

The Extraordinary Journey of Andrew Taylor Still: From Traditional Medicine to the Foundation of Osteopathy
Like other medical visionaries, Andrew Taylor Still, the founder of osteopathy, sought recognition as an original thinker. In his autobiography, Still claimed that the principles of his approach came to him in a single moment of inspiration. He believed that most diseases were caused by spinal displacements, and eliminating them through spinal manipulation would relieve symptoms elsewhere in the body. Despite later modifications to this interpretation, his followers have failed to adequately identify the intellectual currents shaping his thought.
Still, born August 6, 1828, in Jonesville, Virginia, was the third of nine children. His father, Abrahamm, had been a Methodist preacher but turned to farming and medicine to support his family. The family moved to New Market, Tennessee, in 1834, when Abram accepted a preaching position.
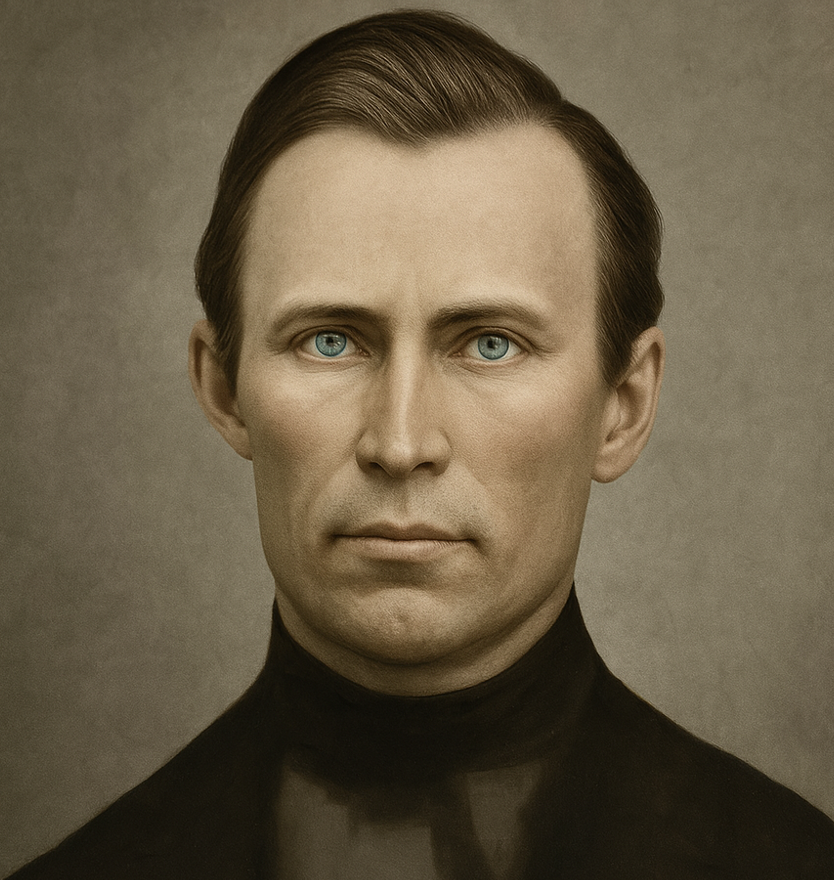
This image features Abraham Still, the father of Andrew Taylor Still, the founder of osteopathy.
Key Features:
Portrait: Abraham Still is depicted in a period-appropriate portrait, reflecting the style and attire of his era. His expression and posture may provide insights into his character and status.
Historical Context: Abraham Still was a prominent figure in the early life of Andrew Taylor Still. As a pioneer in the early American frontier, he played a significant role in shaping the environment and values that influenced his son’s later work in osteopathy.
Legacy: Abraham Still’s contributions to his community and his influence on his son are significant. His experiences and values were foundational in shaping the principles that Andrew Taylor Still would later incorporate into the practice of osteopathy.
Family Background: Understanding Abraham Still’s life and background provides valuable context for appreciating the early influences and familial connections that contributed to the development of osteopathic medicine.
This image of Abraham Still highlights his importance in the historical narrative of osteopathy, emphasizing the familial and historical connections that shaped the development of this medical field.
A colleague described Abram’s sermons as “simple, direct and practical.” This was the highest praise a backwoods Methodist minister could receive, for Methodists at the time did not regard the term “plain” as synonymous with boring: they practiced a fervent style of religion and devotion to the salvation of souls which, today, would be barely recognizable for this denomination. The Methodist preachers of Abram’s day wore dark garments; their steely gazes did not waver in the face of evil, and they were a commanding presence in the lawless environment of the American frontier. Abram and his colleagues were nicknamed the “sons of thunder” because of their fiery preaching, terrifying descriptions of hell, and colorful interpretations of Judgment Day. Imaginary lightning and thunder flashed around their open-air field pulpits as they battled the Devil and the forces of evil in a forest setting, lit eerily by flickering pine torches. Their self-taught vocabulary conjured up images so frightening that many children did not dare.
In the early 19th century, Methodist ministers traveled circuits, covering large geographic areas. Andrew’s education was marked by moves and interruptions, with periods of formal education from 1842 to 1848.
The family’s life as circuit riders was difficult, with frequent moves and insufficient income from the church. Andrew, as a child, took care of household chores and hunting, sometimes accompanying his father on ministerial tours and participating in religious revivals. In 1851, Abraham was appointed a missionary to the Kansas Territory, and Andrew, after marrying and starting a family, joined his parents at the Wakarusa Mission, opting for medicine as a career.

This image represents Abraham Still, the father of Andrew Taylor Still, founder of osteopathy. Abraham was a circuit rider, an itinerant preacher who traveled on horseback to provide religious services in rural and isolated communities during the 19th century. In addition to his spiritual work, Abraham also practiced medicine, blending care for both body and soul. His dual role as preacher and healer had a profound impact on his son, Andrew, who later developed the principles of osteopathy, emphasizing the holistic connection between the body, mind, and spirit. Abraham’s dedication to helping others laid the foundation for Andrew’s revolutionary approach to healthcare.
Growing up as the son of a circuit racer was no easy feat; the family had to endure constant moving and struggled with financial instability due to meager income from the church. However, despite the challenges, Andrew’s upbringing instilled in him a sense of responsibility and a strong work ethic from a young age.
Mother: Martha Hill Still
Andrew Still’s mother, Martha Hill Still, played a crucial role in the life of his family, particularly in the raising of her nine children, of whom Andrew was the third. Although less well known than her husband, Abraham Still, Martha was a loving and devoted figure who contributed to the education and well-being of her children despite the challenges of life in 19th-century rural America.

This image is a photographic print of Martha Poague Moore Still, an important figure in the history of osteopathy and the mother of Andrew Taylor Still.
Key Features:
Photographic Portrait: The print captures Martha Still’s likeness, offering a glimpse into her appearance and demeanor. Her tired look reflects the significant personal and familial challenges she faced.
Personal Life: Martha Poague Moore Still had ten children, and her life was marked by considerable hardship, including the loss of one of her children. These experiences are evident in the weariness visible in her photograph, highlighting the difficulties she endured.
Historical Context: As the wife of Andrew Taylor Still, Martha Still was integral to the Still family’s story. Her life and personal struggles contribute to a deeper understanding of the context in which the osteopathic movement developed.
Significance: The photographic print not only documents her physical appearance but also serves as a testament to her resilience and the demanding circumstances of her life. It provides valuable insight into the personal side of the Still family’s history.
As the wife of a Methodist preacher, Martha shared the challenges and responsibilities inherent in her husband’s itinerant life. With him, she moved several times, following the duties and calls of his ministry. These frequent moves and the resulting interruptions undoubtedly had an impact on the children’s education, including Andrew’s.
Despite hardship and displacement, Martha strove to maintain some stability in family life, providing a warm home and emotional support for her children. She was perhaps the pillar on which the Still family rested during times of transition and uncertainty.
Although history may have less documented Martha’s role compared to that of Abraham, it is likely that she was a quiet and essential force in the lives of her son Andrew and his family as a whole . His legacy is perhaps reflected in the compassion and dedication that Andrew Still later brought to his medical practice and the founding of osteopathy.
As a child, Andrew found himself taking on significant household responsibilities alongside his studies. He learned to help with various tasks and went on hunting expeditions to support his family. Additionally, he often accompanied his father on ministerial tours, becoming familiar with the rigors of religious work and participating in fervent religious revivals that were common at the time.
In 1851, Abraham Still received an important appointment as a missionary in the Kansas Territory. This pivotal moment in the family’s life prompted a major transition, as they once again uprooted themselves to embark on a new chapter in their missionary efforts. Andrew, now a young adult, had already started thinking about his future. Despite the family’s dedication to religious service, Andrew made the decision to pursue another vocation: medicine.
Slavery and Methodism
The relationship between early Methodism and the issue of slavery reveals the complex interplay of religious conviction, social justice, and cultural pressures. Abraham, like many early Methodist preachers in the Holston Circuit, embodied the antislavery ethos championed by John Wesley, the founder of Methodism. Wesley’s teachings emphasized human equality and moral justice, compelling early Methodists to actively challenge the institution of slavery through preaching and personal conduct.
The Antislavery Ethos in Early Methodism
Wesley’s Rules of the Societies promoted principles of universal human dignity. Early Methodist preachers not only exhorted their congregations to engage in acts of charity—such as feeding the hungry, clothing the naked, and visiting the sick—but also challenged societal norms that upheld practices like slavery. Alongside the rejection of slavery, Methodism also discouraged drinking spirits, gambling, excessive adornment, and exploitative practices like charging exorbitant interest. This holistic moral framework sought to cultivate a disciplined and ethical community rooted in social responsibility and spiritual purity.
Challenges in the Holston Circuit
Preachers in the Holston Circuit, like Abraham, faced significant resistance to their antislavery stance. Southern society’s dependence on slavery as an economic and cultural institution made such messages deeply unpopular. Those who preached against slavery were often ostracized, experiencing difficulty in securing basic necessities like food and shelter. This isolation highlights the cost of advocating for social justice in regions where slavery was deeply entrenched.
Methodism’s Institutional Struggles with Slavery
The Methodist Church initially made concerted efforts to eliminate slavery within its ranks. Early resolutions barred clergy and members from owning or trading slaves, reflecting Wesley’s radical opposition to the practice. However, as Methodism expanded into the Southern United States, where slavery was integral to the economy and culture, enforcing these rules became increasingly difficult.
In 1804, the General Conference suspended its regulations on slavery for Southern Methodists, effectively sidestepping the issue at a national level. This decision marked a turning point, as the church prioritized unity over its antislavery principles. By 1816, the General Conference committee on slavery acknowledged the practical impossibility of abolishing slavery under the prevailing societal conditions. Their report, which declared that “little can be done to abolish the practice if contrary to the principles of moral justice,” reflected a growing compromise within the church.
The Rising Schism
The church’s attempts to manage the slavery issue through compromise ultimately failed to bridge the widening divide between Northern and Southern Methodists. The moral clarity of Wesley’s antislavery principles clashed with the realities of a society increasingly polarized by the institution of slavery. The tension between moral justice and pragmatic adaptation led to growing dissatisfaction among both abolitionist members and those who supported slavery.
By the mid-19th century, this division culminated in the 1844 schism of the Methodist Episcopal Church, which split into Northern and Southern branches. This rupture underscored the intractable nature of the slavery debate and the inability of even religious institutions to transcend the societal conflicts of the time.
The Calomel Controversy: Between Heroic Medicine and the Dangers of Mercury
Benjamin Rush maintained that fever alone, by causing tension in the blood vessels, was the cause of disease. He concluded that the safest remedy would be to relieve this tension through the ancient techniques of bleeding and purging the stomach and intestines. Rush’s system was called heroic medicine, and it certainly took courage to endure this therapy, as patients were bled unconscious and purged with calomel (mercuric chloride) until they showed signs of illness. mercurial poisoning or begin to salivate.

This evocative engraving captures a pivotal moment in the history of Western medicine—an era dominated by what was known as heroic medicine. Popular in the 18th and early 19th centuries, this approach was rooted in the belief that disease stemmed from bodily imbalances or excesses, particularly of blood and bile. The image illustrates a physician performing bloodletting, a central tenet of this philosophy, on a young, unconscious woman, while a concerned assistant or apprentice looks on.
With its meticulous linework and somber tones, the scene conveys both the gravity and intensity of the procedure. Bloodletting was believed to reduce vascular tension and restore equilibrium, often paired with other extreme measures like purging and induced vomiting—particularly through substances like calomel (mercuric chloride). These aggressive interventions, though now discredited, were the medical orthodoxy of their time, taught in leading institutions and championed by figures like Benjamin Rush.
This image serves as a historical artifact, reminding us of medicine’s journey—from invasive, often harmful treatments based on theory and tradition, to today’s evidence-based and patient-centered care. It also underscores the enduring importance of critical inquiry in medical evolution.
From the University of Pennsylvania where Rush taught from 1768 until his death in 1813, Rush’s influence spread across the country, propelled by his own prolific writings and by former students who later taught the heroic therapies in other medical schools. From 1780 to 1850, this system dominated American medical thought and practice.

This neoclassical portrait captures Benjamin Rush, a pivotal figure in early American medicine, during the later years of his life. A signer of the Declaration of Independence and a leading physician of his era, Rush was both revered and controversial for his medical theories. In 1793, amid the devastating yellow fever epidemic in Philadelphia, Rush remained in the city to treat patients while many fled. He championed aggressive treatments—particularly bloodletting and purging—based on his belief that all disease stemmed from imbalances in the body’s vascular tension. These methods, known collectively as “heroic medicine,” reflected both his conviction and the limited understanding of pathology at the time.
Rush’s influence extended far beyond the clinic. As a professor at the University of Pennsylvania, he trained a generation of American physicians, and his prolific writings helped shape the development of American medical thought well into the 19th century. Despite the later criticism of his methods, Rush’s dedication to medical ethics, mental health, and public service earned him enduring recognition. He was the first to advocate for humane treatment of the mentally ill, laying the foundation for modern psychiatry in the United States.
When Abram Still began practicing medicine, Rush’s heroic therapy was at its peak, but it was not at all popular with every doctor or patient. Calomel, in particular, was ridiculed in popular songs and poems. A touring group in the 1840s, the Hutchisons Chanteurs, discovered that the song “Anti-Calomel” was their most requested number.
And when I have to take my last breath, pray that I die a natural death. And say goodbye to the world forever, without a single dose of Cal-O-Mell.
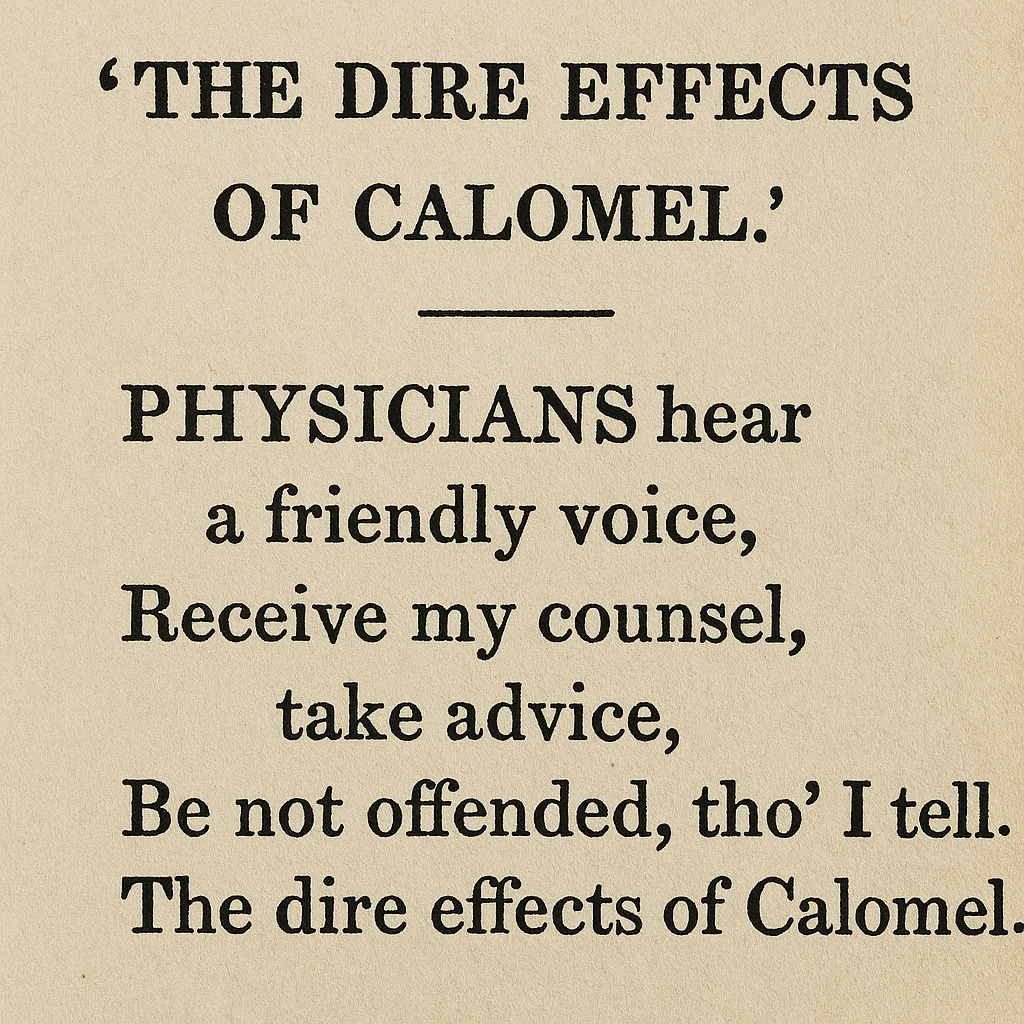
This rare poetic excerpt captures the rising skepticism of early 19th-century practitioners and laypeople toward one of the most aggressively used substances in American medicine: calomel (mercurous chloride). Once a staple of heroic medicine, calomel was praised for its ability to purge the body—through vomiting, diarrhea, and excessive salivation—of what was thought to be “toxic humors.” The verse, addressed to physicians with a tone both respectful and cautionary, illustrates the mounting resistance to such brutal methods.
The lines:
“Physicians hear a friendly voice,
Receive my counsel, take advice,
Be not offended, tho’ I tell,
The dire effects of Calomel.”
serve not only as satire but as historical witness to the turning tide in medical thought.
This kind of folk commentary, often published in broadsides or shared orally, reflected a broader cultural shift toward more conservative and observational forms of medicine. It also prefigures the advent of holistic and patient-centered approaches—like osteopathy, which would emerge later in the century as a response to the harms of over-medicalization.
This image stands as a window into the anxieties, voices, and changing values that shaped the evolution of medical practice in America.
The dire effects of calomel included the symptoms of mercury poisoning: a gray appearance of the tongue and pharynx, excessive salivation, ulcerated lips, cheeks, and tongues, stomach pain often accompanied by bloody diarrhea, and tooth loss.

In addition to calomel, other toxic pharmaceuticals such as arsenic, antimony, tartar emetic, lobelia, strychnine, and belladonna were commonly used. Only a few useful agents, such as quinine for malaria, colchicine for gout, opium for pain, and digitalis for dropsy, were available. However, these were often used for a variety of ailments beyond their original purposes.
After marrying and starting his own family, Andrew chose to join his parents at the Wakarusa Mission in Kansas Territory. It was here that he began to lay the foundation for his future career in medicine. The decision to pursue medicine may have stemmed from a desire to remedy the physical ailments and suffering he witnessed among settlers in the Kansas Territory, where access to medical care was often limited.
Andrew’s early exposure to the challenges faced by settlers on the frontier undoubtedly influenced his decision to pursue a career in medicine. Difficult living conditions, coupled with a lack of adequate medical services, likely fueled his desire to make a significant difference in the lives of others through the practice of medicine. This marked the beginning of Andrew Taylor Still’s journey to becoming a pioneer in the field of osteopathy, a path that would ultimately revolutionize the practice of medicine and health care.
Joining his parents at the Wakarusa Mission and opting for a career in medicine, Andrew Taylor Still embarked on a path that would deviate from his family’s tradition of religious service. However, his education instilled in him values of compassion, service, and commitment to improving the lives of others – principles that would become fundamental to his groundbreaking work in osteopathy.
Initial Reactions to Osteopathy: Challenges and Triumphs
When Andrew Taylor Still announced his revolutionary system of healthcare in 1874, the response from the medical community was anything but welcoming. Still’s holistic philosophy and rejection of conventional practices clashed with the entrenched norms of 19th-century medicine. Osteopathy, rooted in the interrelationship between structure and function and the body’s ability to self-heal, was seen as unorthodox, even dangerous, by many practitioners of the time. Despite initial skepticism, Still’s determination and the success of his methods gradually carved a path toward recognition.
Skepticism from the Medical Community
The prevailing medical landscape of the mid-19th century was dominated by “heroic medicine,” which relied heavily on bloodletting, purging, and the administration of toxic substances like calomel (mercuric chloride). While these methods often caused more harm than good, they were widely accepted as standard practice. Still’s outright rejection of pharmaceuticals and invasive treatments challenged this status quo. Instead of accepting his ideas as innovative, many of his contemporaries viewed them as a direct affront to established medical science.
Doctors labeled Still a charlatan, accusing him of promoting a simplistic and unfounded approach to health. Medical societies dismissed osteopathy as pseudoscience, arguing that its emphasis on manual manipulation lacked empirical support. Still’s emphasis on the body’s ability to heal itself was particularly controversial, as it diverged from the prevailing belief that external interventions, often aggressive, were necessary to cure disease. This skepticism was compounded by Still’s lack of formal medical education from a recognized institution, which further fueled doubts about his credibility.
Personal and Professional Challenges
The criticism from the medical establishment was not limited to words. Still faced tangible consequences, including ostracism from his community. He was expelled from the Methodist Church, where he had been a respected member, after some clergy labeled his hands-on techniques as sacrilegious or akin to faith healing. Friends and colleagues distanced themselves, and his family’s reputation suffered as a result of his unorthodox beliefs.
Financial hardships added to the pressure. With few patients willing to trust his methods in the early years, Still struggled to make ends meet. He was forced to move repeatedly, searching for communities where his ideas might gain traction. In one instance, he set up practice in Macon, Missouri, only to find little acceptance. Eventually, he relocated to Kirksville, Missouri, where his persistence began to yield results.
Resistance from Traditional Medical Institutions
Still’s challenges were not merely social but institutional. Many state medical boards, controlled by allopathic (conventional) physicians, sought to restrict the practice of osteopathy. Licensing laws were crafted to exclude practitioners who did not adhere to allopathic principles, effectively criminalizing Still’s work. Osteopathy was often grouped with unregulated and dubious healing practices, making it difficult for Still and his followers to gain legitimacy.
Still’s attempts to teach his methods also faced resistance. When he approached Baker University, a local institution he had helped establish, to offer a lecture on osteopathy, he was denied. This rejection underscored the uphill battle he faced in gaining academic and institutional support for his philosophy.
Public Perception and Gradual Acceptance
Despite resistance from the medical elite, osteopathy began to attract attention from the public, particularly those disillusioned with the harsh and often ineffective treatments of conventional medicine. Patients who had exhausted traditional options and continued to suffer from chronic pain, digestive disorders, or other ailments turned to Still as a last resort. His success in alleviating their symptoms sparked word-of-mouth endorsements, gradually building a loyal patient base.
One particularly influential case involved the daughter of a local pastor in Kirksville, who suffered from a debilitating condition that had resisted traditional treatment. After receiving osteopathic care from Still, her dramatic recovery earned him the respect of the local community and increased his patient load. These successes also helped break down social barriers, with even the more skeptical residents of Kirksville eventually seeking his care.
Still’s Response to Criticism
Still was unyielding in the face of criticism. Rather than retreating, he doubled down on his commitment to scientific rigor and education. He emphasized the anatomical foundations of osteopathy, often dissecting cadavers to deepen his understanding of the human body and to demonstrate the validity of his approach. He believed that proving his methods through results would ultimately win over skeptics.
Still also sought to differentiate osteopathy from other alternative practices of the time, such as magnetic healing or spiritualist movements, which were often dismissed as superstitious or fraudulent. By grounding osteopathy in anatomy and physiology, he worked to establish it as a legitimate medical discipline rather than a fringe therapy.
The Turning Point
The founding of the American School of Osteopathy (ASO) in 1892 marked a pivotal moment in Still’s journey. The school provided a platform for formalizing his teachings and training a new generation of practitioners. The success of ASO graduates, many of whom went on to establish their own practices and schools, lent credibility to osteopathy and began to shift public and professional opinion.
Legacy of Early Struggles
Still’s perseverance in the face of skepticism laid the groundwork for the eventual acceptance of osteopathy as a respected medical discipline. By the early 20th century, osteopathy had gained legal recognition in several states, and its emphasis on holistic, patient-centered care resonated with a growing number of patients and practitioners. The initial resistance from the medical community, while daunting, ultimately strengthened osteopathy’s foundation as a science-based alternative to conventional medicine.
Andrew Taylor Still’s Personal Struggles and Inspirations
Amid his growing skepticism of conventional medicine, Andrew Taylor Still faced personal tragedies that profoundly shaped his philosophy and ultimate creation of osteopathy. In 1864, Still endured one of the darkest chapters of his life when three of his children succumbed to spinal meningitis, a devastating disease for which 19th-century medicine offered little effective treatment. Shortly afterward, he lost his wife, adding to his immense grief.

These losses deepened Still’s dissatisfaction with the prevailing medical practices of his time, including the heavy reliance on calomel (a mercury-based compound) and aggressive interventions like bloodletting. He began to question the efficacy and safety of these approaches, which often caused more harm than healing.
Fueled by his heartbreak and frustration, Still sought a better way to understand and treat the human body. He immersed himself in anatomy, physiology, and mechanical principles, drawing inspiration from the natural sciences and his father’s teachings as both a physician and a minister. He became convinced that health depended on the body’s structural integrity and its ability to function without interference—a philosophy that would later underpin osteopathy.
Still’s personal struggles catalyzed his rejection of traditional medicine and spurred him to pioneer a holistic approach to healthcare. His belief that the body contained an innate ability to heal itself resonated deeply with his desire to prevent others from suffering the same losses he had endured.
This period of mourning and reflection not only marked a turning point in Still’s life but also laid the groundwork for the revolutionary medical system that would transform modern healthcare.
Andrew Taylor Still’s Personal Struggles and Inspirations
Amid his growing skepticism of conventional medicine, Andrew Taylor Still faced personal tragedies that profoundly shaped his philosophy and ultimate creation of osteopathy. In 1864, Still endured one of the darkest chapters of his life when three of his children succumbed to spinal meningitis, a devastating disease for which 19th-century medicine offered little effective treatment. Shortly afterward, he lost his wife, adding to his immense grief.
These losses deepened Still’s dissatisfaction with the prevailing medical practices of his time, including the heavy reliance on calomel (a mercury-based compound) and aggressive interventions like bloodletting. He began to question the efficacy and safety of these approaches, which often caused more harm than healing.
Fueled by his heartbreak and frustration, Still sought a better way to understand and treat the human body. He immersed himself in anatomy, physiology, and mechanical principles, drawing inspiration from the natural sciences and his father’s teachings as both a physician and a minister. He became convinced that health depended on the body’s structural integrity and its ability to function without interference—a philosophy that would later underpin osteopathy.
Still’s personal struggles catalyzed his rejection of traditional medicine and spurred him to pioneer a holistic approach to healthcare. His belief that the body contained an innate ability to heal itself resonated deeply with his desire to prevent others from suffering the same losses he had endured.
This period of mourning and reflection not only marked a turning point in Still’s life but also laid the groundwork for the revolutionary medical system that would transform modern healthcare.
Detailed Exploration of Still’s Philosophy
Andrew Taylor Still, the founder of osteopathy, revolutionized medicine by emphasizing a holistic and integrative approach to health. His philosophy emerged from deep reflection on human anatomy, physiology, and the limitations of conventional medicine during his time. Central to Still’s principles were the ideas of structural integrity, the interdependence of structure and function, and the body’s innate ability to self-heal. These core beliefs would form the foundation of osteopathy and distinguish it from other medical systems of the 19th century.
The Body as an Integrated Whole
One of Still’s most fundamental principles was that the body operates as an interconnected unit. He rejected the compartmentalized approach of traditional medicine, which often treated diseases as isolated phenomena. Instead, Still believed that every part of the body contributes to the health and function of the whole. This holistic perspective was shaped by his early medical experiences, particularly during his work in the Kansas Territory, where he witnessed settlers battling illnesses without adequate medical care.
Still often used the metaphor of a finely tuned machine to explain his philosophy. Just as a malfunction in one component of a machine can disrupt the entire system, he argued that dysfunction in one area of the body could ripple through the body’s interconnected systems, causing illness. For Still, treating only the symptoms of disease ignored the deeper structural and functional relationships that underlie health.
Structure and Function: A Dynamic Relationship
Still’s second guiding principle was the interdependence of structure and function. He observed that the alignment and mobility of the musculoskeletal system directly influenced the function of other bodily systems, such as the circulatory, nervous, and lymphatic systems. This insight emerged early in his career, informed by his detailed study of human anatomy.
An anecdote from Still’s practice illustrates this concept vividly. He treated a young woman who had been suffering from debilitating headaches for years. Rather than prescribing the medications typical of the time, Still conducted a thorough examination of her spine. He discovered that a slight misalignment in her cervical vertebrae was compressing a nerve. By carefully adjusting her spine, he restored proper nerve function, alleviating her headaches. This experience reinforced his belief that structural issues could manifest as functional disorders, and correcting these structural problems was key to restoring health.
The Self-Healing Capacity of the Body
Still’s philosophy also emphasized the body’s inherent ability to heal itself. He viewed the human body as a self-regulating organism, equipped with the mechanisms to maintain health when its systems were free from obstruction. This belief stemmed from his frustration with conventional medical practices, such as bloodletting and the use of toxic pharmaceuticals like calomel, which often caused more harm than good.
Still believed that the role of the physician was not to impose health through aggressive interventions but to facilitate the body’s natural healing processes. He famously declared, “Find it, fix it, and leave it alone,” underscoring his commitment to minimal intervention. His focus on enabling the body’s self-healing capacity resonated with patients who were disillusioned by the harsh treatments of traditional medicine.
Practical Applications in Early Practice
Still’s hands-on approach to healthcare was grounded in his deep understanding of anatomy and physiology. He developed techniques to diagnose and correct structural misalignments, which he believed were the root causes of many diseases. These techniques became the foundation of osteopathic manipulative treatment (OMT).
In another example from his early practice, Still treated a farmer who had been suffering from chronic back pain and digestive issues. Through careful palpation, Still identified tension and misalignment in the man’s lumbar spine. He performed a series of adjustments to realign the vertebrae and restore mobility. Over the following weeks, the farmer not only experienced relief from his back pain but also noticed significant improvement in his digestion. For Still, this case exemplified the interconnectedness of structure and function and the body’s capacity for self-repair when its systems were properly aligned.
Rejecting the Status Quo
Still’s approach stood in stark contrast to the prevailing medical practices of his time, which often treated symptoms in isolation and relied heavily on drugs and surgical interventions. He was vocal in his criticism of these methods, calling them “heroic medicine” and arguing that they ignored the body’s natural processes. Instead, he championed a system that prioritized the patient as a whole, emphasizing prevention and maintenance of health rather than simply treating disease.
Inspiration from Nature and Mechanics
Still’s philosophy was also shaped by his observations of nature and his background in mechanics. Growing up on the frontier, he witnessed how ecosystems thrived when in balance and faltered when disrupted. He applied this understanding to the human body, seeing it as a self-regulating ecosystem that required harmony between its parts. His early experiences repairing farm machinery further reinforced his belief that structure and function were inseparably linked.
Legacy of Still’s Philosophy
The principles that Still developed—holistic care, the interrelationship of structure and function, and the body’s self-healing ability—remain central to osteopathy today. By viewing the body as an integrated whole and focusing on its capacity for self-regulation, Still offered a revolutionary alternative to the fragmented and often harmful practices of 19th-century medicine.
His pioneering work laid the foundation for a medical discipline that continues to thrive, inspiring generations of practitioners to approach health with the same respect for the body’s complexity and resilience that he demonstrated in his early practice. Still’s philosophy, born from personal loss, meticulous observation, and a desire to alleviate suffering, has transformed the way we think about health and healing.
The Birth of Osteopathy: Andrew Taylor Still’s Revolutionary Insights
Andrew Taylor Still’s journey towards the founding principles of osteopathy was not a linear path but a culmination of experiences, observations, and critical reflections on the limitations of contemporary medical practices. It was during his early years as a physician, marked by encounters with patients and a quest for more effective treatment modalities, that Still began to formulate his groundbreaking ideas. His upbringing as the son of a Methodist preacher instilled in him a sense of compassion and service, traits that would later define his approach to healthcare.
As a young doctor practicing in the challenging frontier of the Kansas Territory, Still was confronted with the stark realities of disease, injury, and inadequate medical care. Inspired by his desire to alleviate suffering and improve the well-being of his patients, he embarked on a journey of exploration and innovation. Drawing from diverse influences, including his experiences as a circuit rider’s son, his observations of nature, and his study of human anatomy and physiology, Still developed a unique perspective on health and disease.
The pivotal moment in Still’s journey came when he experienced a profound revelation regarding the relationship between spinal alignment and overall health. In a moment of clarity, he recognized that many ailments stemmed from disturbances in the musculoskeletal system, particularly the spine, and that restoring proper alignment could facilitate the body’s innate healing abilities. This insight laid the foundation for osteopathy, a holistic approach to healthcare that prioritized the body’s self-regulating mechanisms and emphasized the interconnectedness of structure and function.

Dressed formally in this photograph, Still’s attire reflects the professional stature and respect he garnered during his lifetime. His iconic top hat and neatly groomed beard symbolize the dignity and refinement of his era. Seated with a poised demeanor, he holds a document, possibly indicative of his work in advancing osteopathic practices or the founding of the American School of Osteopathy (now A.T. Still University) in 1892.
Still’s revolutionary approach to medicine focused on holistic care, advocating for the integration of structure, function, and health—a philosophy that continues to influence modern healthcare. This portrait captures the essence of a man who not only redefined medical practice but also inspired generations of practitioners with his vision of treating the patient as a whole rather than merely addressing symptoms.
From this initial revelation, Still continued to refine and expand his understanding of osteopathic principles, incorporating elements of manual therapy, nutrition, and lifestyle modifications into his practice. Despite facing skepticism and resistance from the medical establishment, he remained steadfast in his commitment to challenging conventional wisdom and advocating for a more comprehensive approach to healthcare.
The journey of Andrew Taylor Still from traditional medicine to the foundation of osteopathy is a testament to the power of individual vision and perseverance in the face of adversity. His revolutionary insights not only transformed the practice of medicine but also paved the way for a new paradigm of healthcare focused on promoting wellness and vitality.”
Development and Evolution of Osteopathic Principles
The development of osteopathy by Andrew Taylor Still marked a paradigm shift in the approach to healthcare, one grounded in an understanding of the human body as an interconnected system with innate self-healing capabilities. Central to osteopathy are its core tenets, which Still formalized through years of observation, experimentation, and reflection.
The Core Principles of Osteopathy
- The Body as a Unit:
Still emphasized the idea that the body functions as an integrated whole. He believed that physical, emotional, and spiritual health are interconnected, and any disruption in one area could influence the entire system. This holistic perspective was revolutionary, offering an alternative to the segmented view of medicine common in the 19th century. - Structure and Function are Interrelated:
One of Still’s foundational insights was the relationship between the body’s structure (bones, muscles, tissues) and its function (circulation, nervous system activity, organ performance). He argued that misalignments or restrictions in the musculoskeletal system could obstruct the body’s ability to perform optimally, leading to disease or dysfunction. - The Body Possesses Self-Healing Mechanisms:
Perhaps the most forward-thinking principle of osteopathy is its focus on the body’s inherent capacity to heal itself. Still saw the role of a physician as facilitating this natural process rather than imposing external interventions, which he viewed as often harmful. - Preventive Care and Health Maintenance:
Unlike conventional medicine of the time, which focused on treating symptoms, Still promoted the idea of preventive care. By maintaining the body’s structural integrity and functional balance, osteopathy sought to prevent illness rather than merely cure it.
Refining Osteopathic Techniques
Still’s ideas evolved as he developed specific techniques to align with these principles. He introduced hands-on methods to diagnose and treat structural misalignments, pioneering what is now known as osteopathic manipulative treatment (OMT). These procedures emphasized gentle manipulation to restore mobility, improve circulation, and optimize nerve function, reinforcing the body’s natural healing abilities.
Integration of Science and Philosophy
Osteopathy blended scientific principles with a philosophical outlook. Still’s deep knowledge of anatomy and physiology allowed him to substantiate his theories with empirical evidence, making osteopathy more than just an abstract concept. This integration made his ideas accessible to both medical professionals and patients seeking an alternative to traditional medicine.
Legacy and Adaptation
Over time, osteopathy evolved from its original form into a more comprehensive medical discipline. While Still focused primarily on the musculoskeletal system, his successors expanded the practice to include broader diagnostic and therapeutic techniques, incorporating advancements in medical science while maintaining the core tenets. Today, osteopathy stands as a testament to Still’s enduring vision of holistic healthcare.
The evolution of these principles underscores the ingenuity of Still’s approach, bridging the gap between traditional and modern medicine. By emphasizing the unity of structure and function, osteopathy remains a unique and influential branch of healthcare, promoting well-being through both science and philosophy.
American Medicine in the Mid-19th Century: A Crucial Transition to Modernity
In the mid-19th century, American medicine faced many challenges, characterized by poorly trained practitioners and the application of harsh therapeutic methods. This era was marked by a lack of formal education among doctors, with most pursuing apprenticeships or practicing without any structured background in medicine. The apprenticeship system, typically lasting three years or more, provided a pragmatic but inconsistent education. Preceptor qualifications varied, leading to disparities in the quality of teaching. The popularity of this system stemmed from its economic advantages for teachers and the affordable labor it provided for students, who thus acquired the knowledge necessary to meet public expectations.
With the emergence of medical colleges, the goal was to supplement the training of practitioners with formal lectures and demonstrations. However, the quality of education at these institutions was questionable, driven by financial interests rather than a commitment to comprehensive learning. AT Still, beginning his medical career in 1854, initially acquired his medical knowledge through practical experience alongside his father and self-study.
Medical thought and practice during this period was highly speculative and empirical. Benjamin Rush, a leading figure of the era, believed in physiological tension as the basis of all disease, advocating bloodletting as an effective treatment. This practice has become widespread, even for acute illnesses, with some practitioners recommending bleeding patients into unconsciousness. The popularity of such practices persisted until the 1850s, despite the disqualification of Rush’s theories.

Benjamin Rush was a prominent American physician, politician, and social reformer, who played a pivotal role in the early development of American medicine and politics. Known as one of the Founding Fathers of the United States, Rush was a signatory of the Declaration of Independence and served as a surgeon general in the Continental Army during the American Revolutionary War. Beyond his political contributions, Rush is celebrated for his advancements in medical practice and education, often referred to as the “Father of American Psychiatry” for his pioneering work in mental health care. His approach emphasized humane treatment and the understanding of mental illnesses as medical conditions rather than moral failings. As a passionate advocate for public health, he also supported vaccination, promoted the abolition of slavery, and championed education reform. This portrait captures Rush’s intellectual curiosity and dedication to improving society through science and medicine, highlighting his lasting influence on both the medical and political landscape of his time.
Another frequently used remedy was calomel, a mercury compound known for its powerful cathartic effects. However, its use was accompanied by serious side effects, including stomatitis, excessive salivation, ulcerated lips, and even death. A.T. Still himself suffered the consequences, using a partial set of dentures due to loosening of his teeth from mercury salivation.
In addition to calomel, other toxic pharmaceuticals such as arsenic, antimony, tartar emetic, lobelia, strychnine, and belladonna were commonly used. Only a few useful agents, such as quinine for malaria, colchicine for gout, opium for pain, and digitalis for dropsy, were available. However, these were often used for a variety of ailments beyond their original purposes.
Despite these challenges, not all orthodox physicians adhered to symptomatic management. Jacob Bigelow, as early as 1835, introduced the concept of “self-limiting diseases”, emphasizing that some diseases had inherent limits in their progression. He argued that drastic or heroic measures did not significantly improve patients’ chances of recovery. However, the medical community, as a whole, continued to employ depleting measures.

Medical Revolution in the 19th Century: Holmes and Semmelweis, Pioneers of Infection Control
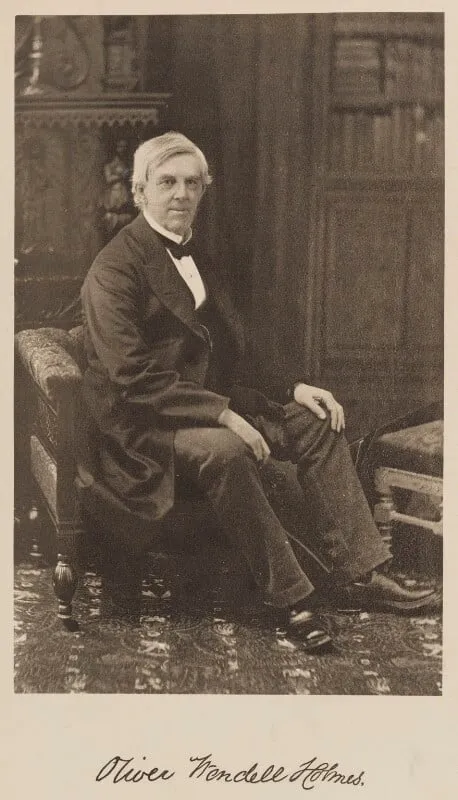
In 1860, Oliver Wendell Holmes, Sr., expressed frustration with prevalent medical practices, claiming that sinking all materia medica to the bottom of the sea would be better for humanity. Despite such criticism, the medical community resisted significant change, with doctors feeling compelled to act rather than passively observe, aligned with the expectations of their patients.
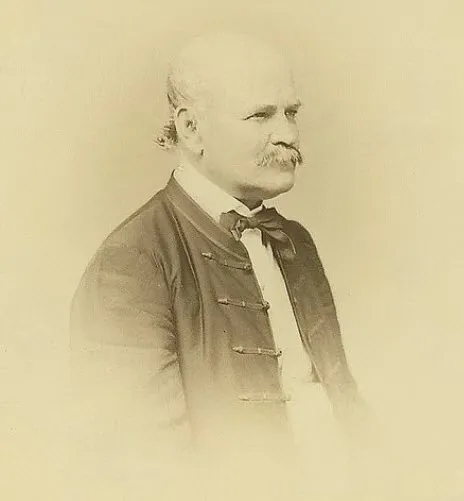
By the mid-19th century, maternal mortality rates in European and American maternity wards were significantly higher than in those attended by midwives or for home births, mainly due to puerperal fever. Doctors, often performing autopsies on dead women without protective gear, were unknowingly spreading deadly bacteria to expectant mothers.
Oliver Wendell Holmes Sr. (1809-1894), an American physician, poet, and author, played a crucial role in solving this problem. Studying in Paris, he learned statistical analysis to challenge ineffective medical practices. In 1846 he coined the term “anesthesia” and in 1860 criticized the predominant drugs.
Holmes focused on puerperal fever after a lecture in 1842. Although his 1843 research into the contagiousness of puerperal fever initially went unnoticed, it gained attention in 1855. Holmes suggested burning clothing and instruments contaminated and to abstain from obstetrical practice for six months.
His study, similar to the work of Semmelweis, preceded germ theory. Despite the skepticism encountered, Holmes made a significant contribution to the understanding of contagious infections. Although debates persist over credit, both Semmelweis and Holmes deserve credit for advocating handwashing, a universal practice for infection control, including in the fight against COVID-19.
In Kansas’ early history, malaria and smallpox were the leading causes of adult mortality. Quinine, known for its effectiveness against malaria, was expensive and difficult to obtain, contributing to the challenges faced by early settlers. Additionally, diseases such as typhoid fever, pneumonia, scarlet fever, typhus, dysentery, and meningitis had no effective therapies, further complicating medical practice.
AT Still, although he initially used generally accepted medications in his practice, began to question regular medicine more seriously after a personal tragedy involving spinal meningitis in his family. This event inspired him to explore alternative systems of practice, marking the beginning of a transformative journey in his approach to medicine. As he reflected on this pivotal moment, he compared himself to Columbus, trimming his sail and launching his craft as an explorer into uncharted territories of medical knowledge.
An Era of Non-Drug Medicines: The Emergence of Alternative Systems
“The Lightning Bonesetter,” chronicles the evolution of Dr. Andrew Still, who in the 1870s became deeply involved in bonebreaking, a generally manipulative practice. related to orthopedics. By exploring these innovative techniques, he harbored ambitions to expand the range of disorders he could treat, paving the way for a significant expansion of his clientele and revenue.
These scavengers were an ancient, if sometimes despised, group of healers. In England, they enjoyed relatively free practice among the working classes, unable to pay a regular doctor and often struggling to find one willing to treat them. These harvesters could also count on the patronage of the upper classes, including royalty. Their special talent was widely believed to be passed down from generation to generation within a family, thus constituting a gift transcending formal learning.
In addition to reducing dislocations, they also manipulated painful and diseased joints, believing that these conditions were also caused by a “displaced bone.” Doctors ridiculed their crude diagnoses and rejected their assertion that such treatment had any value. However, some patients with restricted joint mobility, unrelieved after treatment by qualified orthopedists, appeared to benefit from the manipulative therapy administered by these “quacks.”
In 1867, the eminent surgeon Sir James Paget aroused the astonishment of his peers by making a bold claim: he firmly believed that bone reducers held the power to cure certain joint conditions, regardless of the often imprecise diagnoses of the time.
This groundbreaking statement laid the foundation for a new perspective on healthcare, challenging established paradigms and paving the way for further exploration of the possibilities offered by bone reduction techniques. The idea that practitioners could directly influence the treatment of joint disorders, despite the diagnostic limitations of the time, sparked a lively debate among the medical community of the time, opening the door to future developments in the field. field of medicine and bone manipulation.
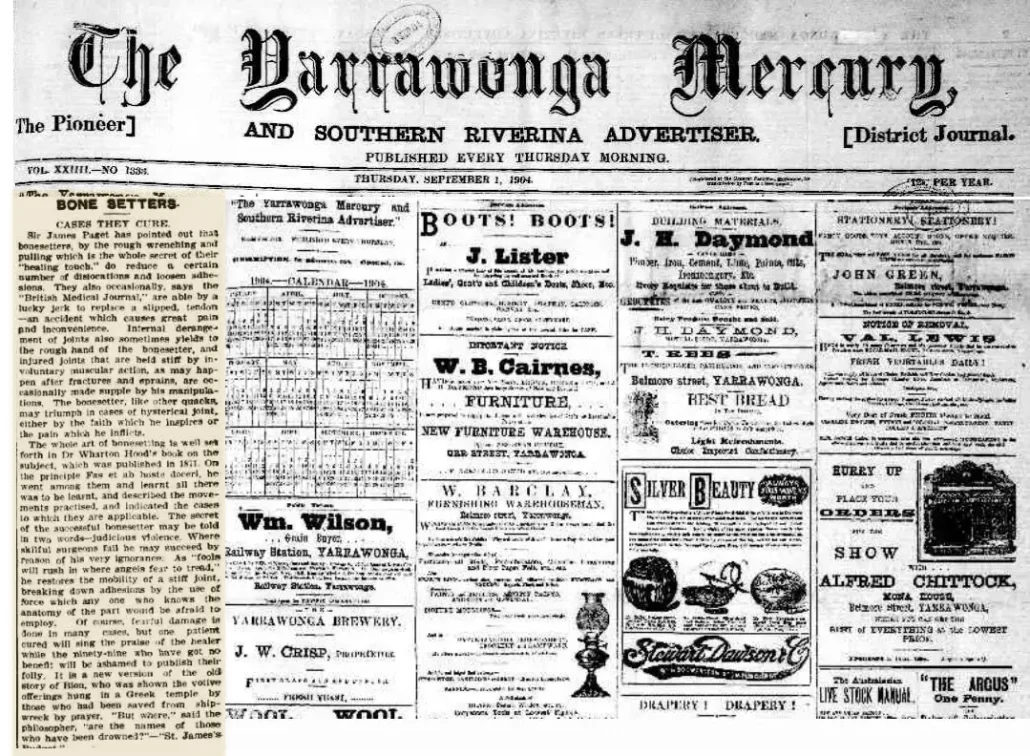
THE CASES THEY HEAL
Sir James Paget pointed out that bone adjusters, through the brutal manipulation and traction which constitute the whole secret of their “healing touch”, manage to reduce a certain number of dislocations and to relax adhesions . From time to time, according to the “British Medical Journal”, they also manage, by a stroke of luck, to put a slipped tendon back into place, an accident causing great pain and inconvenience. Internal derangements of the joints also sometimes yield to the rough hand of the bone fitter, and injured joints held stiff by involuntary muscular action, as may happen after fractures and sprains, occasionally become supple through his manipulations . The bone adjuster, like other charlatans, can triumph in cases of hysterical joints, either by the faith he inspires, or by the pain he inflicts.
The whole art of bone adjustment is well set forth in Dr. Wharton Hood’s book on the subject, published in 1871. On the principle “Fas et ab hoste doceri” (It is permissible to learn even from the enemy), he went among them, learned everything and described the movements practiced, indicating the cases to which they apply. The secret to the Bone Fitter’s success can be summed up in two words: judicious violence. Where skillful surgeons fail, he may succeed even because of his ignorance. As “fools rush where angels fear to tread,” he restores mobility to a stiff joint, breaking adhesions with forces that anyone familiar with the anatomy of the part would fear to employ. Of course, fearful damage is done in many cases, but a cured patient will sing the healer’s praises while the ninety-nine who have had no benefit will be ashamed to publish their folly. This is a new version of the old story of Bion, who was shown the votive offerings hanging in a Greek temple by those who had been saved from shipwreck through prayer. “But where are the names of those who were drowned? » asked the philosopher. “ St James’s Budget ”.
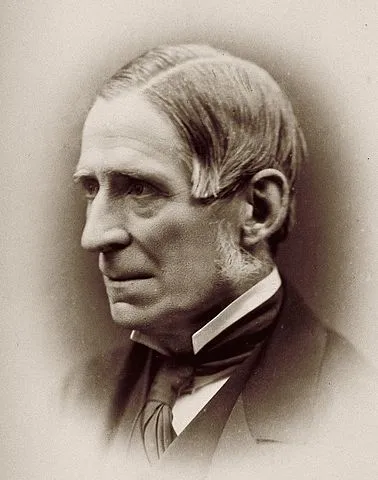
Dr Wharton P Hood makes sense of Bonesetters
In 1871, Dr. Wharton Hood, a friend of Paget’s, published a book based on his experiences as an apprentice bonesetter.
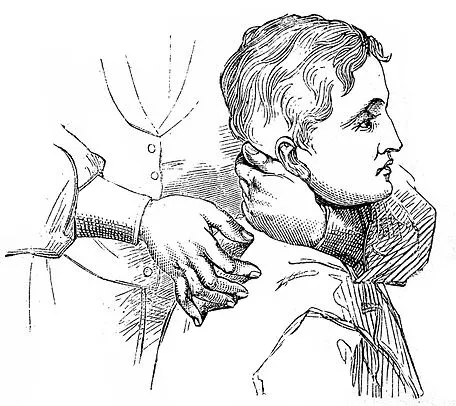
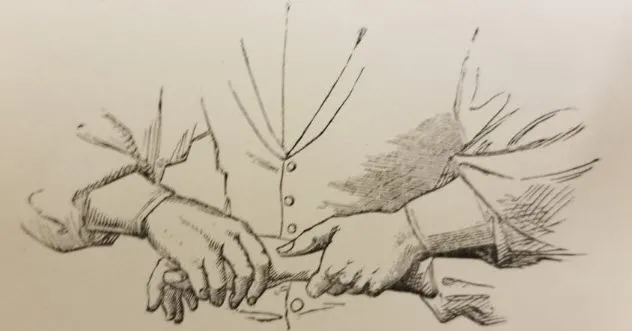
He described the technique of these bone-setters as:
“ To resist alternately flexion and extension is the pons asinorum of manipulators, and, in considerable experience of teaching massage, I found that few people could learn to do it. Its importance cannot be overstated as a means of cultivating strength in weakened muscles, whilst at the same time discovering the extent to which they can be used. Many patients who have recovered from an old injury remain as incapacitated as before, because their latent energies can only be discovered and put to use in this way. Halfway between passive and resistive movements, in the context of certain recoveries, are assistance movements. They are little understood and rarely used. They can be illustrated as follows: Suppose that, in the absence of adhesions and irreparable damage to the nerve centers, the deltoid has only half the strength necessary to raise the arm. As far as any utility goes, it’s as if there is no contraction capacity left in the muscle. But if only the other half of the weakened vigor is supplemented by the carefully graded assistance of the operator, the required movement will occur; and, in some cases, if this is regularly continued, with manipulation and percussion, a more vigorous contraction will be obtained, and, little by little, the patient will exert three-fourths of the necessary force, and later, the whole movement will be done without help; and, as the force increases, resistance may be presented to the movement. Partial loss of motion can often be accurately estimated by holding the limb suspended in tissue attached to a spring. When the patient makes an effort, the limb weighs less. By means of a spring, the resistive movement can also be estimated. Another type of movement can also be discussed, namely vigorous passive movement, with the aim of breaking up adhesions in and around the joints, a description which is beyond the scope of this article. This is the secret of the success and failure of those who call themselves bone-setters, whose methods have been well studied and explained by Dr. Wharton P. Hood, of London, in his very interesting book “On Bone-Setting, so called “. »
Dr. Hood aims to shed light on the principles behind the practice, addressing common misconceptions and the medical community’s skepticism toward bone-setting. The book serves as a bridge between traditional practices and emerging modern orthopedic approaches, providing valuable insights into joint rehabilitation and manipulation techniques of the time.
This publication reflects the 19th-century medical landscape, where traditional and scientific practices often intersected, offering readers a nuanced understanding of bone-setting as a therapeutic intervention. It remains a notable work for its attempt to merge empirical observations with contemporary medical knowledge.
Wharton P. Hood, in his extensive studies, had a strong belief in the effectiveness of the method he advocated for treating a diverse range of musculoskeletal problems. He said this approach was particularly beneficial in treating stiffness, pain and adhesion resulting from fractures and sprains. These conditions, often associated with reduced mobility and feelings of discomfort, seemed to find a positive response to the method advocated by Hood.

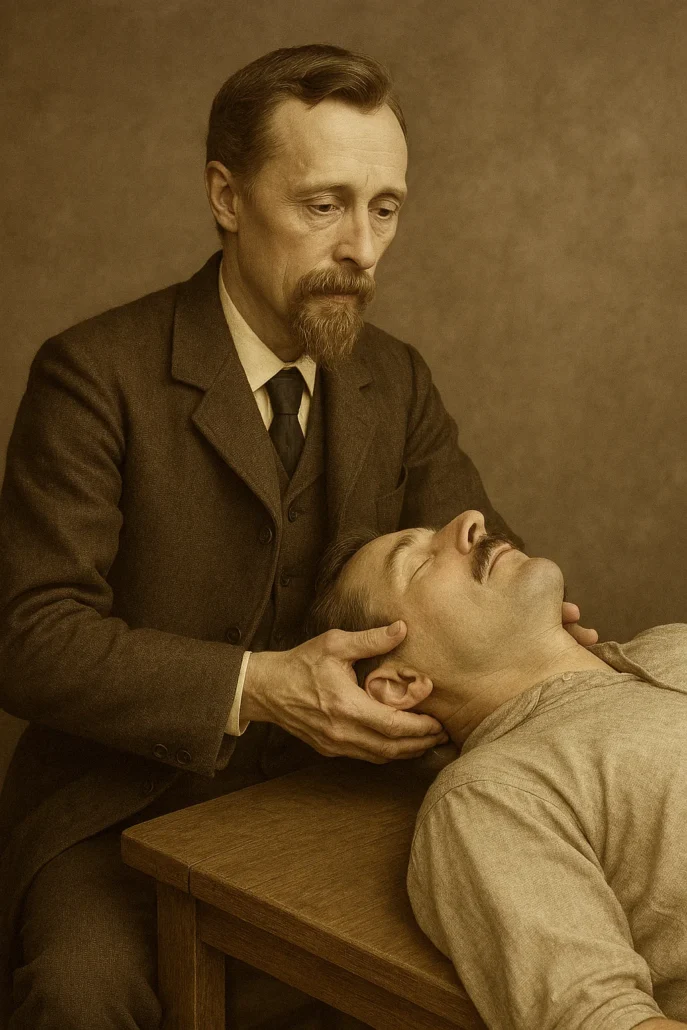
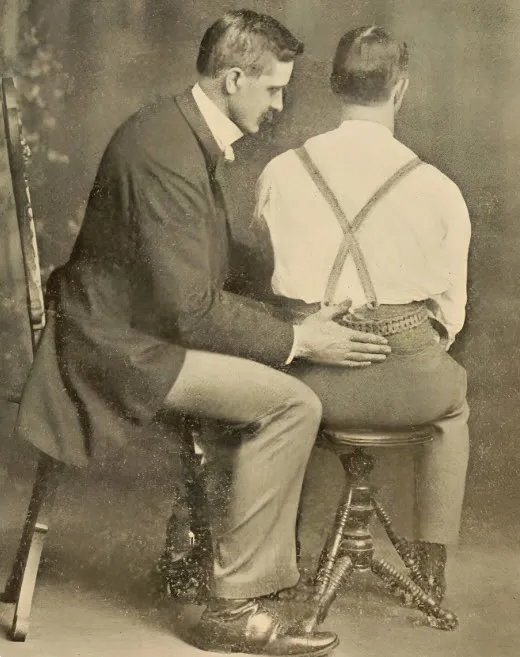
Dr. Wharton Hood, a prominent figure in the field of manual medicine during the 19th century, is seen here performing a physical examination on a patient. Known for his innovative approaches, Dr. Hood emphasized the importance of hands-on treatment, laying the groundwork for future developments in physical and osteopathic therapies. His work contributed to the growing recognition of manual therapy as a legitimate form of medical treatment.
Additionally, Hood considered this method an effective way to treat joint problems, such as rheumatic or gouty joints. These conditions, characterized by inflammation and joint pain, were targeted by the specific manipulation and technique he advocated. Likewise, displaced cartilage, subluxations of the carpal and tarsal bones were also listed as conditions that could benefit from this approach.
Displaced tendons, a problem that can cause loss of function and considerable discomfort, were also among the areas where Hood was seeing positive results with his method. Likewise, hysterical joints, characterized by varied and often complex symptoms, were considered responsive to this treatment technique.
Expanding its scope further, Hood identified lymph node swellings as another area where this method could provide benefit. The ability of this approach to treat such varied conditions demonstrated, in his opinion, notable versatility in the treatment of musculoskeletal and joint disorders.
This expanded perspective on the applications of Hood’s method suggests that his in-depth understanding of musculoskeletal mechanisms allowed him to develop a holistic approach to addressing various problems. His contribution to this field, as outlined in his book “On Bone-Setting, so called”, continues to be studied and considered in the context of evolving musculoskeletal medicine and treatment practices.
However, Hood cautioned against bone-setters being successful only when the joints’ ability to pivot had not already been irreparably destroyed.
He observed that most bonesetters focused on manipulating the extremities, but also treated people complaining of back pain, cured by flexion and extension movements with pressure on painful points, often accompanied by sounds of ” clicking sound” emitted by the joints of the spine.
The article highlights the presence of bone-setters in the United States since colonial times, citing the Sweet family as the most prominent practitioners in New England. However, the spread of these manipulators across the country remains unclear. The author speculates on how Still became the “lightning healer” in the 1880s, suggesting that he may have learned from another practitioner’s observations.
Wharton Hood Method
Wharton P. Hood was a renowned practitioner who specialized in a treatment method called bone-setting. Although the precise details of his method may vary, particularly in the context of his writings and training, the general approach involved manual manipulations aimed at restoring the alignment of bones and joints. Here is a general view of certain aspects of his method:
- Joint manipulations: Hood’s method focused on the manual manipulation of joints and bones. He believed in the importance of restoring natural alignment to improve function and reduce pain.
- Treatment of Fractures and Sprains: Hood paid particular attention to the treatment of fractures and sprains, with emphasis on restoring mobility and normal function while minimizing associated stiffness and pain.
- Treatment of rheumatic and gouty conditions: Hood’s method was also intended to relieve the symptoms of rheumatic and gouty conditions. The manipulations were aimed at reducing inflammation and improving mobility in the affected joints.
- Correction of Displaced Cartilage and Subluxations: For cases of displaced cartilage and subluxations of the carpal and tarsal bones, Hood advocated specific manipulations to restore proper alignment.
- Treatment of Displaced Tendons: Manipulations were used to treat displaced tendons, thereby restoring normal muscle function and improving mobility.
- Assistive approach: Hood also explored assistive movements, where the practitioner helped the patient perform movements to gradually strengthen weakened muscles while promoting recovery.
Wharton Hood Was an Important Figure in the Advancement of Osteopathy
Wharton P. Hood has emerged as a significant figure in the advancement of osteopathy because of his essential contributions to the understanding and promotion of musculoskeletal treatment methods. His fame stems mainly from his expertise in the field of “bone-setting”, a practice which has helped to shape the evolution of osteopathy.
One of the key reasons for Hood’s importance is his ability to systematize and explain the fundamental principles of bone marrow. His book entitled “ On Bone-Setting, so called ” played a crucial role in documenting his observations, methods and clinical results. This work has contributed to establishing a theoretical and practical basis for bone marrow, thus offering practitioners and researchers new perspectives on the treatment of musculoskeletal disorders.
Hood was also a pioneer in recognizing the diversity of conditions that could benefit from bone marrow. By highlighting its effectiveness in treating problems ranging from post-fracture stiffness to rheumatic conditions, from displaced cartilage to displaced tendons, it has broadened the scope of osteopathy. This holistic approach helped establish the idea that musculoskeletal dysfunctions could be addressed in an integrated manner, considering the entire system rather than isolated symptoms.
Additionally, Hood played a crucial role in disseminating and promoting the principles of bone marrow. His influence helped bring attention to the practice and increased interest among health practitioners. This has contributed to the progressive integration of bone marrow into the broader spectrum of osteopathy, thus contributing to enrich and diversify the available therapeutic approaches.
As an experienced practitioner and keen observer, Hood also made valuable contributions to the understanding of human anatomy and physiology, particularly in the context of bone movement and alignment. His observations were a pillar for future generations of osteopaths, providing important practical and theoretical perspectives in the development of this discipline.
Thus, Wharton P. Hood played a crucial role in the advancement of osteopathy by consolidating bone marrow as a viable therapeutic method, broadening its scope of application, and sharing his knowledge through his work. His contribution continues to influence the practice of osteopathy and remains an integral part of the history of this medical discipline.
1880: Still’s Revelation – Flexion and Extension Procedures Redefine Musculoskeletal Treatments
Still’s key revelation came around 1880 when he discovered that sudden flexion and extension procedures were not limited to orthopedic problems, providing a more reliable means of healing than simple spinal massage. It tells the story of an Irish lady suffering from asthma, successfully treated by adjusting her spine and some ribs, which inspired her to expand her treatments to various ailments such as headaches, heart disease , facial and arm paralysis, lower back pain, sciatica, rheumatism, varicose veins, and many others by manipulating the vertebrae into their “correct position”. Still merges elements of magnetic healing and bone reduction into a unified doctrine, attributing the effects of disease to fluid obstruction or imbalance, caused by misplaced bones, particularly of the spine, interfering with nerve supply regulating blood circulation.
Over the next decade, Still traveled throughout Missouri promoting his new approach, performing public demonstrations of hip reduction, attracting local attention and generating excitement. Despite his difficulties in communicating his ideas, with speeches saturated with disconcerting metaphors and an atypical appearance, his reputation grew. Paradoxically, it was after having acquired notoriety elsewhere that the inhabitants of Kirksville began to frequent it in large numbers. One particular incident, where he successfully treated the town pastor’s daughter, helped change his image and lower the social barriers that prevented him from treating “respectable people”. Convinced of his discovery of a new science of healing, Still decided to make Kirksville his permanent base and established an infirmary in 1889. Patients flocking from far and wide enhanced his reputation and fame, convincing him that he had created a new science. However, it still lacks a suitable name. When thinking about terms such as allopathy,
Alternative Medical Systems
Several very different medical movements emerged in America beginning in the 19th century. The first significant threat to orthodox medicine in America was led by Samuel Thomson (1769-1843), a crude, self-educated individual who posited that all disease was due to the body’s inability to maintain its natural heat. As therapy, he rejected bloodletting and calomel, instead using herbal remedies that caused sweating and vomiting. Thomson questioned the legitimacy and integrity of the medical profession on several counts, arguing that orthodox doctors were often motivated by a desire to obtain higher fees by prolonging illness. He also challenged the idea that formal education was an unnecessary prerequisite for medical practice and criticized licensing laws meant to protect the public from “charlatans”, seeing them as a means of monopolizing the healing arts. Although ridiculed by orthodox physicians, Thomson’s criticisms resonated with many Americans in Jackson’s era, when the virtues of the common man were exalted and the granting of special privileges was frowned upon.
This image showcases the title page of Samuel Thomson’s influential 1822 publication, A Narrative of the Life and Medical Discoveries of Samuel Thomson. Thomson, a self-taught herbalist and botanist, revolutionized the 19th-century American medical landscape with his system of botanical medicine, known as “Thomsonian Medicine.” The book details Thomson’s journey and the development of his unique approach to healthcare, which focused on the use of plant-based treatments and steam baths to restore the body’s natural balance and promote healing. By challenging the practices of conventional medicine of his time, Thomson empowered individuals to take control of their own health through natural remedies and self-treatment, democratizing medical knowledge in a way that paved the way for alternative medicine in America. His work was both controversial and popular, leaving a lasting impact on the medical community and contributing to the rise of the herbal medicine movement.
Subimage Caption:
Title page of Samuel Thomson’s 1822 book, “A Narrative of the Life and Medical Discoveries of Samuel Thomson,” a foundational text in the development of botanical medicine and alternative healing practices.
However, Thomson did not hesitate to obtain his own special privilege, obtaining a patent for his medical system and selling the family rights for its use at $20 per unit, with the slogan that every man could be his own doctor. Mobilized by Thomson into “friendly societies,” his supporters lobbied intensively in state legislatures against existing licensing laws that restricted medical practice to orthodox physicians. By the 1840s, almost all of these laws had been repealed, amended, or rendered ineffective. This meant that anyone could practice medicine virtually anywhere in the country without fear of prosecution, a situation that persisted for several decades.
A distinctly different and more intellectual threat to the medical establishment was presented by homeopathy, adopted by thousands of American-educated physicians trained in the orthodox tradition. This movement was originally started in Germany by Samuel Hahnemann (1755-1843), a scholarly university graduate who, like Thomson, opposed the standard remedies then in use. In the 1790s, Hahnemann began experiments on himself, recording the physiological reactions produced by various drugs. The first medicine he tested was the bark of the cinchona tree, from which quinine is derived. He discovered that if he ingested it while he was perfectly healthy, his body would manifest many of the symptoms of malaria. This led him to conclude that the drug best able to cure a given disease was the one that produced most of its symptoms in a healthy person. Other agents were tested by Hahnemann and his followers, who found the use of homeopathic remedies, or “similia similibus curentur”, particularly effective, especially when administered in extremely small quantities.
Homeopaths developed their own comprehensive materia medica and offered their system as a substitute for the practices of orthodox physicians, whom they termed allopaths. The allopath, Hahnemann declared, was one who would propose treatments that produced completely opposite effects of disease when administered to a healthy person. Over the decades, however, the term allopathic lost its original meaning and became a convenient label used by all alternative medical movements to describe “regular” or “orthodox” doctors.
The rapid growth of homeopathy can be easily understood. His followers did not administer toxic levels of the standard pharmaceutical drugs of the day, nor did they use bloodletting. Thus, patients only had to endure the disease, not the treatment.
An Era of Non-Drug Medicines: The Emergence of Alternative Systems
“During the 19th century, several drug-free medical systems emerged and found some success in gathering followers. One early initiative was the “popular health movement,” led by Sylvester Graham (1794–1851), a temperance orator who in the 1830s began lecturing against gluttony, improper clothing, sexual permissiveness, and medications, while advocating bathing, fresh air, exercise, and dietary changes. Graham argued that man was heading toward physical degeneration by not living according to the laws of nature. Some of his arguments seemed reasonable, such as the lack of regular bathing at the time, the unbalanced diet, and restrictive clothing for women. However, some of his ideas, notably his ramblings about the supposed evils of too frequent sexual encounters, were based on “sublimated puritanism.”
This image serves as a reminder of Graham’s legacy in shaping health-conscious eating trends and his influence on the American diet that continues in unexpected ways today.
In 1839, Graham published a collection of lectures that became bestsellers. He claimed that following the principles outlined in his book would make medicines and doctors useless. He said followers would be less likely to get sick, and if they did get sick, they wouldn’t be affected as badly. By allowing their natural self-healing powers to express themselves, they would recover more quickly. Graham eliminated certain “unhealthy” foods such as meat, fresh milk, eggs, coffee, tea, and pastries. Its substitutes were always bland and tasteless; the best known of these was a cookie that still bears his name, originally designed to reduce not only hunger, but also sexual appetite. Its critics were quick to point out that its ultimate goal seemed to be to remove fun not only from the kitchen, but also from the bedroom.

Although Graham claimed that his system was all-inclusive, a number of his disciples were among those who began frequenting the offices of another group of drug-free practitioners, the hydropaths. An Austrian farmer named Victor Priessnitz (1799–1851) had discovered that cold water seemed quite effective in treating many chronic illnesses in humans and animals, including gout and rheumatism. Before long, his approach caused a small sensation in Europe, and several health establishments were opened on the continent to teach and practice his methods.
Priessnitz’s approach to healing involved cold water applications, such as baths, compresses, and showers, combined with a natural lifestyle that emphasized fresh air, exercise, and simple, nutritious foods. This method gained immense popularity in the 19th century as an alternative to invasive and often dangerous medical practices of the time.
Despite initial skepticism and criticism from the medical community, Priessnitz’s treatments attracted patients from all over Europe. His establishment of the first hydrotherapy center in Gräfenberg became a model for health resorts worldwide, laying the foundation for modern spa treatments and holistic medicine.
This portrait captures Priessnitz’s thoughtful demeanor, reflecting his dedication to exploring natural healing methods. His innovative work not only revolutionized medical practices of his era but also contributed significantly to the development of wellness and preventive healthcare principles that continue to influence practices today.
Hydropathy was exported to America in the 1840s. Its proponents founded two medical schools, and by the mid-1850s at least twenty-seven health resorts were in operation, primarily in rural areas of the East. and the Midwest, where the water was considered the purest. The treatment mainly consisted of drinking the precious liquid and wrapping one’s body in it. According to Marshall Legan,
“ a sheet of cotton or linen soaked in cold water was spread over several thick woolen blankets… Everything was covered with an eiderdown, and the patient remained in his cocoon from twenty-five minutes to several hours, in depending on the severity of his condition and his ability to sweat profusely. Then the victim was stripped naked, and cold water poured over him, or he was plunged into a cold bath and finally vigorously dry-rubbed. »
Obviously, “heroic therapy ” could also be practiced by healers without drugs.
Still’s familiarity with the notions of Graham and hydropathy can be traced back to his youth, when, in a utopian colony following a combination of these ideas, he was established near the Shawnee Mission. This experimental community did not last long, but while it existed, Reverend Still had to be called upon several times to care for those who were unresponsive or suffering from the regime. No doubt, André was not particularly impressed then or later by these methods. Yet Still came to believe that the drug-free approach was the right one. It was simply a matter of finding a system that could provide a more logical basis for reliable diagnosis and effective treatment. In this sense, Still would find considerable guidance in the principles and practices of magnetic healing.
In 1774, Franz Mesmer (1734–1815), an Austrian physician, postulated that an invisible universal magnetic fluid circulated throughout the body and that too much or too little in one part or as a whole was one of the main causes of illness, especially nervous disorders. The only rational course of treatment was therefore to restore fluid balance. This could be accomplished by making passes over the body with magnets or one’s hands. Mesmer was not the first to heal through touch; rather, he was the first to shape this approach into a coherent system of medical practice.
Many of his early cures by this method were widely publicized, and soon he attracted patients from all over Austria. His success there was short-lived, however, as pressure from the medical community in his native Vienna forced his departure for Paris. In the French capital, Mesmer’s practices became more irregular. Instead of seeing clients separately and discreetly, he formed groups and cared for several patients at a time. Often he used a huge inner vat with extended “magnetized” rods.
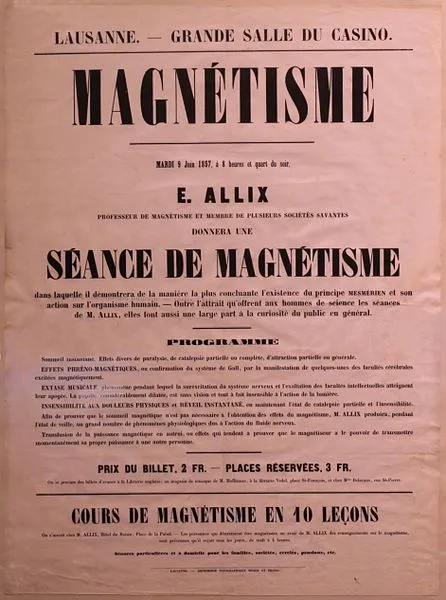
The gathered people bathed together, placing the afflicted parts of their bodies against the metal protrusions, until Mesmer materialized. As an orchestra played solemn music, he entered the room dressed in a flowing lilac robe and touched his patients as he passed. This was designed to bring each individual to a near-seizure state, which Mesmer believed was often necessary to achieve catharsis. The vat was not his only place of healing. Clients were also treated in the open air, under “magnetized” trees or next to “magnetized” rocks.

In 1784, as Mesmer’s practice grew in popularity, two special commissions were created to investigate the relative merits of his claims. One of these groups was named by the French Academy of Sciences and included Benjamin Franklin, Jean Sylvan Bailly and Antoine Lavoisier. This committee declared that a “magnetic fluid” did not exist, that Mesmer’s cures were only the result of suggestion, and that the morals of women undergoing such treatment were threatened. According to them, during an induced crisis, women could become easy targets of seduction. » With the appearance of this study, Mesmer’s personal influence declined. Some of his followers, believing his fundamental principles to be valid, abandoned the vat and other questionable procedures and continued to attempt to gain respectability. Over the next decades, they made progress. In 1831, a somewhat favorable report on the subject was published by the French Academy of Medicine, and indirect support came later, in the writings of James Braid (1795–1860) on what would eventually be called the hypnosis. “
One of the techniques he developed was the “slant gaze upward and inward” induction method of James Braid, a Scottish surgeon and pioneer in the field of hypnosis. Braid made significant contributions to the understanding and practice of hypnosis in the 19th century.
The “gaze up and inward” induction involves instructing the subject to fix their gaze on a fixed point above their line of sight while simultaneously converging their eyes inward. This combination of looking upward and inward is intended to induce a state of heightened concentration and focus, thereby facilitating the process of hypnotic induction.
Braid believed that this specific eye movement could result in a state of mental concentration and suggestibility, essential components of the hypnotic trance. The technique aimed to modify the subject’s state of consciousness and make them more receptive to hypnotic suggestions.
It is important to note that although Braid has made significant contributions to the understanding of hypnosis, the field has evolved, and contemporary hypnotic techniques may differ. The “oblique gaze upward and inward” method, however, remains a historical part of the development of hypnotic induction techniques.
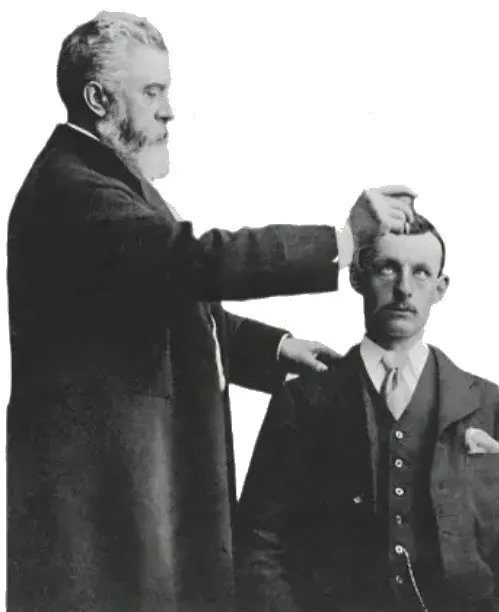
Magnetic healing was introduced to the United States in 1836 by Charles Poyen (d: 1844), who gave a series of public lectures in Boston and took a number of students, training them in massage and other methods then considered useful in restoring fluid balance. Poyen’s activities helped generate considerable interest in magnetic healing, and although his stay in America was relatively brief, the seed he planted was quickly germinated without it. One of those who is said to have heard Poyen lecture was Phineas Parkhurst Quimby (1802–65), who later established a practice consisting mainly of verbal suggestions combined with light caresses of the body. Although Quimby’s writings were not published until after his death, he was an influential figure during his lifetime, serving as a physician, teacher, and inspiration to Mary Baker Eddy (1821–1910), the founder of Christian Science. Quimby’s ideas also provided the intellectual source for the loose confederation of religious groups known as “New Thought.”

The best known mesmerizer before the Civil War was Andrew Jackson Davis (1826–1910), who was also America’s leading advocate of spiritualism. In the first volume of his enormous tome, The Great Harmania (1850), Davis sought to combine the two belief systems.
Conceiving the body as a machine, he maintained that health was simply the harmonious interaction of all parts of man in the performance of their respective functions. This was due to the free and unobstructed flow of the “mind”. Any decrease or imbalance in this “fluid” would cause disease. Like others before him, Davis emphasized healing through the hands. Of particular interest was his treatment of asthma, which in part included vigorous rubbing along the spine.
Although this type of treatment was a small feature of Davis’s practice, later magnetizers, perhaps influenced by the attention paid to the spine by orthodox European medical researchers such as Charles Bell (1774–1842), Francis Magendie (1783–1855), and Marshall Hall (1790–1857), made extensive use of manipulation. One of them was Warren Felt Evans (1817–89), whose name is most often associated with “mental healing.” In his book Mental Medicine (1872), which went through fifteen reprints, Evans noted:
“By rubbing the hand along the spine, an invigorating and revitalizing influence is transmitted to all the organs within the trunk cavity. The hand of benevolence, of purity, of sympathy, applied here by friction combined with light pressure, is a singularly effective remedy against the morbid state of the internal organs. It is always a pleasant medicine to take. »
These sentiments were echoed in the book Vital Magnetism (1874), written by another folk healer, Edwin Dwight Babbitt (1828–1905). He specifically mentioned convulsions, apoplexy, sunburn, headaches, muscular ailments, ordinary rheumatism, and paralysis as disorders that could be cured by spinal treatments. It is unclear whether Still read these works by Davis, Evans, and Babbitt; however, he was well aware of their message. A letter co-signed by him to
editors of the Banner of Light indicates that he was a reader of this journal, oriented towards spiritualism and magnetic healing, and published articles and advertisements from these practitioners in its pages.
Although Still never adopted all of the ideas of his contemporaries, a number of the main principles of magnetic healing made a strong impression on him: the metaphor of man as a divinely ordained machine; health as the harmonious interaction of all parts of the body and the unobstructed flow of fluid; and of course, the use of spinal manipulation. Its most significant difference with them would be on the nature of the fluid. Although he spoke obliquely about the physiological role of magnetic energy for the rest of his life, he believed that free blood flow was the key to health. “I proclaimed,” he later wrote, “that a disturbed artery marked the beginning of an hour and a minute when disease began to sow its seeds of destruction in the human body. That in no case could this be done without a broken or suspended arterial blood flow itself. One who wished to successfully solve the problem of disease or deformity of any kind in every case without exception would find one or more obstructions in an artery or vein. »
In June 1874, Still severed his ties to conventional medicine, an action that shocked his community. Many of his friends and relatives, in reaction to his strange theories and especially to his “laying on of hands”, questioned his sanity. The local minister, seeing him as an agent of the devil, had him expelled from the Methodist Church. Still requested permission to explain his practice at nearby Baker University, a school he had helped establish, but was denied the privilege. Effectively ostracized at Baldwin, Still went to Macon, Missouri, to visit a brother and see if public acceptance of his newly adopted ideas and methods would be better there. It was not the case. After a few months treating only a small number of patients, he moved to Kirksville, located in northeast Missouri, where, to his surprise, “three or four thoughtful people” actually welcomed him. The town then had a population of eighteen hundred and was the commercial capital of Adair County, which had a total population of about thirteen thousand. In a local newspaper, the North Missouri Register, he advertised himself: “AT STILL, MAGNETIC HEALER, Rooms in the Reid Building, south side of the square, above Chinn’s store.” Office Hours – Wednesday, Thursday, Friday and Saturday 9 a.m. to 5 p.m., with a one-hour break from noon to 1 p.m. » Although his practice in this new location was not initially successful, he was comforted that there was no organized persecution by either the clergy or local doctors. Still could also go about his business without much interference from the state. In August 1874, while in Macon, he registered with the county clerk as a physician and surgeon, thereby protecting himself from prosecution for the illegal practice of medicine. Because of the initial tolerance he had enjoyed in Kirksville, he moved his family there in May of the following year.
In the fall of 1876, Still contracted typhoid fever, the effects of which left him disabled for more than six months. After making a full recovery, Still realized that his local clientele would be too small to support his loved ones and repay debts incurred during his illness. In desperation, he applied for a federal army pension, but his application was denied because his service during the Civil War had been entirely in state militias. With few patients in Kirksville, it was necessary to expand its population base. Still became an itinerant practitioner. He traveled for extended periods to several communities across the state, while his wife and children remained in Kirksville. For the next few years, Still’s earnings struggled to keep up with his expenses. On various occasions his relatives offered him financial assistance if he returned to orthodox medicine, but he flatly refused.
The Challenges and Triumphs of Osteopathy: Between Myths, Perceptions and Practical Realities
The newly installed osteopath’s main mission was to create a favorable impression among the city’s inhabitants. The term “osteopathy” sometimes gave rise to misunderstandings, with some wrongly thinking that it was limited to bone conditions. In their advertisements, osteopaths explained that osteopathy was an independent health care system, distinct from faith healing or other medical approaches.
Despite these explanations, skepticism persisted, with some patients confusing osteopathy with esoteric practices such as theosophy or magnetic healing. Osteopaths often found themselves in the delicate position of having to devote time to demystifying these confusions. Additionally, some patients expressed concerns related to their religious beliefs, asking questions about the practitioner’s Christian affiliation.
In this context, osteopaths persuasively emphasized their role as “anatomical engineers,” with in-depth knowledge of the location of each element of the body and its significance for overall health. They often compared their approach to the necessary adjustment of a musical instrument or motor, putting forward the idea that just as these objects require periodic tuning, the human body also requires adjustments to maintain or restore health.
On the contrary, a considerable number of practitioners preferred a more assertive, nevertheless successful, approach, highlighting the superiority of osteopathy compared to traditional medicine. Many osteopaths published detailed lists of the diseases they claimed to treat with particular success, providing specific percentage cure rates for various conditions. Testimonials from satisfied patients also played a crucial role in their marketing strategy. The early clientele of osteopaths across the country consisted primarily of people dealing with chronic problems, repeating the patterns seen in Kirksville.
During their twenty months of practice in Nashville, Dr. JR Schackleford reflected on encountering many cases where patients had exhausted traditional medical avenues, turning to osteopathy as a final option. He emphasized that whether they are the first or last resort for patients, the key was to achieve the desired results. Although reports in the Journal of Osteopathy occasionally address acute infectious disorders, they represent a minor portion of the average osteopathic caseload.
WL Riggs, DO, noted a predominant belief among the public that osteopathy was particularly suited to treating long-standing and chronic cases. However, there was a common perception that its results were relatively slower in countering the rapid processes associated with what are commonly called acute illnesses. This dichotomy of perception highlights the nuanced considerations surrounding the application and effectiveness of osteopathy across different medical conditions.
Osteopaths generally informed patients that rapid recoveries were exceptional, emphasizing the need to adopt realistic expectations. Dr AL Evans warned against overly optimistic advertising, urging practitioners to avoid promising miraculous short-term results. He felt it was more prudent to convey the need to take time to eliminate toxins and induce normal organ function.
To align patient expectations with the progressive nature of osteopathic treatment, practitioners typically charged a monthly fee, often $25 for four weeks of care. Flexible pricing tiering was established for extended treatment periods. However, this organization posed the challenge of patients expecting numerous sessions during the month, regardless of their condition. To remedy this, a customary limit of three treatments per week per client was established, avoiding a possible overload.
Fatigue was a considerable factor, as each session could last up to an hour, impacting both patient and practitioner. Despite these challenges, early osteopaths, as reported in letters to the Journal of Osteopathy and other periodicals, often claimed to be successful in earning a living. They highlighted the growing popularity of osteopathy, customer satisfaction and the expansion of their patient base.
Although these self-congratulatory reports paint a positive picture, they do not provide the complete picture. The newspaper also featured notices of osteopaths changing addresses, indicating the challenges some practitioners were facing. Not all osteopaths viewed osteopathy as a financially stable endeavor; some abandoned the practice altogether. The reasons for business failures varied, including public apathy, failure to impress clientele, and sometimes opposition from local doctors using existing medical licensing laws to hinder the establishment of osteopaths.
In summary, while many osteopaths celebrated success and growth, the reality for others was marked by challenges, changes of address and, in some cases, abandonment of osteopathic practice.
Contextual Background of 19th Century Medicine
The 19th century was a transformative period in the history of medicine, marked by both groundbreaking discoveries and the persistence of archaic practices. During this time, the medical field stood at the crossroads of traditional, often ineffective treatments and the early stages of modern science-based medicine. Understanding this historical context is crucial to appreciating the revolutionary contributions of Andrew Taylor Still and the emergence of osteopathy.
Dominance of Archaic Medical Practices
In the early 19th century, medical treatments were often harsh, invasive, and rooted in outdated theories. One of the most dominant practices of the era was bloodletting, a method believed to balance the body’s “humors.” Physicians would frequently drain significant amounts of blood from patients suffering from illnesses as diverse as fevers, infections, and even mental health disorders. Despite its widespread use, bloodletting often weakened patients and exacerbated their conditions.
Another prevalent treatment involved the use of toxic substances, such as mercury. Mercury compounds, including calomel, were prescribed for a variety of ailments, from syphilis to constipation. These substances, however, were highly toxic and often caused severe side effects, including mercury poisoning, which led to symptoms such as severe gastrointestinal distress, tremors, and even death. These treatments reflected the medical community’s limited understanding of pathology and pharmacology at the time.
Surgical procedures, although increasingly common, were extremely risky due to the lack of anesthesia and antiseptic techniques. Surgeons performed operations without effective pain relief, often relying on brute strength and speed to minimize patient suffering. Infections were rampant, as sterilization of instruments and proper hygiene were not yet standard practices. Consequently, post-surgical mortality rates were alarmingly high.
Prevailing Theories of Disease
The 19th century was also a time when outdated theories of disease causation persisted. The miasma theory, which attributed illness to “bad air” or foul smells, dominated medical thinking. This belief hindered progress in understanding the true causes of disease, such as bacterial and viral pathogens. Physicians and public health officials focused on improving sanitation and ventilation, which, while helpful in reducing disease spread, were based on incorrect assumptions about disease mechanisms.
Simultaneously, the theory of humoral imbalance, rooted in ancient Greek medicine, continued to influence medical practice. This theory proposed that health depended on the balance of four bodily fluids—blood, phlegm, yellow bile, and black bile. Treatments such as purging, emetics, and blistering were employed to restore this perceived balance, often with little regard for their actual effects on the patient’s health.
Early Seeds of Medical Change
Despite the dominance of these archaic practices, the 19th century also witnessed the emergence of new ideas and discoveries that would eventually transform medicine. The advent of germ theory, championed by figures such as Louis Pasteur and Robert Koch, began to challenge traditional views on disease causation. Germ theory established that microorganisms were responsible for many illnesses, laying the groundwork for advances in microbiology, vaccination, and sterilization.
The development of anesthesia in the mid-19th century marked a turning point in surgery. The use of substances such as ether and chloroform revolutionized surgical procedures by enabling pain-free operations, although their application was still in its infancy and fraught with risks. Similarly, the introduction of antiseptic techniques by Joseph Lister dramatically reduced post-surgical infections and mortality, signaling the beginning of modern surgical practice.
Advances in medical education also began to take shape during this period. The establishment of formal medical schools and the standardization of curricula aimed to improve the quality of medical training. However, these changes were slow to gain widespread adoption, and many practitioners still relied on traditional methods and apprenticeships.
Societal Demand for Change
The harsh realities of 19th-century medical practices fueled a growing demand for safer and more effective treatments. Patients, weary of the debilitating effects of bloodletting, mercury poisoning, and other aggressive interventions, began to seek alternatives. This demand coincided with broader societal changes, including the rise of industrialization, which brought with it new health challenges and the need for more efficient healthcare systems.
Alternative medical systems, such as homeopathy and herbal medicine, gained popularity as patients sought gentler approaches to healing. Homeopathy, developed by Samuel Hahnemann, emphasized the use of highly diluted substances to treat illness, offering a stark contrast to the harsh remedies of conventional medicine. Similarly, herbalists promoted the use of natural remedies, arguing that they worked in harmony with the body’s natural healing processes.
This environment of dissatisfaction and exploration created fertile ground for the emergence of new medical paradigms. Andrew Taylor Still, observing the limitations and dangers of contemporary medicine, sought to develop an approach that prioritized the body’s innate ability to heal itself. Osteopathy emerged as a response to the failings of 19th-century medical practices, offering a holistic alternative grounded in the principles of structure, function, and self-regulation.
The Extraordinary Journey of Andrew Taylor Still: From Traditional Medicine to the Foundation of Osteopathy
During the 19th century, several revolutionary medical movements emerged in the United States, posing significant challenges to orthodox medicine. One such movement was led by Samuel Thomson, an autodidact who rejected conventional medical practices, instead advocating the use of botanical remedies to induce sweating and vomiting in patients. Thomson questioned the legitimacy of the medical profession, accusing regular physicians of prolonging illnesses to increase their fees and opposing licensing laws which he believed served to monopolize the healing arts. Although ridiculed by orthodox physicians, Thomson successfully mobilized his supporters to influence state legislatures, resulting in the repeal or amendment of many medical licensing laws.
Another intellectual challenge to orthodox medicine emerged with the adoption of homeopathy in the United States. Initiated in Germany by Samuel Hahnemann, this medical approach was based on the principle of “like cures like,” using remedies that caused symptoms similar to those of the disease. Homeopaths developed their own medical system, positioning themselves as an alternative to orthodox practitioners, whom they called allopaths. Despite criticism of the effectiveness of infinitesimal doses, homeopathy has gained popularity by avoiding the administration of toxic levels of conventional medications.
Before 1860, many homeopaths were trained in orthodox medical schools, but after the Civil War they were expelled from the American Medical Association. This led to the establishment of their own schools and hospitals. Although homeopathic training was as comprehensive as that of allopaths, the split in homeopathy led to the formation of eclectic medicine. Under Wooster Beach’s leadership, the Eclectics rejected the use of mineral-based medicines in favor of resinous medicines, founding their schools before and after the Civil War. However, these eclectic schools were often academically deficient, producing doctors who were less well trained than their orthodox counterparts.
Despite their differences, unorthodox medical movements thrived, accounting for about 15% of doctors at their peak. This diversity included the primarily urban homeopaths and the primarily rural eclectics. The success of these alternative movements prompted some orthodox doctors to reevaluate their practices, gradually abandoning heroic treatments.
Thus, within these medical reforms, Andrew Still, founder of osteopathy, observed that they often offered less harmful diets to patients than regular doctors, although their approach remained empirical and ineffective according to his observations. Still, a Methodist and teetotaler, developed a moral concern about medication use. He questioned the scientific nature of the medication, believing it to be as immoral as alcohol abuse. Convinced that ignorance in medical schools was to blame, he set out to explore a different path, moving away from internal medication and laying the foundations of osteopathy.
In conclusion, 19th-century medical movements in the United States posed diverse challenges to orthodox medicine. Figures such as Samuel Thomson and Samuel Hahnemann challenged established practices, paving the way for alternative approaches like homeopathy and eclecticism. These movements influenced legislation and prompted a reevaluation of orthodox medical practices. In this context, Andrew Still developed his own approach, basing osteopathy on different principles, while criticizing the medical practices of his time.
Legal Conflicts and Institutional Recognition of Osteopathy
The attitude of orthodox doctors towards osteopaths varied considerably, with some considering them harmless and others seeing them as charlatans. The attitude of doctors (MD) often depended on the behavior of osteopaths. If an osteopath worked discreetly, conflicts were less likely; however, those who made grandiose claims and insinuated collusion between MDs and undertakers attracted legal trouble.
Legal clashes took place during arrests, with osteopaths arguing that jealousy and fear motivated such actions. While some osteopaths chose to leave town after legal confrontations, others chose to fight, and most managed to prevail.
An early legal case involved Charles Still, the founder’s son, in Red Wing, Minnesota, in 1893. Arrested for illegal practice during a diphtheria epidemic, public support led to the charges being dropped. Similar legal challenges faced Audrey Moore, DO, in Macon, Illinois, who was jailed but released when patients testified about its benefits.
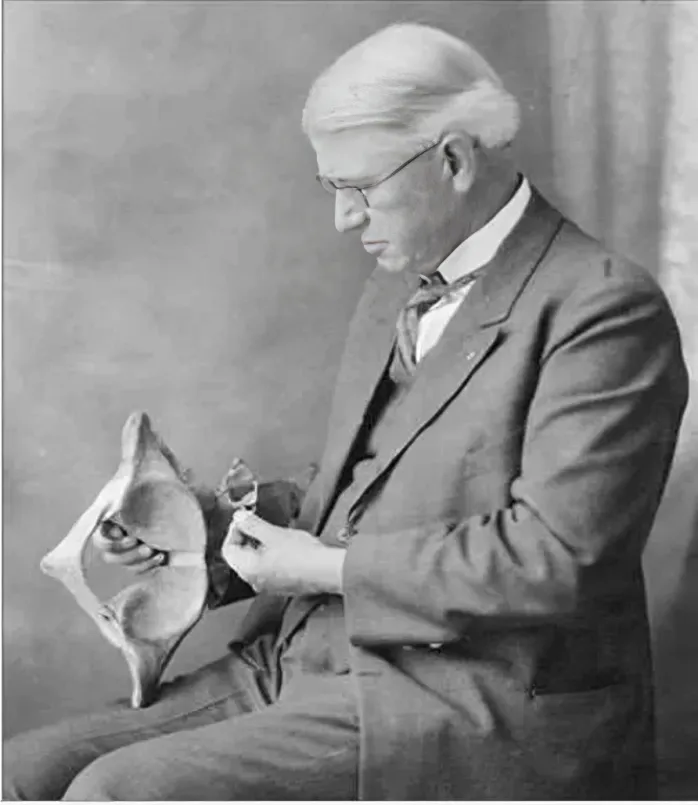
Dr. Charles Edward Still Sr. was a prominent figure in the field of osteopathy and the son of Dr. Andrew Taylor Still, the founder of osteopathic medicine. Born into a family dedicated to advancing healthcare, Charles Edward Still played a crucial role in continuing and expanding his father’s pioneering work. He was known for his meticulous study of human anatomy and dedication to the principles of osteopathic medicine, emphasizing the interrelationship between the body’s structure and function. In this photo, Dr. Still is seen deeply engrossed in examining a pelvic model, illustrating his commitment to understanding the human body’s complexities. Throughout his career, he worked tirelessly to promote osteopathy as a comprehensive approach to health, balancing innovative practices with the foundational philosophies established by his father. His contributions have left a lasting legacy in the medical community, inspiring future generations of osteopaths.
Subimage Caption:
Dr. Charles Edward Still Sr. (1865-1955) examines a pelvic model, reflecting his lifelong dedication to advancing the study and practice of osteopathic medicine.
Some osteopaths have initiated legal action against MDs. In 1898, Harry Lee Nelson, DO, sued the Kentucky Board of Health, demanding an examination and licensing or an end to the threats. Although initially unsuccessful, Nelson won in the Court of Appeal the following year, guaranteeing the right of any DO to practice osteopathy without interference.
The definition of the practice of medicine has become a legal focal point in many state courts. The MDs argued for a broad interpretation, while the DOs insisted that it referred only to the administration of drugs. By 1904, only Nebraska agreed with MD, with other states interpreting “medicine” narrowly. The debates extended beyond the courts to state legislatures, where MDs sought to ban osteopathy, and DOs sought to establish standards of practice.
Vermont was the first to act, granting any graduate of the American School of Osteopathy the right to practice. North Carolina followed, with one patient, Helen DeLenderecie, advocating for osteopathy after her successful treatment. Acceptance of osteopathy faced challenges, including support from Mark Twain in New York, but by 1901, 15 states had passed laws governing osteopathic practice.
Despite initial skepticism, osteopathy has become a formidable competitor to orthodox medicine, challenging the dominance of MDs. Legal struggles and legislative battles underscored the growing institutionalization of osteopathy as a legitimate medical practice at the turn of the century.
The Transatlantic Therapeutic Bridge: Swedish Mechanotherapy and American Osteopathy through the Eyes of Mark Twain
Mechanotherapy, a therapeutic practice rooted in the principles of gymnastics and physiotherapy, holds a vital place in the history of physical medicine. Its development reflects the interplay between European mechanotherapy and the emerging American osteopathic tradition in the late 19th and early 20th centuries. Mechanotherapy involves the use of mechanical means, such as specialized apparatus, exercises, and manual techniques, to treat musculoskeletal disorders, enhance physical function, and promote overall well-being.

In Europe, mechanotherapy gained momentum through the work of pioneers like Gustav Zander, who developed mechanical exercise machines in the 19th century. These devices aimed to replicate the benefits of physical exercise while targeting specific muscles and joints, laying the foundation for the modern field of physical therapy. European mechanotherapy emphasized structured, systematized approaches to rehabilitation, focusing on restoring balance and functionality to the body.
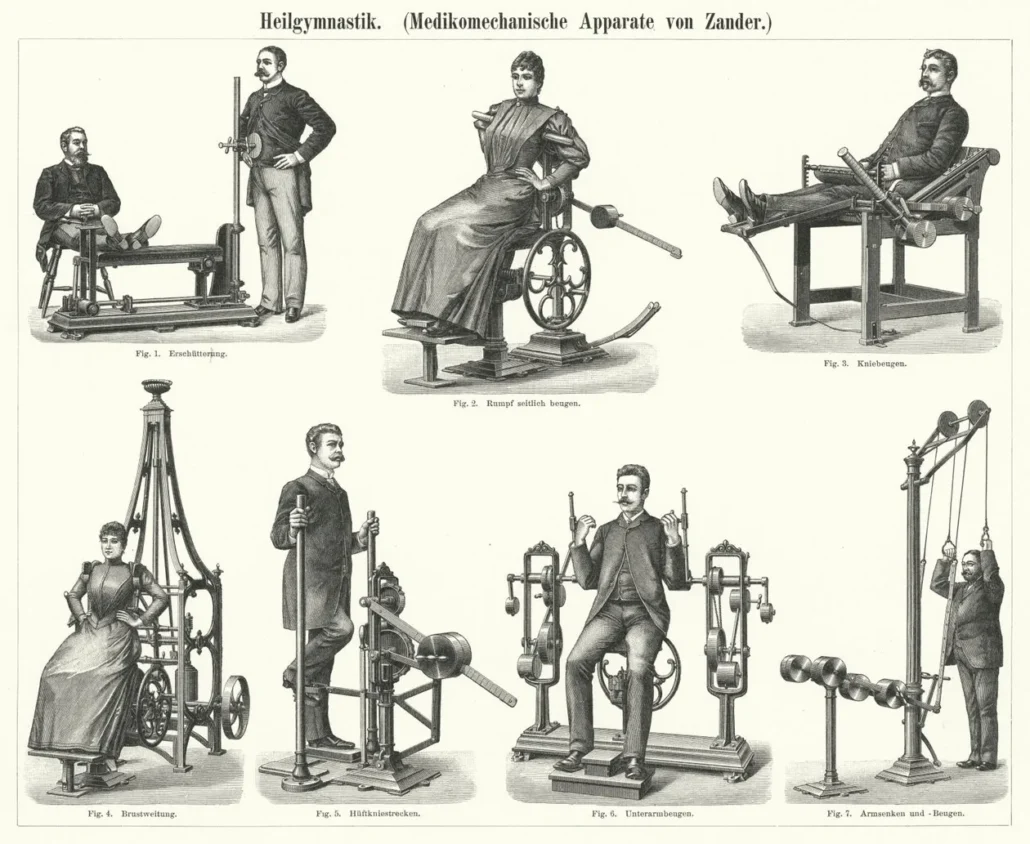
Zander’s apparatuses were designed to replicate specific movements that targeted particular muscle groups or joints. Each device had a unique function, from leg presses to arm extensions, providing resistance or support to the body during exercises. For instance, machines depicted here include devices for knee bending, trunk rotation, chest expansion, and arm curls. They allowed patients to perform controlled and repetitive motions, which were believed to improve strength, flexibility, and mobility.
This mechanotherapy approach was revolutionary in the late 19th and early 20th centuries, offering a systematic and scientific method of physical rehabilitation. Zander’s machines were used in specialized clinics and institutions, where patients could receive targeted treatments under medical supervision. These devices also made therapeutic exercises accessible to individuals with varying levels of physical ability.
Zander’s work significantly influenced the development of modern physiotherapy and exercise science. His emphasis on mechanical precision and individualized therapy set the stage for subsequent advancements in rehabilitation technologies. Today, his mechanotherapy apparatus serves as an enduring testament to the fusion of medical innovation and engineering in the pursuit of better healthcare outcomes.
Simultaneously, in the United States, Andrew Taylor Still, the founder of osteopathy, championed a holistic approach to health that emphasized the body’s natural ability to heal itself when structural integrity was maintained. Osteopathy shared mechanotherapy’s focus on the musculoskeletal system but expanded its scope to include manual manipulations that sought to improve circulation, nervous system function, and overall health.

By 1894, the field was gaining traction, particularly after the establishment of the American School of Osteopathy (ASO) in Kirksville, Missouri, two years earlier in 1892. This institution provided formal training to students, equipping them with knowledge of anatomy, physiology, and manual manipulation techniques to treat ailments. The curriculum reflected Still’s commitment to a holistic, patient-centered approach that prioritized treating the root cause of diseases rather than merely alleviating symptoms.
During this period, osteopathy was met with skepticism and resistance from mainstream medicine. However, it also attracted many supporters, particularly those disillusioned with traditional practices. The year 1894 marked a pivotal time in osteopathy’s journey toward legitimacy and recognition, as its innovative principles began to spread, laying the foundation for what would become a globally recognized healthcare discipline.
The connection between European mechanotherapy and American osteopathy represents a remarkable convergence of innovative ideas and practices that have profoundly influenced the development of modern healthcare. At their core, both disciplines shared a deep understanding of the interplay between movement, structure, and function in achieving and maintaining optimal health. While their approaches differed in technique and focus, the philosophical overlap underscored a shared commitment to holistic, non-invasive treatment methods that emphasized the body’s capacity for self-healing.
European mechanotherapy, spearheaded by pioneers like Gustav Zander, introduced mechanical exercise machines that targeted specific muscle groups and joints. These devices aimed to restore physical function and balance through controlled, repetitive movements. Mechanotherapy’s reliance on precision engineering and systematic approaches to rehabilitation reflected the industrial and scientific ethos of 19th-century Europe. It emphasized the mechanical aspects of the human body, using innovation to complement natural healing processes.
In contrast, American osteopathy, founded by Andrew Taylor Still, focused on manual techniques to restore structural integrity and improve circulation and nervous system function. Osteopathy embraced a broader, holistic view, addressing the interdependence of body systems and emphasizing hands-on care to treat underlying causes rather than symptoms.
The intersection of these two disciplines created a fertile ground for new approaches to health and rehabilitation. Mechanotherapy’s mechanical precision and osteopathy’s hands-on philosophy both recognized the critical role of movement and structure in health. This synergy ultimately influenced the evolution of modern physical therapy and manual medicine, blending the best of both traditions to create comprehensive, patient-centered care.
Mark Twain’s 1900 letter to Andrew Taylor Still highlights a fascinating intersection between Swedish mechanotherapy and the emerging field of American osteopathy, emphasizing their shared principles and goals. Twain’s correspondence reflects not only his wit and frustration with administrative inefficiency but also his deep engagement with medical innovations of the time.
Swedish mechanotherapy, pioneered at the Royal Central School of Gymnastic Instruction in Stockholm, formed the foundation of modern physiotherapy in Europe. Jonas Kellgren, who graduated in 1865, played a pivotal role in shaping this discipline. Mechanotherapy focused on the therapeutic use of movement, structured exercises, and physical manipulation to restore and maintain health. Kellgren’s methods were passed down to his students, including the young Swedish practitioner referenced in Twain’s letter. This applicant sought to expand his expertise by studying osteopathy under Still, bridging the two disciplines.
Twain’s letter humorously critiques the secretary’s inefficiency, describing it with cutting yet entertaining remarks. His primary aim, however, was to secure critical information about enrollment in Still’s osteopathic school, including tuition fees, living costs, and the academic calendar. Twain portrays the Swedish applicant as highly capable and well-trained, having studied under Kellgren, whose techniques shared a kinship with osteopathic principles.
The central purpose of the letter is to secure essential information about enrolling in Still’s osteopathic school. Twain asks specific questions: the start date of the school year, tuition fees, and the cost of living in the area, demonstrating his commitment to ensuring the Swedish applicant has the necessary information to plan his studies. The young man in question, described by Twain as possessing “fine character and capacities,” had studied under the renowned Swedish physiotherapist Kellgren, whose techniques paralleled some osteopathic principles. Twain underscores the applicant’s credentials and his intent to practice osteopathy in America, positioning the young man as a worthy candidate for Still’s program.
Through this letter, Twain not only expresses dissatisfaction with the institution’s communication but also highlights his admiration for the scientific and practical advancements in healthcare represented by both Kellgren and Still. The letter serves as a historical bridge between European mechanotherapy and American osteopathy, capturing Twain’s advocacy for innovation and professionalism in medicine.
The link between Swedish mechanotherapy and American osteopathy lies in the similarity of the fundamental principles. Twain, in his letter, suggests that the bases of Swedish mechanotherapy and American osteopathy are identical. It implicitly recognizes that physical manipulation and movement, characteristic of mechanotherapy, are key elements also present in osteopathy.
In the second example, the 1901 Journal of Osteopathy article reports Twain’s testimony in favor of licensing osteopaths in New York. Twain explicitly recognizes the benefits of osteopathy, emphasizing the services received in London by practitioners trained by Kellgren. This positive experience reinforces Twain’s perception of the effectiveness of osteopathy, in close connection with the principles of Swedish mechanotherapy.
The family connection to the Cyriax lineage, descendants of Jonas Kellgren, underscores the enduring and intergenerational transmission of knowledge and expertise in mechanotherapy. This lineage played a pivotal role in advancing and disseminating the principles of mechanotherapy across Europe and beyond, ensuring that its foundational concepts continued to evolve and influence modern physiotherapy and manual medicine practices.
Jonas Kellgren, a pioneer in Swedish mechanotherapy, passed down his methods to future generations, creating a legacy of innovation in physical rehabilitation. His grandson, James Cyriax, and James’s father, Edgar Cyriax, exemplify this tradition of excellence and advancement. Both Edgar and James Cyriax trained at the Royal Central School of Gymnastic Instruction in Stockholm, the same institution where Kellgren himself studied, solidifying their ties to the origins of mechanotherapy.
Edgar Cyriax contributed significantly to mechanotherapy’s development and adaptation, particularly by integrating its principles into medical education and practice in Europe. He championed the use of movement, structured exercise, and physical manipulation as therapeutic tools, ensuring that mechanotherapy remained a vital element of healthcare. His work laid the foundation for a broader understanding of the interplay between movement and health.
James Cyriax, often referred to as the “father of orthopaedic medicine,” built upon this heritage by refining and modernizing the techniques he inherited. He expanded their application to musculoskeletal diagnostics and treatment, blending mechanotherapy with new insights into pathology and biomechanics. Together, the Cyriax family exemplified how generational expertise can advance a field, making mechanotherapy a cornerstone of modern physiotherapy and manual medicine.
The Rise of Osteopathy Schools and Conflicts Between Still’s Disciples
During the legal battle, several Still graduates started their own schools. The first were the National School of Osteopathy (1895) in Kansas City, the Pacific College of Osteopathy (1896) in Los Angeles, and the Northern Institute of Osteopathy in Minneapolis (1896). In a few years, these schools, as well as the American School of Osteopathy, spread to Boston, Philadelphia, San Francisco, Des Moines, Milwaukee, Chicago, Denver, and smaller cities such as Wilkes-Barre in Pennsylvania, Ottawa in Kansas, Franklin in Kentucky, Fargo in North Dakota, Keokuk in Iowa and Quincy in Illinois. By 1904, about half of the 4,000 practicing DOs had graduated from these alternative schools.
These schools had modest facilities initially, often in offices or converted residences. Admissions criteria were flexible, with an initial tuition fee of $500, lowered to $300-350 to remain competitive. Programs varied, some following the American School model with courses in anatomy, osteopathic diagnosis, and therapy, while others extended the length of study and range of topics. The teaching staff was limited, with sometimes instructors not having a DO degree or osteopathic training.
The equipment also differed, ranging from well-equipped laboratories to more modest facilities with a treatment table, a skeleton and a few posters. Recruitment pitches highlighted the satisfaction of healing naturally, but also the potential earnings, saying graduates could earn $250 to $800 per month.
Catalogs also targeted women, excluded from most regular medical schools, offering osteopathy as a noble alternative. About a fifth of graduates before 1910 were women.
Each school boasted of being the best, highlighting the quality of its facilities, equipment and staff. Rivalries with the American School were heated, with Still believing that its first graduates were unqualified to teach and that these schools were in unfair competition.
The National School of Osteopathy in Kansas City was specifically targeted by the American School, denouncing shorter courses and rumors of degrees for purchase. Tensions were such that legal investigations were carried out, but some schools skirted the rules.
The conflict also extended to schools like the Columbian School of Osteopathy, headed by Marcus Ward, a former associate of Still. Ward, self-proclaimed “co-founder of osteopathy”, had claimed methods similar to Still’s since 1862. Still’s criticism of Ward was fierce, denouncing his inclusion of materia medica in the curriculum.
These tensions between Still’s disciples illustrated the challenges of osteopathy’s rapid growth and the differences of vision that would shape its subsequent development.
Standardization and Professionalization of Osteopathy: Elevating a Medical Discipline
The journey of osteopathy from its humble beginnings in a single school in Kirksville, Missouri, to a globally recognized medical discipline is a testament to the efforts toward standardization and professionalization. As osteopathy grew in popularity and schools began to emerge across the United States, the need for consistency in education, licensing, and practice became apparent. Addressing these challenges laid the groundwork for osteopathy’s acceptance within mainstream medical systems and its expansion on a global scale.
Accreditation of Schools: Ensuring Quality and Consistency
In the early days of osteopathy, schools varied significantly in their approaches to education. Some mirrored Andrew Taylor Still’s original teachings, while others introduced deviations to attract students or align with competing medical paradigms. This lack of uniformity raised concerns about the quality of training and the competence of graduates. By the early 20th century, osteopathy faced a critical juncture: to maintain credibility and ensure consistent care, the profession needed standardized curricula and accreditation mechanisms.
The first major step came with the establishment of the American Osteopathic Association (AOA) in 1897. Initially formed to unite practitioners and protect osteopathy’s unique identity, the AOA also took on the role of accrediting osteopathic medical schools. Schools seeking accreditation had to meet specific standards, including a comprehensive curriculum covering anatomy, physiology, pathology, diagnosis, and treatment techniques. This ensured that all graduates possessed a baseline competence in both osteopathic principles and general medical knowledge.
By 1916, the AOA introduced a formal inspection process to evaluate schools. Institutions that failed to meet its rigorous standards faced closure, helping to weed out diploma mills and unqualified instructors. This move solidified osteopathy’s reputation as a serious and science-based discipline, distinct from other alternative medical practices of the era.
The 1920s and 1930s saw further refinements to osteopathic education. Schools extended their programs from two years to four, aligning with the length of allopathic medical training. Laboratories, clinical facilities, and research programs became integral to osteopathic institutions, elevating their academic standing and preparing graduates for complex medical challenges. These reforms laid the foundation for the modern Doctor of Osteopathy (DO) degree, which rivaled the MD in scope and rigor.
Licensing and Legal Recognition: Establishing Legitimacy
The early 20th century was also marked by legal battles to define osteopathy’s place in the broader medical landscape. Initially dismissed as quackery by mainstream medicine, osteopathy fought to gain legal recognition and the right to practice independently. The process of licensing osteopaths began on a state-by-state basis, with Vermont becoming the first state to grant licensure in 1896.
As more states followed suit, the need for standardized licensing examinations emerged. Early boards often faced opposition from allopathic physicians, who viewed osteopathy as a threat to their monopoly on healthcare. However, the osteopathic community’s commitment to education and patient outcomes gradually earned respect. By the 1930s, most states had established osteopathic licensing boards, and these boards required graduates to pass comprehensive examinations covering both osteopathic principles and general medical knowledge.
A significant milestone occurred in 1936 when the AOA created the Bureau of Professional Education, which oversaw licensing standards nationwide. This organization ensured that only graduates of accredited osteopathic schools could sit for licensure exams, further professionalizing the field. By the mid-20th century, osteopaths were legally recognized as full-fledged medical professionals in all 50 U.S. states, granting them the right to diagnose, treat, and prescribe medication.
Public Perception and Societal Acceptance
The growth of osteopathy as a medical discipline was deeply influenced by how it was perceived by the public and how practitioners navigated societal skepticism. Early osteopaths faced significant challenges in gaining societal acceptance, as their methods were often misunderstood or dismissed as pseudoscience. Over time, strategic efforts in education, public outreach, and patient advocacy reshaped perceptions and helped osteopathy establish its legitimacy.
Early Skepticism and Misconceptions
In its early years, osteopathy was often conflated with alternative and faith-based healing practices, which lacked scientific validation. Many in the medical community dismissed osteopaths as charlatans, while some members of the public viewed their practices with suspicion, associating them with quackery. These misconceptions created barriers for osteopaths seeking to attract patients or secure institutional support.
The Role of Patient Testimonials
Despite skepticism, patient advocacy played a critical role in boosting osteopathy’s reputation. Many patients who experienced relief from chronic conditions or improved mobility after osteopathic treatment became vocal supporters of the practice. Testimonials were frequently shared in local newspapers and public forums, helping to counteract skepticism and foster trust among communities.
Media and Public Campaigns
Osteopathic schools and professional organizations also undertook public awareness campaigns to educate people about the principles of osteopathy. Advertisements emphasized the scientific basis of osteopathic techniques and highlighted their holistic approach to healthcare. Public demonstrations of osteopathic manipulations and lectures by prominent practitioners further helped demystify the practice.
Gaining Support from Influential Figures
The endorsement of osteopathy by prominent individuals, including politicians, clergy, and cultural figures, significantly bolstered its societal acceptance. For example, Mark Twain’s public support for licensing osteopaths in New York highlighted the discipline’s growing credibility. Such endorsements were pivotal in swaying public opinion and legitimizing osteopathy as a serious medical practice.
Impact of Legal Wins on Public Trust
The legal victories achieved by osteopaths not only secured their right to practice but also helped enhance their public image. The recognition of osteopathy as a licensed profession conveyed a sense of legitimacy, reassuring skeptics and encouraging more patients to seek osteopathic care.
Women and Osteopathy: A New Avenue
The inclusive nature of osteopathic education, particularly its openness to female practitioners, also appealed to a broader demographic. Women who entered the field often championed osteopathy as a progressive and patient-centered alternative to traditional medicine, further broadening its appeal.
Public Shifts in the Mid-20th Century
By the mid-20th century, osteopathy had transformed from a niche practice into a respected healthcare option. Its focus on holistic, preventive care resonated with the growing interest in wellness and non-invasive treatments. The integration of osteopathy into broader medical systems further reinforced public confidence, cementing its place in modern healthcare.
The Role of Women in Osteopathy’s Development
The rise of osteopathy coincided with broader societal shifts in the late 19th and early 20th centuries, including the push for women’s inclusion in higher education and professional fields. Unlike many traditional medical schools that barred women, osteopathic institutions embraced their participation, providing opportunities that would shape the trajectory of the profession.
Trailblazing Women in Osteopathy
Andrew Taylor Still’s progressive vision included a belief in equality of opportunity, leading him to welcome women into the first osteopathic school, the American School of Osteopathy (ASO), founded in 1892. Still believed that women brought unique perspectives to patient care, particularly in addressing the holistic needs of families and communities.
Prominent early female osteopaths, such as Nettie Bolles and Blanche Still (daughter of A.T. Still), became pioneers in the field, excelling as practitioners, educators, and advocates. These women not only advanced the science of osteopathy but also served as role models, encouraging others to join the profession.
Women as Practitioners and Educators
Women’s participation in osteopathy grew rapidly, with female students often comprising a significant portion of class enrollments. By 1910, roughly 20% of osteopathic graduates were women, a remarkable figure compared to traditional medical schools at the time.
As practitioners, women were often sought after for their compassionate approach and skill in addressing women’s and children’s health issues. They established practices in urban and rural areas, providing care to underserved populations and earning the respect of their communities.
Many women also became leaders in osteopathic education, shaping curricula and mentoring future generations of practitioners. Their contributions helped solidify osteopathy’s emphasis on holistic care, patient-centered treatment, and preventive medicine.
Overcoming Barriers
Despite the opportunities osteopathy afforded women, female osteopaths faced challenges in gaining acceptance within a male-dominated profession. They often had to prove their competence in the face of skepticism from both patients and peers. Additionally, some female practitioners struggled to balance their professional aspirations with societal expectations of domestic responsibilities.
Women’s leadership in osteopathy also highlighted disparities in access to institutional power. While they played essential roles as educators and practitioners, leadership positions within professional organizations and medical schools were still dominated by men for much of the profession’s early history.
Women’s Advocacy and Public Health Contributions
Female osteopaths became instrumental in advancing public health initiatives, focusing on maternal and child health, nutrition, and hygiene. During the early 20th century, women-led osteopathic clinics and community health programs addressed critical healthcare needs, particularly in rural and underserved areas.
During World War I and II, female osteopaths contributed significantly to the war effort, providing care to soldiers and civilians alike. Their service demonstrated the critical value of osteopathic principles in promoting physical and emotional well-being during times of crisis.
Legacy and Influence
The inclusion of women in osteopathy was a transformative element of the profession’s development, fostering a culture of inclusivity that set it apart from other medical disciplines. Their contributions not only enriched the practice of osteopathy but also challenged societal norms, paving the way for greater gender equity in healthcare.
Today, women make up a significant portion of osteopathic practitioners, researchers, and educators. Their legacy continues to inspire innovation and dedication within the field, underscoring the importance of diversity in shaping the future of medicine.
Challenges and Controversies in Osteopathy’s Evolution
Osteopathy’s journey from an alternative practice to a recognized medical discipline was marked by significant challenges and controversies. These obstacles shaped the profession’s identity and tested its resilience, ultimately paving the way for its standardization and broader acceptance.
Skepticism from the Medical Establishment
From its inception, osteopathy faced fierce opposition from the orthodox medical community. Allopathic physicians often dismissed osteopathy as pseudoscience, questioning its emphasis on manual manipulation and holistic care. This skepticism was rooted in a broader disdain for alternative medical practices that challenged the dominance of conventional medicine.
Medical associations frequently lobbied against osteopathy, seeking to limit its scope of practice through legal and institutional barriers. Early osteopaths were often denied access to hospitals and faced restrictions on their ability to diagnose and prescribe. These limitations spurred the osteopathic community to advocate for legal recognition and fight for the right to practice independently.
Internal Divisions and Philosophical Debates
Osteopathy’s rapid growth led to internal divisions, as practitioners debated the profession’s core identity. Some osteopaths sought to expand their scope by incorporating pharmacology and surgery, while others advocated for a purist approach that adhered strictly to Andrew Taylor Still’s original principles.
These philosophical differences led to the formation of rival schools and organizations, each vying for legitimacy. The tension between traditionalists and progressives created confusion among the public and policymakers, hindering osteopathy’s efforts to present a unified front.
Accusations of Quackery
The early 20th century saw osteopathy embroiled in public controversies over its legitimacy. Critics accused osteopaths of making exaggerated claims about their ability to cure diseases, including conditions beyond their scope. Such accusations fueled negative perceptions and provided ammunition for allopathic detractors seeking to discredit the profession.
Osteopathy also struggled with the presence of unscrupulous practitioners who exploited the lack of standardized regulations to operate diploma mills or offer subpar training. These practices tarnished the profession’s reputation and underscored the urgent need for accreditation and oversight.
Challenges in Standardizing Education
Standardizing osteopathic education was a formidable challenge, as schools varied widely in their curricula, faculty qualifications, and clinical training. Some institutions prioritized accessibility over rigor, leading to inconsistencies in graduate competence. This lack of uniformity undermined osteopathy’s credibility and complicated efforts to establish national licensing standards.
The introduction of accreditation processes by the American Osteopathic Association (AOA) marked a turning point, but resistance from unaccredited schools and competing organizations created friction within the profession. Striking a balance between inclusivity and quality remained an ongoing struggle during osteopathy’s formative years.
Public Perception and Misunderstandings
Osteopathy’s holistic philosophy and emphasis on manual techniques were often misunderstood by the public. Many viewed it as synonymous with chiropractic care or as a niche therapy limited to musculoskeletal issues. Osteopaths worked tirelessly to educate patients and communities about their unique approach, emphasizing their comprehensive training in anatomy, physiology, and pathology.
Public misperceptions were compounded by religious concerns, as some associated osteopathy with faith healing or spiritualism. Osteopaths had to navigate these cultural sensitivities while differentiating themselves from unorthodox practices.
The Struggle for Institutional Inclusion
Osteopathy’s exclusion from mainstream medical institutions posed a significant hurdle. Without access to hospitals, osteopaths were limited in their ability to provide comprehensive care or participate in advanced training. This exclusion reinforced perceptions of osteopathy as a marginal profession and hindered its integration into the broader healthcare system.
Osteopathic leaders recognized the need to address these institutional barriers, advocating for policy changes and forming alliances with sympathetic stakeholders. These efforts laid the groundwork for the eventual inclusion of osteopaths in hospitals and residency programs.
Integration into Broader Medical Systems
The next challenge for osteopathy was integration into the broader healthcare system. While osteopaths had earned the right to practice, they often faced limitations in hospital access and specialization opportunities. Many hospitals were controlled by allopathic physicians who were reluctant to collaborate with osteopaths, perpetuating professional divisions.
The turning point came in the 1960s and 1970s, when osteopathic leaders pursued greater integration. The osteopathic medical curriculum expanded to include advanced surgical and diagnostic training, making DOs virtually indistinguishable from MDs in terms of clinical competence. In 1969, the U.S. Department of Health, Education, and Welfare recognized osteopathy as a complete and distinct branch of medical practice, enabling DOs to participate in federal healthcare programs such as Medicare.
A critical victory came with the establishment of osteopathic residency programs in the 1980s. Osteopathic hospitals began collaborating with allopathic institutions, allowing DOs to train alongside MDs in specialized fields like cardiology, oncology, and neurology. By the early 21st century, a single accreditation system for graduate medical education in the U.S. further unified the two professions, solidifying osteopathy’s place in mainstream medicine.
Osteopathy’s Role in Advancing Holistic and Preventive Healthcare
As osteopathy gained recognition, its principles began influencing broader healthcare trends, particularly the growing emphasis on holistic and preventive care. Osteopathy’s focus on treating the whole person—rather than merely addressing symptoms—resonated with evolving medical philosophies and public health initiatives, carving a unique niche within modern medicine.
The Philosophy of Whole-Body Health
From its inception, osteopathy championed the idea that the body operates as an interconnected system, where the health of one part influences the whole. This philosophy stood in stark contrast to the symptom-focused treatments of conventional medicine in the 19th and early 20th centuries. Osteopaths emphasized maintaining structural balance, promoting circulation, and optimizing nervous system function to enhance the body’s natural ability to heal itself.
Preventive Medicine: A Core Tenet
Osteopathy was among the earliest medical disciplines to advocate for preventive care as a cornerstone of healthcare. Practitioners emphasized the importance of regular adjustments, physical activity, and balanced nutrition to prevent disease. This approach aligned with growing public interest in wellness during the mid-20th century and contributed to osteopathy’s appeal as a forward-thinking medical field.
Integrating Lifestyle and Behavioral Factors
Unlike many contemporary medical practices that focused solely on pharmacological or surgical interventions, osteopaths often considered lifestyle factors—such as stress, posture, and environmental influences—in their diagnoses and treatment plans. This holistic perspective encouraged patients to adopt healthier habits, bridging the gap between treatment and self-care.
Advancing Rehabilitation and Physical Medicine
Osteopathy’s emphasis on manual manipulation and structural alignment positioned it as a leader in the emerging field of physical medicine and rehabilitation. Techniques developed by osteopaths to treat musculoskeletal disorders, sports injuries, and chronic pain were later adopted and adapted by physiotherapists, chiropractors, and other healthcare providers.
Shaping Public Health Policies
Osteopathy’s preventive philosophy also influenced public health policies. In the mid-20th century, osteopathic organizations advocated for greater focus on community health initiatives, emphasizing regular check-ups and early intervention. This approach dovetailed with broader efforts to reduce healthcare costs by preventing chronic illnesses before they required intensive treatment.
Impact on Patient-Centered Care
Osteopathy’s commitment to treating patients as individuals, rather than cases, was a precursor to the modern patient-centered care movement. Osteopaths were often praised for spending more time with patients, listening to their concerns, and tailoring treatments to their unique needs. This empathetic approach fostered trust and satisfaction, setting a benchmark for quality care in medicine.
A Blueprint for Integrative Medicine
The principles of osteopathy laid the groundwork for what is now known as integrative medicine, which combines conventional treatments with complementary therapies. By advocating for non-invasive interventions, osteopathy helped shift medical culture toward approaches that prioritize patient wellness and minimize harm.
Contributions to Medical Knowledge and Research
Osteopathy’s rise as a respected medical discipline was not only due to its professionalization but also to its significant contributions to medical knowledge and research. The field played a crucial role in advancing understanding of the musculoskeletal system, holistic healthcare, and the interconnectedness of bodily systems. These contributions helped bridge gaps between traditional medical approaches and innovative therapies, ultimately fostering integration into broader medical systems.
Development of Musculoskeletal Science
One of osteopathy’s most enduring contributions has been its focus on the musculoskeletal system. Pioneers in the field conducted extensive research into the relationships between bones, muscles, nerves, and vascular systems, developing a nuanced understanding of how structural integrity affects overall health. Techniques such as palpation and spinal manipulation, central to osteopathy, also informed allied fields like physical therapy and chiropractic care. These insights have led to improved diagnostic tools for musculoskeletal disorders and better outcomes in rehabilitative medicine.
Holistic Health Approaches
Another groundbreaking contribution was osteopathy’s emphasis on holistic care—treating patients as whole individuals rather than addressing isolated symptoms. This approach laid the foundation for a patient-centered model of care that is now widely recognized in mainstream medicine. Osteopaths were early advocates for considering lifestyle factors, nutrition, and emotional well-being in healthcare, a perspective that has become central to modern preventive medicine.
Evidence-Based Practice
As osteopathy gained prominence, practitioners sought to substantiate its principles through scientific research. By the mid-20th century, osteopathic institutions established research facilities to study the efficacy of osteopathic manipulative treatment (OMT) and its impact on conditions ranging from chronic pain to respiratory disorders. Published studies in peer-reviewed journals demonstrated the benefits of OMT, bolstering osteopathy’s credibility within the medical community.
Integration with Biomedical Advances
Osteopathy also contributed to bridging traditional and modern medical practices. By incorporating advancements in biomedical sciences—such as radiology, pharmacology, and surgical techniques—osteopathic physicians expanded their scope while preserving their distinct approach to care. This integration highlighted the adaptability of osteopathy and underscored its relevance in a rapidly evolving medical landscape.
National and International Expansion
While osteopathy’s roots were firmly planted in the United States, its principles resonated globally, leading to its expansion into other countries. In Canada, the United Kingdom, and Australia, osteopathy developed along slightly different trajectories. In some nations, it evolved as a manual therapy focused on musculoskeletal health, while in others, it mirrored the American model of full medical practice.
The spread of osteopathy required adaptation to diverse legal and cultural landscapes. For example, in the United Kingdom, osteopathy gained legal recognition in 1993 through the Osteopaths Act, which established a regulatory framework and professional register. In Canada, the practice of osteopathy is more variable, with some provinces recognizing it as a complementary therapy and others aligning it more closely with chiropractic care.
Despite these variations, international organizations such as the Osteopathic International Alliance (OIA) have worked to promote a unified understanding of osteopathy’s principles and practices. Conferences, research collaborations, and educational exchanges have fostered global cooperation, ensuring that osteopathy continues to evolve while maintaining its core philosophy of holistic, patient-centered care.
The Spread and Global Influence of Osteopathy
Andrew Taylor Still’s innovative ideas not only revolutionized healthcare in the United States but also resonated with practitioners and patients across the globe. The holistic philosophy and hands-on techniques of osteopathy gradually spread to every continent, where they adapted to the unique cultural, social, and medical landscapes of each region.
Early Beginnings of Global Expansion
Osteopathy’s first major leap beyond the United States occurred in the early 20th century, as graduates from the American School of Osteopathy (ASO) began to travel and teach abroad. The principles of manual therapy, structural alignment, and self-healing attracted international attention, particularly from Europe, where alternative medical philosophies were already gaining traction.
The United Kingdom emerged as a key player in osteopathy’s global expansion. John Martin Littlejohn, a protégé of Still and a key figure in the discipline, brought osteopathy to Britain and founded the British School of Osteopathy (BSO) in 1917. His efforts established a European hub for osteopathic training and practice, which would influence the discipline’s growth across the continent.
The Evolution of Osteopathy in Europe
In Europe, osteopathy took on a distinctive character, evolving as a manual therapy that complemented conventional medicine. France, Italy, and Germany became strongholds of osteopathy, with practitioners adapting the practice to meet regulatory requirements and cultural preferences. By the late 20th century, many European countries had granted legal recognition to osteopathy, enabling its integration into formal healthcare systems.
Professional organizations, such as the European Federation of Osteopaths (EFO), were established to unify osteopathic practice and advocate for standardization across national borders. These efforts helped to cement osteopathy’s reputation as a credible and effective healthcare discipline throughout Europe.
Global Reach: Commonwealth, Asia, and Beyond
Osteopathy’s holistic approach to health also found fertile ground in Commonwealth countries like Canada, Australia, and New Zealand. In Australia, the discipline became a fully licensed profession, with osteopaths gaining the same legal status as medical doctors. Canada similarly embraced osteopathy, developing a robust community of practitioners who integrated Still’s principles with modern healthcare techniques.
In Asia and Africa, the spread of osteopathy has been slower but steady. Japan, India, and South Africa are among the countries where osteopathy is gaining traction as patients seek alternative, non-invasive solutions to chronic pain and musculoskeletal disorders. Educational initiatives and professional networks are helping to build a foundation for osteopathy’s growth in these regions.
Challenges of Global Standardization
While osteopathy’s global influence continues to expand, it has faced challenges in achieving uniformity. In the United States, osteopathy has evolved into a comprehensive medical discipline, with Doctors of Osteopathy (DOs) practicing as fully licensed physicians. In many other countries, however, osteopathy is still viewed primarily as a manual therapy, creating discrepancies in education, scope of practice, and public perception.
Organizations like the Osteopathic International Alliance (OIA) are working to address these disparities, promoting standardized education and fostering international collaboration among osteopathic communities.
Modern Relevance and Future Prospects
Today, osteopathy is practiced in over 50 countries, with its principles influencing not only musculoskeletal care but also broader areas of preventive medicine and holistic health. As patients worldwide seek more personalized and less invasive treatments, osteopathy’s appeal continues to grow. Its emphasis on structural integrity, patient-centered care, and natural healing has made it a vital component of healthcare in the 21st century.
A Testament to Still’s Vision
The global journey of osteopathy is a testament to the enduring relevance of Andrew Taylor Still’s ideas. From a small community in Kirksville, Missouri, to a worldwide movement, osteopathy has proven its adaptability and universal appeal. Its success reflects the timelessness of its principles: that the body is a unit, structure and function are interrelated, and the human body has an innate capacity for healing.
As osteopathy continues to grow and influence global healthcare, it serves as a powerful reminder of Still’s vision and his transformative contributions to medicine.
Modern Legacy of Andrew Taylor Still
Andrew Taylor Still’s vision of osteopathy as a holistic, patient-centered approach to healthcare has transcended its 19th-century origins to become a respected discipline within modern medicine. His principles of structural integrity, the interrelationship between form and function, and the body’s innate ability to self-heal continue to influence contemporary medical practices worldwide. Today, osteopathy thrives as both a complementary and independent healthcare system, integrated into diverse healthcare models and recognized for its contributions to improving patient outcomes.
A Global Discipline
Osteopathy, once confined to small towns in the United States, has become a global practice embraced in over 50 countries. In regions like Europe, Canada, Australia, and New Zealand, osteopathy has achieved formal recognition, with practitioners playing significant roles in multidisciplinary healthcare teams. The discipline’s success abroad is due, in part, to its adaptability. Modern osteopathy incorporates Still’s foundational principles while accommodating advancements in medical science, including diagnostic imaging, pharmacology, and surgical interventions, ensuring it remains relevant in addressing 21st-century health challenges.
For example, in the United Kingdom, osteopathy is fully regulated by law and integrated into the National Health Service (NHS). Similarly, in France, osteopathy has gained widespread acceptance, with thousands of licensed osteopaths practicing in both private clinics and public healthcare settings. These developments highlight the discipline’s ability to coexist with conventional medicine while providing unique benefits, particularly in musculoskeletal care and chronic disease management.
Contributions to Modern Medicine
Still’s philosophy has had far-reaching implications beyond osteopathy. His emphasis on holistic care and the patient’s active role in their health has influenced broader trends in modern medicine, such as integrative and functional medicine. These fields share osteopathy’s focus on addressing the root causes of disease rather than merely treating symptoms, emphasizing the importance of lifestyle, nutrition, and prevention.
Moreover, osteopathic manipulative treatment (OMT), a hallmark of Still’s approach, has gained recognition for its effectiveness in treating various conditions. Research has demonstrated the efficacy of OMT in alleviating lower back pain, migraines, and respiratory issues, offering a non-invasive alternative to medication or surgery. The integration of manual therapy into pain management strategies reflects Still’s enduring impact on how healthcare professionals approach physical ailments.
Holistic and Preventive Healthcare
Osteopathy’s holistic philosophy aligns closely with modern healthcare’s shift toward preventive care. As healthcare systems grapple with the rising burden of chronic diseases, osteopathy offers a model that prioritizes maintaining health and preventing illness. Practitioners take a whole-person approach, addressing not only physical symptoms but also emotional, social, and environmental factors influencing health. This comprehensive perspective, rooted in Still’s teachings, resonates with patients seeking alternatives to fragmented and symptom-focused care.
Education and Research
The legacy of the American School of Osteopathy (now A.T. Still University) endures through the robust educational and research institutions it inspired. Osteopathic medical schools in the United States train thousands of physicians each year, producing fully licensed doctors of osteopathic medicine (DOs). These professionals practice across all specialties, from primary care to surgery, underscoring the versatility and depth of osteopathic training.
Globally, osteopathy-focused institutions continue to expand their curricula, emphasizing evidence-based practice and research. This commitment to scientific validation has bolstered osteopathy’s credibility, attracting both practitioners and patients who value its integrative approach. Studies published in leading medical journals demonstrate the efficacy of osteopathic techniques, bridging the gap between traditional practices and contemporary scientific standards.
Recognition and Integration
The formal recognition of osteopathy as a legitimate medical discipline is a testament to Still’s enduring legacy. In the United States, osteopathic physicians enjoy the same rights and responsibilities as their allopathic counterparts, with DOs serving as primary care providers, specialists, and leaders in healthcare policy. Outside the U.S., non-physician osteopaths work collaboratively with other healthcare professionals, contributing their expertise in manual therapy and patient-centered care.
This integration has led to osteopathy’s inclusion in global health initiatives. For instance, osteopaths participate in programs addressing non-communicable diseases (NCDs), leveraging their skills to improve musculoskeletal health and enhance mobility among aging populations. These contributions underscore osteopathy’s relevance in tackling pressing health issues on a global scale.
Challenges and Opportunities
Despite its achievements, osteopathy continues to face challenges in gaining universal acceptance. In some regions, misconceptions about its scope and effectiveness persist, limiting its integration into mainstream healthcare. Additionally, variations in training standards across countries can create disparities in practice and public perception. Addressing these issues requires continued advocacy, education, and research to highlight osteopathy’s value and ensure consistent quality of care worldwide.
On the other hand, advancements in technology and an increasing emphasis on patient-centered care present opportunities for osteopathy to expand its reach. Telemedicine, for example, offers a platform for osteopaths to provide consultations and guidance remotely, broadening access to their services. Similarly, collaborations with other medical disciplines can further osteopathy’s role in interdisciplinary care, enriching its contributions to modern healthcare.
A Lasting Vision
Andrew Taylor Still’s vision of a healthcare system grounded in compassion, science, and holistic care remains as relevant today as it was over a century ago. His belief in the body’s innate capacity to heal and the importance of structural integrity has inspired generations of practitioners to challenge conventional norms and prioritize patient well-being.
Through its integration into modern healthcare systems, its contributions to medical research, and its emphasis on holistic and preventive care, osteopathy continues to honor Still’s legacy. It stands as a testament to the enduring power of innovative ideas to transform medicine and improve lives, ensuring that Andrew Taylor Still’s revolutionary insights will continue to shape the future of healthcare.
Annex 1: Timeline of Key Events in the Life of Andrew Taylor Still
Early Life and Influences
- 1828: Andrew Taylor Still is born on August 6 in Jonesville, Virginia, as the third of nine children to Abram and Martha Still. His father is a Methodist preacher, farmer, and physician.
- 1834: The Still family relocates to New Market, Tennessee, where Abram accepts a new preaching position.
- 1837: The family moves to Missouri, exposing young Andrew to the hardships and resilience of frontier life, which later shape his philosophy of self-reliance and healing.
Education and Medical Training
- 1842–1848: Still attends intermittent formal schooling but gains much of his medical knowledge from his father and self-study.
- 1851: Joins his family at the Wakarusa Mission in Kansas Territory, where he begins to study medicine more rigorously under his father’s guidance.
Personal and Professional Milestones
- 1853: Marries Mary Margaret Vaughn and starts a family.
- 1854: Begins practicing medicine, relying on the principles of “heroic medicine,” including bloodletting and the use of mercury-based treatments like calomel.
- 1860: Mary Margaret dies, leaving Still a widower with three children. He later remarries and continues to build his family.
The Civil War Years
- 1861–1864: Serves as a Union Army surgeon during the American Civil War, witnessing firsthand the inadequacies and brutality of conventional medicine, which deepens his dissatisfaction with prevailing medical practices.
- 1864: Suffers personal tragedy when three of his children die from spinal meningitis. These losses profoundly affect him and inspire his search for a better approach to healthcare.
Founding the Principles of Osteopathy
- 1874: Experiences a pivotal moment of inspiration, declaring the founding of osteopathy. He announces his revolutionary ideas on the relationship between the musculoskeletal system, health, and the body’s ability to self-heal.
- 1875–1876: Faces widespread skepticism from the medical community and struggles to gain acceptance. His unorthodox ideas are met with hostility, and he is ostracized by colleagues and community members.
Building a Practice and Reputation
- 1877: Moves to Kirksville, Missouri, where he establishes a clinic and begins treating patients using his new methods, gaining attention through successful cases.
- 1889: Opens his first infirmary in Kirksville, where patients flock from across the country seeking treatment.
Founding of the American School of Osteopathy (ASO)
- 1892: Founds the American School of Osteopathy (ASO) in Kirksville, Missouri, formalizing the education of osteopathic practitioners. The first class comprises five students, including three of his children.
- 1894: Graduates the first class of osteopaths, marking a significant step in legitimizing the discipline.
- 1897: Establishes the American Osteopathic Association (AOA), providing a governing body to promote and regulate the practice of osteopathy.
Legal Recognition and Expansion
- 1899: The state of Vermont becomes the first to grant legal recognition to osteopathy, paving the way for broader acceptance.
- 1901: The Missouri legislature officially licenses the practice of osteopathy, a landmark victory for Still and his followers.
- 1910: Osteopathy gains recognition in several other states, with practitioners expanding its reach across the United States.
Later Life and Legacy
- 1914: Retires from active practice but remains a respected figure in the osteopathic community. By this time, his methods have gained widespread popularity and acceptance.
- 1917: Andrew Taylor Still passes away on December 12 in Kirksville, Missouri, leaving behind a thriving legacy that continues to influence modern medicine.
Posthumous Recognition and Global Influence
- 1920s–1930s: Osteopathy expands internationally, with practitioners establishing schools and clinics in Europe, Australia, and beyond.
- 1960s–1970s: In the United States, osteopathic physicians gain full practice rights, achieving parity with allopathic doctors.
- 2000s: Osteopathy becomes fully regulated in countries such as the United Kingdom, France, and Canada, further cementing its global presence.
Legacy Today
- 2020s: Andrew Taylor Still’s principles remain foundational to modern osteopathic medicine, influencing holistic healthcare approaches and integrative medicine worldwide.
Annex 2: Core Principles of Osteopathy
Osteopathy, founded by Andrew Taylor Still in the late 19th century, is rooted in a revolutionary philosophy that views the human body as an interconnected system. The following principles underpin the practice of osteopathy and have guided its evolution into a respected medical discipline:
1. The Body as a Unit
Osteopathy emphasizes the interconnectedness of all bodily systems. Still believed that the body functions as an integrated whole, where physical, emotional, and environmental factors influence health. This holistic perspective stands in contrast to conventional approaches that often treat diseases in isolation.
- Key Idea: Treat the patient, not the disease. The body is seen as a dynamic, interrelated system, and restoring balance in one area can promote health across the entire organism.
2. Structure and Function Are Interrelated
One of the core tenets of osteopathy is the intimate relationship between the body’s structure (bones, muscles, tissues) and its function (circulation, nerve signaling, organ performance). A disruption in the structural integrity of the body can lead to dysfunction and disease.
- Example: Misalignment of the spine may compress nerves, impair blood flow, or disrupt organ function. Osteopathy seeks to correct these misalignments to restore optimal function.
3. The Body Possesses Self-Healing Mechanisms
Still believed that the body has an innate ability to heal itself when given the opportunity. Osteopathy focuses on removing obstacles to this natural process, such as structural imbalances, poor circulation, or nerve interference.
- Key Idea: The role of the practitioner is to facilitate the body’s natural self-healing capacity rather than impose artificial interventions. This approach aligns with the concept of “do no harm” in medical ethics.
4. Prevention and Health Maintenance
Osteopathy prioritizes prevention over cure by maintaining the structural and functional integrity of the body. By addressing underlying imbalances before they manifest as illness, osteopathy emphasizes long-term well-being.
- Key Idea: Preventive care and lifestyle adjustments, such as proper nutrition, posture, and exercise, are integral to osteopathic philosophy.
5. Holistic and Patient-Centered Care
Osteopathy takes into account the patient’s lifestyle, environment, and emotional state. By understanding the broader context of a patient’s life, osteopaths aim to provide individualized care that addresses the root causes of dysfunction rather than merely alleviating symptoms.
- Key Idea: Every patient is unique, and their treatment should reflect this individuality.
Practical Application
These principles form the basis for osteopathic manipulative treatment (OMT), a hands-on approach to diagnosing and correcting structural imbalances. OMT techniques include:
- Soft Tissue Manipulation: Improving circulation and relieving tension.
- Joint Mobilization: Restoring range of motion.
- Cranial Techniques: Supporting nervous system function.
Through these methods, osteopathy supports the body’s natural systems to function efficiently, promoting health and vitality.

















{kind=link}