

Understanding Lumbar Facet Syndrome: A Common Cause of Low Back Pain
The lumbar spine is a complex structure that provides support, flexibility, and protection for the spinal cord while enabling a wide range of movements. Among its key components are the facet joints, small but vital articulations that connect the vertebrae and stabilize the spine. When these joints become inflamed, irritated, or degenerate due to aging, trauma, or repetitive strain, the condition known as lumbar facet syndrome can develop. This syndrome is a significant cause of low back pain, a condition that affects millions worldwide and profoundly impacts quality of life.
Lumbar facet syndrome is characterized by localized pain, stiffness, and reduced mobility in the lower back, often exacerbated by specific movements like twisting or arching. While the pain may remain confined to the lumbar region, it can radiate into the buttocks or thighs, further limiting daily activities. Understanding this condition requires a closer look at the facet joints’ role and how their dysfunction contributes to the syndrome’s symptoms and progression.
Overview of Lumbar Facet Syndrome
Lumbar facet syndrome is a degenerative condition affecting the small, paired facet joints located in the posterior part of the spine. These joints are integral to spinal stability, providing support during movements such as bending, twisting, and extending the back. Over time, repetitive motion, aging, or trauma can wear down the cartilage that cushions these joints, leading to irritation, inflammation, and pain.
The condition’s development is influenced by various factors, including poor posture, prolonged sitting, physical strain, and even genetic predisposition. It is particularly common in older adults, as the natural aging process often results in cartilage degeneration and reduced joint lubrication. However, individuals with physically demanding jobs or those engaged in high-impact sports are also at an elevated risk.

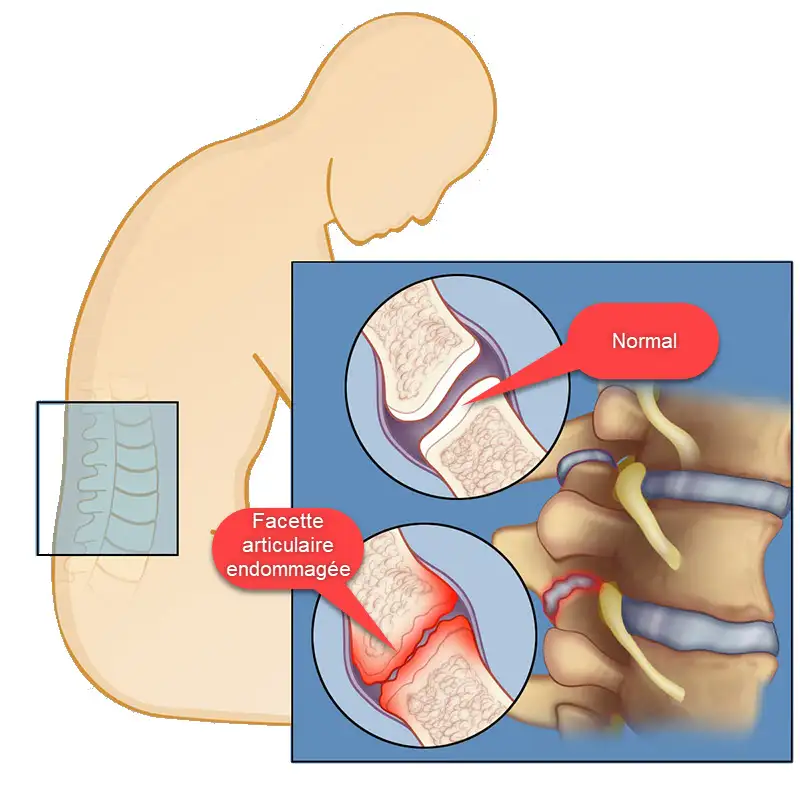
The zoomed-in views in the image highlight the anatomy of the lumbar spine’s facet joints, showing how they connect adjacent vertebrae and contribute to the spine’s overall stability and flexibility. In cases of lumbar facet syndrome, these joints can become stiff, inflamed, or experience bone overgrowth, which may lead to back pain that is typically localized and often worsened by movements like bending or twisting. Lumbar facet syndrome. Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. – Own work, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=27796926
Symptoms of lumbar facet syndrome can vary widely but typically include localized pain in the lower back, stiffness, and discomfort during movements like bending backward or rotating the torso. Unlike conditions such as herniated discs, lumbar facet syndrome rarely causes nerve root compression or sciatica-like pain radiating into the legs. Instead, its hallmark symptoms are centered on mechanical discomfort and restricted mobility.
Early recognition and treatment of lumbar facet syndrome are crucial to prevent the progression of symptoms and minimize its impact on daily life. Effective management often requires a multidisciplinary approach that addresses both the mechanical and inflammatory aspects of the condition.
Warning: The information provided is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before starting any new treatment, exercise program, or health regimen, especially if you experience persistent back pain or symptoms of lumbar facet syndrome. Do not attempt to perform osteopathic manipulation techniques on yourself or others. These techniques require specialized training and should only be performed by a licensed osteopath or qualified healthcare professional. Improper application of these techniques can lead to injury or worsen existing conditions. Early diagnosis and expert guidance are essential for safe and effective management.
Anatomy of the Facet Joints
Facet joints, also known as zygapophyseal joints, are synovial joints located between and behind adjacent vertebrae in the spine. Each vertebra is connected to the one above and below it by a pair of facet joints, which work in conjunction with intervertebral discs to stabilize the spine and facilitate movement.
Structurally, the facet joints are small, flat articulations covered in a layer of cartilage and surrounded by a capsule filled with synovial fluid. This fluid acts as a lubricant, allowing the joint surfaces to glide smoothly against one another during movement. The orientation of the facet joints varies along the spine, influencing the type and range of motion permitted in each region.
- Lumbar Spine: In the lumbar region, the facet joints are vertically oriented, allowing for significant flexion and extension movements but limiting rotation. This design helps the lower back support the body’s weight while maintaining stability.
- Cervical and Thoracic Spine: In contrast, the facet joints in the cervical spine permit greater rotation, while those in the thoracic region are angled to allow limited movement due to their role in rib cage stability.
The facet joints are richly innervated by sensory nerves, making them highly sensitive to irritation and inflammation. When the cartilage within these joints deteriorates or when capsular tears occur due to trauma, the resulting inflammation can stimulate these nerves, leading to pain. The surrounding muscles may also contract reflexively in response to the pain, further exacerbating stiffness and discomfort.
Degeneration of the facet joints is a natural part of aging, but additional stressors like poor posture, repetitive heavy lifting, or obesity can accelerate this process. Over time, the thinning of cartilage and the formation of osteophytes (bony growths) may lead to joint dysfunction, instability, and the characteristic symptoms of lumbar facet syndrome.
Key Symptoms of Lumbar Facet Syndrome: Pain, Stiffness, and Reduced Mobility
Lumbar facet syndrome is a common source of lower back pain, often characterized by a combination of localized discomfort, radiating pain patterns, and functional limitations. The condition stems from irritation, inflammation, or degeneration of the small facet joints located in the posterior portion of the lumbar spine. These symptoms not only affect physical well-being but also significantly impact daily life by limiting mobility and reducing quality of life. Understanding the hallmark symptoms of lumbar facet syndrome is essential for proper diagnosis and effective treatment.
Key Symptoms of Lumbar Facet Syndrome: Pain, Stiffness, and Reduced Mobility
The most prominent symptom of lumbar facet syndrome is localized pain in the lower back. This pain is typically centered around the affected facet joints, which are located near the vertebral column. Unlike other conditions such as herniated discs, the pain in lumbar facet syndrome is not commonly associated with nerve root compression and tends to remain confined to the lumbar region.
Characteristics of Localized Pain:
- Dull, Aching Pain: The pain is often described as a dull, deep ache rather than a sharp or shooting sensation. This discomfort may increase in intensity during specific movements or prolonged static positions.
- Tenderness to Palpation: Direct pressure applied to the lumbar spine, particularly over the affected facet joints, often elicits tenderness. This is a key diagnostic feature during clinical examinations.
- Aggravation by Movement: Certain movements, such as arching the back (extension) or twisting the torso, can exacerbate pain due to increased pressure on the facet joints. Patients frequently report worsening discomfort when rising from a seated position or after prolonged standing.
Localized pain in lumbar facet syndrome can lead to muscle stiffness and tension in the surrounding areas, further contributing to discomfort. This stiffness can create a protective response as the body attempts to limit movement to prevent further irritation.
Referred Pain Patterns: When Low Back Pain Radiates to the Hips or Thighs
While lumbar facet syndrome primarily causes localized pain, it can also produce radiating pain patterns that mimic other conditions. This type of referred pain occurs when inflammation or irritation of the facet joints affects nearby nerves, resulting in discomfort that extends beyond the lumbar region.
Common Radiating Pain Patterns:
- Buttocks and Upper Thighs: Pain often radiates to the buttocks or upper thighs, typically on the same side as the affected joint. This is distinct from sciatica, as the pain does not usually extend below the knee.
- Flank Pain: In some cases, patients may experience discomfort along the flanks or sides of the lower back, reflecting the distribution of sensory nerves connected to the facet joints.
- Worsening with Activity: Radiating pain is frequently triggered or worsened by movements such as bending, twisting, or lifting, which place additional stress on the facet joints.

The pain areas highlighted in the images correspond to this distribution, showing a concentration of discomfort around the sacroiliac region and extending laterally over the hips. Unlike other conditions such as herniated discs, lumbar facet syndrome does not typically cause pain that radiates down the legs (sciatica), but it can still result in significant mobility limitations and discomfort. The pain is often worse with specific movements, such as arching the back or twisting, which place stress on the affected joints. Proper diagnosis and treatment, such as osteopathic manipulation or physiotherapy, can help relieve symptoms and restore mobility.
It is important to note that while radiating pain in lumbar facet syndrome can resemble nerve root compression, it lacks the neurological symptoms (e.g., numbness, tingling, or weakness) typically associated with conditions like herniated discs. This distinction helps healthcare providers differentiate lumbar facet syndrome from other spinal disorders.
How Lumbar Facet Syndrome Limits Daily Activities and Movement
Functional limitations caused by lumbar facet syndrome can have a profound impact on a person’s ability to perform daily activities. These limitations arise from a combination of pain, stiffness, and reduced mobility, which collectively hinder the normal range of motion in the lumbar spine.
Key Functional Limitations:
- Restricted Range of Motion:
Patients often experience difficulty with movements that require flexion, extension, or rotation of the spine. Tasks such as bending to tie shoes, reaching for objects, or twisting to look behind are commonly impaired. - Difficulty with Prolonged Positions:
Sitting or standing for extended periods can be particularly uncomfortable for individuals with lumbar facet syndrome. Prolonged sitting compresses the lumbar spine, exacerbating pain, while standing for long durations increases the load on the facet joints. - Challenges with Physical Activities:
Activities that involve repetitive bending, heavy lifting, or high-impact movements, such as sports or physical labor, can worsen symptoms and lead to further functional impairment. This often results in a reduced ability to engage in work or recreational activities. - Sleep Disturbances:
Pain and stiffness in the lower back can make it difficult to find a comfortable sleeping position. This not only affects sleep quality but also contributes to fatigue and reduced energy levels throughout the day. - Reduced Mobility:
The combination of pain and muscle stiffness often limits mobility, making it challenging to move freely. This restriction can lead to compensatory movements, where other parts of the body are overused to compensate for the limitations in the lumbar region, potentially causing secondary pain or discomfort.
Psychosocial Impact of Functional Limitations:
The functional limitations associated with lumbar facet syndrome can extend beyond physical challenges. Chronic pain and reduced mobility often contribute to feelings of frustration, anxiety, and depression. Patients may avoid social or recreational activities due to fear of aggravating their symptoms, leading to social isolation and a diminished quality of life.
What Causes Lumbar Facet Syndrome? Aging, Trauma, Posture, and More
Facet syndrome, also known as facet osteoarthritis, is a painful condition that affects the small joints between the vertebrae of the spine, called facets. Several factors can contribute to the development of this syndrome. First of all, aging is a key element, because over time the facet joints undergo natural wear and tear, leading to cartilage degeneration. Repetitive or excessive movements of the spine may also play an important role, particularly in individuals involved in demanding physical activities or exposed to prolonged postural stress.
Additionally, previous injuries, such as spinal sprains or fractures, can contribute to the development of facet syndrome. These traumas can alter the structure of the facets and lead to degenerative changes. Chronic poor posture, often linked to sedentary lifestyle habits or prolonged office work, can also increase the risk of developing this syndrome. Indeed, prolonged sitting can exert excessive pressure on the spinal facets, thus promoting their premature wear.
Furthermore, genetic factors may also play a role in the predisposition to facet syndrome. Some people may be genetically more prone to developing joint abnormalities or early cartilage degeneration. Additionally, muscular imbalances or weakness in the stabilizing muscles of the spine can place increased stress on the facets, contributing to facet osteoarthritis.
- Natural wear and tear (Osteoarthritis): Natural aging and wear of the facet joints over time is one of the main causes of lumbar facet syndrome. As we age, the cartilage that covers the joints can deteriorate, leading to increased friction between the joint surfaces.
- Trauma: Trauma such as car accidents, falls, or other injuries can damage the facet joints and contribute to the development of lumbar facet syndrome.
- Poor posture: Improper posture or repetitive movements can put excessive pressure on the facet joints, contributing to their premature wear.
- Overweight: Excess weight can lead to increased pressure on the joints of the lumbar spine, thus promoting the development of facet osteoarthritis.
- Genetic Factors: Some individuals may have a genetic predisposition to developing joint problems, including lumbar facet syndrome.
- Structural Defects: Congenital structural abnormalities of the spine may also contribute to the development of this syndrome.
Diagnosing Lumbar Facet Syndrome: Clinical Signs, Imaging, and Testing
Diagnosing lumbar facet syndrome involves a comprehensive evaluation that combines clinical examination, imaging techniques, and differential diagnoses. This multi-faceted approach ensures accurate identification of the condition, differentiating it from other causes of low back pain and guiding appropriate treatment strategies. By thoroughly assessing the symptoms, physical findings, and structural changes in the lumbar spine, healthcare providers can confirm the presence of lumbar facet syndrome and address its underlying causes.
Clinical Examination
The clinical examination forms the foundation of diagnosing lumbar facet syndrome. During this evaluation, the healthcare provider carefully reviews the patient’s medical history, symptoms, and physical condition to identify signs indicative of facet joint dysfunction.
Key Components of Clinical Examination:
- Patient History:
- The practitioner begins by gathering a detailed history of the patient’s symptoms, including the onset, duration, and nature of pain.
- Typical complaints include localized low back pain that worsens with extension, rotation, or prolonged sitting or standing.
- Patients may also describe stiffness, reduced mobility, and occasional radiating pain to the buttocks or upper thighs.
- Physical Examination:
- Palpation: Tenderness over the lumbar facet joints is a hallmark finding. Pressing on these joints often reproduces the patient’s pain, confirming the involvement of the facet joints.
- Range of Motion Tests: Movements such as backward bending (extension) or lateral rotation can elicit pain by increasing stress on the facet joints, further supporting the diagnosis.
- Postural Assessment: The provider evaluates spinal alignment and posture, identifying compensatory changes or abnormal curvatures (e.g., hyperlordosis) that may contribute to facet joint strain.
- Diagnostic Blocks:
- A common diagnostic tool involves injecting a local anesthetic into the affected facet joints or their innervating nerves (medial branch block).
- If pain is significantly reduced after the injection, it confirms that the facet joints are the primary source of discomfort.
Imaging Techniques
Imaging plays a crucial role in confirming the diagnosis of lumbar facet syndrome and assessing the extent of structural changes in the spine. It also helps exclude other potential causes of low back pain, such as herniated discs or spinal stenosis.
Commonly Used Imaging Modalities:
- X-Rays:
- X-rays are often the first imaging modality used to evaluate lumbar facet syndrome.
- They can reveal characteristic changes, such as narrowing of the joint space, osteophyte formation (bony growths), and subchondral sclerosis (increased bone density).
- Magnetic Resonance Imaging (MRI):
- MRI provides detailed images of soft tissues, including the cartilage, ligaments, and surrounding muscles.
- It is particularly useful for identifying inflammation, effusion (fluid accumulation), or cartilage degeneration within the facet joints.
- MRI can also detect associated conditions, such as nerve root compression or disc abnormalities, which may coexist with facet joint dysfunction.
- Computed Tomography (CT) Scans:
- CT scans offer a more detailed view of the bony structures of the facet joints, making them valuable for identifying subtle fractures, cysts, or advanced degeneration.
- CT imaging is often combined with myelography (contrast injection into the spinal canal) to better visualize nerve involvement.
- Ultrasound:
- While less commonly used, ultrasound can provide a dynamic assessment of the facet joints, particularly during movement.
- It is also a valuable tool for guiding facet joint injections or medial branch blocks.
Imaging findings alone are not definitive for diagnosing lumbar facet syndrome but are critical in confirming clinical suspicions and ruling out other conditions.
Differential Diagnosis: Distinguishing Facet Syndrome from Other Back Disorders
Differential diagnosis is essential to distinguish lumbar facet syndrome from other spinal disorders that present with similar symptoms. Misdiagnosis can lead to ineffective treatment and prolonged discomfort, making this step critical in the diagnostic process.
Conditions to Rule Out:
- Herniated Discs:
- Herniated discs can cause low back pain and radiating symptoms, but they are typically associated with nerve root compression, resulting in leg pain (sciatica) and neurological deficits like numbness or weakness.
- MRI is particularly helpful in differentiating herniated discs from facet joint dysfunction.
- Spinal Stenosis:
- Spinal stenosis involves the narrowing of the spinal canal, leading to nerve compression and symptoms such as pain, numbness, and weakness in the lower extremities.
- Unlike facet syndrome, pain from spinal stenosis often improves with forward bending and worsens with walking or standing.
- Sacroiliac Joint Dysfunction:
- The sacroiliac joints, located below the lumbar spine, can also cause low back pain.
- Pain from sacroiliac dysfunction is often felt lower in the pelvis and buttocks and may worsen with prolonged sitting or climbing stairs.
- Piriformis Syndrome:
- This condition involves compression of the sciatic nerve by the piriformis muscle, leading to buttock pain and sciatica-like symptoms.
- Physical examination and nerve conduction studies can help differentiate it from lumbar facet syndrome.
- Arthritis:
- Generalized arthritis or inflammatory conditions like ankylosing spondylitis can mimic lumbar facet syndrome by causing pain and stiffness in the lower back.
- Blood tests and imaging findings of systemic inflammation can aid in distinguishing these conditions.
- Myofascial Pain Syndrome:
- Trigger points in the lumbar or gluteal muscles can refer pain to the lower back and mimic facet syndrome.
- Palpation and muscle testing are essential to identify these patterns.
Osteopathic care offers a holistic, hands-on approach to managing lumbar facet syndrome. By focusing on restoring balance, mobility, and function in the lumbar spine, osteopathic manipulative treatment (OMT) targets the root causes of facet joint dysfunction. The cornerstone of this approach lies in the integration of structural and functional assessments to tailor treatments for individual patients. Through various manual techniques, osteopathy provides effective relief from pain, improves spinal alignment, and promotes long-term spinal health.
This section explores the key principles of osteopathic care for lumbar facet syndrome and highlights several techniques commonly used in practice.
Osteopathy for Lumbar Facet Syndrome: Hands-On Techniques That Restore Balance
Osteopathic care offers a holistic, hands-on approach to managing lumbar facet syndrome. By focusing on restoring balance, mobility, and function in the lumbar spine, osteopathic manipulative treatment (OMT) targets the root causes of facet joint dysfunction. The cornerstone of this approach lies in the integration of structural and functional assessments to tailor treatments for individual patients. Through various manual techniques, osteopathy provides effective relief from pain, improves spinal alignment, and promotes long-term spinal health.
This section explores the key principles of osteopathic care for lumbar facet syndrome and highlights several techniques commonly used in practice.
Key Principles of Osteopathic Care for Lumbar Facet Syndrome
Osteopathic treatment for lumbar facet syndrome is guided by several fundamental principles:
- The Body is an Integrated Unit:
Osteopathy views the body as a cohesive whole, where dysfunction in one area can influence others. For lumbar facet syndrome, imbalances in the pelvis, sacrum, or thoracic spine may contribute to symptoms, necessitating a comprehensive treatment approach. - Self-Healing Mechanisms:
Osteopathy aims to activate the body’s innate ability to heal itself. By reducing joint irritation, improving circulation, and relieving tension, osteopathic care fosters an environment conducive to recovery. - Structure and Function are Interrelated:
Proper alignment and mobility of the lumbar spine are essential for its optimal function. Osteopathic techniques focus on correcting structural imbalances that lead to facet joint dysfunction. - Individualized Treatment:
Osteopathic care is tailored to each patient’s unique condition, taking into account their anatomy, symptoms, and lifestyle factors.
Osteopathic Techniques for Lumbar Facet Syndrome
Osteopathic care employs a variety of manual techniques to address lumbar facet syndrome. Each technique targets specific aspects of the condition, such as joint alignment, muscle tension, or fascia mobility. Below are some of the most commonly used techniques:
Myofascial Release (MFR)
Myofascial release focuses on reducing tension and restrictions within the fascia, the connective tissue surrounding muscles and joints. For lumbar facet syndrome, this technique targets the lumbar region to alleviate muscle tightness and improve mobility.
- Procedure: The osteopath applies gentle, sustained pressure to areas of fascial restriction, allowing the tissue to release and realign. Movements are slow and guided by the practitioner’s sense of resistance in the fascia.
- Benefits:
- Reduces muscle tension surrounding the facet joints.
- Improves blood flow and lymphatic drainage, reducing inflammation.
- Restores flexibility in the lumbar spine.
Muscle Energy Technique (MET)
MET is an active technique in which the patient performs specific muscle contractions against resistance provided by the osteopath. It is particularly effective for reducing joint dysfunction and restoring proper alignment.
- Procedure:
- The practitioner positions the lumbar spine near the edge of its restricted range of motion.
- The patient is instructed to perform a gentle isometric contraction while the practitioner provides resistance.
- This process is repeated several times to improve joint mobility.
- Benefits:
- Relieves muscle spasms and hypertonicity.
- Improves joint alignment and mobility.
- Enhances coordination between the facet joints and surrounding musculature.
Counterstrain Technique
The counterstrain technique is a gentle, passive approach that alleviates pain by positioning the affected joint or muscle in a shortened, relaxed state.
- Procedure:
- The practitioner identifies tender points in the lumbar region.
- The patient is positioned to minimize discomfort, and the position is held for 90 seconds to allow the muscle to reset.
- Benefits:
- Relieves pain and muscle tension.
- Reduces inflammation around the facet joints.
- Promotes relaxation and improved range of motion.
Functional Technique
The functional technique is a subtle, hands-on approach that gently guides the lumbar spine through its natural movement patterns to reduce restrictions.
- Procedure:
- The osteopath monitors the joint’s motion and applies gentle adjustments to restore its normal range.
- Benefits:
- Improves coordination and mobility in the lumbar spine.
- Addresses both structural and functional imbalances.
Integrating Osteopathy into a Comprehensive Care Plan
While osteopathic techniques are highly effective, they are often integrated into a broader treatment plan that includes lifestyle modifications, exercise programs, and postural training. For lumbar facet syndrome, the following recommendations enhance the benefits of osteopathic care:
- Core Strengthening Exercises: Strengthening the core muscles provides better support for the lumbar spine and reduces the load on the facet joints.
- Postural Awareness: Maintaining proper posture during activities can prevent excessive stress on the lumbar region.
- Ergonomic Adjustments: Modifying workstations and daily habits helps reduce repetitive strain on the spine.
Osteopathic Insights: Evidence-Based Benefits for Treating Lumbar Facet Syndrome
- Grolaux, P. (1995).
- “Work Recovery in Response to Osteopathic Treatment After Hemilaminectomy for Lumbar Disc Herniation.”
- Summary: Explores the role of osteopathic manipulative treatment (OMT) in facilitating recovery from lumbar surgeries. It highlights improved joint function and reduced pain.
- Read PDF
- Hepburn, S.E. (2000).
- “The Relative Effectiveness of Non-Steroidal Anti-Inflammatory Medication vs. OMT in Cervical Facet Syndrome.”
- Summary: Compares the benefits of OMT and traditional medication, concluding that osteopathic interventions provide superior pain relief and mobility improvement.
- Read PDF
- Chemeris, N. (2007).
- “Prevalence and Recovery Rates in Osteopathic Practice for Back Pain.”
- Summary: Reports high recovery rates for lumbar pain patients treated with OMT, emphasizing its effectiveness in alleviating facet-related discomfort.
- Read PDF
- American Osteopathic Association (2016).
- “Guidelines for OMT for Low Back Pain.”
- Summary: Establishes evidence-based protocols for OMT application, highlighting its efficacy in managing lumbar facet syndrome.
- Read PDF
- Martí-Salvador, M., et al. (2018).
- “Osteopathic Manipulative Treatment Improves Chronic Low Back Pain.”
- Summary: Demonstrates that diaphragm-focused OMT techniques alleviate chronic pain and enhance spinal mobility in patients with facet syndrome.
- Read Article
- Frantzis, E., et al. (2014).
- “The Accuracy of Osteopathic Manipulations of the Lumbar Spine.”
- Summary: Highlights the precision of OMT in targeting lumbar facet joints, achieving significant reductions in pain and functional limitations.
- Read PDF
- Roberts, A., et al. (2022).
- “Osteopathic Manipulative Medicine: Hands-On Therapeutic Approaches.”
- Summary: Reviews various OMT methods, emphasizing their effectiveness for lumbar facet syndrome through holistic pain relief.
- Read PDF
- Kennard, E. (2011).
- “The Effects of Flexion Distraction on Segmental Mobility in Lumbar Facet Syndrome.”
- Summary: Explores how osteopathic flexion-distraction therapy improves spinal mobility and reduces facet-related pain.
- Read Study
- Williams, N.H. (2004).
- “Effectiveness of Primary Care-Based Osteopathy Clinics for Spinal Pain.”
- Summary: Concludes that osteopathic treatment offers significant pain reduction and mobility improvements in lumbar spine disorders.
- Read Study
- Rana, P. (2022).
- “Back Pain: Facet Syndrome and the Role of Osteopathy.”
- Summary: Highlights how OMT restores facet joint alignment and relieves chronic pain through manual manipulation techniques.
- Read Article
Preventing and Managing Lumbar Facet Syndrome: Posture, Movement, and Lifestyle
Preventing and managing lumbar facet syndrome involves adopting proactive measures that minimize stress on the lumbar spine and support overall spinal health. A comprehensive approach combines postural awareness, targeted exercises, and lifestyle modifications to prevent symptom recurrence, enhance mobility, and improve quality of life. These strategies are not only crucial for individuals at risk but also for those already experiencing symptoms, as they help maintain spinal stability and reduce the progression of facet joint degeneration.
Postural Awareness and Ergonomics
Maintaining proper posture and employing ergonomic strategies are essential for preventing undue stress on the lumbar spine and its facet joints. Poor posture, prolonged sitting, and repetitive movements are common contributors to lumbar facet syndrome, making postural awareness a key aspect of prevention and management.
Postural Awareness
- Proper Alignment: Keeping the spine in a neutral position during activities minimizes strain on the lumbar region. This involves aligning the ears, shoulders, and hips in a straight line.
- Avoiding Overextension: Movements that excessively arch the lower back can increase pressure on the facet joints. Awareness of this risk is important during activities like lifting or bending.
- Dynamic Sitting: Prolonged sitting should be avoided, especially in slouched positions. Taking regular breaks to stand, stretch, or walk helps maintain spinal health.
Ergonomic Adjustments
- Workstation Setup: Ensure that chairs, desks, and monitors are adjusted to promote proper posture. The feet should rest flat on the floor, and the back should be supported.
- Lifting Techniques: Use proper body mechanics when lifting heavy objects. Bend at the knees rather than the waist, and hold objects close to the body to reduce lumbar strain.
- Sleeping Posture: Sleeping on the back or side with proper lumbar support, such as a pillow under the knees or between the legs, reduces nighttime stress on the spine.
Postural awareness and ergonomic strategies not only prevent lumbar facet syndrome but also relieve stress on the joints, reducing pain and discomfort for those already affected.
Exercise and Strengthening
Regular exercise and muscle strengthening are critical components of both prevention and management. Targeted exercises improve spinal stability, increase flexibility, and reduce the likelihood of facet joint dysfunction.
Strengthening Exercises
- Core Stability Training: Strengthening the abdominal and back muscles provides better support for the lumbar spine, reducing the load on the facet joints. Examples include planks, bridges, and bird-dog exercises.
- Glute and Hip Strengthening: Strengthening the gluteal and hip muscles enhances pelvic stability and reduces compensatory stress on the lumbar region.
- Resistance Training: Light resistance exercises for the lower back muscles promote endurance and support.
Flexibility and Mobility
- Stretching: Stretching the hip flexors, hamstrings, and lower back muscles improves flexibility and reduces tension in the lumbar region.
- Yoga and Pilates: These practices combine flexibility, strength, and mindfulness to promote spinal health. Specific poses, such as child’s pose and cat-cow stretch, target the lumbar spine and relieve tension.
Aerobic Activities
- Low-impact aerobic activities, such as swimming, walking, or cycling, enhance overall fitness without placing excessive strain on the lumbar spine.
Consistent exercise builds a resilient musculoskeletal system, reducing the likelihood of future injuries or flare-ups of lumbar facet syndrome.
Lifestyle Modifications
Making lifestyle changes is an integral part of managing lumbar facet syndrome and preventing its recurrence. These modifications address factors such as body weight, activity levels, and daily habits that influence spinal health.
Weight Management
- Excess body weight increases pressure on the lumbar spine and facet joints. Maintaining a healthy weight through a balanced diet and regular exercise reduces this load and prevents joint degeneration.
Activity Moderation
- Avoiding Repetitive Strain: Limit repetitive bending, twisting, or heavy lifting, which can exacerbate facet joint stress.
- Balanced Activities: Alternate between sitting, standing, and walking during the day to prevent overloading the lumbar spine.
Stress Reduction
- Chronic stress can contribute to muscle tension and exacerbate lumbar facet symptoms. Incorporating stress-reducing practices such as meditation, deep breathing, or progressive muscle relaxation helps maintain overall well-being.
Hydration and Nutrition
- Proper hydration and a diet rich in anti-inflammatory foods, such as fruits, vegetables, and omega-3 fatty acids, support joint health and reduce inflammation. Avoiding processed foods and excessive sugar intake can also help.
Avoiding Sedentary Habits
- Prolonged sedentary behaviors, such as sitting for long hours, can weaken the lumbar region and increase stiffness. Incorporating movement into daily routines, such as taking short walks or stretching breaks, helps maintain spinal flexibility.
Quitting Smoking
- Smoking has been linked to reduced circulation and impaired healing of spinal tissues. Quitting smoking improves blood flow and promotes spinal health.
Lumbar Facet Syndrome FAQ: Top 10 Questions Answered
1. What is facet syndrome?
Facet syndrome is a condition affecting the small joints (facet joints) located between and behind adjacent vertebrae in the spine. It occurs when these joints become inflamed, irritated, or degenerate, leading to pain, stiffness, and reduced mobility.
2. What causes facet syndrome?
Facet syndrome can result from various factors, including:
- Aging: Natural degeneration of the cartilage in the facet joints.
- Trauma: Injuries from accidents or repetitive strain.
- Poor posture: Prolonged improper positioning, such as slouching.
- Overuse: Repetitive movements or heavy lifting.
3. What are the symptoms of facet syndrome?
Common symptoms include:
- Localized pain in the lower back or neck.
- Stiffness, especially after prolonged rest.
- Pain that worsens with twisting, bending, or arching backward.
- Radiating pain to the buttocks or thighs (lumbar) or shoulders (cervical).
4. How is facet syndrome diagnosed?
Diagnosis involves:
- Medical history and physical examination: Identifying pain patterns and triggers.
- Imaging tests: X-rays, MRI, or CT scans to detect joint degeneration.
- Diagnostic blocks: Injections of anesthetic into the facet joints to confirm the source of pain.
5. Is facet syndrome the same as arthritis?
Facet syndrome can be caused by facet joint arthritis (osteoarthritis), which results from the degeneration of cartilage. However, facet syndrome may also arise from trauma, overuse, or inflammation without significant arthritic changes.
6. How is facet syndrome treated?
Treatment options include:
- Conservative care: Physical therapy, medications, and ergonomic adjustments.
- Interventional procedures: Facet joint injections or nerve blocks.
- Manual therapies: Osteopathic manipulative treatment (OMT) and chiropractic care.
- Surgical interventions: Rarely, procedures like rhizotomy or spinal fusion may be needed.
7. Can facet syndrome cause nerve compression or sciatica?
Facet syndrome does not typically compress nerves directly. However, inflammation or swelling around the facet joints can irritate nearby nerves, causing referred pain that mimics sciatica. Unlike true sciatica, facet-related pain rarely extends below the knee.
8. Is exercise safe for facet syndrome?
Yes, low-impact exercises are encouraged to improve mobility, strengthen supporting muscles, and reduce stress on the facet joints. Recommended activities include walking, swimming, yoga, and targeted core-strengthening exercises.
9. Can facet syndrome be prevented?
Prevention involves minimizing strain on the spine through:
- Maintaining proper posture.
- Engaging in regular exercise to strengthen the core and back muscles.
- Avoiding prolonged sitting or repetitive heavy lifting.
- Using ergonomic furniture and techniques.
10. What is the long-term outlook for facet syndrome?
With early diagnosis and proper management, most individuals can effectively manage symptoms and maintain mobility. Long-term prognosis depends on consistent care, including lifestyle changes, exercise, and appropriate medical interventions. Severe cases may require ongoing treatment to prevent flare-ups or progression.
What X-Rays Reveal: Imaging Clues of Lumbar Facet Joint Degeneration
Radiographic signs of lumbar facet syndrome are often key indicators for the diagnosis of this condition. Medical imaging, such as x-rays, can reveal specific alterations in the facet joints of the lumbar spine. One of the characteristic signs is the presence of osteophytes, also called parrot beaks. These bony growths can form around facet joints in response to cartilage degeneration, contributing to compression of surrounding structures.
A decrease in the interarticular space, observable on radiographs, is another common radiographic sign of lumbar facet syndrome. This reduction in space between facet joints often indicates cartilage loss and may be associated with increased stress on the joints, thereby contributing to painful symptomatology.
Possible joint subluxations, where the joint surfaces are not aligned correctly, can also be identified on x-rays. These subluxations can result from wear and aging of the facet joints, contributing to instability and irritation of surrounding structures.
Furthermore, x-rays can reveal possible enlargements of the facet joints, indicating hypertrophy or inflammation of the joints. These morphological changes can be important clues in the diagnosis of lumbar facet syndrome, highlighting degenerative changes in the joints.
- Enlargement of the facet joints: On x-rays, enlargement of the facet joints can sometimes be seen, indicating a degenerative or inflammatory reaction.
- Osteophyte Formation: Bony growths, called osteophytes, can form around facet joints in response to degeneration. These osteophytes may be visible on x-rays.
- Narrowing of the intervertebral space: Degeneration of the facet joints can cause narrowing of the space between the vertebrae, which can be seen on x-rays.
- Spondylosis: Spondylosis is a term used to describe osteoarthritis of the spine. Signs of spondylosis, such as degenerative changes in joints and discs, may be visible.
- Sculpture of the joint margins: Radiographs may show changes in the shape or sculpture of the facet joint margins, indicating degenerative changes.
- Spinal instability: In some cases, x-rays may reveal signs of spinal instability, such as one vertebra sliding over another (spondylolisthesis).
Living with Lumbar Facet Syndrome: Long-Term Outlook and Recovery Pathways
Lumbar facet syndrome is a manageable condition, but its long-term prognosis depends on early intervention, consistent management, and lifestyle modifications. While acute cases often respond well to treatment, chronic pain associated with facet joint dysfunction can require ongoing care. By addressing the root causes of the condition and adopting sustainable strategies for pain management and relief, patients can significantly improve their quality of life and maintain long-term spinal health.
Managing Chronic Pain
Chronic pain is a common challenge for individuals with lumbar facet syndrome, especially if the condition has progressed or been left untreated. Effective management requires a combination of medical, physical, and self-care approaches tailored to the patient’s specific needs.
Medical Interventions
- Pain Medications:
- Over-the-counter (OTC) analgesics like acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs) can reduce inflammation and provide short-term relief.
- For persistent pain, a physician may prescribe muscle relaxants or stronger medications like corticosteroids for targeted pain management.
- Facet Joint Injections and Nerve Blocks:
- These interventional procedures involve injecting a local anesthetic and anti-inflammatory agent directly into the affected facet joint or its surrounding nerves.
- If successful, injections not only alleviate pain but also confirm the facet joint as the pain source.
- Radiofrequency Ablation (RFA):
- For patients with chronic pain that does not respond to other treatments, RFA can offer longer-term relief. This procedure uses heat to disrupt nerve signals, effectively reducing pain for months or even years.
Physical Therapy and Rehabilitation
- Physical therapy focuses on improving mobility, reducing stiffness, and strengthening the muscles supporting the lumbar spine. Therapists often design customized programs that combine stretching, strengthening, and manual therapies to address chronic pain.
- Core stabilization exercises are particularly effective in reducing the mechanical stress on the facet joints.
Psychological Support
- Chronic pain often affects mental health, leading to anxiety, depression, or a diminished sense of well-being. Techniques such as cognitive-behavioral therapy (CBT) or mindfulness-based stress reduction (MBSR) can help patients cope with the emotional impact of chronic pain.
Strategies for Sustained Relief
Sustained relief from lumbar facet syndrome requires a proactive approach that combines lifestyle changes, self-care, and preventive strategies. These measures not only reduce the risk of flare-ups but also support overall spinal health and mobility.
1. Consistent Exercise and Core Strengthening
- Low-Impact Aerobic Activities: Engaging in activities like swimming, walking, or cycling improves circulation, enhances joint mobility, and reduces inflammation.
- Core and Lumbar Strengthening: Regularly performing exercises that strengthen the core and lower back muscles reduces the mechanical stress on the facet joints. Planks, bridges, and bird-dog exercises are effective choices.
- Flexibility Training: Stretching routines, such as hamstring and hip flexor stretches, prevent muscle tightness and enhance range of motion in the lumbar region.
2. Postural Awareness and Ergonomic Adjustments
- Proper posture during daily activities and ergonomic workplace setups can significantly reduce stress on the lumbar spine.
- Simple changes, such as maintaining a neutral spine while sitting or using supportive cushions, can prevent unnecessary strain on the facet joints.
3. Weight Management and Nutrition
- Maintaining a healthy weight is crucial for reducing the load on the lumbar spine. Excess weight increases the mechanical stress on the facet joints, contributing to pain and degeneration.
- A diet rich in anti-inflammatory foods, such as fruits, vegetables, whole grains, and omega-3 fatty acids, supports joint health and reduces inflammation.
4. Stress Management Techniques
- Chronic stress can exacerbate muscle tension and amplify pain perception. Incorporating relaxation techniques like yoga, meditation, or deep breathing can help manage stress and promote relaxation.
- Regular massages or other bodywork therapies can also alleviate tension and improve circulation in the lumbar region.
5. Regular Osteopathic or Chiropractic Care
- Periodic osteopathic or chiropractic treatments help maintain spinal alignment and prevent joint dysfunction. These manual therapies address underlying imbalances, restore mobility, and reduce pain.
6. Adopting Preventive Habits
- Avoid activities that strain the lower back, such as heavy lifting or prolonged sitting without breaks.
- Incorporate movement into daily routines, taking short walks or stretching periodically to maintain flexibility and mobility.
7. Long-Term Maintenance Plans
- Developing a personalized maintenance plan with healthcare providers ensures that strategies for relief are consistent and effective. Regular follow-ups, adjustments to treatment plans, and periodic evaluations help identify and address any emerging issues.
References
- Bogduk N. Degenerative joint disease of the spine. Radiol Clin North Am. 2012 Jul;50(4):613-28. [ PubMed ]
- Grgić V. [Lumbosacral facet syndrome: functional and organic disorders of lumbosacral facet joints]. Lijec Vjesn. 2011 Sep-Oct;133(9-10):330-6. [ PubMed ]
- Marcia S, Masala S, Marini S, Piras E, Marras M, Mallarini G, Mathieu A, Cauli A. Osteoarthritis of the zygapophysial joints: efficacy of percutaneous radiofrequency neurotomy in the treatment of lumbarfacet joint syndrome. Clin Exp Rheumatol. 2012 Mar-Apr;30(2):314. [ PubMed ]
- Manchikanti L, Boswell MV, Singh V, Pampati V, Damron KS, Beyer CD. Prevalence of facet joint pain in chronic spinal pain of cervical, thoracic, and lumbar regions. BMC Musculoskelet Disord. 2004 May 28;5:15. [ PMC free article ] [ PubMed ]
- Kozera K, Ciszek B, Szaro P. Posterior Branches of Lumbar Spinal Nerves – part II: Lumbar Facet Syndrome – Pathomechanism, Symptomatology and Diagnostic Work-up. Ortop Traumatol Rehabil. 2017 Apr 12;19(2):101-109. [ PubMed ]
- Bogduk N. Functional anatomy of the spine. Handb Clin Neurol. 2016;136:675-88. [ PubMed ]
- Falco FJ, Manchikanti L, Datta S, Sehgal N, Geffert S, Onyewu O, Singh V, Bryce DA, Benyamin RM, Simopoulos TT, Vallejo R, Gupta S, Ward SP, Hirsch JA. An update of the systematic assessment of the diagnostic accuracy of lumbar facet joint nerve blocks. Pain Physician. 2012 Nov-Dec;15(6):E869-907. [ PubMed ]
- Boswell MV, Manchikanti L, Kaye AD, Bakshi S, Gharibo CG, Gupta S, Jha SS, Nampiaparampil DE, Simopoulos TT, Hirsch JA. A Best-Evidence Systematic Appraisal of the Diagnostic Accuracy and Utility of Facet (Zygapophysial) Joint Injections in Chronic Spinal Pain. Pain Physician. 2015 Jul-Aug;18(4):E497-533. [ PubMed ]
- Smuck M, Crisostomo RA, Trivedi K, Agrawal D. Success of initial and repeated medial branch neurotomy for zygapophysial joint pain: a systematic review. PM R. 2012 Sep;4(9):686-92. [ PubMed ]
- Bogduk N. On diagnostic blocks for lumbar zygapophysial joint pain. F1000 Med Rep. 2010 Aug 09;2:57. [ PMC free article ] [ PubMed ]
























{kind=link}