

Overview of Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is a neuropathy of the posterior tibial nerve associated with compression of structures within the tarsal tunnel. This syndrome has similarities to carpal tunnel syndrome of the wrist, although it is much less common.
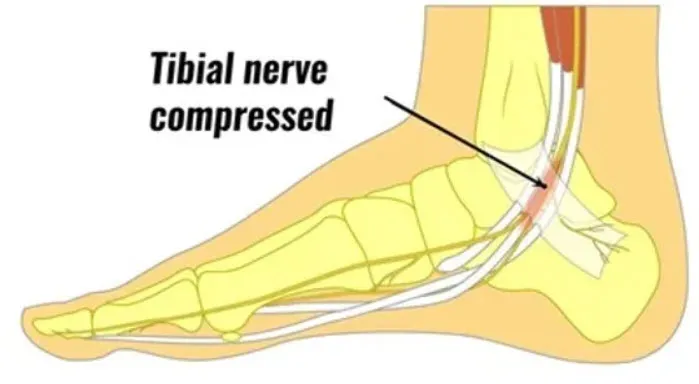
The tarsal tunnel, also called the tarsal canal, is located inside the ankle, behind the medial malleolus. It is formed by the surrounding bones and tissues, creating a space through which several structures pass, including the posterior tibial nerve. This nerve is responsible for the innervation of certain parts of the foot and the plantar flexor muscle.
When there is excessive compression in the tarsal tunnel, the posterior tibial nerve can be compressed, leading to tarsal tunnel syndrome. Causes of this compression can include trauma, foot deformity, tendon inflammation, or cysts.
Symptoms of tarsal tunnel syndrome typically include pain, numbness, tingling, or burning along the posterior tibial nerve, usually on the inner side of the ankle and foot. These symptoms may extend to the sole of the foot, arch, and toes. In more severe cases, muscle weakness in the foot may develop.
Diagnosis of tunneltarsal syndrome usually involves a thorough physical examination, nerve conduction tests, and possibly imaging tests such as X-rays or MRI to evaluate the structure of the tunnel.
Treatment of tarsal tunnel syndrome may include conservative approaches such as rest, foot elevation, ice application, and use of appropriate footwear. Orthotics or insoles may also be recommended to relieve pressure on the nerve. In more severe cases or those resistant to conservative treatment, surgery to release the nerve compression may be considered.
It is essential to consult a healthcare professional for an accurate diagnosis and appropriate treatment plan if tarsal tunnel syndrome is suspected.
Anatomy and function of the tarsal canal
- Location: The tarsal tunnel is located inside the ankle, on the inner (medial) side. It is formed by the bones of the foot, including the navicular bone, calcaneus, and medial tarsal bones.
- Contents: Important structures that pass through the tarsal tunnel include:
- Posterior tibial nerve: This is the most commonly affected element in tarsal tunnel syndrome. The posterior tibial nerve divides into branches that provide sensation and muscle control to the sole of the foot.
- Arteries and veins: Blood vessels that supply blood to the foot also pass through the tarsal tunnel.
- Ligaments: The tarsal tunnel is reinforced by several ligaments that maintain the stability of the ankle. These ligaments play an important role in preventing deformation of the tunnel and compression of the structures inside.
- Soft tissues: Soft tissues surrounding the tarsal tunnel, such as tendons from surrounding muscles, can also influence posterior tibial nerve compression.
- Anatomical variations: Anatomical variations, such as congenital deformities, flat feet, or excessive pronation, may contribute to nerve compression in the tarsal tunnel.
Common causes and risk factors
Tarsal tunnel syndrome, a painful foot condition, originates from compression of the posterior tibial nerve as it passes through the tarsal tunnel, a structure formed by the bones of the foot. The causes of this syndrome can be varied, often related to anatomical factors, trauma, mechanical disorders, or underlying diseases.
A common cause of tarsal tunnel syndrome is foot anatomy, including variation in bone structure. Some individuals have a naturally narrower tarsal tunnel, increasing the likelihood of nerve compression. Similarly, variations in the shape of the bones in the foot can create uneven pressure points on the posterior tibial nerve, contributing to the development of the syndrome.
Trauma, such as sports injuries or foot fractures, can also lead to tarsal tunnel syndrome. When there is injury to the foot, it can cause swelling and changes in the dynamics of the surrounding tissues, compressing the posterior tibial nerve.
Mechanical disorders of the foot can play a significant role in the development of tarsal tunnel syndrome. Flat feet, for example, can create instability that can lead to increased pressure on the nerve. Similarly, excessive pronation of the foot, where the ankle rolls inward, can contribute to compression of the posterior tibial nerve.
Wearing improper shoes, especially those that are too narrow or do not provide adequate support, can worsen tarsal tunnel syndrome. Shoes that compress the feet or put excessive pressure on the tarsal tunnel area can contribute to nerve compression, making symptoms worse.
Repetitive impact activities, such as running, can also be a potential cause of tarsal tunnel syndrome. Repetitive movements and constant stress on the foot can lead to inflammation of the tissues, putting increased pressure on the posterior tibial nerve.
Certain underlying medical conditions can increase the risk of developing tarsal tunnel syndrome. People with diabetes, for example, are more likely to develop peripheral nerve problems, increasing the risk of nerve compression. Similarly, arthritis in the foot region can contribute to changes in bone structure, putting pressure on the posterior tibial nerve.
It is essential to note that several factors can interact to cause tarsal tunnel syndrome. A combination of several causes, such as predisposing anatomy, previous trauma, and mechanical disorders, can lead to the development of this painful condition.
- Trauma: Traumatic injuries, such as ankle sprains, fractures, or soft tissue damage around the tarsal tunnel, can result in compression of the posterior tibial nerve.
- Arthritis: Some forms of arthritis, including rheumatoid arthritis, can cause inflammation of the ankle joints, which can lead to nerve compression.
- Anatomical deformities: Anatomical abnormalities, such as flat feet, excessive pronation (inward rolling) of the foot, or anatomical variations of the tarsal tunnel, may contribute to nerve compression.
- Tumors: Although rare, tumors or cysts near the tarsal tunnel can put pressure on the posterior tibial nerve.
- Tendon swelling: Inflammation or swelling of the tendons surrounding the tarsal tunnel can also cause compression of the nerve.
- Systemic diseases: Systemic medical conditions such as diabetes, rheumatoid arthritis, or posterior compartment syndrome may increase the risk of developing tarsal tunnel syndrome.
- Repetitive activities: Activities that involve repetitive movements of the foot and ankle, such as running, can contribute to irritation and compression of the posterior tibial nerve.
Symptoms: Recognizing Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is characterized by a variety of symptoms that result from compression of the posterior tibial nerve as it passes through the tarsal tunnel, located inside the ankle and foot. Symptoms can be progressive and vary in intensity, but they typically present with painful and uncomfortable sensations.
One of the most common symptoms is pain along the posterior tibial nerve, which runs from the lower leg to the sole of the foot. This pain can feel like a burning, tingling, or electric shock sensation. It can occur intermittently, often exacerbated by activities that involve flexion or inversion of the foot, such as walking, running, or even just standing for long periods of time.
Individuals with tarsal tunnel syndrome may also experience a shooting or burning pain along the arch of the foot, sometimes radiating to the toes. This pain may be worse at night, disrupting the affected person’s sleep.
Another common symptom is a feeling of swelling or warmth in the ankle and foot. Although visible swelling is less common than in other conditions, the person may notice an increase in the size of their foot due to the accumulation of fluids caused by the inflammation.
Symptoms of tarsal tunnel syndrome also include loss of sensation or numbness in the sole of the foot. Individuals may experience tingling or pins and needles, often concentrated in the inner part of the foot. These abnormal sensations may extend to the toes, affecting the overall sensation of the area.
Muscle weakness in the foot and ankle may be an associated symptom of tarsal tunnel syndrome. Muscles controlled by the posterior tibial nerve may be affected, resulting in decreased strength and stability. This may manifest as difficulty walking properly or lifting the toes.
Symptoms of tarsal tunnel syndrome may gradually worsen over time, especially if nerve compression persists without treatment. They may also fluctuate depending on daily activities and foot position, for example, worsening while walking and decreasing while resting.
It is important to note that the symptoms of tarsal tunnel syndrome can be similar to those of other foot conditions, such as plantar fasciitis or peripheral neuropathy. Therefore, an accurate diagnosis requires a thorough medical evaluation, often supplemented with medical imaging tests such as X-rays or MRIs.
- Pain: Pain is one of the most common symptoms. It is often described as a shooting, burning or tingling pain on the inside of the ankle and foot.
- Numbness and tingling: Patients may experience numbness, tingling, or pins and needles sensations along the posterior tibial nerve, which may radiate to the sole of the foot.
- Muscle weakness: Some individuals may experience muscle weakness in the foot, which can cause difficulty lifting the toes or performing normal foot movements.
- Night pain: Symptoms, especially pain, may be worse at night, disrupting sleep.
- Swelling: Mild swelling of the ankle may sometimes accompany tarsal tunnel syndrome.
- Change in gait: Due to pain and muscle weakness, people with the condition may change the way they walk to reduce pressure on the affected area.

Diagnostic methods
Diagnostic methods for tarsal tunnel syndrome are based mainly on clinical assessment and additional examinations. Here is an overview of the main diagnostic methods used:
1. Clinical examination:
Physical examination is the first step in diagnosis. The physician asks the patient about symptoms, including pain, numbness, tingling, or burning in the ankle and foot area. The physician also looks for characteristic clinical signs, such as pain when palpating the tarsal tunnel or when plantar flexing the foot. The Tinel test , which involves gently tapping the tibial nerve to elicit painful symptoms, is often used. A positive response (pain radiating to the foot) may indicate compression of the tibial nerve in the tarsal tunnel.
2. Ultrasound:
Ultrasound is used to evaluate the anatomical structures of the tarsal canal, including tendons, nerves, and blood vessels. It can identify abnormalities such as ganglia, cysts, or tendinopathies, which could be putting pressure on the tibial nerve. It is noninvasive, quick, and often used as a first-line scan to visualize the anatomy of the foot and ankle.
3. Electromyography (EMG):
EMG is a common technique in the diagnosis of compressive neuropathies such as tarsal tunnel syndrome. It is used to assess the electrical activity of the muscles and detect any nerve involvement. This test is useful in determining the degree of compression of the tibial nerve and can help distinguish nerve compression at the tarsal tunnel from more proximal involvement, such as lumbar radiculopathy.
4. Magnetic resonance imaging (MRI):
MRI is a method of choice for visualizing the soft tissues around the tarsal canal. It allows for a thorough evaluation of the structures of the foot and can identify underlying causes of nerve compression, such as tendon injuries, varicose veins, or tumors. MRI is often used if other noninvasive tests, such as ultrasound, are inconclusive or to plan surgery.
5. Nerve conduction studies:
These tests measure the speed at which electrical signals travel along the nerves in the foot. A decrease in nerve conduction speed may indicate compression or dysfunction of the tibial nerve. This type of test is often used in conjunction with EMG to confirm the diagnosis.
6. X- rays:
Although X-rays cannot directly visualize nerves, they can be used to rule out other causes of foot pain and dysfunction, such as fractures or bone abnormalities. X-rays can also show indirect signs of compression, such as a tarsal tunnel deformity.
Pathophysiology
The pathophysiology of tarsal tunnel syndrome involves compression of the posterior tibial nerve as it passes through the tarsal tunnel, an anatomical structure located inside the ankle. This tunnel is formed by the bones and soft tissues that surround the nerve, and it allows the nerve to pass from the back of the leg to the sole of the foot.
When there is compression of the posterior tibial nerve, several pathological mechanisms can occur. Excessive pressure on the nerve can lead to inflammation, swelling and irritation of the nerve tissue. This can gradually cause symptoms such as pain, tingling, numbness and weakness in the region of the foot and ankle innervated by the posterior tibial nerve.
Factors that contribute to the pathophysiology of tarsal tunnel syndrome may include a variety of conditions such as edema (swelling), cyst formation, the presence of scar tissue, or degeneration of surrounding tendons. Nerve compression may be exacerbated by activities that increase pressure within the tarsal tunnel, such as wearing inappropriate footwear, participating in strenuous sports, or the presence of anatomical abnormalities.
The underlying pathophysiology often guides the choice of treatment options, whether through conservative approaches to reduce pressure on the nerve or, in some cases, surgical interventions to release the compression. An accurate diagnosis and a thorough understanding of the specific pathophysiology of each case are essential to developing an effective treatment plan.
Differential diagnosis of tarsal tunnel syndrome
- Plantar fasciitis: Inflammation of the plantar fascia, the connective tissue on the bottom of the foot, can cause heel and arch pain.
- Tarsal tunnel syndrome: This is a condition similar to TTS, but with compression of the anterior tibial nerve in the midfoot region.
- Morton’s neuroma: A thickening of the interdigital nerve, usually between the third and fourth toes, can cause pain, tingling, and numbness.
- Arthritis: Arthritis, especially rheumatoid arthritis, can affect the joints of the foot and cause pain and stiffness.
- Tendinitis: Inflammation of the tendons around the ankle, particularly the Achilles tendon, can cause pain in the heel and calf area.
- Stress Fracture: Stress fractures can occur in the bones of the foot and ankle, causing pain that may be similar to that of TTS.
- Lumbar Nerve Compression: Problems in the lumbar spine can sometimes manifest as symptoms in the foot.
- Infections: Local infections, such as abscess or foot infection, can cause pain and swelling
Conservative and surgical treatments
- Conservative treatments
Conservative treatments are preferred in the early stages of tarsal tunnel syndrome or when symptoms are moderate. They include:
a. Rest and activity modification
The first step is to reduce activities that exacerbate symptoms, such as prolonged walking or wearing improper footwear. Rest helps reduce inflammation around the tibial nerve.
b. Wearing Orthotics
Foot orthotics are often used to correct biomechanical imbalances such as flat feet, which can contribute to nerve compression. These custom-made devices redistribute pressure across the foot, reducing nerve irritation.
c. Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed to reduce inflammation and pain associated with tarsal tunnel syndrome. In some cases, corticosteroid injections may be given directly into the tarsal tunnel to reduce local inflammation and relieve pressure on the nerve.
d. Osteopathy
Osteopathy plays a complementary role in the management of tarsal tunnel syndrome. An osteopath can work on joint mobility, soft tissue relaxation, and improving circulation in the foot and ankle region. Manual techniques used in osteopathy, such as gentle joint mobilizations and myofascial release, can relieve tension in the tarsal tunnel and improve tibial nerve function. In addition, the osteopath can correct postural dysfunctions or structural imbalances, contributing to a holistic approach to healing.
- Surgical treatments
When conservative treatments fail to relieve symptoms or if nerve compression is severe, surgery may be considered.
a. Tarsal tunnel release
The most common operation is tarsal tunnel release. It involves decompressing the tibial nerve by incising the ligament that forms the roof of the tarsal tunnel. This frees the nerve and reduces the pressure on it. The procedure is usually performed on an outpatient basis under local or general anesthesia.
b. Resection of compressive masses
If a mass, such as a cyst or ganglion, is identified as the cause of the nerve compression, it may be removed during surgery to relieve pressure on the tibial nerve. This type of surgery is more complex, but is sometimes necessary when imaging studies show lesions in the tarsal canal.
c. Post-operative and rehabilitation
After surgery, a period of rest and rehabilitation is essential to ensure complete healing. Rehabilitation exercises are prescribed to restore strength, flexibility and function to the foot. Post-operative follow-up also includes care to minimize the risk of scarring and adhesions, which could compress the nerve again.
Rehabilitation and long-term management
Rehabilitation and long-term management of tarsal tunnel syndrome are essential steps to optimize recovery and prevent recurrence. Once the diagnosis has been made and treatment, whether conservative or surgical, has been initiated, it is crucial to implement appropriate rehabilitation to promote healing.
1. Objectives of rehabilitation
The main goal of rehabilitation is to restore mobility, reduce pain, and prevent further compression of the tibial nerve. It also aims to correct muscle imbalances and improve the strength and flexibility of the structures around the tarsal canal.
2. Stretching and strengthening exercises
Stretching exercises are essential to maintain flexibility in the muscles and tendons surrounding the ankle and foot. A physical therapist can prescribe specific calf and Achilles tendon stretching exercises, which can reduce pressure on the tarsal tunnel. Strengthening exercises are also necessary to stabilize the ankle and strengthen the muscles of the foot, helping to provide better arch support.
3. Mobilization and manual therapy
Joint mobilization and manual therapy techniques can be used to improve mobility of the ankle and surrounding soft tissues. These methods are particularly useful for reducing scar adhesions after surgery or for releasing compressed structures in the tarsal canal.
4. Orthotics and plantar supports
Foot orthotics are often recommended for patients with tarsal tunnel syndrome, especially if poor foot posture, such as flat feet or overpronation, is causing nerve compression. Custom orthotics help correct these imbalances and relieve pressure on the tibial nerve. They can be used as part of long-term management, even after the active rehabilitation phase has ended.
5. Complementary therapies
Other complementary therapies may be incorporated into rehabilitation, such as electrotherapy, ultrasound therapy, or shockwave therapy. These techniques can help reduce inflammation, improve blood circulation, and promote tissue healing.
6. Pain management
Pain management plays a central role in rehabilitation. In addition to physical therapies, methods such as applying ice or heat can be used to relieve discomfort. The use of analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs), may also be considered as an adjunct.
7. Prevention of recurrences
Long-term management also relies on preventing recurrences. Lifestyle changes, such as reducing aggravating activities, adopting appropriate footwear, and maintaining a routine of stretching and strengthening exercises, are essential. It is also important to avoid overloading the foot joints and monitor risk factors such as obesity or anatomical abnormalities.
Conclusion
Rehabilitation and long-term management of tarsal tunnel syndrome requires a multidimensional approach, combining exercises, manual therapies and lifestyle modifications to restore foot function and prevent relapse. Personalized and progressive management is essential to maximize the chances of full recovery.
FAQ about Tarsal Tunnel Syndrome
1. What is tarsal tunnel syndrome?
Tarsal tunnel syndrome is a compression neuropathy where the tibial nerve, located behind the ankle, is compressed inside the tarsal tunnel, causing pain, numbness and tingling in the foot.
2. What are the typical symptoms?
The main symptoms include pain, burning, numbness or tingling in the ankle, heel and sole of the foot. These sensations may be worse when walking or standing.
3. What are the causes of the syndrome?
Causes may include ankle injuries, flat feet, cysts, tendonitis, varicose veins, or fractures. Any factor that increases pressure in the tarsal tunnel can lead to this syndrome.
4. How is tarsal tunnel syndrome diagnosed?
Diagnosis is based on physical examination, including the Tinel test, and imaging tests such as MRI or ultrasound to visualize the tarsal tunnel and identify underlying causes of nerve compression. Electromyographic tests can also assess nerve function.
5. What conservative treatments are available?
Conservative treatments include rest, activity modification, foot orthotics to correct biomechanical abnormalities, physical therapy to strengthen ankle muscles, and anti-inflammatory medications to reduce inflammation. Osteopathy can also be used to improve mobility and reduce nerve pressure.
6. When is surgery necessary?
Surgery is considered when conservative treatments fail to relieve symptoms after several months or when compression is severe. Tarsal tunnel release, a procedure in which the ligament compressing the nerve is cut, is the most common surgical procedure.
7. What is the role of osteopathy in the treatment of the syndrome?
Osteopathy works in addition to traditional treatments by working on joint mobility, loosening soft tissues and improving circulation. It can help relieve tension around the tarsal canal and rebalance postural structures.
8. How long does rehabilitation last after surgery?
Rehabilitation after a tarsal tunnel release typically takes several weeks to a few months. Specific exercises are prescribed to restore strength and mobility, and to prevent adhesions that could compress the nerve again.
9. Can tarsal tunnel syndrome be prevented?
Prevention includes wearing proper footwear, maintaining a healthy weight, and avoiding activities that put excessive strain on the feet and ankles. Regular exercises to strengthen the ankle and foot muscles can also help reduce the risk of nerve compression.
10. Can tarsal tunnel syndrome come back after treatment?
Yes, there is a risk of recurrence, especially if underlying factors, such as biomechanical imbalances or pre-existing pathologies, are not corrected. Regular monitoring and management of risk factors are essential to avoid further nerve compression.
Conclusion
In conclusion, tarsal tunnel syndrome represents a neuropathy of the posterior tibial nerve due to compression of structures within the tarsal tunnel. Although less common than carpal tunnel syndrome, it can cause painful and uncomfortable symptoms in the ankle and foot region.
Early diagnosis and an appropriate treatment approach are essential to effectively manage tarsal tunnel syndrome. Conservative treatment options, such as rest, use of appropriate footwear, and orthotics, can often relieve symptoms. However, in some cases, surgery may be considered to release the nerve compression.
It is crucial for individuals experiencing symptoms to consult a healthcare professional to obtain an accurate diagnosis and develop a personalized treatment plan. By taking appropriate measures, it is possible to improve quality of life and prevent the progression of symptoms related to tarsal tunnel syndrome.
References
- Calvo-Lobo C, Painceira-Villar R, López-López D, García-Paz V, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME, Palomo-López P. Tarsal Tunnel Mechanosensitivity Is Increased in Patients with Asthma: A Case-Control Study. J Clin Med. 2018 Dec 12;7(12) [ PMC free article ] [ PubMed ]2.
- Stødle AH, Molund M, Nilsen F, Hellund JC, Hvaal K. Tibial Nerve Palsy After Lateralizing Calcaneal Osteotomy. Foot Ankle Spec. 2019 Oct;12(5):426-431. [ PubMed ]3.
- Zuckerman SL, Kerr ZY, Pierpoint L, Kirby P, Than KD, Wilson TJ. An 11-year analysis of peripheral nerve injuries in high school sports. Phys Sportsmed. 2019 May;47(2):167-173. [ PubMed ]4.
- Rinkel WD, Castro Cabezas M, van Neck JW, Birnie E, Hovius SER, Coert JH. Validity of the Tinel Sign and Prevalence of Tibial Nerve Entrapment at the Tarsal Tunnel in Both Diabetic and Nondiabetic Subjects: A Cross-Sectional Study. Plast Reconstruction Surg. 2018 Nov;142(5):1258-1266. [ PubMed ]5.
- Hong CH, Lee YK, Won SH, Lee DW, Moon SI, Kim WJ. Tarsal tunnel syndrome caused by an uncommon ossicle of the talus: A case report. Medicine (Baltimore). 2018 Jun;97(25):e11008. [ PMC free article ] [ PubMed ]6.
- Komagamine J. Bilateral Tarsal Tunnel Syndrome. Am J Med. 2018 Jul;131(7):e319. [ PubMed ]7.
- Schuh A, Handschu R, Eibl T, Janka M, Hönle W. [Tarsal tunnel syndrome]. MMW Fortschr Med. 2018 Apr;160(6):58-59. [ PubMed ]


















{kind=link}