

Introduction — When leg pain isn’t always sciatica
Pain that radiates down the buttock, the back of the thigh, or sometimes even the calf often immediately brings sciatica to mind. For many people, the word becomes almost automatic: as soon as pain follows a path down the leg, they assume the sciatic nerve is pinched. However, not all pain that resembles sciatica is actually sciatica.
True sciatica typically involves irritation or compression of a nerve root in the lumbar region, often related to a herniated disc, lumbar stenosis, or foraminal stenosis. In such cases, the pain may be accompanied by neurological symptoms such as numbness, tingling, weakness, or pain that follows a fairly precise nerve pathway.
But in practice, several musculoskeletal disorders can produce very similar pain. An irritated sacroiliac joint, a tight piriformis muscle, gluteus medius syndrome, hamstring tendinopathy, or mechanical lower back pain can all cause buttock pain or radiating pain down the leg. The patient then experiences pain “like sciatica,” even if the actual origin lies elsewhere: in the muscles, tendons, fascia, hip, pelvis, or lumbar joints.
This distinction is important because the treatment will differ. Pain related to the sciatic nerve is not treated in the same way as pain originating from the gluteus medius, piriformis, or sacroiliac joint. Confusing these causes can lead to inappropriate exercises, overly aggressive stretching, or treatment that doesn’t target the correct area.
In this article, we’ll explore 10 common causes of pain that mimic sciatica , from hamstring impingement to mechanical lower back pain with referred pain. The goal is simple: to better understand the origins of the pain, recognize the signs that point to true sciatica or sciatica, and know when to seek medical help quickly to prevent a more serious problem from developing.
Section 1 — Sciatica or false sciatica: understanding the difference
Pain radiating down the leg doesn’t always have the same origin. In everyday language, the word sciatica is often used to describe any pain that starts in the lower back, crosses the buttock, or descends into the thigh. However, clinically, it’s important to distinguish between true sciatica , caused by irritation of a lumbar nerve root, and pseudo-sciatica , which resembles sciatica but doesn’t originate directly from nerve compression in the spine.
This distinction is crucial because two types of pain can follow a similar path while having very different underlying mechanisms. Pain can originate from a lumbar disc, a sacroiliac joint, a gluteal muscle, a tendon, fascia, or a restriction of movement in the hip. The patient sometimes experiences the same symptoms: deep pain, radiating pain, a burning sensation, pulling, or tension that extends down the leg. But the source is not always the sciatic nerve itself.
What is true sciatica?
True sciatica generally corresponds to irritation or compression of a nerve root that contributes to the formation of the sciatic nerve. This irritation most often occurs in the lumbar spine, for example in the presence of a herniated disc, lumbar stenosis, foraminal stenosis, or significant disc degeneration.
In this context, the pain often follows a more defined path. It may start in the lower back or buttock, travel down the back of the thigh, reach the calf, and sometimes the foot or toes. It may be accompanied by tingling, numbness, weakness, or altered reflexes. These neurological signs point more towards a genuine nerve injury.
Why do some pains mimic sciatica?
Certain structures in the pelvis, hip, and lumbar region can produce referred pain. This means that the pain is felt at a distance from its actual source. For example, an irritated sacroiliac joint can cause pain in the buttock and thigh. A tight piriformis muscle can cause deep pain in the buttock area. Gluteus medius can create lateral hip pain that radiates down the thigh. Proximal hamstring tendinopathy can cause pain below the buttock, which is aggravated by sitting.
These pains can be misleading because they radiate to areas close to the path of the sciatic nerve. The patient then describes a pain that “runs down,” which immediately suggests sciatica. However, in many cases, it is not due to lumbar nerve compression, but to mechanical, muscular, tendinous, or joint irritation.
Nerve pain, referred pain, and muscle pain: three mechanisms to distinguish
Nerve pain is often associated with electric shock sensations, burning, numbness, or muscle weakness. It can follow a more specific area, corresponding to a nerve root or a peripheral nerve.
Referred pain , on the other hand, is more diffuse. It can radiate down the buttock, thigh, or sometimes calf, but without perfectly following a nerve pathway. It often originates from the lumbar joints, the sacroiliac joint, the fascia, or the deep structures of the pelvis.
Muscular or myofascial pain is often linked to tension, trigger points, or muscle overload. It can be reproduced by palpation, aggravated by certain postures or movements, and improved by relaxation, progressive mobility, or appropriate strengthening.
Understanding these differences helps avoid jumping to conclusions. Saying “I have sciatica” may be true, but it isn’t always. A thorough assessment helps identify whether the pain actually originates from a lumbar nerve root or from a musculoskeletal structure that mimics sciatica.
Table — True sciatica vs. false sciatica
| Criteria | True sciatica | False sciatica |
|---|---|---|
| Main origin | Irritation or compression of a lumbar nerve root | Referred musculoskeletal pain originating from muscles, tendons, joints, or fascia |
| Common cause | Herniated disc, lumbar stenosis, foraminal narrowing | Piriformis syndrome, gluteus medius, sacroiliac joint, hamstrings, mechanical lower back pain |
| Path of pain | Often well-defined, following a nerve pathway | More diffuse, sometimes less precise, often buttocks or thigh |
| Pain in the buttock | Frequent | Very common |
| Pain in the back of the thigh | Frequent | Frequent |
| Pain radiating below the knee | More evocative | Possible, but less typical |
| Pain extending to the foot or toes | More suggestive of nerve damage | Less common |
| Tingling/numbness | Frequent | Sometimes present, but often less pronounced. |
| Muscle weakness | May be present | Usually absent |
| Altered reflexes | Possible | Normal |
| Pain worsened by coughing or straining | May be present | Rare |
| Pain worsens when sitting | Possible | Very common in piriformis syndrome, proximal hamstring problems, or coccydynia |
| Neurological examination | May show abnormalities | Generally normal |
| Muscle palpation | Often less revealing | Often painful over a specific structure |
| Treatment approach | Depending on the neurological cause, monitor for neurological signs. | Mechanical, muscular, postural and functional approach |
Section 2 — When to seek immediate medical attention? Warning signs
Even though many pains that resemble sciatica originate in muscles, tendons, fascia, or joints, pain radiating down the leg should never be ignored. In most cases, the outcome is favorable with appropriate treatment, but certain signs should prompt a prompt consultation with a doctor or an emergency room.
The goal is not to cause unnecessary worry, but to be able to recognize situations where pain could indicate significant nerve damage, severe compression, or a medical cause that goes beyond simple musculoskeletal pain.
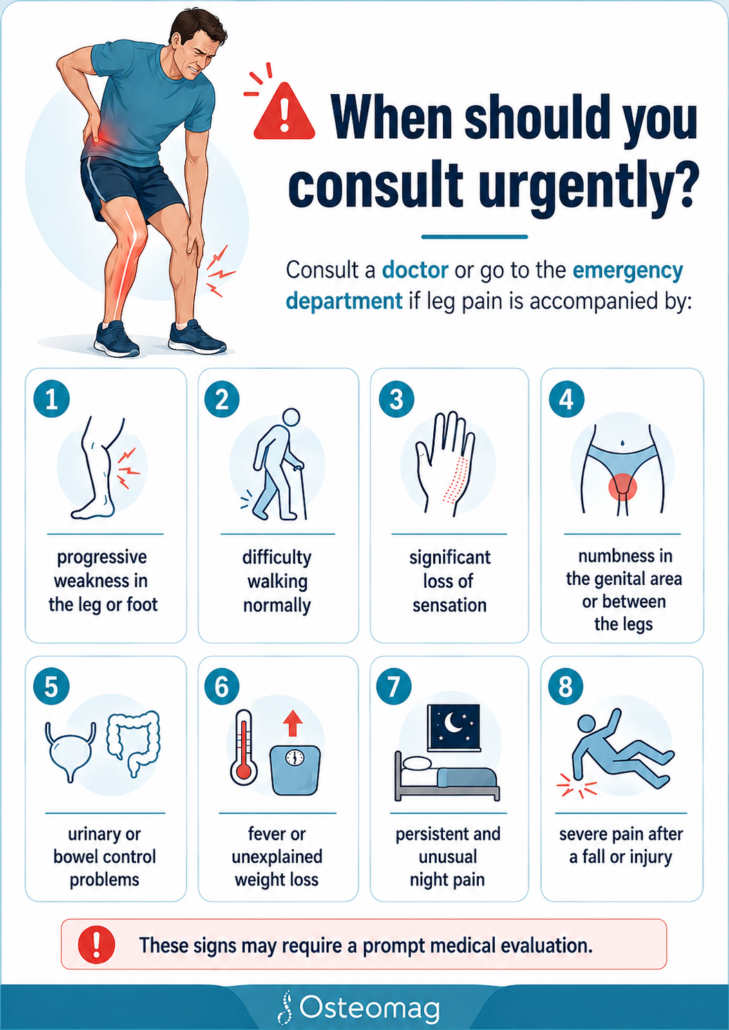
Buttock or lower back pain radiating down the leg can be related to pseudosciatica, such as piriformis syndrome, sacroiliac joint dysfunction, or gluteus medius pain. However, when accompanied by weakness, significant numbness, urinary problems, or general symptoms like fever, much more caution is warranted.
Progressive weakness in the leg or foot
Any weakness that appears or worsens in the leg should be taken seriously. For example, difficulty lifting the foot, walking on the heels, climbing stairs, or pushing off on the toes may suggest a neurological problem.
In true sciatica, certain nerve roots may be irritated or compressed. When this compression affects muscle control, pain is no longer the only problem: nerve function can be compromised.
Pain alone is often less worrisome than pain accompanied by weakness. Therefore, a recent or progressive loss of strength warrants a prompt medical evaluation.
Significant numbness or loss of sensation
Mild tingling can sometimes accompany nerve irritation or local tension. However, significant numbness, a marked loss of sensation, or an area of skin that becomes less responsive to touch should be carefully evaluated.
Particular attention should be paid to numbness that progresses, affects a large part of the leg, or is accompanied by muscle weakness. These signs may indicate that the nerve is more than just irritated: it may be compressed or damaged along its path.
In cases of pseudo-sciatica of muscular or articular origin, the neurological examination often remains normal. The presence of clear sensory disturbances suggests a true nerve lesion.
Urinary or bowel problems, or saddle anesthesia
Certain signs should be considered urgent. Lower back or sciatic pain accompanied by difficulty urinating, loss of urinary or bowel control, or numbness in the genital area or between the legs may suggest severe nerve compression.
This type of situation should not be treated as simple back pain or a case of sciatica. You should seek medical help quickly, as urgent medical attention may be necessary.
Even though these signs are rare, they are too important to ignore. In an article intended for the general public, this section should be visible early, ideally before the list of 10 causes.
Fever, unexplained weight loss, or persistent nighttime pain
Pain that resembles sciatica is not always mechanical. When it is accompanied by fever, unexplained weight loss, general malaise, or persistent nighttime pain that does not change with position, a non-mechanical medical cause should be considered.
Musculoskeletal pain often varies depending on movement, posture, walking, sitting, or rest. Constant, deep pain that awakens the patient every night and does not seem to be affected by any position should be evaluated.
These signs do not automatically mean that there is a serious illness, but they justify a medical consultation to avoid overlooking an important problem.
Table — Reassuring signs vs. warning signs
| Situation | Rather reassuring | To monitor/consult quickly |
|---|---|---|
| Pain in the buttock or thigh | Varies depending on posture, walking or sitting position | Constant, intense pain, with no possible relief |
| Radiation in the leg | Stay mainly in the buttock or thigh | It descends to the foot with marked numbness |
| Muscle strength | Normal force | Progressive weakness, foot drop, difficulty walking |
| Sensitivity | Mild and intermittent tingling | A clear or progressive loss of sensitivity |
| Seated position | Pain increased by local compression, piriformis or hamstring | Pain associated with significant neurological disorders |
| Urine/bowel | No change | Difficulty urinating, loss of control, saddle anesthesia |
| General condition | No fever, no weight loss | Fever, unexplained weight loss, general malaise |
| Nighttime pain | Improved by changing position | Waking up every night, persistent, non-mechanical |
Section 3 — The 10 Common Causes of Pain That Resembles Sciatica
Pain radiating down the leg doesn’t always originate from a compressed nerve root in the lumbar region. In many cases, the pain stems from a musculoskeletal structure: a gluteal muscle, a tendon, a sacroiliac joint, an irritated hip, or mechanical lower back pain with referred pain.
These pains can create the impression of sciatica because they radiate to areas close to the path of the sciatic nerve: the buttock, the back of the thigh, the side of the hip, sometimes even the calf. However, their mechanism is different. Therefore, they do not always require the same approach.
The following table allows you to quickly visualize the 10 common causes , from least frequent to most frequent, with their typical painful area and clues that can guide the assessment.
Table — 10 musculoskeletal causes that can mimic sciatica
| Rang | Cause possible | Common painful area | This could be indicative of sciatica. | Distinguishing feature |
|---|---|---|---|---|
| 10 | Hamstring conflict | Deep buttocks, back of hip, upper thigh | Deep pain that radiates down the back of the thigh | Often aggravated by hip extension or large steps |
| 9 | Deep rotator cuff syndrome of the hip | Deep buttocks, pelvis, back of thigh | Buttock radiation close to the path of the sciatic nerve | Pain reproduced by certain hip rotations |
| 8 | Proximal hamstring tendinopathy | Under the buttock, back of the thigh | Pain in the back of the thigh, sometimes when sitting | Localized pain near the ischium, aggravated by running or hip flexion |
| 7 | Piriformis syndrome | Buttock, back of thigh | Buttock pain with pseudo-sciatic radiation | Often aggravated by prolonged sitting |
| 6 | Deep gluteal syndrome | Deep gluteal pain, sciatic nerve | Compression or irritation of the sciatic nerve outside the spine | Pain related to the deep gluteal space rather than the lumbar disc |
| 5 | Coccygodynie | Coccyx, buttock, pelvis | Pain when sitting that may radiate to the buttocks | Pain closely linked to sitting and the coccyx |
| 4 | Greater trochanteric pain syndrome | Hip side, lateral thigh | Pain that radiates down the side of the thigh | Pain when lying on one’s side or upon palpation of the greater trochanter |
| 3 | Sacroiliac dysfunction | Lower back, buttocks, pelvis, thigh | Buttock pain sometimes radiating into the leg | Pain often near the sacroiliac joint, sometimes asymmetrical |
| 2 | Gluteus medius syndrome | Hip side, buttock, lateral thigh | Lateral pain that may radiate down the leg | Weakness or pain when bearing weight on one leg |
| 1 | Mechanical lower back pain with referred pain | Lower back, buttocks, thigh | Lower back pain that radiates down without any real neurological involvement | Pain varies depending on the movement, often without loss of strength or altered reflexes. |
10. Hamstring impingement: a deep pain in the buttock
Ischiofemoral impingement is a less common cause of sciatica-like pain, but it’s worth noting. It occurs when the space between the ischium, located at the base of the pelvis, and the lesser trochanter of the femur becomes narrowed. This area contains, among other things, the quadratus femoris muscle and is located near deep structures of the hip and pelvis.
The pain is often felt deep in the buttock, sometimes radiating to the back of the hip or the upper thigh. It can feel like sciatica because it is felt in an area close to the path of the sciatic nerve. The patient may describe a deep, hard-to-localize pain that is aggravated by certain hip movements, long strides, or prolonged walking.
This condition can be confused with piriformis syndrome, hamstring tendinopathy, or sacroiliac joint pain. The distinction is primarily made through clinical examination, hip analysis, and, in some cases, imaging when symptoms persist.
In an osteopathic approach, the goal is not to “force” the painful area, but to understand the overall constraints that can increase compression: hip mobility, pelvic position, tension in the deep rotators, gait quality, and weight-bearing strategy. Exercises should remain progressive, as some aggressive hip stretches can sometimes increase irritation.
9. Deep rotator syndrome of the hip: obturator internus and pelvic gastrocnemius
The deep rotators of the hip are small muscles located deep in the gluteal region. They contribute to hip stability and fine pelvic control. These include the obturator internus, the gastrocnemius, the obturator externus, and the quadratus femoris. When they become tight, irritated, or overused, they can cause deep pain in the buttock.
This pain can resemble sciatica because it is located near the path of the sciatic nerve and can radiate down the back of the thigh. The patient often describes a deep pain, sometimes difficult to reach, that worsens with sitting, certain hip rotation movements, or prolonged walking.
This type of pain is sometimes classified as deep gluteal syndrome. The piriformis muscle is the most well-known, but it is not the only one that can irritate the gluteal region. Therefore, it is simplistic to attribute all cases of pseudo-sciatica in the buttocks to the piriformis.
The assessment should consider the hip, pelvis, lumbar mobility, weight-bearing capacity, and the presence or absence of neurological signs. If strength, reflexes, and sensation are normal, a musculoskeletal origin becomes more likely.
8. Proximal hamstring tendinopathy: pain under the buttock and back of the thigh
Proximal hamstring tendinopathy affects the upper insertion of the hamstring muscles, near the ischium. It often causes pain under the buttock, sometimes radiating down the back of the thigh. This location can easily be mistaken for sciatica, especially when the pain extends down the leg.
The pain is often aggravated by prolonged sitting, running, climbing hills, accelerating, hamstring stretches, or movements that combine hip flexion and knee extension. The patient may experience deep pain at the junction of the buttock and thigh, sometimes described as persistent tightness or a localized burning sensation.
Unlike true sciatica, proximal tendinopathy is not usually accompanied by loss of neurological strength, altered reflexes, or numbness in a specific nerve distribution. The pain is often more mechanical: it appears with certain loads, positions, or exertion.
In this context, aggressive hamstring stretching can sometimes worsen the problem. A more appropriate approach often involves temporarily reducing stress, progressively increasing the load, improving pelvic and hip mobility, and then carefully incorporating strengthening exercises.
7. Piriformis syndrome: irritation of the sciatic nerve in the buttock
Piriformis syndrome is one of the best-known mimics of sciatica. The piriformis is a deep muscle in the buttock, located near the sciatic nerve. When it becomes tight, irritated, or overworked, it can contribute to buttock pain that radiates down the back of the thigh.
The patient often describes a deep pain in the buttock, aggravated by prolonged sitting, driving, certain hip movements, or activities that engage the external rotators. The pain may sometimes be accompanied by sensations of pulling, burning, or tingling, which can lead to confusion with true sciatica.
The important distinction is that piriformis syndrome does not originate from a compressed nerve root in the lumbar spine. The irritation is located instead in the gluteal region. It is therefore sometimes referred to as extra-spinal sciatica or pseudo-sciatic pain.
The assessment must remain cautious, as not all buttock pain is piriformis syndrome. The sacroiliac joint, deep rotators, gluteus medius, hamstrings, hip, and lumbar spine must also be considered. Effective management aims to reduce local compression, improve pelvic and hip mobility, and then gradually restore movement tolerance.
6. Deep gluteal syndrome: extra-spinal compression of the sciatic nerve
Deep gluteal syndrome refers to a group of situations where the sciatic nerve can be irritated or compressed deep within the buttock, outside the lumbar spine. Unlike classic sciatica related to a lumbar nerve root, the source of the problem here lies in the deep gluteal space, near the muscles, fascia, ligaments, and structures of the hip.
This syndrome can include the piriformis muscle, but it is not limited to it. Other structures may be involved: the obturator internus, pelvic gastrocnemius, quadratus femoris, fibrous bands, scar tissue, fascial tension, or mechanical restrictions around the nerve. This is why the term deep gluteal syndrome is often more comprehensive than simply “piriformis syndrome.”
The pain is often felt deep in the buttock. It can radiate down the back of the thigh and sometimes feels like a burning, pulling, or shooting sensation. It is frequently aggravated by prolonged sitting, driving, certain hip movements, or activities that put significant strain on the buttocks.
The clinical difficulty arises from the fact that this pain can closely resemble true sciatica. The patient may say, “It starts in the buttock and goes down the leg.” However, examination can sometimes show normal strength, normal reflexes, and relatively preserved sensation, which suggests peripheral or musculoskeletal irritation rather than lumbar nerve root compression.
The osteopathic approach must remain precise and cautious. It’s not simply a matter of massaging the buttocks or stretching the piriformis muscle. Some overly forceful stretches can even increase local compression. The work should instead aim to improve the mobility of the pelvis, hip, and lumbar spine, reduce excessive tension in the deep rotators, and restore a better distribution of stress during walking, sitting, and everyday movements.
5. Coccydynia: when the coccyx alters the sitting posture
Coccydynia refers to pain located in the coccyx, often aggravated by sitting, standing up from a seated position, or prolonged pressure on a hard surface. While it doesn’t always follow the classic path of sciatica, it can sometimes cause buttock or pelvic pain that misleads the patient.
When the coccyx becomes painful, the person often spontaneously changes their sitting posture. They may tilt their pelvis, shift their weight more onto one buttock, avoid direct contact with the coccyx, or sit further back. These protective strategies can provide temporary relief, but they can also put extra strain on the gluteal muscles, proximal hamstrings, sacroiliac joint, or lower lumbar region.
This is how pain that initially originates in the coccyx can transform into a more diffuse pain around the buttock, pelvis, or back of the thigh. The patient may then mistake it for sciatica, especially if the pain radiates slightly down the leg or is accompanied by significant tension in the buttocks.
The distinguishing feature is often the severity of the pain when sitting. The pain is usually very localized to the coccyx or the base of the sacrum. It can be reproduced by direct pressure, certain changes in position, or a previous fall onto the buttocks.
In an osteopathic approach, the assessment should not be limited to the coccyx. It is also necessary to observe pelvic mobility, breathing, pelvic floor tone, gluteal tension, sitting posture, and lumbar compensations. The goal is to reduce stress on the painful area while helping the body regain a more balanced posture.
4. Greater trochanter pain syndrome: lateral hip pain or pseudo-sciatica?
Greater trochanteric bursitis, also known as trochanteric pain syndrome , is a common cause of pain on the side of the hip. It is often related to irritation of the gluteal tendons, especially the gluteus medius and gluteus minimus, sometimes associated with tenderness of the trochanteric bursa. The pain is usually located on the lateral aspect of the hip, near the bone that can be felt on the side.
This pain can be mistaken for sciatica because it can radiate down the thigh, sometimes towards the knee. However, unlike true sciatica, it runs down the side of the thigh rather than the back of the leg. It is often aggravated by walking, climbing stairs, prolonged standing, crossing the legs, or sleeping on the affected side.
Another important indicator is tenderness upon palpation of the greater trochanter. The patient may precisely indicate the side of the hip and report that the pain is sharp when lying on it. This lateral location is very different from typical lumbar radicular pain, although the two can sometimes coexist.
Greater trochanteric pain syndrome is often associated with an imbalance in hip weight distribution. Weakness of the gluteus medius, pelvic instability, a compensatory gait, or repetitive overloading can perpetuate the irritation.
Treatment should avoid two common mistakes: aggressively stretching the glutes or directly compressing the painful area. In some cases, positions that bring the thigh inward can increase tendon compression against the greater trochanter. A more appropriate approach is to temporarily reduce irritating stresses, improve pelvic stability, work on overall mobility, and gradually strengthen the hip muscles.
3. Sacroiliac dysfunction : pelvic pain that can radiate down the leg
The sacroiliac joint connects the sacrum to the iliac bones of the pelvis. When it becomes irritated or is involved in a compensatory mechanism, it can cause pain in the lower back, buttocks, pelvis, and sometimes the thigh. This radiating pain can easily be mistaken for sciatica, especially when the pain extends down below the buttocks.
Sacroiliac pain is often felt on one side only, near the lumbar dimple or the posterior region of the pelvis. It can be aggravated by prolonged walking, climbing stairs, sitting down, standing on one leg, or certain twisting movements. The patient may sometimes be able to point directly at the sacroiliac region with a finger.
The confusion with sciatica arises from the fact that the pain can radiate down the buttock or the back of the thigh. However, it less frequently extends to the foot and is rarely accompanied by clear neurological signs such as weakness, diminished reflexes, or numbness in a specific nerve distribution.
The sacroiliac joint functions as a transfer zone between the spine, pelvis, and lower limbs. Lumbar restriction, psoas tension, gluteal weakness, weight-bearing asymmetry, or a previous injury can alter the stresses in this region.
The osteopathic approach aims to understand how the pelvis distributes weight. The work may include lumbar mobility, hip, sacrum, diaphragm, muscle chains, and the quality of grounding. The goal is not simply to “realign” the joint, but to restore better function between the trunk, pelvis, and leg.
2. Gluteus medius syndrome: a false lateral sciatica often overlooked
Gluteus medius syndrome, or gluteus medius syndrome, is a common cause of lateral hip and buttock pain. This muscle plays a major role in pelvic stability, especially during walking, climbing stairs, and standing on one leg. When it becomes weak, irritated, tight, or overused, it can cause pain similar to sciatica, but often with a more lateral distribution.
The pain may be located on the side of the hip, in the buttock, or radiate down the thigh. The patient may sometimes experience a diffuse pain that feels like it’s “going down the leg.” However, unlike true sciatica, gluteus medius pain is often aggravated by prolonged weight-bearing, walking, climbing stairs, standing on one leg, or sleeping on the affected side.
The gluteus medius can also generate trigger points that refer pain to the buttock, hip, and sometimes the lateral thigh. This referred pain can be misleading, especially when it co-occurs with lower back pain or sacroiliac joint irritation.
An important clinical indicator is pelvic stability. If the pelvis drops slightly when bearing weight on one leg, if the gait becomes asymmetrical, or if pain occurs during hip stabilization exercises, the gluteus medius may be involved.
Treatment must be progressive. Stretching the gluteal region is not enough. It is often necessary to improve hip mobility, reduce lumbar compensations, decrease lateral tension, and gradually strengthen the gluteus medius without causing pain. The goal is to restore better dynamic stability to the pelvis.
1. Mechanical low back pain with referred pain: the most frequent confusion
Mechanical lower back pain with referred pain is probably one of the most common causes of confusion with sciatica. In this case, the pain originates in the lower back, lumbar joints, discs, ligaments, muscles, or fascia, but it can also be felt in the buttock, hip, or thigh.
This pain can radiate down the leg without any actual nerve compression. It is often more diffuse than true sciatica and doesn’t always follow a precise path. It can vary depending on movements, positions, fatigue, posture, walking, or prolonged sitting.
The patient may say, “I have sciatica,” because the pain radiates down the spine. However, the neurological examination may be normal: no weakness, no diminished reflexes, no loss of clear sensation. In this case, the pain is more likely referred, meaning it is radiating from an irritated lumbar structure to a distant area.
Mechanical lower back pain can be linked to several factors: lumbar stiffness, postural overload, trunk weakness, lack of hip mobility, repetitive mechanical stress, prolonged sitting, or poorly tolerated movements. It can also coexist with other conditions that mimic sciatica, such as sacroiliac joint or gluteal muscle pain.
The osteopathic approach seeks to identify the areas that maintain the restriction: lumbar spine, pelvis, hips, diaphragm, posterior chain, weight-bearing, and breathing strategy. Treatment aims to reduce mechanical sensitivity, improve mobility, and support a gradual return to movement.
Table — Quick clues to differentiate the 10 causes
| Cause | Index here east | Pain especially aggravated by |
|---|---|---|
| Hamstring conflict | Deep pain between the ischium and hip | Big strides, hip extension |
| Deep rotators | Deep buttock pain | Hip rotation, sitting position |
| Hamstring tendinopathy | Pain under the buttock near the ischium | Sitting, running, stretching |
| Piriformis | Buttock pain with posterior radiation | Prolonged sitting, driving |
| Deep gluteal syndrome | Sciatic irritation outside the spine | Buttock and hip compression |
| Coccygodynie | Pain closely related to the coccyx | Seated, transition from sitting to standing |
| Grand trochanter | Lateral hip pain | Lying on my side, stairs |
| Sacroiliac | Pain near the posterior pelvis | Walking, asymmetrical support |
| Gluteus medius | Lateral pain, pelvic instability | Standing on one leg, stairs |
| Referred lower back pain | Neurological examination is often normal | Flexion, extension, prolonged posture |
Section 4 — Comparative table: true sciatica or pain that imitates it?
After identifying the main musculoskeletal causes that can resemble sciatica, it becomes useful to compare the signs that point towards a true nerve injury and those that suggest referred , muscular, tendinous or joint pain.
This distinction isn’t always straightforward. Buttock pain can radiate down the thigh without being true sciatica. Conversely, genuine nerve irritation can sometimes begin as subtle pain in the lower back or buttock before becoming more characteristic. Therefore, several factors must be considered together: the path of the pain, associated sensations, aggravating factors, the presence or absence of weakness, and the results of the clinical examination.
The following table helps to clarify the most frequent differences.
Table — True sciatica vs. pain that mimics sciatica
| Criteria | True sciatica | Pain that mimics sciatica |
|---|---|---|
| Probable origin | Irritation or compression of a lumbar nerve root | Muscle, tendon, fascia, sacroiliac joint, hip or mechanical lower back pain |
| Path of pain | Often more precise, following a nervous territory | More diffuse, sometimes varying according to the movements |
| Frequent area | Lower back, buttocks, back of thigh, calf, foot | Buttock, hip, thigh, pelvis, sometimes calf |
| Pain below the knee | More suggestive of nerve damage | Possible, but less typical |
| Pain all the way down to the foot | Common in root-related forms | Less common |
| Tingling | Frequent, sometimes in a specific area | Possible, but often less clear-cut. |
| Numbness | Can track a specific nerve area | More diffuse or absent |
| Muscle weakness | It’s possible, especially if the nerve root is affected. | Usually absent or related to pain |
| Altered reflexes | Possible | Generally normal |
| Pain when coughing, sneezing or straining | May increase nerve pain | Less typical |
| Pain upon local palpation | Not always present | Often found on a muscle, tendon, or joint |
| Seated position | May worsen depending on the underlying lumbar cause | Very often aggravating in piriformis, hamstrings, coccyx |
| Neurological examination | May exhibit altered strength, reflexes, or sensitivity | Often normal |
| Response to the movement | Certain lumbar movements can reproduce the pain | Often related to the hip, pelvis, weight-bearing, or palpation |
| Main approach | Neurological assessment, management of the underlying lumbar cause | Mechanical, muscular, postural and functional analysis |
Pain pathway: a useful but never sufficient clue
The path of the pain often provides an initial clue. Pain that starts in the lower back, crosses the buttock, travels down the back of the thigh, reaches the calf, and then the foot is more suggestive of true sciatica. This path is particularly indicative when accompanied by tingling, numbness, or weakness.
However, the path of pain alone is not enough to make a diagnosis. Some muscle or joint pain can radiate down the leg without following a compressed nerve. The piriformis, gluteus medius, proximal hamstrings, or sacroiliac joint can all cause radiating pain that misleads the patient.
Pain that remains primarily in the buttock, hip, or thigh, without clearly extending down to the foot, more often points to a musculoskeletal cause. However, there are exceptions. This is why a clinical examination remains essential.
Neurological signs: what changes the interpretation
Neurological signs are among the most important to monitor. Pain radiating down the leg becomes more concerning when accompanied by weakness, loss of sensation, or changes in reflexes.
For example, difficulty lifting the foot, walking on the heels, pushing off with the toes, or controlling certain leg movements may suggest nerve damage. Similarly, distinct numbness in a specific area of the leg or foot may point to an irritated nerve root.
In a case of pseudosciatica of muscular or articular origin, these signs are generally absent. The pain may be severe, bothersome, and debilitating, but strength, reflexes, and sensation often remain normal.
Aggravating factors: understanding what triggers the pain
Aggravating factors also help to differentiate the causes. Pain that increases with coughing, sneezing, or straining can sometimes indicate disc or nerve irritation. Pain that worsens with certain lower back movements may point to a problem in the spine.
Conversely, pain triggered mainly by putting weight on one leg, climbing stairs, lying on one’s side, or lateral palpation of the hip is more suggestive of gluteus medius or greater trochanter pain syndrome.
Pain under the buttock, worsened by sitting or hamstring stretching, suggests proximal hamstring tendinopathy. Deep buttock pain aggravated by prolonged sitting may indicate piriformis syndrome or deep gluteal pain syndrome.
Table — What the symptoms may suggest
| Dominant symptom | Cause plus probable |
|---|---|
| Pain that radiates down to the foot with precise numbness | True sciatica / lumbar radiculopathy |
| Deep buttock pain worsened when sitting | piriformis or deep gluteal syndrome |
| Pain under the buttock, worse when sitting or after running | Proximal hamstring tendinopathy |
| Pain on the side of the hip, worse when lying on my side | Greater trochanteric pain syndrome |
| Lateral pain with weakness or instability of the pelvis | Gluteus medius syndrome |
| Pain near the sacroiliac joint, worse when bearing weight asymmetrically | Sacroiliac dysfunction |
| Coccyx pain, worse when sitting | Coccygodynie |
| Diffuse lower back pain that radiates down the thigh without neurological signs | Mechanical lower back pain with referred pain |
Why self-diagnosis is often misleading
Many patients use the word sciatica as soon as they experience pain radiating down their leg. This is understandable, but sometimes misleading. The pain felt doesn’t always reveal its exact source. The body can project pain to distant areas, create protective tension, alter weight distribution, or amplify a sensation depending on the mechanical and neurological context.
That’s why it’s best to first describe the pain as resembling sciatica , and then determine the likely cause after evaluation. This approach avoids misdiagnosing all radiating pain as nerve compression, when many cases actually originate in the hip, pelvis, or soft tissues.
The goal is not simply to name the pain, but to understand its mechanism. True sciatica requires particular attention to neurological signs. Pseudo-sciatic pain, on the other hand, requires an analysis of mechanical stresses, mobility, stability, and the body’s compensatory mechanisms.
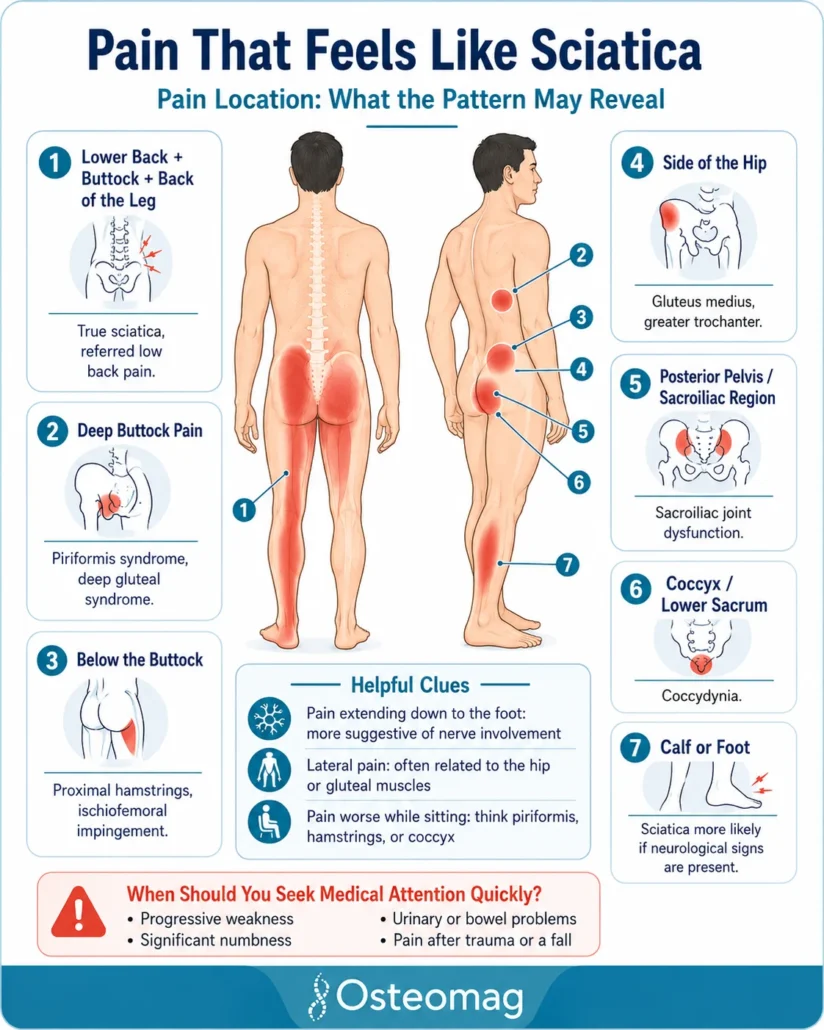
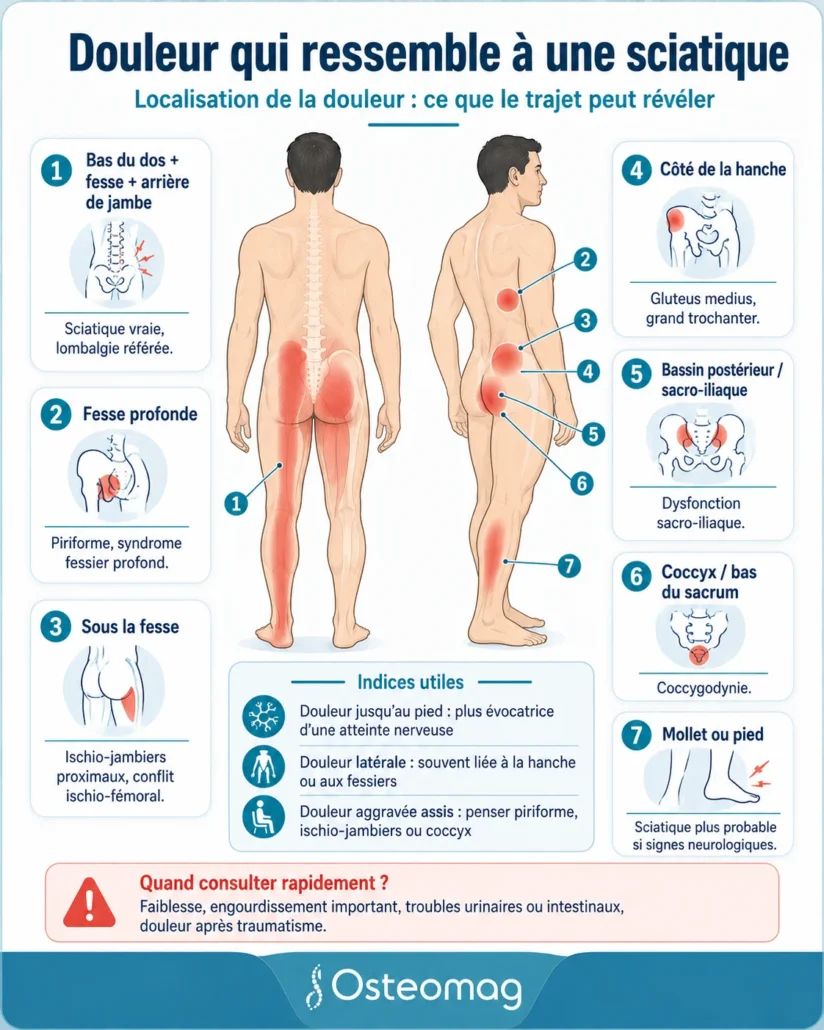
Section 5 — Localizing the pain: what the path can reveal
The location of the pain is often the first clue a patient uses to describe what they are experiencing. Pain in the buttock, the back of the thigh, or the calf is quickly associated with sciatica. However, the path of the pain is not always enough to identify the true cause. Two pains can radiate down the leg but originate from very different structures: a lumbar nerve root, a sacroiliac joint, a gluteal muscle, a tendon, the hip, or a myofascial area.
The purpose of this section is therefore to link the dominant painful area to the most likely causes. This does not replace a clinical evaluation, but it allows the reader to better understand why pain resembling sciatica may originate from sources other than the sciatic nerve itself.
Table — Location of pain and possible causes
| Main location | Possible causes | Useful clues |
|---|---|---|
| Lower back + buttocks + back of leg | True sciatica, referred lower back pain, herniated disc, lumbar stenosis | Pain that follows a more defined path, sometimes with tingling or numbness. |
| Deep buttocks | piriformis syndrome, deep gluteal syndrome, deep hip rotators | Pain aggravated by sitting, in the car, or by certain hip rotations |
| Under the buttock | Proximal hamstring tendinopathy, hamstring impingement | Pain near the ischium, aggravated by sitting, running or stretching the hamstrings |
| Hip side | Gluteus medius, gluteus minimus, painful syndrome of the greater trochanter | Pain when lying on one side, on stairs, or putting weight on one leg |
| Posterior pelvis / sacroiliac joint | Sacroiliac dysfunction, referred lumbopelvic pain | Pain near the lumbar dimple, aggravated by asymmetrical weight-bearing |
| Coccyx / base of the sacrum | Coccydynia, pelvic floor tension, sitting compensation | Pain closely linked to sitting and the transition from sitting to standing |
| Calf or foot | True sciatica is more likely, radiculopathy, nerve irritation | More suggestive if accompanied by numbness, weakness, or loss of reflexes. |
| Lateral thigh | Gluteus medius, gluteus minimus, greater trochanter, referred lower back pain | Pain often more lateral than posterior, sometimes mistaken for sciatica |
Pain in the back of the thigh
Pain in the back of the thigh often suggests sciatica, especially when it radiates from the buttock down to the calf. However, this area can also be painful in several musculoskeletal disorders.
Proximal hamstring tendinopathy can cause pain under the buttock that radiates down the back of the thigh. It is often aggravated by sitting, running, climbing hills, or stretching the hamstrings. In this case, the pain is not necessarily nerve-related: it may originate from the tendon insertion located near the ischium.
The piriformis and deep hip rotators can also cause deep buttock pain radiating to the back. This pain is often more pronounced during prolonged sitting or certain hip rotation movements.
True sciatica becomes more likely when the pain goes down below the knee, reaches the calf or foot, and is accompanied by tingling, numbness, or muscle weakness.
Pain on the side of the hip
Pain located on the side of the hip is less typical of true sciatica. It is more suggestive of a problem with the gluteus medius, gluteus minimus, or greater trochanteric pain syndrome.
The patient may experience lateral pain, sometimes burning or deep, that radiates down the thigh. This pain may be aggravated by walking, climbing stairs, prolonged standing, or sleeping on the affected side. It can also occur when the pelvis lacks stability while bearing weight on one leg.
Gluteus medius syndrome is important to recognize because it can be mistaken for sciatica, although its path is often more lateral. The gluteus medius plays a major role in stabilizing the pelvis. When it is overloaded or weakened, the hip can become painful, and the pain can radiate down the thigh.
Pain under the buttock
Pain under the buttock often points to the ischial tuberosity, where the hamstrings attach. This location is typical of proximal hamstring tendinopathy, especially if the pain worsens when sitting, running, or stretching the posterior chain.
Hamstring impingement can also cause deep pain under the buttock or at the back of the hip. This pain is sometimes aggravated by long strides, hip extension, or certain movements that reduce the space between the pelvis and the femur.
This region is very close to the path of the sciatic nerve, which explains the confusion. The patient may experience radiating pain, but the actual source may be tendon, muscle, or mechanical rather than nerve-related.
Pain that goes down to the foot
Pain that radiates down to the foot deserves special attention. It doesn’t always mean there’s an emergency, but it’s more suggestive of genuine nerve irritation, especially when it follows a specific path and is accompanied by neurological signs.
True sciatica can cause pain in the buttock, back of the thigh, calf, foot, or toes. Depending on the nerve root affected, the path of the pain can vary. Tingling, numbness, burning, electric shocks, or weakness in the foot may accompany the pain.
Conversely, musculoskeletal pain that mimics sciatica more often radiates down the buttock or thigh, and less frequently to the foot. If the foot is affected with loss of sensation or weakness, extra caution is advised, and a medical evaluation should be considered.
Pain worsens when sitting
Sitting is a very common aggravating factor in pseudo-sciatic pain. It can increase pressure on the buttock, coccyx, proximal hamstrings, piriformis muscle, or deep hip rotators.
Pain that occurs mainly when sitting may indicate:
| Pain worsens when sitting | Cause possible | Distinguishing feature |
|---|---|---|
| Deep pain in the buttock | piriformis or deep gluteal syndrome | Even worse in the car or after prolonged sitting |
| Pain under the buttock | Proximal hamstring tendinopathy | Sensation near the ischium, worse on hard surfaces |
| Coccyx pain | Coccygodynie | Pain in the center, aggravated when going from sitting to standing |
| Lower back pain that radiates down | Mechanical referred low back pain | Varies depending on sitting posture and lumbar support |
| Lateral hip pain | Gluteus medius or greater trochanter | Often worse when lying on one’s side or in prolonged contact with the bed |
Sitting can therefore reveal a great deal of information. Pain that worsens with prolonged sitting should not automatically be interpreted as true sciatica. It could originate from local compression, an irritated tendon, a deep muscle, or a protective posture of the pelvis.
Why the path of pain can be deceiving
The body doesn’t always project pain in a straightforward way. An irritated structure can send pain to a distant area. A tense muscle can create referred pain. A joint can cause radiating pain to a nearby area. A protective posture can shift the pain load to another region.
This is why two people can say “I have pain like sciatica” but have two very different causes. In one person, the pain may originate from a lumbar nerve root. In the other, it may originate from the gluteus medius, the sacroiliac joint, or the hamstrings.
Analysis of the path is therefore useful, but it must always be cross-referenced with other elements: onset of pain, aggravating factors, neurological signs, palpation, lumbar mobility, hip mobility, ground support and response to movements.
Summary table — Painful journey and clinical orientation
| Route described by the patient | Orientation possible |
|---|---|
| “It starts at the lower back and goes down to the foot.” | True sciatica or radiculopathy to consider |
| “It’s mostly in my deep buttocks when I’m sitting down.” | piriformis or deep gluteal syndrome |
| “I have pain under my buttock, especially when sitting or after running.” | Proximal hamstring tendinopathy |
| “I have pain on the side of my hip and when going up and down stairs.” | Gluteus medius or greater trochanter syndrome |
| “I have pain near my pelvis, especially when I’m standing on one leg.” | Sacroiliac dysfunction or lumbopelvic instability |
| “My tailbone hurts when I sit down.” | Coccygodynie |
| “The pain is subsiding, but my strength and sensations are normal.” | Possible referred musculoskeletal pain |
| “I have weakness in my foot or a loss of sensation.” | Medical evaluation recommended promptly |
Section 6 — How the osteopath assesses pseudo-sciatic pain
When a patient consults for pain radiating down their leg, the goal is not to jump to a conclusion about sciatica. The role of the assessment is first to understand the origin of the pain , how it manifests, what aggravates it, what relieves it, and whether there are any signs that require a medical referral.
Pseudo-sciatic pain can originate from several areas: the lumbar spine, the sacroiliac joint, the hip, the gluteal muscles, the piriformis muscle, the hamstrings, the coccyx, or the pelvic fascia. The osteopath must therefore consider the body as a functional whole, without focusing solely on the painful area.
The assessment is based on several elements: the history of the pain, observation of posture, gait, lumbar mobility, pelvic mobility, hip tests, tissue palpation, and certain basic neurological tests. This approach helps to distinguish between pain that is primarily nerve-related and pain that is mechanical, muscular, or articular.
Table — What the osteopath seeks to understand
| Item evaluated | What this may reveal |
|---|---|
| Onset of pain | Sudden or gradual onset, after exertion, a fall, or prolonged positioning |
| Path of pain | Possible nerve pain or referred musculoskeletal pain |
| This position aggravates | Sitting, walking, stairs, lumbar flexion, extension, standing on one leg |
| A position that provides relief | Rest, gentle movement, change of posture, bending or extension |
| Presence of numbness | Possible nerve irritation if the area is specific |
| Presence of weakness | A more worrying sign if it is progressive or marked |
| Lumbar mobility | Restriction, referred pain, possible disc or facet joint irritation |
| Hip mobility | Involvement of the gluteus medius, piriformis, deep rotators or trochanter |
| Buttock palpation | Muscle pain, trigger points, tension in the piriformis or gluteus medius |
| Neurological tests | Strength, reflexes, and sensitivity to detect nerve damage |
Observation of posture and gait
Posture often provides important clues. A person suffering from sciatica-like pain may avoid putting weight on one leg, lean their torso to one side, shorten their stride, or walk with a slight pelvic rotation. These adaptations are not simply “bad posture”; they are often protective strategies.
When pain originates from the gluteus medius, for example, the pelvis may lack stability during walking. The patient may exhibit a slight pelvic tilt to the opposite side or trunk compensation toward the painful side. When the pain originates from the proximal hamstrings, walking may be shorter, as longer strides put more strain on the tendon insertion under the buttock.
In sacroiliac pain, weight-bearing may become asymmetrical. The patient may avoid certain weight transfers, experience discomfort when climbing stairs or moving from a sitting to a standing position. In coccydynia, observing sitting posture becomes particularly important: the patient may sit on one buttock, tilt their pelvis, or avoid central weight-bearing.
Lumbar, sacroiliac and hip mobility tests
Mobility assessment helps identify which areas contribute to the pain. The lumbar spine can be tested in flexion, extension, lateral flexion, and rotation. Certain movements can reproduce pain in the buttock or leg, without necessarily indicating true sciatica.
The sacroiliac region is assessed through pelvic movements, weight-bearing tests, weight transfers, and the pain response to mechanical stress. Sacroiliac pain is often located near the posterior pelvis, but it can also radiate down into the buttock or thigh.
The hip is also crucial. Limited rotation, lateral pain, discomfort when bearing weight on one leg, or pain reproduced during certain movements may point to the gluteus medius, gluteus minimus, deep rotators, or greater trochanteric syndrome. It’s a common mistake to focus solely on the lower back when the hip may be the primary source of pain.
Assessment of the gluteal and deep rotator muscles
The gluteal muscles play a central role in pain that mimics sciatica. The piriformis, gluteus medius, gluteus minimus, obturator internus, and other deep rotators can all produce local or referred pain.
Palpation can help identify tender areas, tension, trigger points, or pain that reproduces the patient’s symptoms. For example, deep pain in the buttock that worsens when sitting may suggest piriformis syndrome or deep gluteal syndrome. Pain that is more lateral, near the hip, points more towards gluteus medius or greater trochanteric pain syndrome.
However, palpation alone is not enough. A painful area may be a consequence rather than the primary cause. The osteopath must therefore relate palpation to mobility, posture, the patient’s history, and triggering factors.
Basic neurological tests: strength, reflexes and sensation
Even when the pain appears to be musculoskeletal, a basic neurological assessment is important. It helps determine whether the radiating pain is accompanied by signs more suggestive of true nerve damage.
The elements to observe include:
| Neurological test | What it allows us to verify |
|---|---|
| Muscle strength | Ability to lift the foot, push off on the toes, stabilize the leg |
| Sensitivity | Presence of a loss of sensation in a specific area |
| Reflexes | Nerve response that may be altered in case of nerve root damage |
| Walking on heels/toes | Function of muscles controlled by certain nerve roots |
| Progressive signs | Worsening of weakness or numbness requiring a referral |
If strength decreases, if reflexes change, if numbness progresses, or if the patient presents with urinary or bowel problems, the assessment should go beyond the purely osteopathic framework and lead to a prompt medical consultation.
When to refer for a medical evaluation or imaging
Imaging is not always necessary for pain that resembles sciatica. Many musculoskeletal pains can be evaluated clinically and respond well to appropriate management. However, certain signs warrant a medical referral.
Prompt medical attention is necessary in the presence of progressive weakness, significant loss of sensation, pain following trauma, fever, unexplained weight loss, unusual nighttime pain, or urinary and bowel problems. Pain radiating to the foot with marked neurological signs also requires particular attention.
The aim of this guideline is not to dramatize the situation, but to protect the patient. A good osteopathic assessment must recognize its limitations and be able to identify situations where medical advice, imaging, or further examination becomes necessary.
Table — Clinical orientation based on assessment results
| Observed result | Orientation possible |
|---|---|
| Deep buttock pain, worse when sitting, normal neurological examination | piriformis or deep gluteal syndrome |
| Lateral hip pain, worse when lying on your side | Gluteus medius or greater trochanter syndrome |
| Pain under the buttock, worse when sitting or after running | Proximal hamstring tendinopathy |
| Pain near the posterior pelvis, worse when bearing weight asymmetrically | Sacroiliac dysfunction |
| Coccyx pain, worse when sitting | Coccygodynie |
| Lower back pain radiating down, but normal strength and sensation. | Mechanical lower back pain with referred pain |
| Pain radiating down to the foot with precise numbness | True sciatica to consider |
| Progressive weakness or urinary/intestinal problems | Rapid medical referral |
The osteopathic assessment of pseudo-sciatic pain must therefore be both comprehensive and cautious. Comprehensive, because the pain can originate in the hip, pelvis, muscles, or lower back. Cautious, because true nerve damage should never be overlooked. This dual approach allows for better treatment guidance and avoids mistaking all descending pain for classic sciatica.
Section 7 — Osteopathic approach: relieving pain without confusing the causes
The osteopathic approach to pain resembling sciatica must first avoid a common mistake: treating all descending pain as if it originated from the sciatic nerve. Pain in the buttock, thigh, or leg can indeed be related to nerve irritation, but it can also originate from a gluteal muscle, a tendon, the sacroiliac joint, the hip, or from mechanical lower back pain with referred pain.
The goal of osteopathic treatment is therefore to understand the dominant mechanism . Is it nerve pain? Myofascial pain? Tendon pain? Pelvic compensation? Gluteus medius overload? Sacroiliac region irritation? This distinction allows for the adaptation of techniques, advice, and exercises.
The osteopath does not simply aim to reduce local pain. They observe how the body distributes stress between the lumbar spine, pelvis, hip, and leg. Pseudo-sciatic pain can be maintained by reduced lumbar mobility, a stiff hip, asymmetrical weight-bearing, gluteal muscle overload, restricted breathing, or a protective strategy that becomes too persistent.
Table — Adapt the approach according to the suspected cause
| Suspected cause | Main osteopathic objective | Important precaution |
|---|---|---|
| Piriformis / deep gluteal syndrome | Reduce local compression and improve hip mobility | Avoid aggressive stretching that increases irritation. |
| Gluteus medius / grand trochanter | Reduce lateral overload and stabilize the pelvis | Avoid prolonged direct compression on the side of the hip |
| Sacroiliac | Improve the distribution of stress between the lumbar region, pelvis, and hip | Do not reduce the pain to a simple “displaced joint” |
| proximal hamstrings | Reduce traction under the buttock and manage tendon load | Avoid intense hamstring stretching during the painful phase |
| Coccygodynie | Improving sitting posture, pelvic alignment, and associated tension | Avoid prolonged direct pressure on the coccyx |
| Mechanical referred low back pain | Restore lumbopelvic mobility and reduce mechanical sensitivity | Monitor for the appearance of neurological signs |
| suspected true sciatica | Carefully guide mobility and monitor developments | Refer if weakness, progressive numbness or warning signs occur. |
Reduce lower back and pelvic tension
Pseudo-sciatic pain is often part of a broader pattern of lower back and pelvic issues. When the lumbar spine becomes stiff, painful, or protective, the gluteal muscles and hip may compensate. Conversely, limited hip mobility or pelvic instability can increase stress on the lumbar spine.
Osteopathic treatment can aim to improve lumbar mobility, pelvic flexibility, the quality of sacroiliac joint movement, and coordination between the trunk and lower limbs. The goal is not to “force” a painful area, but to restore the body’s range of motion.
In mechanical lower back pain with referred pain, this approach is particularly important. The pain may radiate down the buttock or thigh, but the primary source is often in the lumbar or lumbopelvic region. Gentle work on mobility, breathing, muscle tone, and the posterior chain can help reduce the perceived strain.
Improve hip and pelvic mobility
The hip plays a central role in pain that resembles sciatica. A stiff hip can transfer too much stress to the lower back, sacroiliac joint, or deep gluteal muscles. Conversely, an overly unstable hip can overload the gluteus medius and pelvic stabilizers.
The osteopath can assess hip flexion, extension, rotation, and abduction. Restricted rotation may suggest involvement of the deep rotators. Lateral pain may indicate overload of the gluteus medius or greater trochanter. Pain below the buttock may suggest excessive tension on the proximal hamstrings.
Treatment may include joint mobility techniques, myofascial release, functional exercises, and advice on reducing irritating postures. Improving hip function often reduces stress on the pelvis and lumbar region.
Reduce stress on the gluteal muscles
The gluteal muscles can become painful when they compensate for instability, weakness, asymmetrical weight-bearing, or repetitive strain. The piriformis, gluteus medius, gluteus minimus, and deep rotators can all produce pain that radiates down the thigh.
In gluteus medius syndrome, the goal is not simply to release the muscle. It is necessary to understand why it is overloaded: pelvic weakness, asymmetrical gait, stiff hip, prolonged weight-bearing, stairs, sleeping on the painful side, or poor load tolerance.
In piriformis syndrome or deep gluteal syndrome, further compression of the area should be avoided. Some patients worsen their symptoms by using a hard ball directly in the buttock or by performing overly intense stretches. A gentler, gradual, and functional approach is often preferable.
Working on breathing, muscle tone, and postural compensations
Breathing directly influences the pelvis, lumbar spine, and overall muscle tone. When pain persists, the body often adopts a protective strategy: shallower breathing, a rigid pelvis, contracted glutes, a shorter stride, and decreased lumbar mobility.
An osteopath can work on the diaphragm, rib cage, psoas muscle, pelvis, and fascial chains to help the body move out of an overprotective mode. This is important because sciatic pain is not just localized; it can alter how you walk, sit, breathe, and stand.
The goal is to restore better adaptive capacity. A body that moves better distributes stress more effectively. A more mobile pelvis, freer hip movement, and deeper breathing can reduce pressure on painful areas.
Supporting the resumption of movement without causing pain
Movement is essential, but it must be well-controlled. Pseudo-sciatic pain can be aggravated by poorly chosen exercises: excessive stretching of the piriformis muscle, direct compression of the greater trochanter, too rapid strengthening of the gluteus medius, intense hamstring stretches, or long walks before tolerance has returned.
An osteopathic approach can help identify movements that are helpful, neutral, and those that worsen pain. The patient can then gradually resume walking, mobility exercises, hip strengthening, and pelvic stabilization.
Manual treatment alone is not always sufficient. It often needs to be accompanied by simple advice: change position regularly, avoid prolonged pressure on the painful area, adjust sitting position, resume walking in small doses, and gradually strengthen without aiming for performance.
Table — Techniques and advice according to the dominant mechanism
| Dominant mechanism | Useful techniques | Related advice |
|---|---|---|
| Buttock muscle pain | Gentle relaxation, hip mobility, myofascial work | Avoid strong pressure and aggressive stretching. |
| Tendon pain under the buttock | Comprehensive pelvic-hip work, reduction of posterior chain tension | Temporarily reduce running, hard sitting, and intense stretching |
| Lateral hip pain | Hip-pelvic mobility, lateral release, progressive stabilization | Avoid sleeping on the painful side and crossing your legs |
| Sacroiliac pain | Lumbopelvic mobility, weight-bearing exercises, balance of muscle chains | Break up the walking and avoid prolonged asymmetrical weight-bearing. |
| Referred lower back pain | Lumbar mobility, breathing, release of protective muscle tone | Resume lumbar movements gradually |
| Possible nerve irritation | Gentle techniques, relief positions, neurological monitoring | Consult a doctor if you experience weakness, numbness, or warning signs. |
A complementary approach, not a replacement for medical diagnosis
Osteopathy can help understand and relieve several musculoskeletal pains that mimic sciatica. It can improve mobility, reduce tension, support the return to movement, and help the patient avoid behaviors that perpetuate the pain.
However, it does not replace a medical evaluation when symptoms suggest significant nerve damage or a more serious cause. Progressive weakness, significant loss of sensation, urinary or bowel problems, pain after trauma, fever, or unusual nighttime pain should be evaluated promptly.
The strength of a cautious approach lies in not pitting osteopathy against medicine. For pain resembling sciatica, the right approach involves identifying the dominant mechanism, relieving what can be manually relieved, guiding movement, and referring when the symptoms go beyond simple musculoskeletal pain.
Section 8 — Exercises and advice: what to do and what to avoid
Exercises can help relieve pain that resembles sciatica, but they must be chosen carefully. A common mistake is to forcefully stretch the buttocks, hamstrings, or lower back as soon as the pain radiates down the leg. However, depending on the actual cause, some stretches can increase compression, irritate a tendon, or further aggravate an already painful area.
The goal, therefore, is not to do a lot of exercises, but to choose the right movements at the right time. Pain related to the piriformis muscle is not managed in the same way as pain in the gluteus medius, hamstring tendinopathy, coccydynia, or true nerve irritation. Movement must remain gradual, comfortable, and adapted to the body’s reaction.
Table — Exercises: what to do and what to avoid depending on the probable cause
| Cause probable | To be preferred | Avoid at first |
|---|---|---|
| Piriformis / deep gluteal syndrome | Gentle hip mobility, short walks, gradual relaxation | Aggressive deep stretches, hard ball in the buttock |
| Gluteus medius / grand trochanter | Gentle hip strengthening, pelvic stability, measured walking | Sleeping on the painful side, crossing the legs, compression stretches |
| proximal hamstrings | Progressive strengthening, reduced load, adapted seating | Intense hamstring stretches, fast running, prolonged hard sitting |
| Sacroiliac | Gentle lumbopelvic mobility, breathing, symmetrical support | Prolonged weight-bearing on one leg, sudden twisting movements |
| Coccygodynie | Seat adjustment, gentle pelvic mobility, adapted cushion | Prolonged sitting on a hard surface, direct pressure on the coccyx |
| Referred lower back pain | Progressive walking, gentle lumbar mobility, short, repeated movements | Prolonged complete rest, forced movements with pain |
| suspected true sciatica | Relief positions, light walking if tolerated, monitoring | Exercises that increase numbness, weakness, or pain all the way down to the foot |
Gentle exercises to regain mobility
Gentle mobility exercises are often the most helpful initially. They allow movement to be restored without triggering a defensive reaction. When the pain is recent or irritable, it is best to avoid intense exercises and choose simple, slow, and controlled movements.
Gentle pelvic movements while lying down can help reduce lower back stiffness. A slight forward and backward tilt of the pelvis, without aiming for maximum range of motion, can restore fluidity to the lower back. Small hip movements, such as gently opening and closing the knee while lying down, can also help release tension in the gluteal region.
Short, intermittent walks are often preferable to long walks that aggravate the pain. The idea is to walk enough to stimulate movement, but not to the point of triggering a significant increase in symptoms. A good indicator is the reaction after the activity: if the pain increases sharply or remains aggravated for several hours, the dose was probably too high.
Stretching should be used with caution
Stretching is often automatically suggested for sciatica-type pain, but it’s not always appropriate. In piriformis syndrome or deep gluteal syndrome, excessive stretching can increase tension around the sciatic nerve or further compress the deep tissues of the buttock.
In proximal hamstring tendinopathy, forceful stretching can irritate the tendon insertion under the buttock. The patient sometimes believes they are “unlocking” the area, but they are actually increasing the tension on an already sensitive tendon.
In greater trochanteric pain syndrome or gluteus medius syndrome, certain stretching positions that bring the thigh inward can compress the gluteal tendons against the greater trochanter. This can perpetuate lateral hip pain.
An acceptable stretch should be gentle, brief, and not forceful. It should not increase radiating pain, tingling, numbness, or a burning sensation. If a stretch causes sharp pain or increased pain radiating down the leg, it is best to stop and choose a gentler movement.
Progressive strengthening of the glutes and hips
Strengthening is often necessary, especially when the pain originates in the gluteus medius, pelvis, or hip instability. However, strengthening should be gradual. Starting too intensely can irritate the painful area and make the exercise seem ineffective.
For the gluteus medius, you can start with gentle contractions while lying down or standing, without pain. Then, you can progress to pelvic stability exercises, such as standing on one leg with support, small lateral movements, or hip abduction exercises. The goal is not to quickly fatigue the muscle, but to restore stable and tolerable function.
For the proximal hamstrings, strengthening exercises must respect the tendon’s sensitivity. Light isometric exercises, where the muscle works without significant movement, may sometimes be better tolerated initially. The load can then be gradually increased depending on the response.
For referred mechanical lower back pain, strengthening the trunk, hip, and glutes may help, but only after restoring minimal mobility and tolerance to movement.
Sitting positions: avoid aggravating the pain
Sitting is often a significant factor in pseudo-sciatica. It can compress the buttock, irritate the piriformis muscle, increase proximal hamstring pain, or worsen coccydynia.
It is often helpful to break up sitting. Instead of remaining seated for long periods, the patient can get up regularly, walk around for a few minutes, change the angle of their pelvis, or use a suitable support. For pain under the buttock, a surface that is too hard can be irritating. For coccydynia, a suitable cushion can reduce direct pressure on the coccyx.
It’s also important to avoid always sitting on the same side to escape the pain. This strategy may provide temporary relief, but it can create asymmetrical overload of the pelvis, gluteus medius, or sacroiliac region.
Walking, stairs and sleep: simple daily adjustments
Walking is generally beneficial when done in moderation. A short, regular, and pain-free walk is often more helpful than complete rest. However, if pain increases with prolonged walking, it’s best to break it up: several short walks throughout the day rather than one long outing.
Stairs can irritate the gluteus medius, greater trochanter, or sacroiliac joint. During a painful phase, it can be helpful to slow down, use the handrail, and avoid putting strain on the affected leg. The goal is to temporarily reduce the load without completely eliminating movement.
Sleep can also influence pain. For lateral hip pain, sleeping directly on the affected side can perpetuate the compression. Sleeping on the opposite side with a pillow between the knees can sometimes better distribute the pressure. For lower back or buttock pain, a comfortable position that reduces tension in the leg is preferable to an “ideal” but painful posture.
Table — 10 practical dos and don’ts
| To do | Avoid |
|---|---|
| Walk for short periods if the pain allows. | Remaining still all day |
| Change position often | Sitting for several hours without a break |
| Use a suitable seat if the buttock or coccyx is painful. | Sitting on a hard surface if it increases the pain |
| Gradually strengthen your glutes | Starting with exercises that are too intense |
| Gently mobilize the hip and pelvis | Forcing painful ranges of motion |
| Observe what triggers the pain | Repeat the movements that increase radiation |
| Sleeping with a pillow between your knees is so helpful | Sleeping directly on a painful hip |
| Take the stairs again gradually | Climbing stairs quickly in pain |
| Respect the reaction after exercise | Continue if the pain moves further down the leg |
| Consult a doctor if neurological signs progress. | Ignoring significant weakness or numbness |
When to stop an exercise?
An exercise should be stopped if the pain spreads further down the leg, if tingling increases, if numbness becomes more pronounced, or if weakness develops. Mild local tension may be acceptable, but stronger nerve radiating pain is a warning sign.
You should also stop and seek medical help quickly if the pain is accompanied by urinary or bowel problems, significant loss of sensation, progressive weakness, or intense pain after trauma.
The right exercise is the one that helps the body regain mobility and confidence without triggering a defensive reaction. In cases of pain that mimics sciatica, gentle progression is often more effective than intensity.
Section 9 — Prevention: preventing false sciatica from becoming chronic
Pain resembling sciatica can sometimes disappear quickly when the cause is correctly identified. But when it is ignored, misunderstood, or perpetuated by the same daily stresses, it can become persistent. The body then develops protective strategies: it avoids certain movements, overloads other areas, alters weight distribution, shortens walking distances, or increases tension in the gluteal and lumbar muscles.
Prevention therefore does not consist solely of “doing exercises”. It consists primarily of reducing the factors that maintain the pain: prolonged sitting, lack of hip mobility, pelvic weakness, tendon overload, asymmetrical support, sleeping on the painful area or poorly adapted stretches.
The goal is to allow the body to regain better tolerance to movement. False sciatica often becomes chronic when the musculoskeletal system remains trapped between protection, compensation, and repeated irritation.
Table — Preventing the chronicity of pseudo-sciatic pain
| Factor to watch | Why this is important | Preventive action |
|---|---|---|
| Prolonged sitting | It can compress the buttock, piriformis muscle, hamstrings, or coccyx. | Get up regularly, vary your positions |
| Weakness of the gluteus medius | May increase pelvic instability and lateral hip pain | Progressive hip strengthening |
| Hip stiffness | Can transfer stress to the lower back or sacroiliac joint | Gentle and regular mobility |
| Aggressive stretching | They can irritate tendons or compress deep tissues. | Favor gentle movements |
| Asymmetrical support | Can put undue stress on the sacroiliac joint, hip, or buttocks | Rebalancing posture and gait |
| Painful side sleeping | It can compress the greater trochanter or the gluteal tendons. | Use a cushion or change sides |
| Prolonged complete rest | Decreases tolerance to movement | Resume activity gradually |
| Pain ignored for too long | May promote compensation | Consult a doctor if the pain persists or worsens. |
Limit prolonged sitting
Sitting is one of the most common causes of pain that mimics sciatica. It can increase pressure on the buttocks, coccyx, proximal hamstrings, and deep hip rotators. In some people, the pain is most noticeable after a long car ride, a day at the office, or prolonged sitting on a hard surface.
Limiting sitting time doesn’t mean avoiding sitting altogether. It’s more about breaking it up. Getting up every 30 to 45 minutes, walking a few steps, slightly changing the angle of your pelvis, or alternating positions can reduce mechanical irritation.
For pain under the buttock, a softer cushion or a less firm seat can help. For coccydynia, a suitable cushion can reduce direct pressure on the coccyx. For piriformis syndrome or deep gluteal pain, excessive localized pressure on the buttock should be avoided.
Strengthen the stability of the pelvis
The pelvis acts as a platform between the lumbar spine and the legs. When it lacks stability, certain structures can compensate: the gluteus medius, piriformis, sacroiliac, lumbar, or hamstring muscles. This compensation can create pain that radiates down the leg and resembles sciatica.
The gluteus medius is particularly important. It stabilizes the pelvis during walking and when standing on one leg. When it is weak or overused, pain can occur on the side of the hip, in the buttock, or in the lateral thigh.
Prevention involves gradual strengthening. It’s important to avoid starting with overly difficult exercises. The work can begin with small contractions, exercises performed lying down, then progress to standing, controlled walking, stair climbing, and functional exercises.
Vary your movements throughout the day
The body tolerates varied movement better than fixed positions. Pseudo-sciatic pain can develop when the same stress is constantly repeated: always sitting on the same side, always crossing the legs, remaining in a bent position for long periods, walking with a shortened stride, or always sleeping on the painful hip.
Varying your movements helps to distribute the strain. Even small changes can help: getting up more often, alternating leg positions, adjusting the chair height, walking for a few minutes, changing sides while sleeping, avoiding long periods in a single posture.
This variety is particularly useful for pain related to the gluteus medius, sacroiliac joint, or piriformis muscle. It prevents the body from repeatedly using the same protective strategy.
Avoid aggressive self-stretching
Many people try to relieve sciatic pain by strongly stretching their buttocks, hamstrings, or lower back. Sometimes this helps temporarily. But in many cases, it can perpetuate the irritation.
Aggressive stretching of the piriformis muscle can further compress the deep gluteal region. Intense hamstring stretching can irritate proximal tendinopathy under the buttock. Lateral hip stretching can increase compression of the gluteal tendons against the greater trochanter.
Prevention involves respecting the body’s reaction. Movement should not increase radiating pain, tingling, numbness, or a burning sensation. If stretching causes sharp pain or increased radiating pain, it’s best to choose a gentler approach or seek an evaluation.
Resume activity gradually
Rest can be helpful during a very painful phase, but prolonged complete rest often perpetuates stiffness, weakness, and apprehension about movement. To prevent the pain from becoming chronic, activity must be reintroduced gradually.
Walking is often a good starting point. It’s better to walk short distances regularly than to take a long walk that triggers pain. Mobility exercises can then be added, followed by strengthening exercises for the hip, pelvis, and core.
The important rule is progression. If an activity significantly increases pain or causes more pronounced radiation in the leg, the dose is probably too high. The body should be stimulated, but not forced.
Table — Simple plan for gradual recovery
| Stage | Objective | Example |
|---|---|---|
| Step 1 | Calmer l’irritation | Short walks, sitting breaks, relief positions |
| Step 2 | Regain mobility | Gentle mobility of the pelvis, hip and lower back |
| Step 3 | Reactivate the muscles | Gentle glute contractions and gentle stabilization |
| Step 4 | Increase tolerance | Longer walks, gradual stair climbing, functional exercises |
| Step 5 | Preventing relapses | Regular strengthening exercises, variety of movements, and proper posture. |
Recognizing the signs of relapse
Pseudo-sciatic pain can recur if the same stresses are repeated. Early signs are often subtle: buttock stiffness upon waking, pain after prolonged sitting, discomfort on stairs, tension under the buttock, lateral hip pain when sleeping on the side, or a pulling sensation behind the thigh.
Recognizing these signs early allows for quick adjustments: temporarily reduce the load, vary positions, resume gentle exercises, avoid irritating stretches, and consult a doctor if the pain progresses.
Prevention is therefore less about a list of fixed rules than about being attentive to the body. The body often gives signals before the pain becomes intense. Recognizing these signals helps prevent sciatica from becoming a chronic condition.
Section 10 — FAQ: Sciatica, piriformis, gluteus medius and buttock pain
Pain that resembles sciatica raises many questions because the patient’s experience can be very misleading. Pain that radiates down the leg naturally gives the impression of a pinched nerve. However, several musculoskeletal structures can cause similar radiating pain: gluteal muscles, tendons, the sacroiliac joint, the hip, the coccyx, or the lumbar spine.
This FAQ summarizes the most frequently asked questions and helps to better distinguish true sciatica from pseudo-sciatic pain.
Table — Frequently Asked Questions and Quick Answers
| Question | Short answer |
|---|---|
| Is leg pain always sciatica? | No. Several muscle, joint, or tendon pains can mimic sciatica. |
| Can the piriformis muscle cause pain similar to sciatica? | Yes. It can irritate the sciatic nerve area in the buttock. |
| Can the gluteus medius cause leg pain? | Yes. It can refer pain to the hip, buttock, or lateral thigh. |
| Can sacroiliac pain radiate down the leg? | Yes, especially in the buttock and thigh, but rarely down to the foot. |
| Is pain that radiates down to the foot more worrying? | It deserves more attention, especially with numbness, weakness, or loss of sensation. |
| Are stretches always good? | No. Some stretches can aggravate the piriformis, hamstrings, or lateral hip. |
| When should you seek medical help quickly? | In case of weakness, significant numbness, urinary/intestinal problems, fever, trauma or unusual nighttime pain. |
How can you tell if it’s real sciatica or false sciatica?
It is not always possible to know for sure based solely on sensation. True sciatica is more likely when the pain radiates down below the knee, reaching the calf or foot, and is accompanied by neurological signs such as sharp tingling, distinct numbness, loss of strength, or altered reflexes.
False sciatica, or pseudo-sciatic pain, is more likely when the pain remains mainly in the buttock, hip or thigh, varies greatly with positions, is reproduced by palpation or appears with certain hip movements, sitting or leaning.
The difference therefore rests on several indicators: path of the pain, neurological signs, posture, lumbar mobility, hip mobility, palpation, reaction to sitting and response to movements.
Is piriformis syndrome a true form of sciatica?
Piriformis syndrome can produce pain very similar to sciatica, but it is not always a true case of lumbar sciatica. In classic sciatica, the irritation often originates from a nerve root in the lumbar spine. In piriformis syndrome, the irritation is located more often in the buttocks, near the passage of the sciatic nerve.
This is why it is sometimes referred to as extra-spinal sciatica or pseudo-sciatic pain. The patient may experience deep pain in the buttock, aggravated by sitting, sometimes radiating down the back of the thigh.
The important point is not to attribute all buttock pain to the piriformis muscle. Other structures can produce a similar presentation: deep rotators, sacroiliac joint, gluteus medius, proximal hamstrings, or referred lower back pain.
Can the gluteus medius cause leg pain?
Yes. The gluteus medius, or middle buttock, can cause pain on the side of the hip, in the buttock, and sometimes in the lateral thigh. This pain can be mistaken for sciatica, especially if the patient experiences radiating pain down the leg.
However, the pain pattern is often different from true sciatica. Gluteus medius pain more often causes lateral pain, aggravated by walking, stairs, prolonged standing, putting weight on one leg, or sleeping on the affected side.
This pain is often linked to overloading or weakness in the pelvis. Treatment therefore involves not only relaxing the muscle, but also improving hip stability, gait, and weight distribution.
Can sacroiliac pain radiate down to the calf?
Sacroiliac pain can radiate down the buttock and thigh. It can sometimes feel like leg pain, but it less often extends down the calf or foot than true sciatica.
If the pain clearly affects the calf or foot, especially with tingling, numbness, or weakness, nerve damage should be considered and an appropriate evaluation sought.
Sacroiliac dysfunction often manifests as pain near the posterior pelvis, sometimes around the lumbar dimple, with aggravation during asymmetrical weight-bearing, walking, stairs, or sitting-to-standing movements.
Why does the pain increase when sitting?
Sitting increases pressure on several structures: the deep gluteal muscles, piriformis, coccyx, proximal hamstrings, and pelvis. Therefore, pain that worsens when sitting does not automatically mean it is true sciatica.
Deep pain in the buttock when sitting may suggest piriformis syndrome or deep gluteal syndrome. Pain under the buttock may suggest proximal hamstring tendinopathy. Central pain at the base of the sacrum may point to coccydynia.
Prolonged sitting can also maintain mechanical lower back pain, especially if the pelvis remains in flexion for a long time or if the person always sits asymmetrically to avoid pain.
Are piriformis muscle stretches recommended?
They can be helpful for some people, but they must be gentle. Overstretching the piriformis muscle can increase compression deep in the buttock or further irritate a sensitive area.
Particular caution is needed if stretching increases radiating pain, tingling, or a burning sensation. In this case, it’s best to focus on gentle hip mobilization, breathing exercises, light walking, and gradual progression.
Proper stretching should not cause increased nerve pain. It should provide a sensation of controlled release, without increased pain radiating into the leg.
When should you consult a doctor for sciatica-type pain?
You should seek medical help quickly if the pain is accompanied by progressive weakness in the leg or foot, significant loss of sensation, difficulty walking, numbness in the genital area or between the legs, urinary or bowel problems, fever, unexplained weight loss, persistent night pain, or intense pain after a fall.
These signs are not the most common, but they should be taken seriously. They may indicate significant nerve damage or a medical cause that requires prompt evaluation.
For more mechanical pain, without warning signs, a consultation may also be useful if the pain persists, returns often, limits walking, prevents sleep or does not improve despite simple adjustments.
Conclusion — Finding the true cause leads to better pain relief
Pain that radiates down the leg isn’t always sciatica. The term is often used whenever pain originates in the lower back, crosses the buttock, or travels down the thigh. However, several musculoskeletal disorders can produce very similar pain without necessarily involving lumbar nerve compression.
Piriformis syndrome, deep gluteal syndrome, gluteus medius syndrome, sacroiliac joint dysfunction, proximal hamstring tendinopathy, coccydynia, greater trochanteric pain syndrome, and referred mechanical low back pain can all mimic sciatica. The location, aggravating factors, the presence or absence of neurological signs, and the response to movement help guide the evaluation.
The key is not to treat only the path of the pain, but to understand its origin. True sciatica requires particular attention to neurological signs. False sciatica, on the other hand, requires an analysis of the muscles, tendons, pelvis, hip, posture, gait, and postural compensations.
Osteopathy can play a useful role in this overall assessment, helping to improve mobility, reduce tension, support the return to movement, and guide the patient toward more suitable exercises. However, a cautious approach remains essential: weakness, significant numbness, urinary or bowel problems, fever, unusual nighttime pain, or pain following trauma should always prompt a prompt medical evaluation.
Better distinguishing sciatica from its imitators helps avoid treatment errors, inappropriate stretches, and unnecessary anxiety. Often, identifying the correct source—nerve, muscle, tendon, joint, or compensatory mechanism—makes relief more precise, longer-lasting, and safer.
References
- Jensen RK, Kongsted A, Kjaer P, Koes B. Diagnosis and treatment of sciatica. BMJ . 2019;367:l6273.
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth. 2007;99(4):461-473.
- Hicks BL, Lam JC, Varacallo M. Piriformis Syndrome. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- Martin HD, Reddy M, Gómez-Hoyos J. Deep gluteal syndrome. J Hip Preserv Surg. 2015;2(2):99-107.
- Yoon YH, et al. Beyond nerve entrapment: a narrative review of muscle–tendon contributions in deep gluteal syndrome. Diagnostics. 2025;15(19):2531.
- Speers CJB, Bhogal GS. Greater trochanteric pain syndrome: a review of diagnosis and management in general practice. Br J Gen Pract. 2017;67(663):479-480.
- Gomez LP, et al. Greater Trochanteric Pain Syndrome. StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
- Grimaldi A, et al. Gluteal tendinopathy masterclass: refuting the myths and improving clinical reasoning. Musculoskelet Sci Pract. 2025.
- Cohen SP. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment. Expert Rev Neurother. 2013;13(1):99-116.
- Telli H, Telli S, Topal M. Determination of the prevalence from clinical diagnosis of sacroiliac joint dysfunction in patients with lumbar disc hernia and low back pain. Pain Physician. 2020;23(2):E185-E191.
- Mattiussi G, Moreno C. Treatment of proximal hamstring tendinopathy-related sciatic nerve entrapment: presentation of an ultrasound-guided “intratissue percutaneous electrolysis” application. J Hum Sport Exerc. 2016;11(2):1-9.
- Klerx SP, et al. Clinimetric properties of sacroiliac joint mobility tests: a systematic review. Musculoskelet Sci Pra









{kind=link}