

Introduction
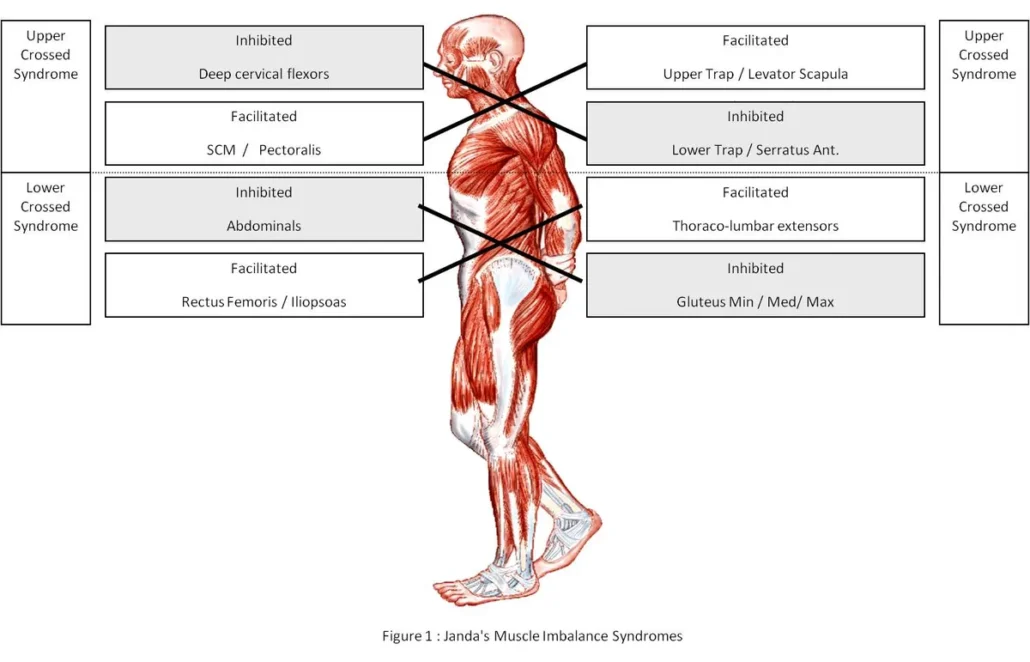
Janda Crossed Muscle Imbalance Syndrome, named after famous Czech physiotherapist Vladimir Janda, is a complex condition that results from muscular imbalances between agonist and antagonist muscles, as well as between stabilizer and mobilizer muscles. This syndrome can have a significant impact on posture, body biomechanics and overall musculoskeletal function.

One of the fundamental features of crossed muscle imbalance syndrome is the development of inadequate compensatory motor patterns. These patterns are often the result of neuromuscular dysfunctions and are triggered by factors such as pain, muscle fatigue, trauma or incorrect postural habits. For example, an imbalance between the hip flexor muscles and the extensor muscles can lead to excessive lumbar lordosis and abdominal protrusion, contributing to back problems.
One of the most common muscle imbalances associated with crossed muscle imbalance syndrome is that between the hip flexor muscles and the abdominal muscles. In many individuals, especially those who spend long periods of time sitting, the hip flexor muscles become shortened and tight, while the abdominal muscles become weak and stretched. This creates an imbalance in the pelvic region, leading to forward posture of the pelvis, lumbar hyperlordosis, and eventually lower back pain.
Additionally, an imbalance between the neck and shoulder muscles can lead to postural problems such as upper cross syndrome. In this condition, the neck muscles, such as the upper trapezius and levator scapula muscles, become hypertrophied and tight, while the muscles of the mid and lower back become weak and stretched. This can lead to forward head posture, rounded shoulders, and increased thoracic curvature, which in turn can cause neck and chest pain.
To diagnose and treat Janda Crossed Muscle Imbalance Syndrome, a thorough assessment of posture, joint mobility, and muscle strength is necessary. Assessment techniques often include muscle length testing, isometric strength testing, and dynamic posture assessments. Once the imbalance is identified, a specific rehabilitation program can be developed to restore muscle balance and improve posture and function.
This rehabilitation program may include targeted muscle strengthening exercises for weak muscles, stretches for tight muscles, and posture correction techniques. The goal is to restore muscle balance and reestablish optimal body biomechanics to reduce pain, improve function and prevent recurrence.
Vladimir Janda (1928-2002)
Vladimir Janda (1928-2002) was a renowned physiotherapist from Czechoslovakia, now the Czech Republic. He is widely recognized as one of the pioneers of physical medicine and rehabilitation, particularly for his contributions to the understanding of muscular imbalances and postural disorders.
Janda has spent much of his career studying the complex interactions between muscles and joints, and their impact on posture and musculoskeletal function. He developed the concept of muscle imbalance syndromes, which describes compensatory motor patterns that develop in response to chronic muscular imbalances.
Among his most important contributions are the description of various muscle imbalance syndromes, such as upper crossed syndrome and lower crossed syndrome. These syndromes describe specific patterns of muscular imbalances between agonist and antagonist muscles, as well as between stabilizer and mobilizer muscles, which can contribute to postural disorders and musculoskeletal pain.
Janda has also developed specific assessment and treatment techniques to identify and correct these muscular imbalances. His treatment methods often included targeted muscle strengthening exercises, stretching, and posture correction techniques.
Janda’s work has had considerable influence in the field of rehabilitation and physical therapy, and his concepts continue to be widely used by healthcare professionals across the world. His legacy lives on through the many books and articles he wrote, as well as the training and teaching he provided to numerous physical therapists and health care professionals throughout his career.
Upper crossed syndrome
Upper crossed syndrome is a muscular and postural imbalance characterized by a combination of muscle weakness and excessive tension in certain areas of the body, resulting in an unbalanced posture. This syndrome is often associated with imbalances between the muscles of the upper body, particularly those of the neck, shoulders and trunk.
The main elements of upper crossed syndrome include weakness of the rhomboid muscles, lower trapezius, serratus anterior muscles, as well as the muscles of the deep cervical region. At the same time, there is excessive tension in the neck muscles, such as the upper trapezius, levator scapula, scalene muscles, and sternocleidomastoid muscles.
This combination of weakness and tension creates a postural imbalance that results in forward head posture, forward rounded shoulders, and increased thoracic curvature. Visually, this gives the impression that the shoulders are tucked forward and the head is forward in relation to the midline of the body.
The causes of upper crossed syndrome are multiple and can include long periods of sitting, excessive use of electronic devices, incorrect postural habits, and muscle imbalances that are inherited or developed over time. These factors contribute to musculoskeletal misalignment that can lead to upper body pain and dysfunction.
Diagnosis and treatment of upper cross syndrome
Diagnosis and treatment of upper crossed syndrome involves a multidisciplinary approach, including precise posture assessment, muscle strength testing, and clinical examinations to identify specific muscle imbalances. Here is a general approach to the diagnosis and treatment of this condition:
Diagnostic
- Detailed history: Ask the patient about their medical history, lifestyle, postural habits, daily activities and current symptoms.
- Physical examination:
- Observation of general posture, including the position of the head, shoulders, trunk and upper limbs.
- Assessment of joint mobility, with emphasis on the cervical region, shoulders and rib cage.
- Palpation of the muscles to identify areas of tension and sensitivity, as well as possible trigger points.
- Muscle strength tests: Assess the strength and endurance of the muscles involved in upper crossed syndrome, focusing on the muscles of the back, shoulders and neck.
- Dynamic Posture Assessment: Observe the patient’s posture during functional movements such as walking, going up and down stairs, and raising the arms.
Treatment
- Posture Correction: Educate the patient on the principles of good posture and teach them techniques to actively correct their posture on a daily basis.
- Muscle strengthening: Develop a specific strengthening exercise program for weakened muscles, with emphasis on the rhomboids, lower trapezius and stabilizing muscles of the cervical region.
- Stretching: Prescribe stretching exercises to loosen tight muscles, especially neck and shoulder muscles, such as the upper trapezius and scalenes.
- Joint Mobilization: Use joint mobilization techniques to improve mobility of the cervical and thoracic joints, promoting better posture and function.
- Manual therapy: Use manual therapy techniques such as myofascial release and massage to relieve muscle tension and associated pain.
- Ergonomic correction: Provide advice on workspace layout and adoption of ergonomic postures to reduce stress on upper body muscles.
- Monitoring and Reassessment: Monitor the patient’s progress over time and adjust the treatment plan based on their specific response and needs.
Lower crossed syndrome
Lower Crossed Syndrome, also known as Lower Crossed Syndrome, is a condition characterized by a set of symptoms related to muscular imbalance and poor posture in the pelvis and lower back. It is often associated with lower back pain and mobility problems.
In this syndrome, there is an imbalance between the muscles of the pelvis, particularly between the iliopsoas muscle (hip flexor) and the gluteal muscles, such as the gluteus muscle. This imbalance can lead to anterior pelvic tilt, pelvic rotation, and lumbar hyperlordosis (increased curvature in the lumbar region of the spine).
Possible causes of lower Crossed syndrome include muscle imbalance due to poor posture, muscle weakness, or unfavorable movement habits. People who spend a lot of time sitting or who perform activities that disproportionately use certain muscle groups, such as athletes, may be more likely to develop this syndrome.
Treatment for lower Crossed syndrome generally aims to restore muscle balance, improve posture, and relieve associated symptoms. This may involve specific strengthening and stretching exercises, postural adjustments, manipulation techniques, as well as changes to daily movement habits.
Diagnosis and treatment of lower Crossed syndrome
Diagnostic
- History: Collect the patient’s medical history, lifestyle habits, physical activities and current symptoms.
- Physical examination:
- Observation of general posture, with emphasis on the position of the pelvis, lumbar spine and lower limbs.
- Assessment of muscle strength of the abdominal muscles, glutes, lumbar muscles and hip flexors.
- Palpation to identify areas of tension and sensitivity, as well as muscular imbalances.
- Functional tests: Perform functional tests to assess hip mobility, pelvic stability and coordination of movements.
Treatment
- Muscle strengthening: Develop a strengthening exercise program for the abdominal muscles and glutes to strengthen them and restore muscle balance.
- Stretches: Prescribe stretches for the lower back muscles and hip flexors to reduce excess tension and improve flexibility.
- Postural Rehabilitation: Teach posture correction techniques to help the patient realign the pelvis and lumbar spine and adopt a more neutral position.
- Manual Therapy: Use manual therapy techniques such as spinal manipulation and myofascial release to relieve muscle tension and improve joint mobility.
- Patient Education: Provide guidance on ergonomics, correct postural habits, and lifestyle modifications to prevent recurrence and promote healthy posture.
- Correction of Biomechanical Imbalances: Work on correcting the underlying biomechanical imbalances that contribute to lower Crossed syndrome, such as lower extremity length imbalances or pelvic alignment disorders.
- Monitoring and adjustment: Monitor the patient’s progress over time and adjust the treatment plan based on their specific response and needs.
Muscle Imbalance Syndromes: An In-Depth Analysis
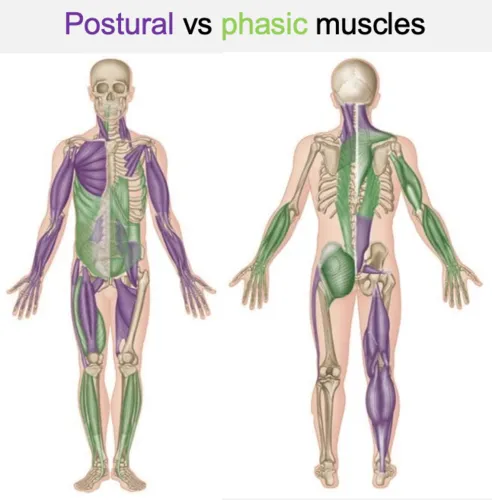
When considering muscle classifications based on their primary role, it is essential to note that these muscles are dynamic and can change function depending on the context in which they operate. In general, two main groups emerge: postural muscles and phasic muscles. Postural muscles are primarily involved in maintaining posture and tend to contract more when dysfunction occurs, while phasic muscles are mobilized for dynamic movements and tend to weaken when dysfunction occurs.
Over time, the motor programming of these muscles can be altered in response to chronic patterns. This adaptation leads to an inhibition of communication aimed at changing the pattern, thereby creating a perpetual cycle of muscular imbalance. Two major muscle imbalance syndromes are associated with these patterns: upper Crossed syndrome and lower Crossed syndrome.
Postural muscles, predominant in upper Crossed syndrome, are often anti-gravity muscles characterized by high resting tone. They are generally flexor muscles and are less prone to injury than phasic muscles. These muscles are primarily slow-twitch, geared toward endurance, and are constantly activated to maintain posture. As a result, they tend to be short and tight, but they atrophy less quickly than phasic muscles.
On the other hand, the phasic muscles, dominant in lower Crossed syndrome, do not fight against gravity but are used in response to a specific demand. They are often extensor muscles and are more vulnerable than postural muscles. These muscles are primarily fast-twitch, geared toward power and speed, and require strengthening for dynamic movements. However, when malfunctioning, they tend to be inhibited and weak. Additionally, they are more responsive to injury than postural muscles and atrophy more quickly, especially when involved in two-joint movements.
Conclusion
In conclusion, lower Crossedsyndrome is a complex condition that can lead to lower back pain and decreased mobility. It is important to recognize the signs and symptoms of this syndrome, such as anterior pelvic tilt and lumbar hyperlordosis, so that you can intervene quickly. The treatment, led by qualified healthcare professionals, aims to restore muscular and postural balance through exercises, postural adjustments and manipulative techniques. An individualized approach is essential to ensure optimal results and improve the quality of life of people affected by this syndrome.
References
- Ahearn EL, Greene A, Lasner A. Some effects of supplemental Pilates training on the posture, strength, and flexibility of dancers 17 to 22 years of age. J Dance Med Sci. 2018;22:192–202. [ PubMed ] [ Google Scholar ]
- Aladro-Gonzalvo AR, Machado-Díaz M, Moncada-Jiménez J, Hernández-Elizondo J, Araya-Vargas G. The effect of Pilates exercises on body composition: a systematic review. J Bodyw Mov Ther. 2012;16:109–114. [ PubMed ] [ Google Scholar ]
- Berglund L, Aasa B, Michaelson P, Aasa U. Sagittal lumbopelvic alignment in patients with low back pain and the effects of a high-load lifting exercise and individualized low-load motor control exercises-a randomized controlled trial. Spine J. 2018;18:399–406. [ PubMed ] [ Google Scholar ]
- Curnow D, Cobbin D, Wyndham J, Boris Choy ST. Altered motor control, posture and the Pilates method of exercise prescription. J Bodyw Mov Ther. 2009;13:104–111. [ PubMed ] [ Google Scholar ]
- Cuthbert SC, Goodheart GJ., Jr On the reliability and validity of manual muscle testing: a literature review. Chiropr Osteopat. 2007;15:4. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Freeman MA, Dean MR, Hanham IW. The etiology and prevention of functional instability of the foot. J Bone Joint Surg Br. 1965;47:678–685. [ PubMed ] [ Google Scholar ]
- Gleim GW, McHugh MP. Flexibility and its effects on sports injury and performance. Sports Med. 1997;24:289–299. [ PubMed ] [ Google Scholar ]
- Graven-Nielsen T, Lund H, Arendt-Nielsen L, Danneskiold-Samsøe B, Bliddal H. Inhibition of maximal voluntary contraction force by experimental muscle pain: a centrally mediated mechanism. Muscle Nerve. 2002;26:708–712. [ PubMed ] [ Google Scholar ]
- Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP) Arthritis Care Res (Hoboken) 2011;63(Suppl 11):S240–252. [ PubMed ] [ Google Scholar ]
- Hrysomallis C, Goodman C. A review of resistance exercise and posture realignment. J Strength Cond Res. 2001;15:385–390. [ PubMed ] [ Google Scholar ]
- Ihara H, Nakayama A. Dynamic joint control training for knee ligament injuries. Am J Sports Med. 1986;14:309–315. [ PubMed ] [ Google Scholar ]
- Janda V. On the concept of postural muscles and posture in man. Aust J Physiother. 1983;29:83–84. [ PubMed ] [ Google Scholar ]
- Janda V. Some aspects of extracranial causes of facial pain. J Prosthet Dent. 1986;56:484–487. [ PubMed ] [ Google Scholar ]
- Kelly BT, Kadrmas WR, Speer KP. The manual muscle examination for rotator cuff strength. An electromyographic investigation. Am J Sports Med. 1996;24:581–588. [ PubMed ] [ Google Scholar ]
- Krebs EE, Carey TS, Weinberger M. Accuracy of the pain numeric rating scale as a screening test in primary care. J Gen Intern Med. 2007;22:1453–1458. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Mannion AF, Balagué F, Pellisé F, Cedraschi C. Pain measurement in patients with low back pain. Nat Clin Pract Rheumatol. 2007;3:610–618. [ PubMed ] [ Google Scholar ]
- Mine K, Nakayama T, Milanese S, Grimmer K. Effectiveness of stretching on posterior shoulder tightness and glenohumeral internal-rotation deficit: a systematic review of randomized controlled trials. J Sport Rehabil. 2017;26:294–305. [ PubMed ] [ Google Scholar ]
- Nussbaumer S, Leunig M, Glatthorn JF, Stauffacher S, Gerber H, Maffiuletti NA. Validity and test-retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients. BMC Musculoskelet Disord. 2010;11:194. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Nyland J, Gamble C, Franklin T, Caborn DNM. Permanent knee sensorimotor system changes following ACL injury and surgery. Knee Surg Sports Traumatol Arthrosc. 2017;25:1461–1474. [ PubMed ] [ Google Scholar ]
- Page P. Current concepts in muscle stretching for exercise and rehabilitation. Int J Sports Phys Ther. 2012;7:109–119. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Page P. Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. Int J Sports Phys Ther. 2011;6:51–58. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Paolucci T, Zangrando F, Palladino D, Monaco A, Cordiani B, Mannocci A, Saraceni VM, Villani C. The sagittal spinal alignment in young swimmers and glide performance: the importance of lumbar lordosis. J Sports Med Phys Fitness. 2018;58:1555–1557. [ PubMed ] [ Google Scholar ]
- Rubini EC, Costa AL, Gomes PS. The effects of stretching on strength performance. Sports Med. 2007;37:213–224. [ PubMed ] [ Google Scholar ]
- Watson T, Graning J, McPherson S, Carter E, Edwards J, Melcher I, Burgess T. Dance, balance and core muscle performance measures are improved following a 9-week core stabilization training program among competitive collegiate dancers. Int J Sports Phys Ther. 2017;12:25–41. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Yuktasir B, Kaya F. Investigation into the long-term effects of static and PNF stretching exercises on range of motion and jump performance. J Bodyw Mov Ther. 2009;13:11–21. [ PubMed ] [ Google Scholar ]

 Weakness: Causes, Implications, and Solutions")








 Weakness: Causes, Implications, and Solutions")
{kind=link}