

When the Body Overcompensates: More Than Just a Knee Problem
What if that persistent tension in your neck, or that strange ache in your lower back, didn’t originate where you feel it? What if the root cause lay far from the site of pain — in a knee injury that occurred months, or even years, ago?
In osteopathy, this idea isn’t just plausible — it’s foundational.
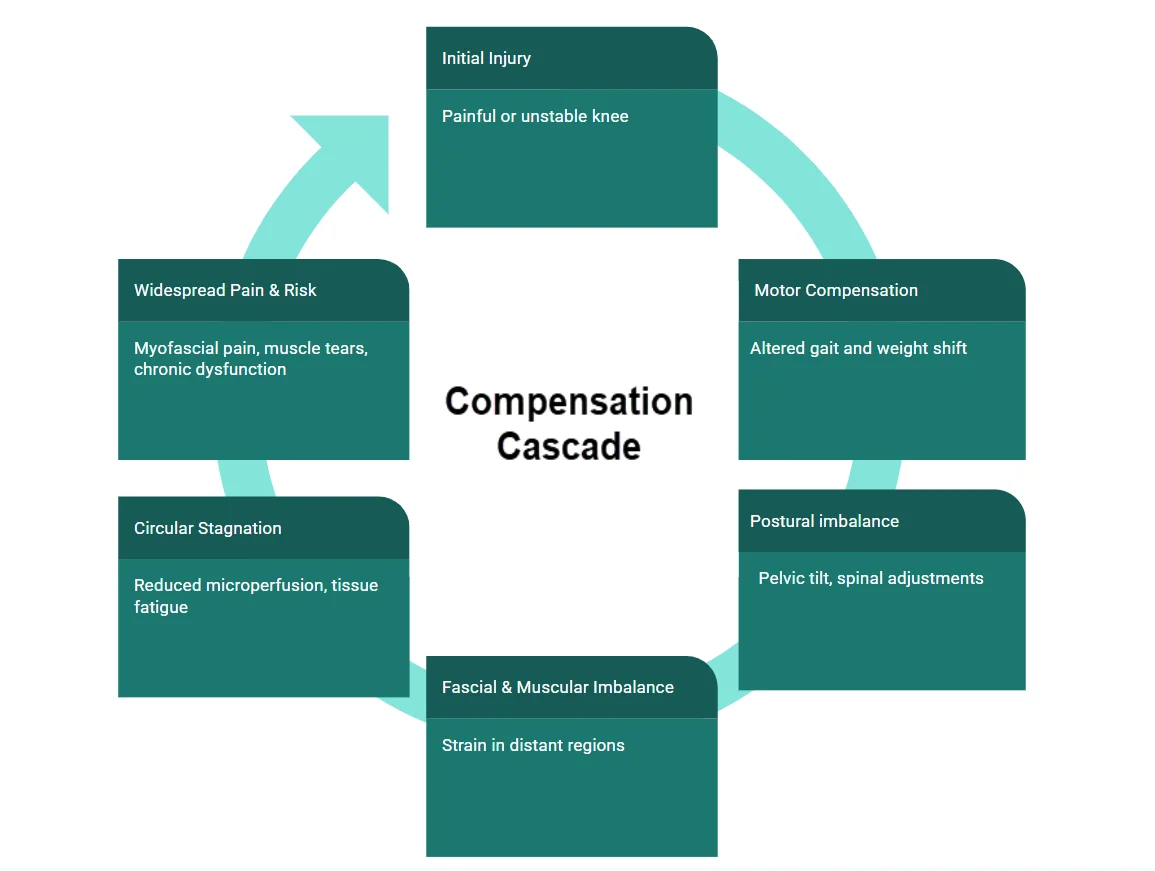
The body is a complex, interconnected system. An injury is never isolated; it’s an event that sends ripples across the fascial, muscular, neural, and vascular networks. When one part fails, the rest adapts. But that adaptation, if prolonged, becomes compensation. And compensation, if left unaddressed, can become a new source of dysfunction.
A chronic knee injury is a perfect example. It might begin with a ligament tear, a cartilage lesion, or post-surgical stiffness. Pain or instability leads the person to subtly shift their gait, redistribute their weight, and unconsciously avoid using the affected limb fully. In the short term, this is intelligent — the body’s way of protecting itself. But over time, this “new normal” triggers a cascade of structural and functional changes.
The pelvis rotates to accommodate. The opposite hip bears more load. The spine adapts its curves to maintain balance. The neck tightens to keeps the eyes level. Slowly, a web of tension forms — not pathological at first, but increasingly dysfunctional. Muscles that were once peripheral to the injury become primary actors. Fascia thickens, mobility declines, and local microcirculation is compromised. In this context, distant symptoms begin to appear: headaches, shoulder pain, plantar fasciitis, even visceral discomfort.
Just because it hurts in your back doesn’t mean the problem started there.
A past injury — even a minor one — can throw your whole system out of sync.
Many patients — and even some clinicians — fail to connect the dots. They treat the area that hurts. But they miss the deeper story: a body that has been compensating for too long, locked into a spiral of overuse, strain, and exhaustion.
This article is an invitation to read the body differently.
We’ll explore how a seemingly local issue like a knee injury can create systemic disturbances — from fascial tension and trigger point formation to myofascial pain syndromes and increased risk of muscle tears. We’ll examine how these adaptations affect circulation, proprioception, and even the emotional and symbolic layers of the body. And we’ll show how an osteopathic approach, which looks beyond the symptom to find the original lesion, can help restore not only function, but coherence and resilience.
In the clinic, we often see patients who’ve “tried everything” for their back pain, their headaches, or their unexplained fatigue — only to discover, through careful osteopathic listening, that the key was hidden in a scarred knee or a long-forgotten fall. The body remembers, even when the mind does not.
To heal is not just to treat the area of pain. It is to understand the logic of the body’s compensations, to unwind the tensions that bind it, and to listen for the silent story carried through fascia, posture, and movement.
This is the story we’ll unfold — step by step, joint by joint, from knee to chaos… and back toward balance.
Postural Adaptation: Shifting Center of Gravity to Avoid Knee Pain
When a person experiences knee pain (especially chronic or weight-bearing related), the body’s immediate instinct is to protect the joint by unloading it. This is done through a lateral shift in the center of gravity (CoG) toward the uninjured side — which has several effects:
Key Adaptation Mechanics:
✅ 1. Pelvic Elevation on the Uninjured Side
- The pelvis may hike slightly on the side of the “good leg”
- Functionally, this makes the non-injured leg “longer” — better able to absorb load
✅ 2. Trunk Shift Away from the Painful Knee
- The torso leans away from the injured side
- This decreases compressive load on the painful knee by altering the vector of gravity
✅ 3. Compensatory Shortening and Lengthening
- The gluteus medius and quadratus lumborum of the opposite side often become overactive
- Fascial tension lines (especially the lateral line and spiral line) are asymmetrically loaded
⚠️ Consequences of This Adaptation
- Creates lumbopelvic imbalance and asymmetrical gait
- Leads to chronic tightness in the thoracolumbar fascia and opposite hip
- Over time, can trigger sacroiliac pain, lumbar discomfort, or even cervical compensation
- Weakens intrinsic foot stabilizers and causes uneven loading patterns
A patient with chronic right knee pain walks with a noticeable lean to the left. The left QL and gluteus medius are hypertensed, the right hip is dropped, and over time, they develop contralateral low back pain. What began as a “simple knee issue” becomes a global postural spiral.
The Silent Spiral of Compensation
How the Body Adapts — and Why It Eventually Fails
The human body is a master of adaptation. When one area becomes compromised — like a chronically injured knee — the rest of the system instinctively reorganizes to preserve function, mobility, and equilibrium. This capacity for compensation is one of the reasons we can keep moving even when we’re hurt. But when these compensations persist, they stop being helpful and start becoming harmful.
Let’s take a closer look at what happens after a knee injury.
Initially, the body adjusts in subtle ways. The person may unconsciously reduce weight-bearing on the affected leg, shifting load toward the opposite limb. The pelvis, responding to the uneven forces, may rotate slightly or tilt asymmetrically. The lumbar spine adapts to support this shift, leading to mild scoliosis or altered curvature. Even the cervical spine may participate — the head subtly reorients to maintain gaze stability and balance. These small, nearly imperceptible changes build up over time, creating a silent but powerful spiral of compensation.
In osteopathy, we view this not merely as a local postural change, but as a global adaptation pattern. Muscles that were not meant to stabilize or support weight become primary actors: the quadratus lumborum tightens to assist hip stability, the paraspinals overactivate to maintain trunk control, and the contralateral leg begins to show signs of overuse. Fascia — the connective tissue that links all structures — thickens and loses glide, restricting motion and compressing neural and vascular pathways.
But why does this matter?
Because the body is now operating with a false sense of alignment. Movement efficiency decreases. Muscle firing patterns become less coordinated. Strain accumulates where there was none before. This doesn’t cause immediate pain — and that’s the trap. The person often believes they’ve “recovered” from the original injury because the knee no longer hurts. But in reality, they’ve simply moved the stress elsewhere.
Eventually, these compensatory areas start to speak — often loudly. Pain in the opposite hip. Tension in the thoracolumbar junction. Recurrent neck stiffness. These symptoms may appear unrelated but are part of the same chain. The body’s clever workaround is now a source of dysfunction.
Clinically, this is where confusion arises. Patients come in with back pain, unaware that it’s rooted in a gait imbalance from an old knee trauma. They’ve tried stretching, strengthening, even imaging — all focused on the area that hurts. But no intervention seems to “hold.” The pain keeps coming back because the primary cause remains untreated.
From an osteopathic perspective, this is the critical moment: to trace the body’s story backward, to follow the trail of adaptation to its origin. It’s not about treating the symptom — it’s about restoring the integrity of the system. This requires palpatory listening, an understanding of compensatory hierarchies, and a map of how the body’s kinetic chain reacts under chronic stress.
Left unchecked, this spiral leads to increased energy expenditure, decreased functional reserve, and eventual tissue breakdown — not just in the knee, but in distant regions like the sacrum, scapular stabilizers, or even the cervical spine. What began as a localized biomechanical issue becomes a systemic somatic burden.
The key insight here is this: compensation is not dysfunction — until it is.
The body doesn’t lie, but it does whisper. And in the early stages of this spiral, those whispers are easy to miss. This is why prevention, early intervention, and a holistic view are essential — not just to resolve pain, but to preserve the intelligence of the body’s movement and adaptation patterns.
Fascia, Fatigue and the Microcirculatory Trap
When Movement Stops Flow: Understanding Local Stagnation
The body is not only mechanical — it is fluid. Every movement, every muscular contraction, every breath supports a deeper rhythm: the continuous flow of blood, lymph, and interstitial fluids. This circulation doesn’t just nourish; it clears, it cools, it regenerates. And when it slows — or worse, stagnates — tissue health begins to suffer.
In the context of chronic compensation, as seen following a knee injury, one of the most insidious consequences is not pain or loss of mobility, but a silent degradation of microcirculation in overloaded tissues.
Fascia and Flow: An Inseparable Pair
Fascia is not just a passive envelope around muscles — it’s a dynamic, innervated, and vascularized structure. When healthy, fascia glides, transmits force, and supports vascular flow. But under chronic tension, it becomes thickened, less elastic, and begins to act like a compressive cuff.
In regions where muscles are recruited to compensate — such as the contralateral quadriceps, paraspinal muscles, or gluteal stabilizers — the fascia surrounding them becomes densified. This loss of sliding impairs venous and lymphatic return, creating a localized pressure build-up. Even if arterial input continues, outflow is restricted, and with it, the clearance of metabolic waste products like CO₂, hydrogen ions, and inflammatory mediators.
Hypoxia, Acidosis, and Pain Sensitization
When tissues become hypoxic — even mildly — their pH drops. Acidity affects both nerve endings and the surrounding matrix. Nociceptors (pain receptors) become more sensitive in an acidic environment, even to normal pressure or stretch. This is why patients often report tenderness on palpation, even in areas that don’t seem injured.
Moreover, the build-up of pro-inflammatory molecules such as prostaglandins and bradykinins further irritates local nerves and perpetuates the state of vigilance in the tissue. Over time, these chemical messengers may spill into the bloodstream, triggering more generalized symptoms like fatigue, malaise, or brain fog — especially in sensitive individuals.
From a fascia-centric view, this situation resembles a functional ischemia — not because of a blocked artery, but due to an internal pressure system gone awry. This process is especially visible in muscular compartments like the thoracolumbar area or interscapular region, where multiple compensations converge.
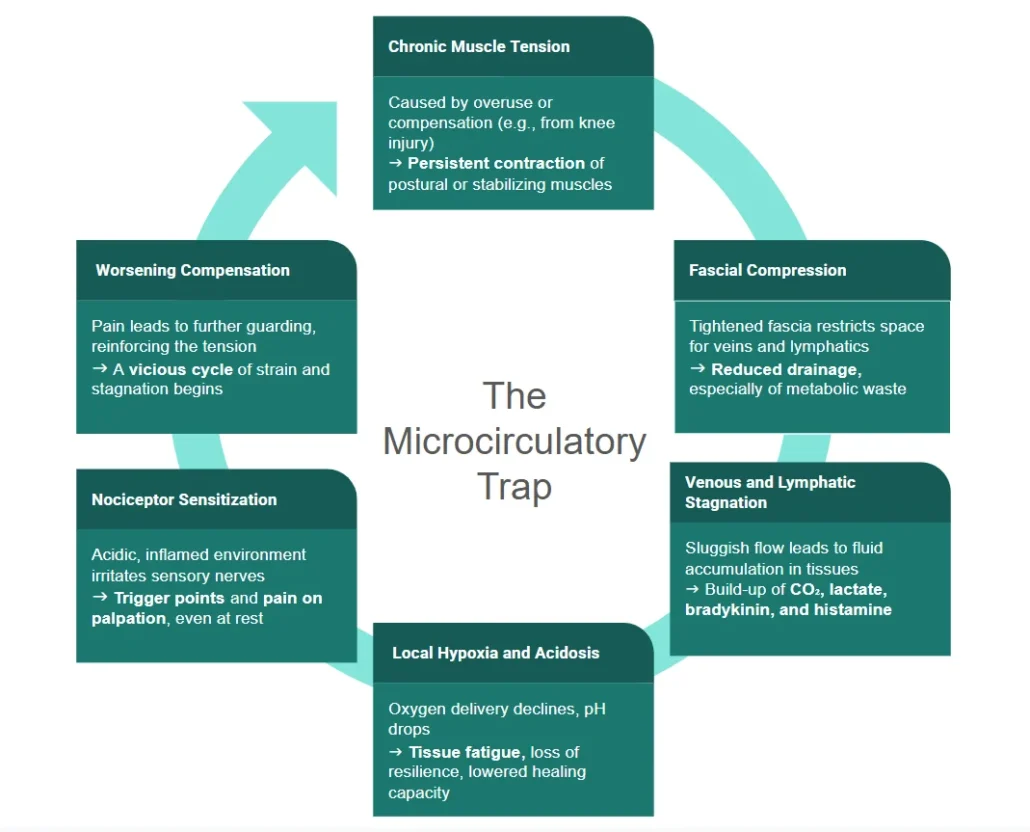
A Downward Spiral of Effort and Exhaustion
This microcirculatory trap becomes self-reinforcing. The more a muscle compensates, the more it tightens. The tighter it gets, the more it compresses its own vessels. As circulation declines, fatigue sets in faster. The muscle becomes stiff, painful, and ultimately less efficient — which forces adjacent muscles to step in, spreading the dysfunction even further.
From an osteopathic lens, this state of tissue congestion is not inert — it’s active, reactive, and reversible. But only if we can restore mobility and pressure differentials that favor normal drainage. Osteopathic techniques such as myofascial release, balanced ligamentous tension, or gentle pumping can help reestablish physiological glide and circulation.
Clinical Signs Not to Miss
Patients caught in this trap may not show “clear pathology” on imaging, but they present with:
- Localized pain that worsens with sustained posture
- Sensation of heaviness, stiffness, or “blocked” areas
- Tender points in muscles that are overused but not injured
- Unusual fatigue after minor efforts
- Poor response to stretching or strengthening protocols alone
These signs call for a different approach — one that listens to the tissue’s metabolic state, not just its range of motion.
In the end, movement is life — but only when that movement sustains flow. A body compensating too long may still walk, still bend, still lift… but it does so under strain, often without the circulatory vitality needed for true healing. Recognizing this hidden stagnation is a key step in unraveling the full story behind chronic pain and persistent dysfunction.
Trigger Points and the Illusion of Distance
Why Pain Shows Up Where the Problem Isn’t
One of the most confusing — and revealing — aspects of chronic musculoskeletal dysfunction is the disconnect between the site of pain and the site of origin. A patient may complain of persistent neck tension or a sharp pain between the shoulder blades, yet the root cause lies in a compensatory chain triggered by an old knee injury. This phenomenon is not only real — it is fundamental to understanding myofascial trigger points and their deceptive referral patterns.
The Anatomy of a Trigger Point
A trigger point is a hyperirritable spot located in a taut band of skeletal muscle or its fascia. These points are not just tight — they are biochemically active. Studies have shown elevated concentrations of inflammatory molecules, lower pH, and sustained electrical activity in these zones. Under pressure, they reproduce the patient’s familiar pain — often in a completely different region.
This is the clinical challenge: the body doesn’t always hurt where it suffers. In the context of a knee injury, muscles recruited to compensate — like the quadratus lumborum, gluteus medius, or thoracic paraspinals — begin to overwork. Over time, they develop trigger points that refer pain upward or downward, giving rise to seemingly unrelated symptoms: a stiff neck, tension headaches, or burning pain around the scapula.
Referred Pain: The Invisible Map
Each muscle has a predictable referral pattern. For example:
- Gluteus minimus trigger points may refer pain down the lateral thigh, mimicking sciatica.
- Levator scapulae trigger points often radiate to the medial border of the scapula and posterior neck.
- Soleus trigger points can cause deep ankle or heel pain, especially during gait.
These maps were painstakingly documented by Travell and Simons, and remain a powerful diagnostic tool. But they are often overlooked in conventional practice, where imaging is prioritized over palpation, and symptoms are treated in isolation.
From an osteopathic perspective, this is precisely where manual medicine shines: we listen with our hands. By palpating along fascial chains, observing compensatory postures, and tracing tension lines, we identify the primary lesion hidden beneath secondary symptoms.
The Fascial Continuum of Pain
Trigger points do not live in isolation. They are embedded in a fascial continuum — a web that links muscles, bones, organs, and even the nervous system. When fascia loses its glide and becomes densified, the likelihood of pain referral increases. What’s more, tension in one area can load another — like pulling a wrinkle across a bedsheet.
For example, if the right knee is dysfunctional, the left piriformis may overcompensate, pulling on the sacrum and altering lumbar lordosis. This, in turn, creates tension in the thoracolumbar junction, where trigger points form in the multifidus or iliocostalis. A patient may then present with mid-back pain that worsens when sitting or turning, unaware that it traces back to gait asymmetry.
Treating the Source, Not the Shadow
Osteopathic treatment aims not just to deactivate trigger points — though that is part of it — but to understand why they appeared. What biomechanical demand created them? What fascial restriction sustains them? What distant injury initiated the pattern?
When we address the primary dysfunction — in this case, the old knee injury — the satellite symptoms often dissolve. The trigger points fade. The postural strain corrects itself. This is what distinguishes structural thinking from symptomatic chasing.
In the end, pain is a messenger — but not always a reliable narrator. It tells us something is wrong, but not where or why. The illusion of distance is part of the body’s brilliance — and its complexity. As osteopaths, our task is to see beyond the site of pain, to read the deeper story inscribed in the tissue, and to guide the body back toward balance and clarity.
The Risk of Muscle Tear in a Body on Edge
Why Compensation Makes Us More Vulnerable to Injury
At first glance, the human body appears strong and adaptable — and it is. But beneath this resilience lies a fragile balance. When an area like the knee becomes dysfunctional, the rest of the body rushes to compensate. While this allows for short-term function, it comes at a long-term cost: compensatory overload. And when that cost accumulates, the risk of acute injuries like muscle tears increases — often far from the original problem.
This isn’t just theoretical. Clinically, we see it time and time again: a hamstring tear in someone with an old knee sprain, a groin strain in a patient with hip compensation, a calf rupture after months of postural asymmetry. These injuries are rarely isolated accidents — they are the final snap in a system already overstretched.
How Compensation Sets the Stage for Tearing
When the knee can no longer function normally — due to pain, instability, or limited mobility — the body naturally redistributes load. This often leads to:
- Overuse of contralateral muscles (e.g., left hamstring compensating for a right knee)
- Altered movement timing in muscle groups (e.g., delayed activation of stabilizers)
- Tension accumulation in support structures (e.g., iliotibial band, soleus, erector spinae)
These patterns are subtle at first but become embedded in motor programs over time. Muscles that are meant for brief, dynamic support are now working constantly. They don’t get a chance to fully recover. This leads to microtrauma, metabolic fatigue, and fascial densification.
The Danger of Subtle Imbalances
The problem is that the body often hides its fatigue until it’s too late. A patient might feel “tight” but not injured — until one unexpected movement (a sprint, a misstep, lifting a heavy object) triggers a sharp tear. The underlying tissue was already compromised — not because of direct trauma, but because it had been compensating beyond its functional limits.
Think of a rubber band left under tension for too long. It doesn’t snap the first day. It stretches, strains, thins… and then, with one extra pull, it breaks.
In a compensatory body, force vectors are no longer optimal. Muscles contract in shortened or lengthened states. Joints move off-axis. Even proprioception — our sense of body position — becomes less accurate. These biomechanical faults increase the likelihood of overstretching or tearing a tissue that’s already fatigued.
Typical At-Risk Areas in Compensation Chains
- Hamstrings – especially in altered gait or pelvic tilt
- Adductors – in asymmetrical loading or hip instability
- Calves and soleus – in forefoot overload from poor knee extension
- Paraspinals – in compensatory spinal curves
- Rotator cuff muscles – especially supraspinatus, in scapular imbalance
Each of these areas is commonly recruited to “fill in the gap” left by dysfunction elsewhere — and each is prone to injury when pushed too far.
Osteopathic Insight: Prevention Is in Restoration
In osteopathy, we do not wait for the tear to appear. The goal is to recognize patterns of overload before they break down into acute injury. This means:
- Identifying areas of chronic hypertonicity and loss of resilience
- Restoring joint mechanics in dysfunctional segments (like the knee)
- Rebalancing fascial tensions along kinetic chains
- Teaching patients to move with awareness and symmetry again
Manual therapy, when combined with proprioceptive retraining and load management, can reverse the vulnerability created by chronic compensation.
Conclusion: Don’t Blame the Movement — Blame the Pattern
When a muscle tears, we tend to blame the moment: the sprint, the jump, the twist. But the true culprit often lies in months or years of silent strain, in a body compensating for something it couldn’t heal on its own.
Osteopathy offers a different lens — one that sees the system, not just the symptom. And in doing so, it helps protect the body not only from pain, but from breaking.
Somatic Memory and the Body’s Global Alarm System
Can One Knee Alter the Whole Being?
In the osteopathic world, we often hear it: “It’s just a knee.” But the body doesn’t think in isolated parts — it functions as a complex, unified organism. And when a joint as fundamental as the knee is injured, the repercussions ripple far beyond ligaments or gait mechanics. Over time, that one injury can reverberate through the nervous system, the fascia, and even the psyche, creating what might be called a global somatic alarm state.
This is not abstract theory — it’s observable in clinical practice.
The Body Remembers
The concept of somatic memory refers to the body’s capacity to encode and retain the imprint of physical trauma. When an injury occurs, especially if accompanied by fear, frustration, or helplessness, the nervous system doesn’t just manage the pain — it also stores the emotional tone of the experience.
In a chronic knee injury, this can manifest as:
- Protective posturing, long after the tissue has healed
- A persistent sense of vulnerability on that side
- Guarded movement, even unconsciously
- Amplified pain response to benign stimuli (central sensitization)
The body, in effect, acts as if the danger is still present — not because of the tissue, but because of the nervous system’s learned vigilance.
The Role of the Autonomic Nervous System
Ongoing compensation leads to increased sympathetic tone — the fight-or-flight arm of the autonomic nervous system. This state is not just about stress; it’s a physiological state of preparedness. The problem is, when this tone becomes the new baseline, the entire body begins to function as if it’s under constant threat.
- Heart rate variability decreases
- Breathing becomes shallow and chest-dominant
- Digestive function slows
- Fascial tone increases, preparing for defense
- Microcirculation diminishes, as blood flow prioritizes core survival zones
In this context, a simple trigger — a long walk, a postural challenge, a stressful event — can push the system over its limit. What began as a knee issue now echoes through the entire neurofascial matrix.
The Polyvagal Perspective
The polyvagal theory, developed by Dr. Stephen Porges, helps us understand this from a broader view. When the body shifts into chronic defense (even subtly), the vagus nerve’s calming, parasympathetic influence weakens. The result? A nervous system locked into a low-grade state of defense — vigilant, stiff, and hypersensitive.
This can explain why patients with chronic compensation patterns often present with:
- Difficulty relaxing
- Worsening symptoms under emotional stress
- Inconsistent pain patterns
- A sense that “everything is connected — and everything hurts”
They’re right — it is.
Osteopathy: Rebalancing the Global Alarm
Osteopathic care offers a unique doorway out of this loop. Gentle techniques like cranial osteopathy, balanced ligamentous tension, and facilitated unwinding help restore the parasympathetic tone and encourage a more coherent somatic dialogue.
It’s not just about correcting biomechanics — it’s about downregulating the alarm system that keeps the body in a defensive loop.
By working with respiration, fascia, and subtle palpation, the osteopath can help the system feel safe again. And when the body no longer feels under threat, it can begin to release its compensations, soften its tone, and recover its innate adaptability.
Osteopathic Approach: Treating the Pattern, Not Just the Pain
From Listening Hands to Systemic Healing
By the time most patients arrive in an osteopath’s clinic, they’ve already followed the classic route: localized treatment, imaging, painkillers, maybe physiotherapy. And still, the pain persists. What they often lack is not more therapy, but a different lens — one that sees the body as an integrated whole, where a distant knee injury might be quietly destabilizing the shoulder, the spine, or even the breath.
This is the strength of osteopathy: we treat not just the site of pain, but the logic behind its appearance.
Listening Before Correcting
Every effective osteopathic intervention begins with listening — through the hands, the observation, and the patient’s narrative. The goal is not to chase symptoms but to trace patterns of dysfunction.
For example, a patient with chronic neck pain may demonstrate:
- A rotated pelvis due to compensatory gait
- Overactivity in the thoracolumbar fascia
- Reduced diaphragmatic motion
- Guarded proprioception on the side of a prior knee trauma
This global picture reveals what imaging often misses: the pain is local, but the dysfunction is global and relational.
Techniques to Unwind the System
Osteopathy offers a wide range of tools to address these patterns. The choice of technique depends not just on the tissue but on what the body is ready to release.
1. Myofascial Release
Reestablishes fascial glide in overloaded areas. Key zones: thoracolumbar fascia, iliotibial band, cervical-thoracic junction.
2. Balanced Ligamentous Tension (BLT)
Excellent for joints that have adapted structurally, like a tibiofemoral joint subtly misaligned post-injury.
3. Visceral and Diaphragmatic Techniques
Chronic compensation often compromises respiratory dynamics. Treating the diaphragm, psoas, and visceral suspensory ligaments restores fluidity to the central body axis.
4. Cranial Osteopathy
Especially powerful in cases of autonomic dysregulation, persistent tension, or somatic memory. Balancing craniosacral rhythms helps downregulate the global alarm system.
5. Functional and Indirect Techniques
Gentle methods that allow tissues to find ease, excellent when the body is reactive, fatigued, or in a protective mode.
These techniques are not chosen randomly, but based on the body’s hierarchy of needs. The aim is not just to fix structure but to restore adaptability — the true foundation of health.
Beyond Hands: Education and Reintegration
Treatment doesn’t end on the table. In cases of chronic compensation, patients need help relearning how to move and sense their bodies.
Key tools:
- Mirror gait retraining to break asymmetrical walking habits
- Breathwork to restore diaphragmatic function and vagal tone
- Proprioceptive drills to reactivate dormant stabilizers
- Micro-movement awareness to reconnect with subtle internal cues
The osteopath becomes not just a technician, but a movement educator, helping the patient out of patterns that have become unconscious prisons.
Treat the Person, Not the Lesion
Ultimately, osteopathy is not a system of techniques — it’s a philosophy. We’re not just fixing a joint or stretching a muscle. We’re helping the body remember how to coordinate, how to breathe, how to trust its own balance again.
When we treat the pattern — not just the pain — we give the person back access to their own intelligence. And in many cases, it’s not about adding more force, but removing the interference that prevents the system from healing itself.
Clinical Checklist: Clues That the Primary Lesion Is Elsewhere
A Guide for Practitioners and Patients
One of the core challenges in clinical practice is determining whether the site of pain reflects the origin of dysfunction — or merely the end result of a long compensatory chain. For osteopaths, this question is fundamental. Because when the primary lesion is missed, treatments remain superficial, symptoms recur, and the patient loses trust in their own healing process.
To help orient the diagnostic process, this section offers a clinical checklist of signs that suggest the pain is not where the problem started — but where the compensation has failed.
Key Indicators of a Compensatory Pain Pattern
- Pain migrates or shifts location
The patient reports that the pain “travels” or moves over time.
Example: From the hip, to the back, then to the neck — with no clear injury at each site. - Standard imaging is unremarkable
X-rays, MRI, or ultrasound show no structural damage at the symptomatic site.
Suggests a functional, not anatomical, disturbance. - Symptoms worsen with fatigue or emotional stress
Pain flares under load, after workdays, or during periods of tension.
Often a sign of autonomic involvement or body-wide adaptation limits. - Tension patterns are asymmetrical
One side of the body consistently more restricted or overactive.
Palpation reveals chronic hypertonicity on the side opposite a known injury. - The original trauma is distant in time and space
A knee sprain from 3 years ago… and today, the patient presents with thoracic pain.
The injury was never fully integrated or corrected, and the chain adapted. - The patient describes “fragile” stability
”I feel fine — until I do too much.”
The body is functioning on a narrow margin of resilience. - Manipulative therapy gives short-lived relief
Symptoms improve briefly after massage, adjustments, or stretching — but always return.
Indicates the primary driver was not addressed.
Palpatory Clues for Osteopaths
- Reduced diaphragmatic mobility on the side of a distant injury
- Inhibition or hypoactivity in deep stabilizers (e.g., transversus abdominis, multifidus)
- Fascial densification in planes opposite the site of pain
- Delayed proprioceptive response during movement testing
- Painful trigger points not aligning with the patient’s description of the trauma
Red Flags That You’re Treating the Wrong Site
- No long-term improvement despite targeted therapy
- New symptoms appearing elsewhere after treating the original pain
- The patient reports “something feels off” even after “correction”
- Movement quality improves, but load tolerance does not
Conclusion: The Site of Pain Is a Clue, Not a Conclusion
When a patient presents with pain, it’s the start of a conversation — not the answer. Pain marks the site where compensation has collapsed, not necessarily where dysfunction began. The real work of osteopathy is to follow the trail backward, with clarity, patience, and systemic vision.
Case Study: The Knee That Echoed Into the Neck
Real-Life Scenario and Osteopathic Resolution
Patient: Marianne, 42 years old, marketing executive
Chief Complaint: Persistent neck stiffness and headaches for 8 months
Previous Treatments: Physiotherapy, cervical traction, ergonomic assessment, analgesics
Imaging: Normal cervical X-ray and MRI — no disc lesion, no arthrosis
Osteopathic Finding: A 6-year-old medial meniscus injury on the left knee — never surgically treated, resolved “spontaneously”
Initial Presentation
Marianne arrived with a classic complaint: “I wake up with neck pain that builds into a headache by the afternoon.” She described tension behind her eyes, stiffness when turning her head, and occasional numbness in her fingers. Her posture was slightly anterior, head forward, shoulders tight. Most clinicians had focused on her cervical spine — and understandably so.
But something didn’t add up. Her cervical ROM was limited, but not structurally blocked. Her trapezius and levator scapulae were hypertonic, yet unresponsive to release work. Her pain migrated slightly from day to day — and became much worse when she was fatigued or stressed.
In her history, one detail stood out: a “healed” left knee injury from a skiing accident six years prior. No surgery, just rest. She had “compensated” and continued working, walking, living. The knee no longer hurt — but her body remembered.
Assessment and Osteopathic Hypothesis
On examination:
- Left knee extension was subtly reduced, with compensatory tension in the popliteus and vastus lateralis.
- Pelvic rotation was evident: the left hemipelvis was posteriorly rotated, with sacroiliac asymmetry.
- Right quadratus lumborum and thoracolumbar fascia were densified, suggesting lateral chain compensation.
- Fascial lines traced a continuous tension from the left leg up to the right scapula.
- Cervical palpation revealed protective hypertonicity rather than acute spasm.
The picture became clear: the knee injury had created a spiral of mechanical adaptations, gradually migrating tension toward the cervico-thoracic junction. The neck was the last point in a long kinetic chain failure.
Treatment Strategy
Treatment began not with the neck, but with the foundation.
Session 1–2: Releasing the base
- Myofascial release of left IT band and popliteus
- BLT to left tibiofemoral joint
- Sacroiliac balancing with functional technique
- Thoracolumbar decompression
Session 3–4: Restoring integration
- Diaphragmatic mobility work (noted shallow upper-chest breathing)
- Fascial balancing along the deep front line
- Cranial-sacral support to help calm sympathetic tone
Session 5: Local cervical support
- Functional release of scalenes and levator scapulae
- Facilitated unwinding of upper thoracic cage
Outcome
After the third session, Marianne reported:
“My neck feels lighter — and strangely, my left leg feels more grounded.”
By the fifth session, her headaches had vanished, and she had resumed working without ergonomic pain. Most strikingly, she began noticing that her gait had changed — walking felt smoother and more symmetrical. The neck hadn’t been “fixed” — the system had been realigned.
Clinical Takeaway
This case exemplifies the osteopathic principle: don’t chase the pain — trace the pattern. Marianne’s neck symptoms were real, but they were not primary. Her body had done its best to adapt to a forgotten injury. Osteopathy helped reveal the deeper truth: that health is not only about what hurts, but about where function was lost.
Prevention and Education: Avoiding the Compensation Cascade
Empowerment Through Movement and Awareness
One of the most powerful tools in osteopathic care is not a technique — it’s education. While manual therapy can restore mobility and rebalance tension, long-term healing depends on the patient’s understanding of their own body. Preventing the spiral of compensation that follows a localized injury — like a knee lesion — requires early detection, conscious re-education, and proactive self-care.
Because the body is brilliant at adapting… but even brilliance has limits
Early Signs the Body Is Compensating
The compensation process is subtle at first. Patients don’t feel pain — they feel “off.” That’s when intervention is most effective. Key warning signs include:
- A sensation of walking “unevenly”
- One shoe wearing down faster than the other
- Fatigue after minimal activity, especially asymmetrically
- Subtle shifts in posture (e.g., one shoulder always elevated)
- Discomfort when lying symmetrically on the back
- “Phantom” pains — sensations that come and go without clear origin
These signs are invitations — not failures. The body is communicating, asking for realignment before breakdown occurs.
Patient Education: Restoring Body Literacy
Helping patients reconnect with their somatic signals is a cornerstone of preventive osteopathy. Key strategies include:
1. Movement Mindfulness
Teaching patients to observe how they move — not just that they move. Simple practices:
- Walking barefoot at home and noticing weight distribution
- Filming short walking clips to detect lateral deviations
- Standing in front of a mirror with eyes closed, then opened, to reveal compensations
2. Breathing Awareness
Compensation often restricts diaphragmatic motion. Encourage:
- Daily diaphragmatic breathing (3–5 minutes)
- Side-lying breath checks to compare rib expansion
- Gentle thoracic mobility work with a roller or towel
3. Functional Asymmetry Testing
Simple at-home checks can alert the patient:
- Can you balance on each leg for 30 seconds?
- Can you sit cross-legged comfortably on both sides?
- Is one ankle always tighter?
These are not diagnostic — but directional.
Preventive Treatment Timing
Osteopathic care shouldn’t begin when pain is chronic — it’s most effective when used proactively:
- After a knee sprain, even if “it’s healed”
- Post-surgery, even if the joint is replaced
- After periods of prolonged immobilization or bracing
- Following childbirth or major life stressors
These are windows of vulnerability when compensation is most likely to begin. A few osteopathic sessions at this stage can prevent years of dysfunction.
Bridging the Gap with Movement Professionals
Osteopaths don’t replace movement educators — we collaborate. Referring patients to:
- Feldenkrais practitioners
- Postural re-education specialists
- Somatic educators or mindful movement therapists
… reinforces the sensory learning initiated in the treatment room.
True prevention happens when the patient becomes an active participant, not a passive recipient.
Symbolic Dimension: When the Knee Speaks for the Whole Self
Psychosomatic Echoes of a Physical Injury
In osteopathy, we learn to listen to the body — not just as a mechanical system, but as a living expression of the person. Beyond fascia, joints, and gait, there is a story: one that sometimes speaks more through symptoms than through words. And in that story, a knee injury is never just a knee injury.
For many patients, especially those with chronic compensation patterns, the body begins to reflect deeper themes — of fear, of control, of collapse and resistance. When the knee falters, it may be more than a biomechanical loss — it may also represent a symbolic destabilization.
The Knee as a Locus of Flexibility and Submission
Anthropologically and symbolically, the knee is associated with:
- Humility (to kneel before something greater)
- Adaptability (to bend without breaking)
- Support and stability (as a hinge between mobility and grounding)
When the knee is injured and becomes rigid, guarded, or unstable, we may ask: What in this person’s life has lost flexibility? What are they resisting bending to?
A patient who refuses to slow down after injury, who resents needing help, who fears loss of control — may be embodying this inner tension in the joint meant to soften and adjust.
Trauma, Control, and the Protective Body
For some individuals, the onset of physical compensation parallels an emotional defense. A sudden injury may:
- Reinforce beliefs of vulnerability
- Trigger past experiences of helplessness
- Challenge identity (e.g., “I’m strong — I don’t break”)
- Evoke shame or fear around losing independence
The body, in response, begins to armor itself. It over-recruits. It tenses. It refuses to move where it once flowed. This is not weakness — it is a form of wisdom, an attempt to survive through structure when emotion feels unsafe.
Reading the Fascia as Narrative
In osteopathic palpation, we often sense more than texture. The body may reveal:
- A sudden densification in an area when discussing a memory
- A holding pattern that resists release, until trust is established
- A shift in breath or tone when we approach the origin of pain — or its emotional counterpart
The fascia remembers what the mind forgets. And sometimes, a chronic dysfunction persists not because it is untreated, but because it is unresolved.
Inviting Integration Through Therapeutic Presence
To accompany a patient through this process is not to psychoanalyze them — but to hold space. To notice when a release is more than physical. To witness when posture shifts and emotion follows. To offer touch that is not only corrective, but compassionate.
This is where osteopathy becomes more than structural — it becomes relational and symbolic. The practitioner becomes a guide, not only toward alignment, but toward re-integration of self.
Conclusion: Healing the Whole by Listening to the Origin
A knee injury seems simple — a twisted joint, a damaged ligament, a scar left behind. But as we’ve explored, its impact may be far from local. In truth, the body does not work in parts. It compensates, connects, adapts. It absorbs dysfunction like a sponge — until it can’t anymore.
This is where pain reappears, not as a signal of new damage, but as a cry for coherence.
From Symptom to System
By following the journey of a single injury, we’ve uncovered a cascade of physiological and somatic consequences: muscular overload, fascial stagnation, postural distortion, microcirculatory stress, and ultimately, systemic fatigue. We’ve seen how pain can radiate away from its cause, how trigger points mask their origins, and how the nervous system — when trapped in vigilance — locks the body into a state of protection and contraction.
We’ve also witnessed how an osteopathic approach, rooted in touch, observation, and narrative, can reverse this spiral — not by “fixing” the site of pain, but by realigning the pattern and reawakening the body’s own intelligence.
A Call for a Broader Understanding
This article is more than a case study on chronic compensation. It’s an invitation.
An invitation to see pain not only as a dysfunction to eliminate, but as a message to decode.
An invitation to see the body not as a puzzle of isolated segments, but as a living continuum of motion, memory, and meaning.
An invitation to treat patients not just where they hurt, but where they adapted — and perhaps, where they broke silently.
Because if we only treat the end of the story, we risk missing the truth hidden in its beginning.
Restoring Balance Is Not a Linear Process
Healing from long-standing compensation patterns is not a one-session miracle. It often requires:
- Time
- Dialogue
- Recoding of movement
- Release of guarded patterns — both physical and emotional
- Reconnection to breath, space, and bodily sovereignty
It is not always comfortable. But it is deeply human.
The osteopath’s role in this process is both technical and relational. We mobilize, unwind, rebalance — but we also witness, reflect, and guide. We are there to remind the body of its original coherence — and help the person feel safe enough to return to it.
No Final Word — Only New Questions
There is no perfect closure to this kind of journey. And maybe there shouldn’t be.
Instead of ending with answers, let us leave with questions:
- What old injuries are we still carrying — not just in our joints, but in our habits and silences?
- Where have we compensated in life, not just in posture?
- What part of ourselves might unfold differently if we felt more aligned, more supported — more heard?
As osteopaths, we work with bodies. But in truth, we work with histories. And every pain, every shift, every asymmetry holds the echo of something that once mattered — and still matters.
Perhaps the greatest act of care is not to fix what’s broken, but to help the body remember it was never truly disconnected — only diverted.
References
1. Fascial Compensation and the Common Compensatory Pattern (CCP)
- Boesler, D. R. (2014). Common Compensatory Pattern – Treatment in a Busy Practice.
- Discusses the CCP’s role in structural evaluation and treatment, emphasizing the importance of fascial patterns in osteopathic practice.
2. Somatic Dysfunction and Its Clinical Relevance
- Fryer, G. (2016). Somatic dysfunction: An osteopathic conundrum.
- Explores the concept of somatic dysfunction, its diagnostic criteria, and its significance in modern osteopathic medicine.
3. Fascial Tissue Research in Sports Medicine
- Schleip, R., et al. (2018). Fascial tissue research in sports medicine: from molecules to tissue adaptation, injury and diagnostics.
- Provides insights into the role of fascial tissues in sports medicine, highlighting their adaptability and response to mechanical stress.
4. Fascial Aspects in Osteopathic Practice
- Tozzi, P. (2012). Selected fascial aspects of osteopathic practice.
- Examines the significance of fascia in osteopathic treatment, discussing techniques aimed at releasing fascial tensions.
5. Reconceptualizing Somatic Dysfunction
- Liem, T., & Lunghi, C. (2023). Reconceptualizing Principles and Models in Osteopathic Care: A Clinical Application of the Integral Theory.
- Proposes a new framework for understanding somatic dysfunction, integrating neuroaesthetic principles into osteopathic assessment.
6. Fascial Distortion Model (FDM)
- Typaldos, S. (1994). Introducing the Fascial Distortion Model.
- Introduces the FDM, an anatomical perspective on musculoskeletal injuries based on specific pathological alterations in connective tissues.
7. Somatic Memory and Its Role in Osteopathy
- Hanna, T. (1988). Somatics: Reawakening the Mind’s Control of Movement, Flexibility, and Health.
- Discusses the concept of somatic memory and its implications for movement and health, foundational for understanding chronic compensation patterns.
8. Osteopathy and Mental Health
- Liem, T., & Neuhuber, W. (2020). Osteopathic Treatment Approach to Psychoemotional Trauma by Means of Bifocal Integration.
- Explores the intersection of osteopathic treatment and mental health, emphasizing the body’s role in processing emotional trauma.
9. Fascial Elements in Osteopathic Practice
- ACS College. (2019). The Fascial Element in Osteopathic Practice – Part Two.
- Highlights the efficacy of fascial osteopathic treatment, particularly in post-operative care and various dysfunctions.
10. Fascia in Osteopathy
- Ladewig, M. (Year Unknown). Fascia in Osteopathy.
- A comprehensive thesis discussing the anatomy, physiology, and application of the fascial system in osteopathic practice.
11. The Common Compensatory Pattern (CCP)
- Zink, G. T., & Lawson, W. B. (1979). The Common Compensatory Pattern: Its Origin and Relationship to the Postural Model. This foundational work introduces the CCP, detailing how fascial patterns influence postural adaptations and compensatory mechanisms in the body.
12. Somatic Dysfunction in Osteopathy
- Fryer, G. (2016). Somatic dysfunction: An osteopathic conundrum. This article critically examines the concept of somatic dysfunction, its diagnostic challenges, and its relevance in contemporary osteopathic practice. ScienceDirect
13. Fascial Tissue Research in Sports Medicine
- Zügel, M., Maganaris, C. N., Wilke, J., et al. (2018). Fascial tissue research in sports medicine: from molecules to tissue adaptation, injury and diagnostics. This consensus statement provides a comprehensive overview of the role of fascial tissues in sports medicine, emphasizing their adaptability and significance in injury prevention and rehabilitation. British Journal of Sports Medicine+6ResearchGate+6PubMed+6
14. Fascial Aspects in Osteopathic Practice
- Tozzi, P. (2012). Selected fascial aspects of osteopathic practice. This paper discusses the importance of fascia in osteopathic treatment, highlighting techniques aimed at releasing fascial tensions to restore function.
15. Reconceptualizing Somatic Dysfunction
- Liem, T., & Lunghi, C. (2023). Reconceptualizing Principles and Models in Osteopathic Care: A Clinical Application of the Integral Theory. This work proposes a new framework for understanding somatic dysfunction, integrating neuroaesthetic principles into osteopathic assessment.


 Weakness: Causes, Implications, and Solutions")















{kind=link}