
The mechanism of sciatic nerve compression in piriformis syndrome is generally associated with the anatomical proximity of the piriformis muscle to the nerve. Here’s how compression can occur:
- Sciatic Nerve Passage: The sciatic nerve, which is the largest nerve in the body, usually passes under or through the piriformis muscle in the deep region of the buttocks.
- Anatomy Varies: The anatomical relationship between the piriformis and the sciatic nerve can vary from person to person. In some cases, the sciatic nerve may pass through the muscle, while in other cases it may pass just underneath.
- Muscle Contractions: The piriformis can spasm or contract involuntarily, often in response to overuse of the muscle, trauma, or strain. These contractions can cause the muscle to tighten.
- Nerve Compression: When the piriformis muscle contracts excessively or for a prolonged period, it can put pressure on the sciatic nerve that passes nearby. This compression can cause irritation of the nerve, leading to symptoms such as pain, tingling, or numbness along the nerve’s path.
- Inflammation and Swelling: Chronic compression can lead to inflammation of the sciatic nerve. Inflammation can increase pressure on the nerve, worsening symptoms and creating a vicious cycle of compression and inflammation.
Piriformis Syndrome vs. Piriformis Myofascial Syndrome: Two Close, But Distinct Conditions
Although Piriformis Syndrome and Piriformis Myofascial Syndrome share some symptoms and can be confused due to their anatomical proximity, they are two distinct conditions.
Piriformis syndrome is mainly characterized by compression or irritation of the sciatic nerve by the piriformis muscle, located in the gluteal region. This compression can cause pain in the lower back, buttocks and sometimes down the leg, mimicking the symptoms of sciatica. Risk factors for piriformis syndrome include prolonged sitting, specific physical activities, and muscle imbalances.
Piriformis myofascial syndrome , on the other hand, focuses on trigger points or muscle knots (trigger points) in the piriformis muscle. These trigger points can cause local pain, but they can also cause distant pain, making the differentiation between piriformis myofascial syndrome and other conditions, including piriformis syndrome, sometimes complex. Myofascial triggers can be caused by trauma, repeated strain, or overuse of the muscle.
Piriformis myofascial syndrome
Myofascial syndrome is characterized by the presence of trigger points, which are sensitive and tense areas in the muscles. When myofascial syndrome affects the piriformis muscle, it is often referred to as “piriformis myofascial syndrome.” In this condition, trigger points in the piriformis muscle can cause local pain in the gluteal region and can also lead to referred pain in the lower back, hips, and even along the sciatic nerve.
Treatment for piriformis myofascial syndrome may involve approaches to release tension in the muscle, reduce inflammation, and relieve trigger points. Massage techniques, stretching, physical therapy, and in some cases, trigger point injections may be used to alleviate symptoms.
Two localized trigger points
- At the level of the lateral border of the sacrum and approximately one third of the medial part of the greater trochanter.
- They involve the sacroiliac region, the buttocks and the hip joint, and sometimes extend to the proximal two thirds of the posterior part of the thigh.


In the presence of trigger points in the piriformis, the muscle tends to shorten and increase in volume, resulting in compression of the sciatic nerve.
The pain resulting from this compression spreads along the posterior aspect of the thigh to the calf and the sole of the foot. Therefore, pain can emanate from various sources simultaneously.
Causes of piriformis syndrome
Several factors can contribute to the development of this syndrome. First, physical trauma, such as falls or sports injuries, can cause inflammation of the piriformis muscle, leading to compression of the nerve. Additionally, muscular imbalances, often linked to a sedentary lifestyle or inadequate postural habits, may also play a role in piriformis syndrome. People who spend long hours sitting or have improper lifting habits can overstrain this muscle, contributing to its inflammation. Additionally, anatomical variations, such as the abnormal position of the sciatic nerve relative to the piriformis muscle, may increase predisposition to this syndrome. Additionally, certain repetitive activities, such as running, can also be a trigger. By understanding these different potential causes, it becomes possible to implement prevention and management strategies for piriformis syndrome, ranging from correcting postural habits to targeted exercises aimed at strengthening the muscles involved.
- Individual Anatomy: The anatomical arrangement of the sciatic nerve in relation to the piriformis muscle can vary from person to person. Some individuals may have anatomy that increases the risk of nerve compression.
- Overuse: Strenuous or repetitive physical activities, such as running, cycling, or other exercises that strain the piriformis muscle, can cause overuse of the muscle, leading to strain and compression of the nerve.
- Trauma: Traumatic injuries, such as falls on the buttocks, car accidents, or sports injuries, can damage the piriformis muscle or cause muscle spasms that lead to compression of the sciatic nerve.
- Muscle Contractions: Prolonged muscle contractions or spasms of the piriformis can result from strain, trauma, or excessive activity, leading to compression of the nerve.
- Prolonged sitting: A sedentary lifestyle with long periods of sitting can contribute to muscle weakness and stiffness in the piriformis, thereby promoting the development of the syndrome.
- Inflammation: Inflammation of the piriformis muscle due to trauma, infections, or inflammatory conditions can contribute to sciatic nerve compression.
- Underlying musculoskeletal conditions: Disorders such as scoliosis, spinal abnormalities, or other musculoskeletal conditions can influence posture and muscle function, contributing to piriformis syndrome.
- Heredity: There may be a genetic predisposition to develop musculoskeletal disorders, including piriformis syndrome.
It is important to note that piriformis syndrome can result from several of these factors combined. The presence of these causes does not necessarily guarantee development of the syndrome, and many people may have similar anatomy or activities without experiencing symptoms.
Symptoms of Piriformis Syndrome
Piriformis syndrome is a rare but often disabling musculoskeletal condition that affects the piriformis muscle, located in the buttocks region. This syndrome occurs when the piriformis muscle compresses or irritates the sciatic nerve, causing a specific set of symptoms. People with this syndrome may experience pain similar to that caused by sciatica. Here’s a detailed look at the symptoms associated with piriformis syndrome, which can vary in intensity from person to person.
List of Symptoms
1. Pain in the buttocks area
One of the most common symptoms of piriformis syndrome is persistent, localized pain in the buttocks area. This pain can be deep, throbbing, or diffuse. It is often felt on one side only and may be worse after physical activities such as walking, running, or climbing stairs. Sitting for long periods of time can also make the pain worse.
Patients may also describe a feeling of tightness or stiffness in the affected buttock, limiting hip movement. This can make everyday tasks, such as sitting down or getting up from a chair, particularly painful.
2. Pain radiating to the leg
Piriformis syndrome pain is not limited to the buttocks area. Because of the piriformis muscle’s proximity to the sciatic nerve, irritation of this nerve can cause pain that radiates down the leg, often to the knee or even the foot. This descending pain, similar to sciatica, is often described as a shooting, burning, or electric pain.
This radiation of pain to the leg can cause sensations of tingling, numbness or muscle weakness. These symptoms can worsen after a period of prolonged rest, especially after sitting for long hours.
3. Numbness and tingling
In addition to pain, patients may experience numbness or tingling (paresthesia) in the buttock and down the affected leg. These sensations, similar to an “electric current,” usually occur because the piriformis muscle compresses the sciatic nerve. The numbness may be concentrated in the buttock or extend down the thigh, sometimes to the foot.
Paresthesias are often more noticeable when the person sits for a long time or adopts positions that increase pressure on the piriformis muscle, such as crossing the legs.
4. Difficulty moving the hip and leg
Hip and leg mobility may be reduced in people with piriformis syndrome. This reduced mobility is often due to muscle pain and stiffness. For example, movements such as abduction (stretching the leg) or external rotation of the hip may be particularly painful.
Additionally, some people may notice weakness in the affected leg, making it difficult to walk or maintain certain postures. Discomfort may be exacerbated after physical exercise or repetitive activities involving the legs.
5. Increased pain after specific activities
Certain activities exacerbate symptoms of piriformis syndrome. Exercises that involve flexion or rotation of the hip, such as running or lifting weights, can make pain worse. Similarly, prolonged sitting, especially on hard or inclined surfaces, can worsen sciatic nerve compression and cause symptoms to flare up.
Repetitive movements, especially those that involve the lower back and legs, can also contribute to the return or worsening of symptoms. It is common for patients to experience increased pain after a day of physical activity or after lifting heavy objects.
6. Lower back pain
Although the pain of piriformis syndrome is usually concentrated in the buttocks and leg, some patients may also experience pain in the lower back. This lower back pain is not directly related to disc or spinal pathology, but rather is the consequence of muscular and postural compensation due to tension in the piriformis muscle.
When the piriformis muscle is tight or contracted, it can disrupt the natural alignment of the pelvis and lower back, causing discomfort in that area. The lower back pain associated with this syndrome may be more diffuse and less intense than that felt in the buttock or leg, but it can make diagnosis more complex.
7. Night pains
Piriformis syndrome can disrupt sleep for those who suffer from it. The pain may be worse when a person is lying down, especially on their back or on the affected side. Staying in one position for a long time, even at night, can increase the pressure on the piriformis muscle and, therefore, cause increased discomfort.
Some people report frequent nighttime awakenings due to radiating pain or numbness in the affected leg. Specific sleeping positions, such as with the legs bent or crossed, can also exacerbate symptoms at night.
8. Difficulty sitting on hard surfaces
The inability to sit comfortably on hard surfaces is another distinct symptom of piriformis syndrome. Compression of the sciatic nerve by the piriformis muscle is amplified when the person sits on a hard chair or bench. Buttock pain and nerve irritation often worsen in these situations.
Many patients report temporary relief by changing position or standing up, but the pain quickly returns once they resume prolonged sitting. This can make daily life, especially at work or when traveling, particularly uncomfortable.
9. Local sensitivity to touch
Some people with piriformis syndrome may notice increased tenderness in the affected buttock. When palpated, there may be trigger points or tender areas, often near the piriformis muscle itself. This sensitivity to touch can make even simple actions, such as sitting or lying down, uncomfortable and can lead to daily discomfort.
This local sensitivity can be exacerbated by increased inflammation of the piriformis muscle, particularly after physical exertion or prolonged irritation of the sciatic nerve.
10. Alterations in gait
Due to persistent pain in the buttock and leg, some people may unconsciously alter their gait to avoid engaging the piriformis muscle. This compensation can result in a limp or a leaning of the body to one side, creating an imbalance in posture and gait.
In the long term, this alteration in gait can lead to additional pain, particularly in the lower back, hips and knees, due to overload and muscular compensation.
11. Muscle spasms
Muscle spasms are a manifestation that some people with piriformis syndrome may experience. The piriformis muscle can contract involuntarily in response to pain or inflammation. These uncontrolled contractions can lead to additional pain, intensifying discomfort in the buttock area and sometimes down the leg.
Muscle spasms can occur as a result of intense physical exertion or prolonged positioning, such as sitting or standing for long periods of time. They can also make it harder for the piriformis muscle to relax and contribute to a constant feeling of stiffness.
12. Local inflammation
Although inflammation is not a directly noticeable symptom, it plays a central role in the onset of piriformis syndrome symptoms. Irritation of the sciatic muscle and nerve can cause a local inflammatory reaction in the buttock region. This inflammation may be accompanied by mild swelling or a feeling of warmth in the affected area.
This inflammatory response can be exacerbated by intense or repetitive physical activities, increasing pain and other symptoms such as numbness or tingling in the leg.
13. Muscle fatigue
Due to the constant tension and irritation of the piriformis muscle, some people may experience muscle fatigue in the affected leg. This fatigue is usually due to overuse of the muscle or the effort required to compensate for the pain. This results in general weakness in the leg, which may be worse after physical activities or prolonged exertion.
This can make simple tasks, such as climbing stairs or getting up from a seated position, more difficult and tiring. Muscle fatigue can also slow recovery, especially if symptoms are ignored or left untreated.
14. Burning sensation
Another common manifestation of piriformis syndrome is a burning sensation, often described in the buttock and thigh. This symptom is related to irritation of the sciatic nerve, and it can be triggered or aggravated by specific activities such as running, lifting weights, or even sitting in an uncomfortable position.
The burning sensation is often accompanied by other symptoms such as numbness or tingling, and it can make sitting or walking more difficult for long periods of time.
15. Disturbance of balance
In some people, piriformis syndrome can affect balance because of muscle weakness or pain that disrupts posture and gait. This disruption may be subtle, but it can make activities like walking, standing, or climbing stairs more risky, increasing the risk of falling.
Patients may sometimes involuntarily adjust their posture to avoid pain, which can misalign the body and compromise overall balance. Over the long term, these adaptations can also cause pain in other parts of the body, including the hips, knees, and lower back.
16. Bilateral pain (rarer)
Although piriformis syndrome usually affects only one side of the body, some people may experience bilateral symptoms, meaning pain in both buttocks or both legs. This is rarer but can occur in cases where both piriformis muscles are irritated or tight, or in situations where structural abnormalities or muscle imbalances are present on both sides of the pelvis.
When the pain is bilateral, it can be difficult to diagnose and may be confused with other conditions, such as a herniated disc or spinal cord injury.
17. Feeling of heavy legs
Some people with piriformis syndrome report a feeling of heaviness in the affected leg, which may be associated with prolonged compression of the sciatic nerve. This sensation can make movement more difficult and contribute to muscle fatigue.
The feeling of heavy legs is often more pronounced after activities that put strain on the leg, such as walking or running, or after prolonged periods of standing or sitting.
18. Increased pain when pressing on the abdomen
Some people with piriformis syndrome may experience an exacerbation of their symptoms when they perform efforts that increase intra-abdominal pressure, such as sneezing, coughing, or lifting heavy objects. These actions can further compress the sciatic nerve via involuntary contraction of the piriformis muscle, intensifying the pain that radiates to the leg or buttock.
This pain accentuated by intra-abdominal pressure is also observed in conditions such as herniated disc, which can make a differential diagnosis difficult without additional tests.
19. Feeling of heat or cold in the leg
Another less common symptom reported by some patients is an abnormal sensation of heat or cold in the affected leg. These thermal sensations are probably related to irritation of the sciatic nerve, which can lead to sensory disturbances. The person may feel as if their leg is “on fire” or, conversely, ice cold.
These sensory symptoms can be added to the numbness and tingling already mentioned, further complicating the daily life of the affected person.
20. Generalized fatigue
Chronic pain associated with piriformis syndrome can, in the long term, contribute to generalized fatigue. Indeed, the constant effort to compensate for the pain and physical limitations can exhaust the body. In addition, the lack of sleep caused by nighttime pain can accentuate this feeling of fatigue.
This fatigue can also affect concentration and productivity, making it difficult to complete daily tasks, both professional and personal.
21. Impact on mental health
Like any chronic painful condition, piriformis syndrome can impact the mental health of those affected. Living with constant or intermittent pain can cause anxiety or depression, especially if symptoms limit daily activities or lead to social isolation.
It is essential to consider this psychological aspect as part of the overall management of piriformis syndrome. Patients may benefit from psychological support or therapy to cope with the emotional impact of chronic pain.
22. Pain in internal rotation of the hip
Although external rotation of the hip is often cited as a painful movement for people with piriformis syndrome, internal rotation of the hip can also cause discomfort. This is because this movement stretches the piriformis muscle, increasing compression of the sciatic nerve. Therefore, movements involving internal rotation, such as crossing the legs while sitting, can also make the pain worse.
23. Long-term posture problems
Patients with piriformis syndrome, in an attempt to reduce pain, may adopt compensatory postures that, in the long term, lead to other musculoskeletal imbalances. For example, poor weight distribution on the hips or altered gait can cause pain in the lower back, knees, or even neck.
These postural compensations are particularly frequent when the pain persists over a long period without adequate treatment.
24. Iliotibial band syndrome
Piriformis syndrome, by affecting gait and disrupting muscle balance in the hips, can lead to the onset of other disorders, such as iliotibial band syndrome. This syndrome manifests itself as pain on the outer side of the knee, usually due to irritation caused by the iliotibial band rubbing against the thigh bone. Although these two conditions are distinct, they can be linked by problems with posture and muscle imbalance.
25. Increased sensitivity to changes in temperature or atmospheric pressure
Some people with chronic musculoskeletal pain, including those with piriformis syndrome, may experience increased sensitivity to weather changes, such as a drop in temperature or changes in air pressure. This can lead to increased muscle and nerve pain, although this relationship is not always well understood scientifically.
This sensitivity can make symptoms more unpredictable and make pain management difficult, especially for people living in areas with changing weather conditions.


Incidence of piriformis syndrome
- Piriformis syndrome accounts for about 6-8% of sciatica cases, according to some clinical studies.It is more common in women, potentially due to anatomical differences in the pelvis and lower body alignment.Athletes, particularly those engaged in activities that involve repetitive lower body motions (e.g., runners, cyclists), may be at a higher risk.
- It is more common in women, potentially due to anatomical differences in the pelvis and lower body alignment.
- Athletes, particularly those engaged in activities that involve repetitive lower body motions (e.g., runners, cyclists), may be at a higher risk.
Ballet and piriformis syndrome
Ballet practice, due to its specific movements and physical demands, can potentially influence the development of piriformis syndrome in some dancers. Here is how classical dance, especially ballet, may be linked to piriformis syndrome:
- Foot Position and External Rotation: Ballet frequently involves externally rotated foot positions, which stresses the piriformis muscle. Repetition of these movements can lead to overuse of the muscle and, in some cases, contribute to the development of piriformis syndrome.
- Repeated Flexion and Extension: Hip flexion and extension movements, common in ballet, can put increased stress on the piriformis muscle and sciatic nerve, especially if these movements are performed repeatedly and excessively.
- Intense Stretching: Ballet dancers are often subjected to intensive stretching, which can potentially lead to muscle strain, including in the piriformis muscle.
- Specific postures: Certain specific postures in ballet can involve significant external rotation of the hips, thereby straining the piriformis and increasing the risk of sciatic nerve compression.
- Physical Demands: The high physical demands of ballet can lead to muscle overuse and fatigue, increasing the likelihood of strains and spasms in the piriformis muscle.
Although dancing can benefit physical and mental health, dancers, particularly ballet dancers, may be more susceptible to developing certain musculoskeletal conditions due to the specific movements of their art.
It is important for dancers, as well as dance professionals, to be aware of potential risks and take preventive measures, such as adequate warm-up, appropriate stretching, and careful management of exercise intensity.
Differential diagnoses
- Lumbar herniated disc: A herniated disc can cause sciatic pain similar to piriformis syndrome by compressing the sciatic nerve in the spine.
- Spinal Stenosis: Spinal stenosis, a narrowing of the spinal canal, can also cause sciatic pain and symptoms similar to piriformis syndrome.
- Hip bursitis: Inflammation of the bursa (a small pocket of fluid) near the hip can cause pain similar to piriformis syndrome.
- Osteoarthritis of the hip: Osteoarthritis of the hip can cause pain in the hip and buttocks area, which may be confused with piriformis syndrome.
- Spondylolisthesis: A condition in which one vertebra slips forward relative to the lower vertebra can cause symptoms similar to piriformis syndrome.
- Pudendal neuralgia: Irritation of the pudendal nerve can cause pain in the pelvic area and buttocks, which can be confused with piriformis syndrome.
- Eosinophilic myofasciitis: Inflammation of muscle and fascial tissue can cause muscle pain and symptoms similar to piriformis syndrome.
- Cauda Equina Syndrome: Compression of the nerve roots at the base of the spine can cause symptoms similar to piriformis syndrome.
- Muscle or ligament injuries: Injuries to the muscles or ligaments around the hip can cause pain in the gluteal area.
Recommendations
- Avoid activities that cause piriformis syndrome. So, if the syndrome is triggered by cycling, look for another way to exercise, at least for a few days.
- Do a deep tissue massage of the hips and buttocks.
- Get up from your chair often.
- Stand, walk and stretch. This is especially important for people who sit at work, such as truck drivers and office staff.
- Sit on a chair that is cushioned. At work, used an ergonomic chair.
- Do not put the wallet in the back pocket, this will have the effect of compressing the sciatic nerve further.
- Have a healthy weight.
- Do recommended stretches for piriformis syndrome
Logical Pathway to Piriformis Syndrome Diagnosis
Piriformis syndrome is a neuromuscular disorder characterized by the compression or irritation of the sciatic nerve by the piriformis muscle, located deep in the buttock. As the symptoms of piriformis syndrome often mimic other conditions, such as lumbar disc herniation or sciatica, it is essential for an osteopath to use a structured, thorough approach to diagnose this condition accurately. Here is the logical pathway an osteopath may follow to diagnose piriformis syndrome within their office.
1. Comprehensive Patient History and Symptom Inquiry
The first step in diagnosing piriformis syndrome is collecting a detailed patient history and understanding the nature of their symptoms. During the initial consultation, the osteopath will ask the patient questions related to the location, onset, and nature of their pain, which is often concentrated in the buttock region and may radiate down the leg, resembling sciatica.
Key questions include:
- When did the pain start, and how has it progressed?
- What activities worsen or relieve the pain?
- Is the pain more intense when sitting, standing, or walking?
Typically, patients with piriformis syndrome report a dull ache or sharp pain in the buttock, which can radiate down the posterior thigh and calf due to sciatic nerve involvement. Activities that aggravate the piriformis muscle, such as sitting for extended periods, walking uphill, or squatting, often worsen the pain. Additionally, patients may describe a feeling of numbness, tingling, or weakness in the affected leg.
An osteopath may also inquire about a history of trauma, such as a fall, sports injury, or repetitive strain from activities like running, which can contribute to piriformis syndrome.
2. Posture and Gait Assessment
In an osteopathy office, a comprehensive evaluation of the patient’s posture and gait is fundamental. Piriformis syndrome can lead to subtle postural imbalances as the patient compensates for the pain. The osteopath will observe whether the patient favors one side while standing or walking, which can be a sign of muscle imbalance or nerve irritation.
Additionally, gait analysis can reveal biomechanical dysfunctions, such as asymmetry in hip movement or weight-bearing patterns, which may contribute to piriformis muscle strain. Osteopaths will assess whether the patient avoids placing weight on the affected side or alters their walking pattern due to discomfort.
3. Palpation and Soft Tissue Examination
A crucial step in diagnosing piriformis syndrome involves manual palpation of the piriformis muscle. The osteopath will assess the area deep in the buttock, feeling for tightness, tenderness, or muscle spasms. Direct palpation over the piriformis or the greater sciatic notch may reproduce the patient’s pain, further suggesting piriformis involvement.
Osteopaths are trained to assess the surrounding muscles and soft tissues, as tension in the piriformis can cause compensatory patterns in other muscles, such as the gluteus maximus, hamstrings, or lower back muscles. By identifying these imbalances, the osteopath can better understand how the piriformis muscle is contributing to the patient’s discomfort.
4. Range of Motion and Functional Testing
Osteopaths often use specific physical tests to evaluate the piriformis muscle and its effect on the sciatic nerve. The following tests are commonly used to provoke symptoms and assess the piriformis’s involvement:
- The FAIR test (Flexion, Adduction, and Internal Rotation): The patient lies on their side while the osteopath flexes the hip and knee, moving the leg into internal rotation. If this position elicits pain or discomfort, it may indicate sciatic nerve compression by the piriformis.
- Pace sign: The patient performs resisted abduction and external rotation of the hip. Pain during this test suggests that the piriformis muscle is overstressed.
- Freiberg’s maneuver: By passively internally rotating the hip, the osteopath can assess for discomfort or pain, which points to piriformis muscle tightness.
These tests are designed to reproduce the symptoms experienced by the patient, aiding in the identification of piriformis involvement.
How long does piriformis syndrome last?
Several factors influence the temporality of this condition, making each case a unique experience. Understanding the potential duration of piriformis syndrome is crucial for affected individuals and healthcare professionals seeking to provide effective care.
The first variable to consider is the severity of the condition. Mild cases, where compression of the sciatic nerve by the piriformis muscle is minimal, can often resolve more quickly. On the other hand, more severe situations, involving significant compression and more pronounced symptoms, can prolong the duration of the syndrome. The intensity of symptoms, such as shooting pain, muscle stiffness and numbness, can influence recovery.
How quickly piriformis syndrome is diagnosed and treated also plays a key role in how long it lasts. Early diagnosis allows a treatment plan to be initiated more quickly, which can contribute to a faster recovery. Unfortunately, the insidious nature of some symptoms can sometimes delay diagnosis, thereby prolonging the duration of the condition.
Individual response to treatment is a third crucial variable. Each person responds differently to therapeutic interventions. Treatment approaches, such as manual techniques used by osteopaths to release muscle tension and improve nerve mobility, may have varying effects from one individual to another. Some patients may experience rapid relief, while others may require more extensive follow-up to achieve optimal results.
In general, the medical literature indicates that piriformis syndrome can last from a few weeks to several months. Acute cases, properly diagnosed and quickly treated, tend to resolve more quickly. However, more complex situations, associated with factors such as significant anatomical variations or complications, can prolong the duration of the syndrome.
It is important for healthcare professionals, particularly osteopaths, to consider these nuances when managing piriformis syndrome. A personalized approach, taking into account the severity of the condition, timeliness of diagnosis and treatment, and individual response to treatment, is essential to optimize clinical outcomes.
Scientific Insights: Osteopathy and Its Role in Managing Pîriformis Syndrome
Piriformis Syndrome: Diagnosis and Treatment (Tanveer, 2021)
This article focuses on the diagnosis and management of piriformis syndrome, highlighting osteopathic medical approaches and the use of techniques such as physical therapy and injections.
Myositis Ossificans of the Piriformis Muscle: An Unusual Cause of Piriformis Syndrome (Beauchesne & Schutzer, 1997)
This paper describes a rare case of piriformis syndrome caused by myositis ossificans, where the sciatic nerve was entrapped by the ossified piriformis muscle, resulting in nerve compression.
Posttraumatic Piriformis Syndrome: Diagnosis and Results of Operative Treatment (Benson & Schutzer, 1999)
This study presents the outcomes of operative treatments in patients with posttraumatic piriformis syndrome, offering insights into the surgical release of the piriformis tendon and neurolysis of the sciatic nerve.
Piriformis Syndrome: Anatomic Considerations and a New Injection Technique (Benzon et al., 2003)
This paper examines anatomical variations of the piriformis muscle and discusses an innovative injection technique to treat piriformis syndrome, alongside osteopathic strategies.
Diagnosis and Management of Piriformis Syndrome: An Osteopathic Approach (Boyajian-O’Neill et al., 2008)
This paper discusses the osteopathic approach to diagnosing and managing piriformis syndrome, highlighting non-pharmacological treatments like osteopathic manipulative therapy.
Piriformis Syndrome: Diagnosis and Treatment (Tanveer, 2021)
This article reviews clinical approaches to piriformis syndrome, emphasizing diagnosis and treatment methods, including osteopathic approaches and interventions like botulinum toxin injections.
Piriformis Syndrome: A Rational Approach to Management (Barton, 1991)
This article discusses the management of piriformis syndrome through osteopathic techniques like stretching, physical therapy, and steroid injections.
Piriformis Syndrome: A Systematic Review (Hopayian et al., 2010)
This systematic review evaluates the clinical features of piriformis syndrome and discusses osteopathic and other treatment strategies.
Screening test
Freiberg maneuver
Forced horizontal adduction of the flexed thigh – pain during testing indicates piriformis syndrome (stretching of the muscle).


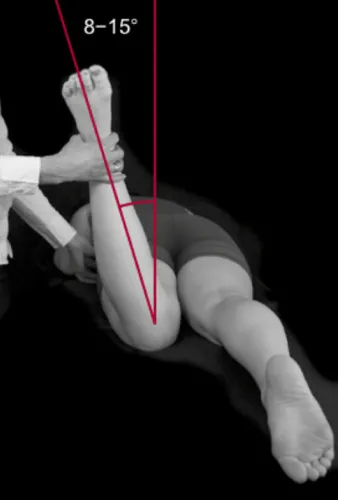
Hibbs maneuver
Patient is lying on his stomach, knee flexed to 90°, the examiner then stabilizes the patient’s pelvis with one hand and slowly pushes the patient’s ankle in a lateral direction (the internal rotation of the femur causes stretching of the piriformis muscle, which can compress the sciatic nerve)

Exercises and Stretches
Here are some exercises and stretches that are often recommended for piriformis syndrome:
Muscle Strengthening Exercises
- Side plank exercise:
- Lie on your side with your elbow directly under your shoulder.
- Lift your hips off the floor, forming a straight line from foot to shoulder.
- Hold the position for a few seconds, then lower back down.
- Repeat on the other side.
- Leg raise in quadruped position:
- On all fours, lift one leg backwards while keeping your back straight.
- Hold the position at the top for a few seconds before lowering back down.
- Alternate legs.
Stretching
- Seated stretch for the piriformis:
- Sit with the affected leg crossed over the other.
- Hold your opposite knee with the arm on the opposite side and gently twist your torso toward the crossed leg.
- You should feel a stretch in your buttock.
- Pigeon stretch:
- In a quadruped position, bring the knee of the affected leg forward and outward.
- Stretch the leg back while lying on your side.
- You should feel a stretch in your buttock.
Flexibility Exercises
- External rotation of the hip while seated:
- Sit with your legs apart.
- Turn the affected leg outward, keeping the knee bent.
- Hold for a few seconds and return to the starting position.
- Internal rotation of the hip while seated:
- Sit with your legs apart.
- Turn the affected leg inward, keeping the knee bent.
- Hold for a few seconds and return to the starting position.
These exercises and stretches aim to strengthen the surrounding muscles, improve flexibility and reduce tension in the piriformis region. However, their effectiveness can vary from person to person, and it is essential to do them correctly to avoid any aggravation.








Osteopathic treatment approach
Muscle energy
- Lay the patient supine, the therapist stands on the same affected piriformis side.
- Flex the knee on the affected side and place the foot on that side on the lateral aspect of the opposite knee.
- The therapist pushes the knee medially until it meets the restrictive barrier.
- Ask the patient to push against the practitioner’s resistance for 3 to 5 seconds, allow a period of isometric relaxation, then engage a new barrier; repeat three times[10].


Combined ischemic compression (elbow or thumb)
Treatment of the piriformis muscle and its central trigger points can be usefully accomplished by direct pressure from the elbow, applied to the area of the main trigger point in the muscle belly, while the leg of the patient lying on the side is rotated. to internally rotate the hip, in order to lengthen the muscle.


Strain Counterstrain
- Lay the patient in a supine position and instruct the practitioner to sit on the same side as the affected piriformis muscle.
- Locate the tender point of the piriformis muscle.
Classically, it is found 2 or 3 inches medial and slightly cephalad to the greater trochanter. - Instruct the practitioner to suspend the patient’s lower extremity over the edge of the table, flexing the hip (approximately 135 degrees) while abducting and externally rotating as needed until tenderness is relieved.
- Hold the position for 90 seconds and slowly return the patient to neutral position.
- Reassess the patient’s sensitivity.


References
- Siddiq MAB. Piriformis Syndrome and Wallet Neuritis: Are They the Same? Cureus. 2018 May 10;10(5):e2606. [ PMC free article ] [ PubMed ]
- Chang A, Ly N, Varacallo M. StatPearls [Internet]. Stat Pearls Publishing; Treasure Island (FL): Feb 12, 2022. Piriformis Injection. [ PubMed ]
- Cassidy L, Walters A, Bubb K, Shoja MM, Tubbs RS, Loukas M. Piriformis syndrome: implications of anatomical variations, diagnostic techniques, and treatment options. Surg Radiol Anat. 2012 Aug;34(6):479-86. [ PubMed ]
- Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequences: a review. Clin Anat. 2010 Jan;23(1):8-17. [ PubMed ]
- Huang ZF, Yang DS, Shi ZJ, Xiao J. [Pathogenesis of piriformis syndrome: a magnetic resonance imaging-based comparison study]. Zhonghua Yi Xue Za Zhi. 2018 Jan 02;98(1):42-45. [ PubMed ]
- Hopayian K, Danielyan A. Four symptoms define the piriformis syndrome: an updated systematic review of its clinical features. Eur J Orthop Surg Traumatol. 2018 Feb;28(2):155-164. [ PubMed ]
- Misirlioglu TO, Palamar D, Akgun K. Letter to the editor involving the article ‘Piriformis muscle syndrome: A cross-sectional imaging study in 116 patients and evaluation of therapeutic outcome’. Eur Radiol. 2018 Dec;28(12):5354-5355. [ PubMed ]
- Ro TH, Edmonds L. Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging. J Clin Imaging Sci. 2018;8:6. [ PMC free article ] [ PubMed ]
- Safarpour Y, Jabbari B. Botulinum toxin treatment of pain syndromes -an evidence based review. Toxicon. 2018 Jun 01;147:120-128. [ PubMed ]
- Nazlıkul H, Ural FG, Öztürk GT, Öztürk ADT. Evaluation of neural therapy effect in patients with piriformis syndrome. J Back Musculoskelet Rehabil. 2018;31(6):1105-1110. [ PubMed ]
- Cass SP. Piriformis syndrome: a cause of nondiscogenic sciatica . Curr Sports Med Rep. 2015 Jan;14(1):41-4. [ PubMed ]









")


{kind=link}