

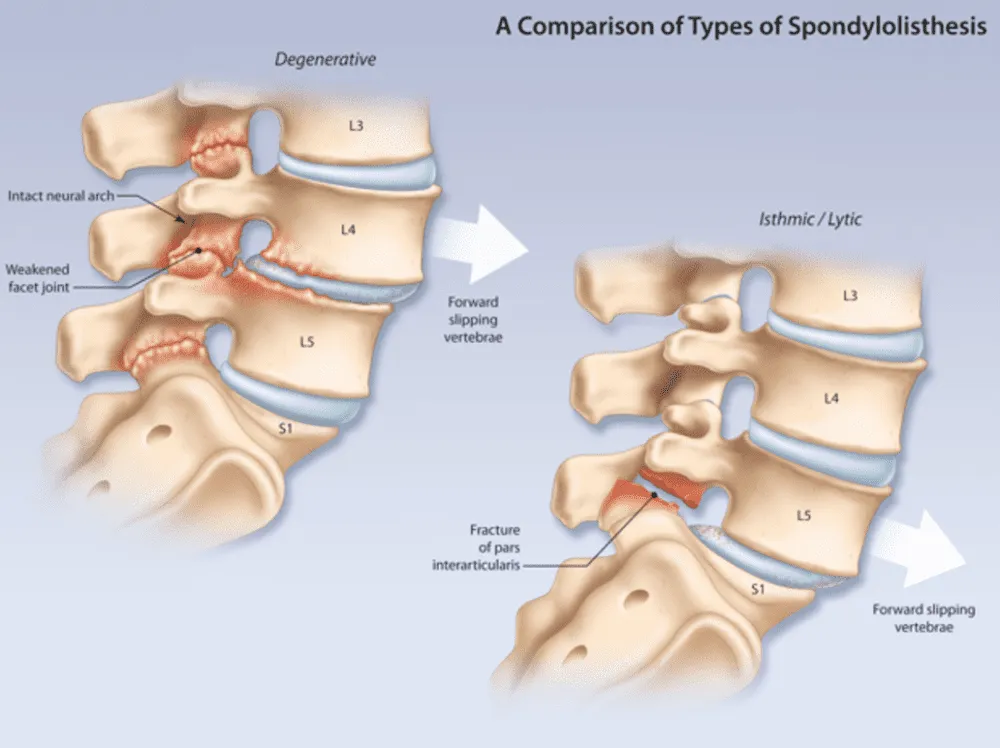
Degenerative spondylolisthesis is a forward slippage of a lumbar vertebral body that is the result of degeneration and alteration of the facet joints in conjunction with degenerative changes to the intervertebral disc (normal drying of the disc with aging).
Introduction
By definition, the lamina and pars interarticularis remained intact. This condition most commonly occurs between the fourth and fifth vertebral bodies. Degenerative spondylolisthesis is more common in women over the age of 40. This condition is a result of the general aging process during which the bones, joints and ligaments of the spine weaken and are less able to maintaining the spine in alignment during which the bones, joints, and ligaments of the spine weaken and are less able to hold the spine in alignment.
Degenerative spondylolisthesis, a delicate condition of the spine, originates from degenerative changes in the intervertebral discs. This alteration can lead to symptoms such as lower back pain and stiffness, significantly impacting quality of life. For people seeking a holistic approach, osteopathy presents itself as a valuable ally. Using adapted techniques, osteopaths work to relieve pain, restore mobility, and strengthen the stability of the spine, thus offering a complete response to the challenges posed by degenerative spondylolisthesis. Explore with us the different facets of this condition and discover how osteopathy can play a crucial role in the search for lasting solutions.
Vertebral degenerative process leading to spondylolisthesis
- As we age, general wear and tear causes changes in the spine.
- The intervertebral discs begin to dry out and weaken.
- They lose height, become stiff and begin to swell.
- This disc degeneration is the beginning of both arthritis and degenerative spondylolisthesis (DS).
- As arthritis develops, it weakens the joints and ligaments that hold your vertebrae in the correct position.
- The ligament at the back of the spine (yellow ligament) may begin to deform.
- One of the vertebrae on either side of a worn, flattened disc may loosen and advance onto the vertebra below.
- This slippage can narrow the spinal canal and put pressure on the spinal cord.
- This narrowing of the spinal canal is called spinal stenosis and is a common problem in patients with DS.
Foraminal stenosis (foramen)
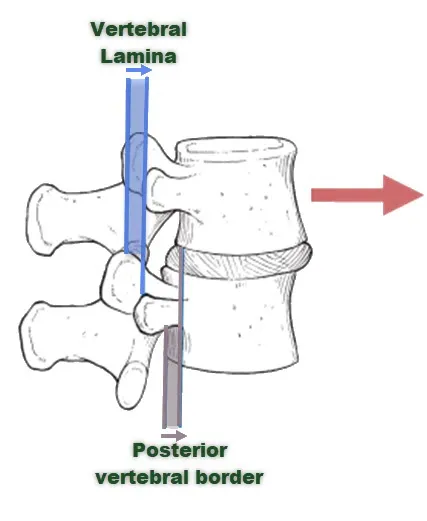
Narrowing of the intervertebral joint space and the development of facet osteoarthritis subsequently lead to forward vertebral subluxation. Additionally, hypertrophy of the ligamentum flavum may occur. This will then result in stenosis between the vertebral lamina and the posterior edge of the underlying vertebra. This condition mainly occurs after fifty years, it is four to six times more common in women than in men and it more frequently affects the L4-L5 level. The displacement is normally less than or equal to one third of the anteroposterior diameter of the upper border of the adjacent vertebral body. This movement does not progress, but is slowed down by the continued degeneration of the intervertebral joints and facets.
Epidemiology
- More common in diabetics and women over 40.
- Eight times more common in women than men, possibly due to the presence of ligamentous hyperlaxity due to hormonal changes during pregnancy and menopause.
- Present 5 times more common at the L4-S5 level (isthmic spondylolisthesis is more common at the L5-S1 level)
What causes degenerative spondylolisthesis
- Aging:
- Aging is one of the main causes of degenerative spondylolisthesis. With age, intervertebral discs lose water and elasticity, becoming more prone to wear. The joints between the vertebrae may also show signs of degeneration.
- Wear of Intervertebral Discs (Osteoarthritis):
- Osteoarthritis, a form of joint degeneration, can affect the intervertebral discs. Disc wear can cause the discs to lose height, which contributes to one vertebra slipping over another.
- Heredity and Genetic Predisposition:
- Some individuals may have a genetic predisposition to developing degenerative spinal problems, including degenerative spondylolisthesis. Genetic factors can influence the structure and strength of the intervertebral discs.
- Trauma or Injury:
- Although degenerative spondylolisthesis is often linked to natural degenerative changes, trauma or injury to the spine can also contribute to the condition. This can include fractures or damage to the intervertebral joints.
- Ligament Weakness:
- Weakness in the ligaments that hold the vertebrae together can increase the risk of spinal slippage. Weakened ligaments may not provide adequate support, allowing abnormal movement of the vertebrae.
- Congenital Defects:
- Some individuals are born with congenital spinal abnormalities that can make the spine more susceptible to degenerative spondylolisthesis. These abnormalities can affect the normal structure of the vertebrae and joints.
- Obesity :
- Being overweight or obese can increase the load on the spine, especially on the intervertebral discs. This can accelerate the degeneration process and increase the risk of spinal slippage.
- Physical Inactivity:
- Low physical activity can contribute to the degeneration of intervertebral discs. Regular exercise is important for maintaining spinal health, strengthening supporting muscles, and preventing vertebrae from slipping.
Symptoms
- Lower back pain :
- Lower back pain is one of the most common symptoms of degenerative spondylolisthesis. It may be felt in the lower back and worsen with certain activities, such as walking, prolonged standing, or flexion of the spine.
- Lumbar stiffness:
- Stiffness in the lumbar region is often associated with degenerative spondylolisthesis. Patients may experience limitation in spinal mobility, particularly during forward bending or rotational movements.
- Sensations of Tingling or Numbness:
- If degenerative spondylolisthesis compresses nearby nerves, it may cause tingling sensations, numbness, or sensory disturbances along the path of the affected nerve. These symptoms can extend to the buttocks, thighs, or even down to the legs and feet.
- Muscular weakness :
- Significant spinal slippage can compress nerve roots, causing muscle weakness in the legs. This can affect the ability to walk normally and maintain balance.
- Radicular Pain (Sciatica):
- If the compressed nerve roots are located in the lower back, this can cause radicular pain that travels along the sciatic nerve. This pain can radiate into the buttocks, thighs, and even down to the feet.
- Spinal Instability:
- Some patients may experience a feeling of instability in the spine, which can lead to difficulty maintaining certain positions, such as standing for long periods of time.
- Modification of the Lumbar Curvature (Lordosis):
- In some individuals, degenerative spondylolisthesis can change the natural curvature of the lumbar spine (lordosis). This may be noticeable visually and may contribute to pain and posture distortion.
Osteopathic Diagnosis and Evaluation
Osteopaths play an important role in evaluating patients with symptoms of degenerative spondylolisthesis. Although the final diagnosis usually requires medical imaging tests such as x-rays, the initial osteopathic evaluation process relies on a thorough clinical examination and collection of a detailed medical history. Here is how osteopaths generally approach the diagnosis of degenerative spondylolisthesis:
- History and Medical History:
- The osteopath will begin by gathering detailed information about the patient’s medical history, including any history of lower back pain, trauma, orthopedic problems, or pre-existing medical conditions. Information on lifestyle, physical activity, and symptom triggers will also be assessed.
- General Physical Examination:
- A general physical examination is performed to assess the patient’s posture, mobility, and any apparent asymmetry. Osteopaths are trained to detect physical signs that could indicate problems with the spine, including degenerative spondylolisthesis.
- Spine Mobility Assessment:
- The osteopath will assess the mobility of the patient’s spine by performing various tests and movements. This may include assessments of flexion, extension, rotation, and lateral tilt to identify any movement limitations or asymmetries.
- Neurological Assessment:
- Neurological tests are performed to evaluate the function of the nerves. This may include assessments of muscle strength, reflexes, and sensations along nerve pathways that may be affected by degenerative spondylolisthesis.
- Palpation and Search for Sensitive Points:
- The osteopath will use palpation to assess the anatomical structures of the spine, including the intervertebral discs, facet joints, and surrounding muscles. Looking for trouble spots or areas of tension can provide clues to the location and nature of problems.
- Postural Assessment:
- The osteopath will examine the patient’s posture during different positions, including standing, sitting and moving. Postural changes related to degenerative spondylolisthesis may be observed.
- Symptom Assessment:
- The osteopath will gather information about the patient’s specific symptoms, including the nature of the pain, activities that trigger or worsen the symptoms, and any radiation of the pain to other areas of the body.
Osteopathic Treatment of Degenerative Spondylolisthesis
- Stretching and Gentle Mobilization:
- Stretches and gentle mobilizations can be used to improve spinal flexibility and mobility. This can help reduce stiffness and make movement easier without causing undue strain.
- Work on the Paravertebral Muscles:
- Degenerative spondylolisthesis can cause overstrain of the paraspinal muscles. Osteopathic techniques may include gentle manipulations to release muscle tension and improve muscular balance around the spine.
- Postural Rehabilitation:
- Osteopaths can provide posture advice and postural rehabilitation exercises to help patients maintain optimal spinal position and prevent excessive pressure on the intervertebral discs.
- Relaxation and Stress Management Approaches:
- Stress management is important in treating degenerative spondylolisthesis because stress can make pain worse. Relaxation techniques, deep breathing, and other stress management methods can be integrated into osteopathic treatment.
- Lifestyle and Exercise Education:
- Lifestyle education, including advice on appropriate physical activity, workplace ergonomics, and weight management, is essential. Osteopaths can recommend specific exercises to strengthen supporting muscles and improve spinal stability.
- Collaboration with Other Health Professionals:
- The osteopath can work in collaboration with other health professionals, such as physiotherapists, orthopedists, or neurosurgeons, to ensure an integrated approach to treatment. This may include surgical procedures if necessary.
Exercises and Rehabilitation for Spondylolisthesis
Rehabilitation and specific exercises for degenerative spondylolisthesis aim to strengthen the stabilizing muscles of the spine, improve flexibility, and promote optimal posture. However, it is essential to consult a healthcare professional, such as an osteopath, physiotherapist or doctor, before starting any exercise program. Here are some general tips on exercises and rehabilitation for degenerative spondylolisthesis:
- Strengthening the Abdominal Muscles:
- Strong abdominal muscles can help stabilize the spine. Exercises such as planks, leg raises, and modified crunches can be adapted to strengthen the abdominals without creating undue stress on the lumbar spine.
- Strengthening the Lumbar Muscles:
- Lower back muscle strengthening exercises are important for stabilizing the spine. Lumbar extensions, hyperextensions on an incline bench, and superman exercises can be included in the program.
- Strengthening the Glutes:
- The gluteal muscles play a crucial role in pelvic stability. Exercises such as lunges, pelvic bridges, and lateral leg raises can help strengthen the gluteal muscles.
- Hamstring Stretches:
- Soft hamstrings can help reduce strain on the spine. Static hamstring stretches, such as seated forward bends, can be incorporated into the program.
- Pelvic Stabilization Exercises:
- Pelvic stabilization exercises, like pelvic rotations and pelvic raises, can help strengthen the deep muscles that stabilize the pelvic region.
- Unilateral Stabilization Exercises:
- Unilateral stabilization exercises, such as single-leg exercises or balancing movements, can help improve balance and strengthen the stabilizer muscles.
- Lateral Shaping Exercises:
- Lateral core exercises, such as side planks, can strengthen the oblique muscles and contribute to increased lateral stability.
- Coordination and Balance Exercises:
- Exercises that improve coordination and balance, such as walking in a straight line or using a balance board, can help strengthen the stabilizing muscles of the spine.
- Controlled Breathing Exercises:
- Controlled breathing exercises, such as diaphragmatic breathing, may be included to promote core stability.
- Swimming (according to Tolerance):
- Swimming, especially breaststroke or backstroke, can be a beneficial exercise option for strengthening core muscles while minimizing pressure on the spine.
Pain Management: Osteopathic Approaches
- Myofascial Release Techniques:
- Osteopaths may use myofascial release techniques to release muscular tension around the spine. This may include massage, muscle rolling, and other methods aimed at relaxing the paraspinal muscles.
- Targeted Stretches:
- Specific stretches may be prescribed to improve flexibility and reduce muscle tension. Stretches can target the muscles of the lower back, hips, and hamstrings to help relieve pressure on the spine.
- Manipulations of the Pelvic Region:
- Manipulations of the pelvic region can help restore pelvic balance and reduce pressure on the lumbar vertebrae. This can help relieve pain and improve spinal stability.
- Nerve Release Techniques:
- Nerve release techniques can be used to release tension around compressed nerves. This may include gentle mobilizations to improve nerve mobility and reduce sensations of tingling or numbness.
- Spine Stabilization Exercises:
- Specific exercises aimed at strengthening the stabilizing muscles of the spine may be prescribed. These exercises help support the spine and minimize the load on the intervertebral discs.
- Relaxation and Stress Management Techniques:
- Stress management is an important aspect of pain management. Osteopaths can teach relaxation techniques, such as deep breathing and visualization, to help patients manage stress and ease associated muscle tension.
- Self-Care Education:
- The osteopath can provide advice on self-care, including correct postures, home stretching exercises, and strategies to avoid movements that could worsen the pain.
Tips for Preventing Degenerative Spondylolisthesis
- Maintain a Healthy Weight:
- Maintaining a healthy weight is essential, as excess weight can increase pressure on the spine and contribute to degeneration of the spinal discs.
- Adopt Good Posture:
- Good posture is crucial for spinal health. Avoid leaning forward or slouching. Be sure to maintain a neutral posture when walking, sitting, and standing.
- Practicing Regular Exercises:
- Regular exercise strengthens the supporting muscles of the spine, improves flexibility and contributes to stability. Exercises such as swimming, walking and strength training may be beneficial.
- Avoiding Traumatic Repetitive Movements:
- Avoid repetitive movements that can be traumatic to the spine, especially excessive twisting and bending movements.
- Ergonomics at Work:
- If you work long hours at a computer, make sure your workstation is ergonomic. Use a chair that supports the natural curvature of your spine and position your screen at eye level.
- Educate on Safe Lifting:
- When lifting heavy objects, bend your knees, keep your back straight, and use your leg muscles to lift rather than bend at the waist.
- Maintain Good Hydration:
- Dehydration can contribute to the degeneration of intervertebral discs. Make sure you stay well hydrated to keep the discs supple.
- Avoid Smoking:
- Smoking has been linked to spinal disc problems. Avoiding tobacco can help with overall spinal health.
- Practice Relaxation and Stress Management:
- Stress can make symptoms worse and contribute to muscle tension. Practicing relaxation techniques, such as meditation or deep breathing, can be beneficial.
- Do Regular Stretching:
- Incorporate regular stretching into your daily routine to maintain flexibility in muscles and joints.
- Consult a Health Professional:
- If you have a family history of spinal problems or experience persistent lower back pain, consult a healthcare professional for personalized advice.
Degenerative Spondylolisthesis in the Elderly
- Accurate Diagnosis:
- Because degenerative spondylolisthesis may be related to natural age-related degenerative changes of the spine, an accurate diagnosis is essential. Imaging tests, such as X-rays or MRIs, may be needed to assess the severity of the condition and guide the treatment plan.
- Taking Comorbidities into Account:
- Older adults may have other health conditions or comorbidities that require special attention. Osteopaths should take these factors into account when developing a treatment plan tailored to the patient’s overall condition.
- Conservative Approaches:
- Conservative osteopathic approaches, such as gentle spinal manipulation, stretching, and muscle strengthening exercises, can be used to relieve pain, improve mobility, and promote spinal stability.
- Self-Management Education:
- Osteopaths can play a crucial role in educating older adults on self-management techniques, including home exercises, postural advice, and strategies to alleviate symptoms on a daily basis.
- Pain Management:
- Pain management is often a priority in older adults with degenerative spondylolisthesis. Osteopaths can use gentle manipulation techniques and myofascial release approaches to relieve pain and improve quality of life.
- Adaptation of Techniques:
- Osteopathic techniques must be adapted according to the individual tolerance and potential fragility of the elderly. Delicate adjustments and gentle approaches may be preferred to avoid any risk of complications.
- Multidisciplinary collaboration:
- Working in collaboration with other healthcare professionals, such as physiotherapists, rheumatologists, or pain specialists, can contribute to a holistic and comprehensive approach to degenerative spondylolisthesis in older adults.
- Promotion of Autonomy:
- Encouraging independence is an important aspect of treatment in older adults. Osteopaths can work with patients to develop strategies that promote independence and functionality.
Pseudo-claudication (neurogenic) and intermittent claudication (vascular)
As with classic intermittent claudication, the pain is triggered by walking and relieved by rest. However, it appears that pseudo-claudication is secondary to mechanical compression of spinal contents, whereas intermittent claudication is the result of vascular insufficiency. The two conditions can be distinguished by their symptoms.
| Neurogenic | Vascular | |
| Location | Wave | Especially in the calf |
| Paresthesia | Present | Absent |
| Walk | Worse | Worse |
| Standing without moving | Worse | Better |
| Leaning | Better | No change |
| Cycling | No change | Worsen |
| Laying down on the chest | Worsen | No change |
Conclusion
In conclusion, degenerative spondylolisthesis is a condition that can have a significant impact on the quality of life of individuals, particularly in the elderly. Natural age-related degenerative changes to the spine contribute to the development of this condition, requiring tailored treatment approaches. Osteopaths play an important role in the management of degenerative spondylolisthesis by using specific techniques to relieve pain, improve mobility and promote spinal stability.
The osteopathic approach takes into account the whole individual, considering the physical, psychological and emotional dimensions. For older adults, consideration of comorbidities, safety and respect for individual tolerance are essential in developing an effective treatment plan.
Prevention of degenerative spondylolisthesis, particularly in the elderly, is based on healthy lifestyle habits, adequate posture, and management of risk factors. Education about self-care and the promotion of autonomy are an integral part of care.
It is imperative that osteopaths work collaboratively with other healthcare professionals, adapt their techniques according to the specific needs of each patient and integrate holistic approaches to ensure comprehensive and effective management of degenerative spondylolisthesis. Ongoing research and knowledge sharing also contribute to improving practices and providing quality care for this particular population.
























{kind=link}