

")
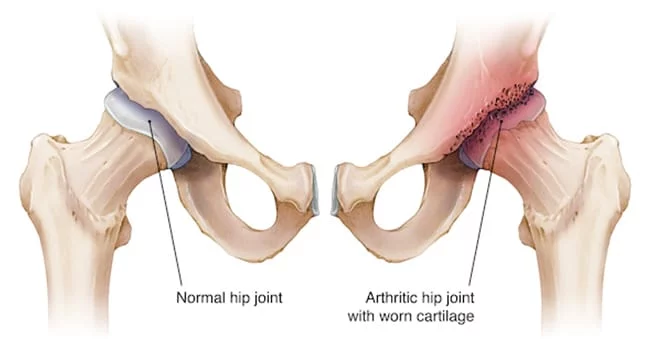
Hip osteoarthritis is characterized by the breakdown of articular cartilage in the hip joint.
Introduction
Osteoarthritis (OA) of the hip can arise either as an idiopathic condition, meaning without an obvious cause, or secondary to factors such as childhood hip diseases, trauma, osteonecrosis, or previous joint infections. While OA is commonly associated with aging and is more prevalent among older adults, it can occur at any age.
This condition is not the result of a single underlying process but rather emerges from various distinct factors, each with its own etiology and potential treatments, ultimately converging on a shared final pathway. The effects of OA on crucial lower limb joints like the hips can lead to significant reductions in mobility and physical function, potentially resulting in a loss of independence and a profound impact on daily activities.
OA is characterized by a gradual breakdown of articular cartilage, which is accompanied by the body’s attempt at repair. This repair process involves the formation of reactive bone, the development of osteophytes (bony growths), and structural remodeling. The progression includes cartilage deterioration, the body’s reparative response, and efforts to stabilize the joint.
As articular cartilage degrades, it damages the joint surface and triggers an inflammatory response. In an attempt to stabilize the joint, the body produces osteophytes. However, this compensatory mechanism can lead to joint deformity, contributing to stiffness and pain.
The structural remodeling observed in OA reflects the body’s effort to restore joint balance, but these changes can impair normal joint function, leading to decreased mobility and reduced physical performance.
A thorough understanding of these processes is essential for guiding effective therapeutic approaches, from managing symptoms to preventing disease progression. Recognizing the complexity of OA allows for tailored, individualized treatment strategies based on each patient’s unique characteristics.

Hip anatomy
The hip, a glenoid joint also known as the ball in the socket joint, is a complex anatomical structure essential to human mobility. Made up of several key components, including the hip bone, acetabulum, femoral head, and femur, the hip provides a significant range of motion in all directions.
The hip bone is a fundamental part of the hip, forming the upper part of the pelvis. It consists of two symmetrical parts on each side of the body, contributing to the formation of the coxofemoral joint. The joint itself is characterized by the round head of the femur which fits into a hemispherical socket called the acetabulum. This unique joint configuration gives the hip great stability while allowing fluid and varied movements.


Within the joint, the bony surfaces are covered in cartilage, a resilient tissue that acts as an impact absorber. Cartilage also facilitates smooth gliding of joint surfaces, minimizing friction and preventing premature wear. To reinforce stability and optimize the functionality of the joint, several small satellite muscles surround the hip. These muscles contribute not only to shock absorption but also to the dynamic stabilization of the joint, thus supporting its structural integrity.
The hip can be considered from two complementary perspectives. On the one hand, it represents the movement of the femur below the pelvis, allowing actions such as flexion, extension, abduction and adduction. On the other hand, it can be conceptualized as an oscillating movement of the pelvis above the head of the femur. This duality of perspectives provides an in-depth understanding of hip functionality, particularly crucial in everyday activities such as walking and running.
By examining the reference plane involved in hip movement, it becomes possible to visualize the muscular lever arms that influence this complex joint. The muscles acting on the hip are essential for maintaining balance, ensuring a smooth gait, and supporting the weight of the body. The precise coordination between these muscles allows for smooth and efficient movements, highlighting the crucial importance of the hip in human locomotor function.
In conclusion, the anatomy of the hip, with its key components such as the iliac bone, acetabulum, femoral head, and femur, forms a complex and interconnected structure. This glenoid joint not only offers great mobility but also the stability necessary for daily life. Understanding hip functionality is essential for healthcare professionals, physical therapists, and anyone seeking to maintain optimal musculoskeletal health.
Cartilage Destruction Cycle
- Joint Cartilage Destruction:
- The initial stage involves the breakdown of articular cartilage due to mechanical stress, inflammation, or other factors. This leads to a loss of cartilage integrity and function.
- Osteophyte Formation:
- In response to cartilage loss, the body attempts to repair the joint by forming osteophytes (bony growths) around the affected area. These osteophytes are intended to stabilize the joint but often exacerbate the problem.
- Joint Deformity:
- Osteophytes and other changes in joint structure lead to joint deformity. This can alter the normal joint alignment and function, contributing to further mechanical stress and inflammation.
- Increased Cartilage Destruction:
- The joint deformity and altered mechanics cause additional stress on the remaining cartilage, leading to further cartilage degradation. This intensifies the cycle of damage.
Degenerative stage of hip osteoarthritis
Osteoarthritis of the hip, also called coxarthrosis, is a degenerative joint condition that results from wear and tear of the cartilage that covers the joint surfaces of the hip bone. This joint disease usually progresses gradually through several stages, ranging from mild discomfort to severe impairment of joint function. Here are the typical stages of degenerative progression of hip osteoarthritis:
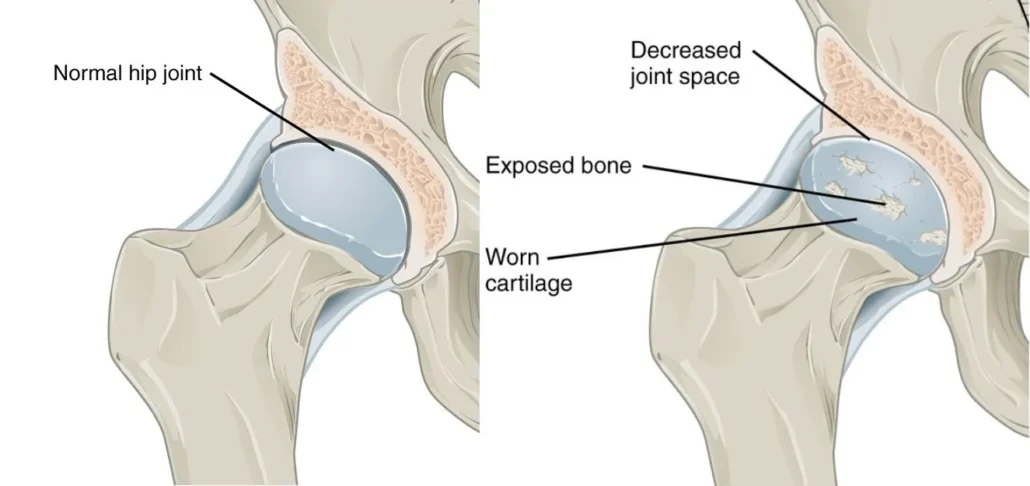
- Normal condition: Initially, the hip joint is healthy, with smooth cartilage and normal joint function.
- Cartilage wear: Factors such as age, normal wear and tear, joint abnormalities or trauma can contribute to progressive wear and tear of the hip cartilage. This can lead to cracking, friction and decreased elasticity of the cartilage.
- Inflammation and changes in the synovium: As cartilage wears away, the body may respond with inflammation of the synovium (the membrane that lines the joint). This inflammation can lead to the production of excess synovial fluid, causing swelling in the joint.
- Osteophyte Formation: In response to wear and loss of cartilage, the body can develop bony growths called osteophytes. These bony growths can cause pain, stiffness, and limitations in movement.
- Reduced joint space: As osteoarthritis progresses, the joint space may become narrower due to less cartilage. This can lead to increased friction between bones, causing more pain and stiffness.
- Joint deformity: Advanced osteoarthritis can lead to structural changes in the joint, including deformity of the femoral and acetabular heads. This can significantly impair the mobility of the joint.
- Constant pain and functional limitation: As the disease progresses, pain becomes more constant, and joint function is significantly limited. Daily activities may become difficult to accomplish.
- Functional disability: At an advanced stage, hip osteoarthritis can cause significant functional disability, affecting the patient’s quality of life. Loss of mobility and constant pain may require medical interventions, including hip replacement surgery (hip arthroplasty) in some cases.
It is important to note that the progression of osteoarthritis can vary from person to person, and not all patients will go through all of these stages. Early treatment and appropriate management can help slow the progression of the disease and relieve symptoms. Treatment approaches may include lifestyle changes, medications, physical therapy, and in severe cases, surgery.
Unfortunately, I cannot provide real-time statistics or updated epidemiological data after my last update in January 2022. However, I can give you an example of how you could integrate epidemiological statistics in a general context.
Prevalence of hip osteoarthritis
Hip osteoarthritis, a debilitating condition, exerts a significant influence on a considerable number of people across the world. Epidemiological data collected until 2022 reveal a variable prevalence of this degenerative disease, depending on geographic regions and age groups.
In various regions of the globe, the prevalence of hip osteoarthritis may differ due to several factors, including lifestyle habits, genetic characteristics, socioeconomic conditions, and health care practices. Some places have higher rates due to environmental factors, such as physical activity level, diets, and other cultural influences that can contribute to the deterioration of joint cartilage.
Within age groups, hip osteoarthritis can affect a variety of people, although its prevalence generally increases with advancing age. Older people are often more likely to develop this condition, in part due to the natural wear and tear on joints over time. However, it is important to note that hip osteoarthritis is not exclusively linked to aging, and cases can also occur in younger individuals due to various factors such as genetic predispositions, previous trauma or metabolic disorders.
The implications of hip osteoarthritis go beyond simple numerical prevalence. This disease can have a devastating impact on the quality of life of affected individuals, leading to chronic pain, reduced mobility and limitation in daily activities. The social and economic repercussions of this condition are also considerable, affecting not only those affected but also their families, health systems and society as a whole.
In-depth understanding of the prevalence of hip osteoarthritis globally is crucial to guide prevention strategies, treatment protocols, and public health policies. Researchers, health professionals, and policymakers can use these data to design targeted approaches that meet the specific needs of affected populations. Public education on risk factors, early signs and management options is also essential to promote awareness and encourage healthy lifestyles.
Canada
Globally, hip osteoarthritis represents a major public health challenge, with significant implications for the Canadian population. According to data provided by Statistics Canada, it is estimated that 12.3% of the population in Canada suffers from this debilitating condition. These alarming figures highlight the magnitude of the burden posed by hip osteoarthritis, affecting the quality of life of thousands of Canadians and generating substantial impacts on the health care system.
Most affected age groups
Data show that hip osteoarthritis mainly affects older people, with a notable prevalence in individuals aged 50 to 64. However, it is worth noting a recent increase in cases among younger adults, likely due to various lifestyle factors.
Distribution by age group (Statistics Canada 2009)
- 20-49 ans : 8.8%
- 50-64 ans : 47.2%
- 65 and over: 44%
Economic and social impact
In addition to the impact on individual health, hip osteoarthritis also has significant economic and social repercussions. Healthcare costs, lost work days, and implications for patients’ quality of life highlight the need for a holistic approach to addressing this public health issue.
While this data provides a general overview, it is crucial to refer to the most recent, region-specific sources to get a more accurate picture of the current situation.
Risk factors
Several risk factors can contribute to the development of hip osteoarthritis. Some of these factors are unavoidable, such as age, but others are lifestyle-related and can be modified or managed to reduce risk. Here are some of the main risk factors for hip osteoarthritis:
- Age: Aging is one of the main risk factors for osteoarthritis. With age, articular cartilage tends to wear away naturally, increasing the risk of developing hip osteoarthritis.
- Gender: Women are more likely to develop hip osteoarthritis than men, although the exact reason is not completely understood.
- Genetic predisposition: There is evidence that genetics may play a role in predisposition to osteoarthritis. If family members have had problems with hip osteoarthritis, this may increase the risk.
- Anatomical factors: Congenital anomalies of the hip or anatomical factors such as malformation of the femoral head or acetabulum may increase the risk of osteoarthritis.
- Joint trauma: Previous injuries to the hip, such as fractures or dislocations, can increase the risk of osteoarthritis. Damaged joints may be more susceptible to cartilage degeneration.
- Overweight and obesity: Excess weight puts additional pressure on joints, especially those that support the body’s weight, such as the hip. This can accelerate cartilage wear and increase the risk of osteoarthritis.
- Strenuous or repetitive physical activities: Certain strenuous or repetitive physical activities, such as running on hard surfaces, can contribute to premature wear of cartilage.
- Poor posture: Poor posture can cause weight to be distributed unevenly across the hip joints, increasing the risk of osteoarthritis.
- Inflammatory joint diseases: Conditions such as rheumatoid arthritis, which cause chronic inflammation of the joints, can increase the risk of hip osteoarthritis.
- Other medical illnesses: Certain medical conditions such as diabetes may also be associated with an increased risk of osteoarthritis.
Managing modifiable risk factors, such as maintaining a healthy body weight and engaging in regular physical activity, can help prevent or reduce the risk of hip osteoarthritis. It is always advisable to consult a healthcare professional for personalized advice on osteoarthritis prevention based on your individual situation.
Symptoms of hip osteoarthritis
- Pain: Pain is one of the most common symptoms of hip osteoarthritis. It can be felt in the hip area, groin, outer thigh, or even the knee. The pain may be more intense during or after physical activity.
- Stiffness: People with hip osteoarthritis may experience joint stiffness, especially after sitting or lying down for a prolonged period of time. Stiffness tends to improve with movement.
- Loss of mobility: Osteoarthritis of the hip can lead to decreased mobility of the hip joint. Movements such as flexion, extension and rotation may become more difficult.
- Crepitations: Some individuals may feel or hear crepitations or cracking sounds when they move their hip due to friction of irregular joint surfaces.
- Lameness: Due to pain and stiffness, a limp may develop naturally to relieve pressure on the affected hip.
- Locking sensations: Some patients report sensations of locking or “grabbing” of the joint, which can limit range of motion.
Differential diagnoses of hip osteoarthritis
- Rheumatoid arthritis: This autoimmune disease causes inflammation of the joints, including those of the hip. Morning stiffness, fatigue, and symmetry of affected joints are hallmarks of rheumatoid arthritis.
- Hip bursitis: Inflammation of the bursae around the hip can cause pain and stiffness similar to osteoarthritis. Hip bursitis is often associated with repetitive movements or prolonged pressure on the area.
- Tendinitis: Inflammation of the tendons surrounding the hip can lead to pain and limitations in movement. Hip tendinitis can be caused by injury, overuse, or chronic inflammation.
- Torn Labrum: The labrum is a ring of cartilage that surrounds the edge of the hip joint. A torn labrum can cause hip pain, especially with certain movements.
- Avascular necrosis of the femoral head: This condition results from loss of blood supply to the femoral head, leading to deterioration of the bone. It can cause hip pain and loss of mobility.
- Hip joint infection: Joint infections, although less common, can cause joint pain and inflammation. Infections can be caused by bacteria or viruses.
- Ankylosing spondylitis: This form of arthritis primarily affects the spine, but can also affect the hips. It is characterized by morning stiffness and inflammation of the joints.
- Bone tumors: Although less common, bone tumors can cause hip pain. Benign or malignant tumors may require further evaluation.
Preventative Approaches to Reduce the Risk of Hip Osteoarthritis
Prevention of hip osteoarthritis is crucial to maintaining good joint health and reducing the personal and economic burden of this condition. Here are some essential preventive approaches to reduce the risk of hip osteoarthritis:
- Maintaining a Healthy Weight: Maintaining an optimal body weight reduces pressure on joints, including the hip. Regular exercise and a balanced diet are essential to prevent excessive weight gain.
- Regular Physical Activity: Physical exercise strengthens the muscles around the hip, improves flexibility and maintains joint mobility. Activities such as walking, swimming and cycling are recommended.
- Avoiding Risky Behaviors: Avoiding smoking, which has been linked to an increased risk of osteoarthritis, and taking precautions during high-risk physical or occupational activities can prevent early deterioration of the hip.
- Adopt an Ergonomic Posture: Maintaining correct posture during daily activities and at work can prevent joint overload. Ergonomic adjustments to the work environment are beneficial.
- Moderate Alcohol Consumption: Moderate alcohol consumption can have beneficial effects on joint health. However, it is essential to respect the recommended limits.
- Nutritional Supplements: Certain supplements like glucosamine and chondroitin can support joint health. Consult a healthcare professional before beginning any supplement regimen.
- Regular Medical Consultation: Regular health examinations allow any joint problem to be detected and treated early. Health professionals can provide personalized advice.
Promising Research and Developments
- Biological Therapies: Research is focusing on the development of biological therapies, such as the injection of growth factors or stem cells, to promote the regeneration of damaged cartilage.
- Innovations in Imaging: Advances in imaging techniques, such as high-resolution magnetic resonance imaging (MRI), allow for a more precise assessment of joint condition and guide the choice of treatments.
- Personalized Treatments: Personalized medicine is growing in importance, with researchers exploring treatments tailored to each patient’s specific genetics and biomolecular profile.
- Nanotechnology: The use of nanomaterials to deliver drugs directly to the affected area is an interesting avenue of research, offering the possibility of targeted delivery.
- Innovative anti-inflammatory therapies: The development of drugs specifically targeting the inflammatory processes associated with osteoarthritis may offer more effective and targeted approaches.
Diagnosis hip osteoarthritis
The diagnosis of hip osteoarthritis is based on a combination of clinical examinations, medical imaging and the patient’s medical history. Diagnostic steps may include:
- History: The doctor will collect information about the patient’s medical history, symptoms experienced, risk factors, and progression of symptoms.
- Physical exam: The healthcare professional will perform a physical exam to assess hip mobility, looking for signs of inflammation, pain, and limitation of movement.
- X-rays: Hip X-rays may be taken to visualize the condition of the joints, identify cartilage loss, and assess the presence of structural changes characteristic of osteoarthritis.
- MRI (Magnetic Resonance Imaging): MRI can provide more detailed images of soft tissue and joint structure, helping to assess the extent of damage.
- Synovial fluid analysis: If inflammation of the joint is suspected, a synovial fluid analysis may be performed to look for signs of infection or other conditions.
Treatment of hip osteoarthritis
Treatment for hip osteoarthritis aims to relieve pain, improve joint function, and slow the progression of the disease. Approaches may vary depending on the severity of symptoms and the patient’s general condition. Treatment options include:
- Drugs :
- Analgesics: To relieve pain.
- Nonsteroidal anti-inflammatory drugs (NSAIDs): To reduce inflammation.
- Intra-articular injections: Corticosteroids or hyaluronic acid to temporarily relieve pain.
- Physical therapy: Specific exercises can strengthen surrounding muscles, improve mobility and reduce pain.
- Weight loss: Reducing the load on the hip through weight loss can relieve symptoms.
- Lifestyle changes: Avoiding high-impact activities, using walking aids, and adopting ergonomic modifications can help.
- Orthotics and walking aids: Crutches, canes or orthotics can relieve pressure on the hip.
- Surgery :
- Hip arthroplasty (hip prosthesis): For severe cases, surgery may be considered to replace the damaged joint with a prosthesis.
- Complementary Therapies: Acupuncture, heat therapy, and other approaches may offer additional relief.
The choice of treatment depends on the severity of the osteoarthritis, the patient’s tolerance to the different options, and the specific symptom management goals. An individualized treatment plan should be developed in collaboration with the healthcare professional.
Beneficial exercise and stretching for those with hip osteoarthritis
Exercise and stretching can play an important role in managing hip osteoarthritis by strengthening the surrounding muscles, improving flexibility and reducing pain. However, it is essential to consult a healthcare professional before beginning any exercise program to ensure that it is suitable for each individual’s specific condition. Here are some beneficial exercises and stretches for people with hip osteoarthritis:
Muscle strengthening exercises
- Hip Abductions: Lie on your side, then lift your top leg up. This exercise strengthens the muscles on the outside of the hip.
- Hip Extensions: Standing, lift your leg back, keeping your knee straight. This strengthens the posterior hip muscles.
- Seated Hip Flexions: Sitting in a chair, raise your knee toward your chest. This strengthens the muscles in the front of the hip.
Range of motion exercises
- Lying Hip Rotation: Lying on your back, bend your knees and let them fall gently from side to side to improve hip mobility.
- Seated Hip Flexion: Sitting on the floor, spread your legs and lean forward to stretch your hip muscles.
Stretching
- Quadriceps stretch: Stand, bend your knee and bring your foot toward your buttocks, holding it with your hand to stretch your quadriceps.
- Adductor Stretch: Sitting on the floor, spread your legs as wide as possible to stretch the adductor muscles on the inside of your thighs.
Low impact activities
- Swimming: Swimming is a low-impact exercise that strengthens muscles without putting too much strain on the hip joints.
- Cycling: Stationary cycling can be a gentle option for improving hip strength and mobility.
Important Tips
- Start slowly and progress gradually.
- Avoid sudden or excessive movements.
- Maintain correct posture during exercises.
- If an exercise causes pain, stop and consult a healthcare professional.
It is crucial to personalize the exercise program based on individual needs, and supervision from a physiotherapist can be beneficial to ensure the safety and effectiveness of the exercises.
Beneficial factors
- Appropriate physical exercise: Gentle physical activities, such as swimming, walking and pool exercise, can strengthen surrounding muscles, improve joint flexibility and help with weight management, thereby reducing pressure on the hip.
- Weight loss: Maintaining a healthy weight is essential to reduce the load on the hip joints. Losing weight can relieve pain and slow the progression of osteoarthritis.
- Physical therapy: Personalized physical therapy programs can help strengthen muscles, improve mobility and teach techniques to prevent movements that could worsen the condition.
- Nonsteroidal anti-inflammatory drugs (NSAIDs): These may be prescribed to relieve pain and reduce inflammation associated with hip osteoarthritis.
- Corticosteroid injections: These injections directly into the joint can provide temporary relief by reducing inflammation.
- Lifestyle adaptation: Adjustments such as using crutches, using a cane or other walking aids can reduce pressure on the hip, making it easier to get around.
- Heat and cold therapy: Applying hot or cold compresses can help relieve pain and reduce inflammation.
- Education and psychological support: Understanding the nature of hip osteoarthritis and learning to manage pain can help improve the psychological quality of life of those affected.
X-ray sign of hip osteoarthritis
Radiographic signs of hip osteoarthritis are often seen in medical images such as x-rays. These signs reflect degenerative changes occurring in the hip joint due to wear and tear of the surrounding cartilage and bone structures. Here are some of the common radiographic signs of hip osteoarthritis:
- Narrowing of the joint space: One of the first radiographic signs of hip osteoarthritis is narrowing of the joint space between the femoral head (thigh bone) and the acetabulum (hip socket). This indicates cartilage loss.
- Osteophytes (bony growths): Osteophytes, also called parrot beaks, can form around the hip joint. These are bony growths that result from the body’s response to cartilage loss. Osteophytes may be visible on x-rays and contribute to joint deformity.
- Subchondral Sclerosis: Subchondral sclerosis refers to a thickening or hardening of the bone located just below the cartilage. This may appear as a denser white area on x-ray images.
- Subchondral Cysts: Cysts can form in the subchondral bone in response to cartilage degeneration. These cysts can be detected on x-rays.
- Deformity of the femoral head or acetabulum: Advanced osteoarthritis can lead to deformity of the femoral head or acetabulum. These structural changes can be seen on x-rays and contribute to the loss of mobility of the joint.
- Joint erosions: Areas of erosion or wear may be visible on x-ray images, indicating cartilage deterioration.
- Joint asymmetry: Due to degenerative changes, the hip joint may exhibit asymmetry, and this asymmetry can be detected on x-rays.
It is important to note that radiographic signs may vary depending on the stage of osteoarthritis and the severity of joint changes.

This caption highlights the differences between the two types of joints and the consequences of osteoarthritis. Case courtesy of Dr Humberto Rodrigo Prochnow Tibau, Radiopaedia.org. From the case rID: 47973
Radiographs early in the disease indicate that changes are concentrated in the superolateral aspect of the joint, the section most subject to mechanical stress. Narrowing of the joint space is followed by osteophyte formation, sclerosis and cyst formation. Remodeling of the medial and lateral femoral head occurs and can lead to its collapse and flattening. The medial space of the acetabulum fills with osteophytes, resulting in progressive superolateral migration of the femoral head.


the joint space is reduced . This reduction in the space between the femoral head and the acetabulum suggests
wear of the articular cartilage , a characteristic of conditions such as
hip osteoarthritis . Cartilage, which serves as a protective cushion between the bones, gradually degrades, leading to the bone surfaces coming closer together and potentially causing joint pain and stiffness.
This radiographic sign is a classic indicator of joint degeneration, requiring clinical evaluation to determine the stage of the condition and the treatments to consider.
- Subchondral cysts
- Osteophyte formation
- Loss of joint space
- Surface difforme


hip osteoarthritis with clear pathologic changes. The annotations indicate several characteristic features:
Major decrease in joint space : This reduction in the space between the femoral head and the acetabulum is a classic sign of osteoarthritis, suggesting the progressive wear of the articular cartilage, which prevents the bones from rubbing directly against each other.Noncongruence of the articular surfaces : The articular surfaces, which should normally be smooth and perfectly adapted to each other, here show an irregularity, indicating bone deformation and remodeling related to advanced osteoarthritis.
Bone sclerosis : This densification of the subchondral bone results from repeated mechanical overload due to cartilage degradation. It appears as whitish areas on the X-ray, indicating the bone reaction to the cartilage lossThese radiographic findings are typical of advanced stages of hip osteoarthritis and are often associated with pain, joint stiffness and loss of mobility for the patient.Case courtesy of Dr Roberto Schubert,
Radiopaedia.org . From the case rID: 16376Case courtesy of Dr Roberto Schubert, Radiopaedia.org. From the case rID: 16376
Advanced osteoarthritis of the right hip. Compared to the unaffected hip, the diseased joint exhibits severe narrowing and misalignment, with extensive osteophyte formation. Also note the buttressing (widening) of the femoral neck in response to abnormal loads.


Key elements of the physical exam
- Assessment of hip range of motion (ROM), provocative maneuvers and gait analysis.
- Hip range of motion may reveal restricted and painful internal rotation, which is considered one of the first signs of hip osteoarthritis.
- The process is often analgesic.
- Provocative maneuvers, including the flexion abduction and external rotation test (FABER):
- The examiner flexes, abducts, and externally rotates the patient’s leg and supports the ipsilateral ankle of the leg on the contralateral stationary thigh or knee. The examiner then compresses the ipsilateral knee posteriorly while stabilizing the contralateral ASIS.
- Positive: Pain in the groin of the ipsilateral hip joint with posterior compression of the ipsilateral knee indicates intra-articular hip pathology and possible osteoarthritis of the hip, while pain in the contralateral buttock indicates pathology of the sacroiliac (IS) joint.


Faber (Flexion, Abduction, External Rotation) test , which is often used in the clinical evaluation of hip or low back disorders. The patient lies supine with one leg fully extended on the table. The other leg is positioned so that the ankle rests on the opposite knee, forming a figure-four position.
The practitioner then applies gentle pressure to the bent knee while stabilizing the opposite hip, to mobilize the hip joint and sacroiliac joint. This test assesses the presence of pain or stiffness in adjacent structures, including the sacroiliac joints, piriformis muscles, and the lumbar region.
Pain in the anterior region of the hip may suggest intra-articular hip pathology, while pain in the posterior region may indicate sacroiliac dysfunction. This is a test commonly used in osteopathy and physiotherapy to guide the diagnosis and treatment of pelvic or lower back pain.
- Assessment of lumbar lordosis, lumbosacral and sacroiliac movement:
- The degree of lumbar lordosis and pelvic tilt should be assessed as they can influence the effects of anteversion or retroversion of the acetabulum and lead to a reduction in force at the hip joints.
Assessment of mobility and provocative maneuvers
- Hip range of motion (ROM): Examining hip range of motion may reveal restricted and painful internal rotation, which is considered one of the first signs of hip osteoarthritis. It is important to note any limitations in movement and document the presence of pain during these movements.
- Gait: The way a person walks can be affected by hip osteoarthritis. An analgesic gait, that is, impaired walking to relieve pain, may be observed. Patients may have a limp to reduce pressure on the affected hip.
- Provocative maneuvers:
- Flexion Abduction and External Rotation (FABER) Test: The examiner flexes, abducts, and externally rotates the patient’s leg, then posteriorly compresses the ipsilateral knee. Pain in the groin of the ipsilateral hip joint indicates possible osteoarthritis of the hip, while pain in the contralateral buttock indicates pathology of the sacroiliac joint.
- Assessment of lumbar lordosis, lumbosacral and sacroiliac movement: The patient’s overall posture, including lumbar lordosis and movements in the lower back and sacrum, can influence the effects of anteversion or retroversion of the lumbar lordosis. acetabulum. It can also impact the force exerted at the hip joints.
References
- Barbour KE, Helmick CG, Boring M, Brady TJ. Vital signs: Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2013–2015. MMWR Morb Mortal Wkly Rep. 2017 Mar 10;66(9):246–53. DOI: https://doi.org/10.15585/mmwr.mm6609e1. [PMC free article] [PubMed] [Google Scholar]
- Hutton CW. Osteoarthritis: The cause not result of joint failure? Ann Rheum Dis. 1989 Nov;48(11):958–61. DOI: https://doi.org/10.1136/ard.48.11.958. [PMC free article] [PubMed] [Google Scholar]
- Aronson J. Osteoarthritis of the young adult hip: Etiology and treatment. Instr Course Lect. 1986;35:119–28. [PubMed] [Google Scholar]
- Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010 Aug;26(3):355–69. DOI: https://doi.org/10.1016/j.cger.2010.03.001. Erratum in: Clin Geriatr Med 2013 May;29(2):ix. DOI: https://doi.org/10.1016/j.cger.2013.01.013. [PMC free article] [PubMed] [Google Scholar]
- Murphy NJ, Eyles JP, Hunter DJ. Hip osteoarthritis: Etiopathogenesis and implications for management. Adv Ther. 2016 Nov;33(11):1921–46. DOI: https://doi.org/10.1007/s12325-016-0409-3. [PMC free article] [PubMed] [Google Scholar]
- Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: An integrated mechanical concept. Clin Orthop Relat Res. 2008 Feb;466(2):264–72. DOI: https://doi.org/10.1007/s11999-007-0060-z. [PMC free article] [PubMed] [Google Scholar]
- Harris WH. Etiology of osteoarthritis of the hip. Clin Orthop Relat Res. 1986 Dec;(213):20–33. DOI: https://doi.org/10.1097/00003086-198612000-00004. [PubMed] [Google Scholar]
- Murray RO. The aetiology of primary osteoarthritis of the hip. Br J Radiol. 1965 Nov;38(455):810–24. DOI: https://doi.org/10.1259/0007-1285-38-455-810. [PubMed] [Google Scholar]
- Frankel S, Eachus J, Pearson N, et al. Population requirement for primary hip-replacement surgery: A cross-sectional study. Lancet. 1999 Apr 17;353(9161):1304–9. DOI: https://doi.org/10.1016/S0140-6736(98)06451-4. [PubMed] [Google Scholar]
- Dagenais S, Garbedian S, Wai EK. Systematic review of the prevalence of radiographic primary hip osteoarthritis. Clin Orthop Relat Res. 2009 Mar;467(3):623–37. DOI: https://doi.org/10.1007/s11999-008-0625-5. [PMC free article] [PubMed] [Google Scholar]
- Cushnaghan J, Dieppe P. Study of 500 patients with limb joint osteoarthritis. I. Analysis by age, sex, and distribution of symptomatic joint sites. Ann Rheum Dis. 1991 Jan;50(1):8–13. DOI: https://doi.org/10.1136/ard.50.1.8. [PMC free article] [PubMed] [Google Scholar]
- Shao Y, Zhang C, Charron KD, Macdonald SJ, McCalden RW, Bourne RB. The fate of the remaining knee(s) or hip(s) in osteoarthritic patients undergoing a primary TKA or THA. J Arthroplasty. 2013 Dec;28(10):1842–5. DOI: https://doi.org/10.1016/j.arth.2012.10.008. [PubMed] [Google Scholar]
- Jordan J, Helmick C, Renner J, Luta G. Prevalence of hip symptoms and radiographic symptomatic hip osteoarthritis in African-Americans and Caucasians: The Johnston County Osteoarthritis Project. J Rheumatol. 2009 Apr;36(4):809–15. [PMC free article] [PubMed] [Google Scholar]
- Felson DT. Preventing knee and hip osteoarthritis. Bull Rheum Dis. 1998 Nov;47(7):1–4. [PubMed] [Google Scholar]
- Lawrence JS, Sebo M. The geography of osteoarthritis. In: Nuki G, editor. The aetiopathogenesis of osteoarthrosis. London, UK: Pitman; 1980. Apr, pp. 101-1 155–83. [ Google Scholar ]
- Mukhopadhaya B, Barooah B. Osteoarthritis of hip in Indians an anatomical and clinical study. Indian Journal of Orthopaedics. 1967;1(1):55–62. [Google Scholar]Lanyon P, Muir K, Doherty S, Doherty M. Assessment of a genetic contribution to osteoarthritis of the hip: Sibling study. BMJ. 2000 Nov 11;321(7270):1179–83. DOI: https://doi.org/10.1136/bmj.321.7270.1179. [PMC free article] [PubMed] [Google Scholar]
- Neumann G, Mendicuti AD, Zou KH, et al. Prevalence of labral tears and cartilage loss in patients with mechanical symptoms of the hip: Evaluation using MR arthrography. Osteoarthritis Cartilage. 2007 Aug;15(8):909–17. DOI: https://doi.org/10.1016/j.joca.2007.02.002. [PubMed] [Google Scholar]
- McCarthy JC, Busconi B. The role of hip arthroscopy in the diagnosis and treatment of hip disease. Can J Surg. 1995 Feb;38(Suppl 1):S13–7. [PubMed] [Google Scholar]
- Muraki S, Akune T, Oka H, et al. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: A longitudinal population-based cohort study. Arthritis Rheum. 2012 May;64(5):1447–56. DOI: https://doi.org/10.1002/art.33508. [PubMed] [Google Scholar]










{kind=link}