

Hammer toe is a common forefoot deformity characterized by an abnormal flexion of the proximal interphalangeal (PIP) joint of one or more lesser toes, most frequently affecting the second toe. Over time, this altered digital alignment can progress from a flexible imbalance to a rigid structural deformity, leading to pain, pressure points, corns, calluses, and difficulties with footwear.
While hammer toe is often treated as a localized problem of the toe itself, a broader biomechanical perspective reveals that it is usually the consequence of dysfunction within the entire lower kinetic chain — including the foot arches, ankle mechanics, tibial rotation, and even pelvic alignment. Osteopathic care offers a comprehensive and integrative approach that seeks to address both local and global contributing factors.
What Is Hammer Toe? A Clear Definition
Hammer toe is defined as a flexion deformity at the proximal interphalangeal joint, often accompanied by extension at the metatarsophalangeal (MTP) joint. In early stages, the deformity may be flexible, meaning the toe can still be manually straightened. In later stages, the soft tissues adapt, the joint capsule tightens, and the deformity becomes rigid.
The condition typically develops gradually and may initially be painless. However, progressive mechanical imbalance leads to abnormal pressure distribution during gait, particularly during the push-off phase.
Anatomy and Biomechanics of the Lesser Toes
The lesser toes consist of three phalanges connected by interphalangeal joints and anchored proximally at the metatarsophalangeal joints. Their stability depends on a delicate balance between:
- Intrinsic muscles (lumbricals, interossei)
- Extrinsic flexors (flexor digitorum longus and brevis)
- Extensor tendons
- Plantar plate and ligaments
During normal gait, the toes assist in stabilizing the forefoot and optimizing propulsion. When muscular balance is disrupted — particularly when extensors overpower intrinsic stabilizers — the toe begins to elevate at the MTP joint and flex at the PIP joint, creating the classic hammer configuration.
Causes and Risk Factors
Hammer toe rarely develops in isolation. Common contributing factors include:
- Excessive pronation or collapsed medial arch
- Long second metatarsal (Morton’s toe pattern)
- Tight footwear with narrow toe boxes
- Neuromuscular imbalance
- Diabetes-related neuropathy
- Rheumatoid arthritis
- Previous trauma
Biomechanically, chronic forefoot overload shifts tension patterns within the flexor-extensor apparatus. Over time, adaptive shortening and capsular tightening lock the toe into deformity.
Signs and Symptoms
Patients may experience:
- Visible bending of the toe
- Pain at the top of the toe due to shoe friction
- Corns or calluses
- Plantar forefoot pain (metatarsalgia)
- Reduced push-off strength
- Difficulty finding comfortable shoes
As rigidity progresses, symptoms often increase due to constant mechanical irritation.
Conventional Treatment Options
Initial management typically includes:
- Wider footwear
- Toe spacers or splints
- Protective padding
- Orthotics
- Anti-inflammatory medication
In rigid and painful cases, surgical correction may be considered. However, surgery addresses structural alignment without necessarily correcting the underlying biomechanical drivers.
Osteopathic Approach to Hammer Toe
The osteopathic perspective views hammer toe as an expression of systemic adaptation rather than an isolated digital failure. Treatment aims to restore functional balance across the kinetic chain.
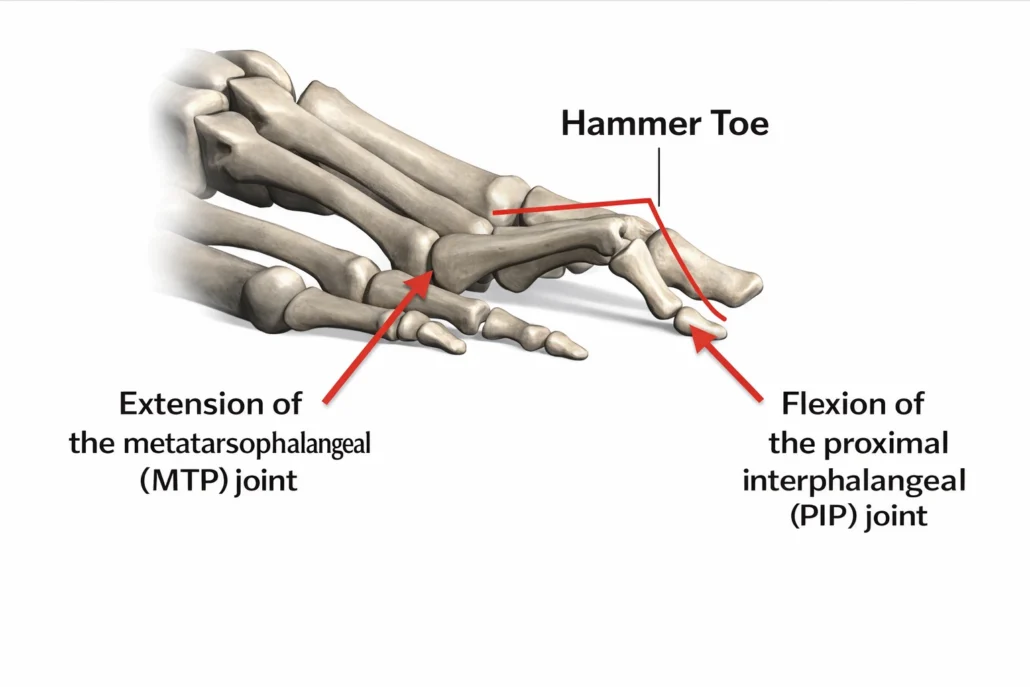
This illustration demonstrates the typical alignment seen in hammer toe, characterized by extension at the metatarsophalangeal (MTP) joint and flexion at the proximal interphalangeal (PIP) joint. The imbalance between intrinsic and extrinsic toe muscles alters normal biomechanics during gait, leading to progressive joint adaptation. Over time, this configuration may become rigid, contributing to pressure points, pain, and forefoot overload.
Key areas of assessment include:
1. Foot Arches and Load Distribution
Mobilization of the midfoot and restoration of arch dynamics reduce compensatory overload of the lesser toes.
2. Metatarsophalangeal Joint Mobility
Gentle articulatory techniques help restore MTP joint glide and reduce dorsal capsule tension.
3. Intrinsic Muscle Activation
Manual release combined with targeted strengthening encourages rebalancing between intrinsic and extrinsic muscles.
4. Tibial and Ankle Mechanics
Restricted ankle dorsiflexion often increases forefoot pressure. Improving talocrural mobility reduces compensatory toe gripping.
5. Pelvic and Postural Integration
Altered pelvic mechanics influence lower limb rotation patterns, indirectly affecting digital alignment.
Osteopathic manual techniques may include:
- Myofascial release
- Articulatory mobilization
- Counterstrain
- Functional techniques
- Fascial balancing
The objective is not merely straightening the toe, but reducing the mechanical environment that sustains the deformity.
Exercises and Practical Advice
Patients benefit from:
- Toe spreading exercises
- Towel scrunches
- Short foot exercises
- Calf stretching
- Barefoot proprioceptive training (when appropriate)
Footwear modifications are essential — wide toe boxes allow intrinsic muscle reactivation.
Prevention Strategies
- Avoid narrow shoes
- Maintain ankle mobility
- Strengthen intrinsic foot muscles
- Address pronation early
- Monitor changes in toe alignment
Early intervention during the flexible stage significantly improves outcomes.
Conclusion
Hammer toe represents more than a bent toe — it reflects a deeper biomechanical adaptation within the foot and lower limb. While conventional approaches may reduce symptoms, osteopathic care seeks to restore global balance and prevent progression.
When the body reorganizes under chronic load, the toe may become the visible messenger. Listening to that message — rather than silencing it — allows for more sustainable correction and long-term functional integrity.



















{kind=link}