Facebook
X
Vimeo
VKontakte
Youtube
English
Français
(
French
)
简体中文
(
Chinese (Simplified)
)
Pain Map
Ankle
Back arm
Chest
Elbow
Feet
Groin
Hand
Head
Hip
Knee
Leg
Pelvis
Rib
Shoulder
Spine
Thigh
TMJ
Wrist
Pediatry
Adolescent
Infant:
Newborn
Preschooler
School-Age Child
Toddler
Women
Female Hypermobility & Biomechanics
Pregancy
Structural Adaptations in Female Anatomy
Women health issue
Sport
Ballet
Baseball
Basketball
Bodybuilding
Exercise and stretch
Football
Golf
Hockey
Soccer
Surfing
Tennis
Mind-Body
Emotional Regulation Techniques
Emotional Transmission & Somatic Memory
Evolutionary Neuropsychology
Holistic Osteopathy
Holistic Public Health Perspectives
Intuition & Healing in Osteopathy
Mind‑Body Integration
Philosophy and Ethics in Healing
Psychogenealogy & Healing
Social Neuroscience & Connection
Somatic and Planetary Health
Somato‑Emotional Release Techniques
Somatosensory and Neurological Disorders
Spiritual‑Clinical Integration
History
Advocacy & Legal Struggles
Development of Osteopathy in Canada
Early Opposition & Recognition
Evidence-Based Osteopathy
Founders
Holistic Medicine Roots
Institutional Evolution
Medical Revolution
Philosophical Principles & Legacy
Pioneers
Techniques Through Time
Viscero‑Somatic Reflex Theory
Search
OsteoMag
OsteoMag
English
Français
(
French
)
简体中文
(
Chinese (Simplified)
)
Pain Map
All
Ankle
Back arm
Chest
Elbow
Ballet
Common Ballet Injuries: Causes, Symptoms, and Prevention
Baseball
Suprascapular Nerve: Injuries and Osteopathic Treatment
Knee
When a Knee Injury Disrupts the Whole Body
Knee
Knee Anatomy: Dr. Eng’s Fascial Slip and IT Band Link
Pediatry
All
Adolescent
Infant:
Newborn
Preschooler
Ballet
Common Ballet Injuries: Causes, Symptoms, and Prevention
Pediatric osteopathy
Osteopathy and Childhood Constipation: A Complete Approach for Natural Relief
Emotional Transmission & Somatic Memory
Healing from Within: How Parental Anxiety Influences Child Behavior and the Role of Osteopathy
Pediatric osteopathy
Understanding SIDS: The Role of Osteopathy in Infant Health and Safety
Women
All
Female Hypermobility & Biomechanics
Pregancy
Structural Adaptations in Female Anatomy
Women health issue
Women health issue
Managing Endometriosis with Osteopathy
Biomecanic
At the Crossroads of Postures: Deciphering Postural Changes During Pregnancy
Female Hypermobility & Biomechanics
Female Body: Hypermobility & Structural Adaptations
Pregancy
Osteopathy and pregnancy
Sport
All
Ballet
Baseball
Basketball
Bodybuilding
Ballet
Common Ballet Injuries: Causes, Symptoms, and Prevention
Baseball
Suprascapular Nerve: Injuries and Osteopathic Treatment
Ballet
Foot Instability En Pointe: Ballet Challenges & Fixes
Bodybuilding
Deadlifts at the Gym: Should You Avoid Them or Include Them With Caution?
Mind-Body
All
Emotional Regulation Techniques
Emotional Transmission & Somatic Memory
Evolutionary Neuropsychology
Holistic Osteopathy
Mind-Body Connection
Critical Thinking in Health: A Lesson from Bonhoeffer
Mind-Body Connection
Confucius and Osteopathy: Healing Through Harmony
Mind-Body Connection
Contempt and Connection: How Division Affects Our Health & Society
Holistic Public Health Perspectives
A World in Crisis: Holistic Solutions for Global Health
History
All
Advocacy & Legal Struggles
Development of Osteopathy in Canada
Early Opposition & Recognition
Evidence-Based Osteopathy
Early Opposition & Recognition
Rediscovering Magnetism: The Hidden Legacy of Osteopathy
Holistic Medicine Roots
Osteopathy’s Origins: The 19th Century Rise of Alternative Medicine
Founders
Native American Medicine’s Influence on Osteopathy
Founders
Helen Keller’s Journey with Osteopathy Advocacy
Search
articles
Home
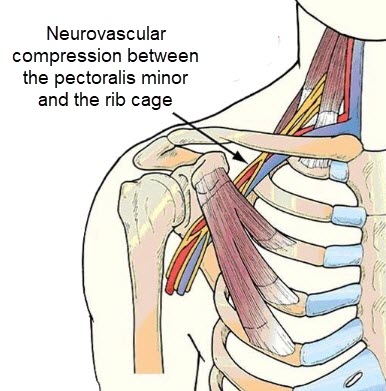
Osteopathic care: Pectoralis minor and thoracic outlet syndrome
pectoral-minor-syndrome
pectoral-minor-syndrome
pectoral minor syndrome