

Lumbar degenerative disc disease is a common spinal condition that occurs when the intervertebral discs in the lumbar region begin to break down and lose their normal function.
Synonyms: Herniated disc or disc bulge, disc prolapse, herniated nucleus pulposis (HNP).
Introduction
Intervertebral discs are ring-shaped structures located between the vertebrae of the spine that act as shock absorbers and allow flexible mobility of the spine.
“At the Heart of the Spine: Understanding Lumbar Degenerative Disc Disease”
Lumbar degenerative disc disease, a reality that is often overlooked but affects many people, presents as a delicate condition affecting the lumbar region of the spine. This region, which supports a large part of the body’s weight and is constantly stressed in our daily activities, can undergo degenerative changes over time.
Understanding this complex condition requires a deeper look at the underlying mechanisms. Lumbar degenerative disc disease is characterized by the progressive degradation of the intervertebral discs, the natural cushions located between the vertebrae. These discs, responsible for shock absorption and flexibility of the spine, can lose their elasticity and ability to absorb stress, leading to a series of symptoms that can affect quality of life.
It is essential to demystify this condition by exploring the contributing factors, such as aging, genetics, trauma, and lifestyle habits. A thorough overview of lumbar degenerative disc disease provides insight into the warning signs, such as lower back pain, stiffness, and sometimes even radiation to the lower extremities. Understanding these symptoms provides a solid foundation for early intervention and effective management strategies.
Understanding lumbar degenerative disc disease is about uncovering the complex mechanisms at work in the spine while providing practical knowledge for proactive management of this condition. By navigating through this information, we aim to illuminate the path to relief, autonomy, and well-being for those facing the daily reality of lumbar degenerative disc disease.
Evolution of understanding of lumbar degenerative disc disease
The evolution of understanding of lumbar degenerative disc disease has been marked by advances in medicine, orthopedic research, and medical imaging. Here is a general overview of this evolution over time:
- Early 20th century: Early work on the spine and intervertebral discs began to develop. X-rays allowed doctors to visualize the spine and detect certain abnormalities.
- Mid-20th century: With the advent of more advanced imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI), researchers were able to examine the structure of intervertebral discs in more detail. This led to a better understanding of degenerative changes.
- Late 20th century: Epidemiological studies began to examine the prevalence of degenerative disc disease and identify associated risk factors. Genetic aspects of disc disease also began to be explored.
- Early 21st century: Advances in genomics and molecular biology have allowed a deeper understanding of the molecular mechanisms involved in degenerative disc disease. Researchers have become interested in biomarkers and potential treatments.
- Current Research: Research continues to explore more personalized approaches to the prevention and treatment of degenerative disc disease. Work is also underway to develop regenerative therapies to restore function to damaged discs.
It is important to note that degenerative disc disease is often considered a normal part of the aging process, and not all degenerative changes necessarily cause lower back symptoms or pain.
Stage of Deterioration
Disc degeneration is a normal process
With the natural aging process, the vertebral discs undergo a slow wear that causes characteristic changes. These alterations are mainly manifested at the level of the nucleus and the organization of the rings of the annulus fibrosus, as well as by the progressive disappearance of the cartilaginous plates. The discs located in the lumbar and cervical region are particularly subject to these changes.
As early as the age of 20, discernible transformations can occur within the lumbar discs. At this stage, the vascular supply of the disc may begin to be obstructed, with consequences for the nutrition of the disc itself. The posterior parts of the annulus fibrosus undergo compression and bulging, influenced by lumbar lordosis. These posterior annular fibers appear to be thinner and shorter than their anterior counterparts. The discs gradually adopt a wedge shape, becoming narrower at the back than at the front.
At the same time, the disc nucleus undergoes a gradual transformation from a gelatinous consistency to a fibrous structure. This development is accompanied by a reduction in the nucleus’ ability to retain water, while its collagen content increases. The total height of the disc gradually decreases, contributing to the narrowing of the disc space.
In summary, these morphological and structural changes in the spinal discs are an integral part of the natural aging process and can influence the health and function of the spine over time.
The posterolateral portion of the disc fibers weakens first.
Lumbar degenerative disc disease represents a complex and common medical problem, particularly prevalent with aging. A thorough understanding of the contributing factors can help clarify this condition.
A key element is associated with functional movements of the spine. These movements, involving a combination of flexion and diagonal rotation, impose specific constraints on the posterolateral part of the annular fibers of the intervertebral disc. At the same time, the more robust posterior longitudinal ligament accentuates the vulnerability of the thinner and lateral parts of the annulus.
Over time, repeated stresses can cause the posterolateral annular fibers to compress and deform, resulting in splits between the layers of the annulus. These splits can progress to radial and horizontal tears, allowing the disc nucleus to protrude into the annulus.
The annular fibers gradually lose their elasticity, generating tension on the external fibers. Associated with altered disc mechanics and the weight load on the spine, this promotes bone reinforcement on the outer edges of the vertebrae, leading to the formation of osteophytes in front and behind.
Between the ages of 40 and 50, although the discs can still absorb water, the nucleus undergoes a transformation into a fibrous material almost indistinguishable from the annular fibers. This leads to narrowing of the disc space and reduced range of motion, a phenomenon frequently observed in people aged 55 to 64.
Understanding these processes is essential to raise awareness of the changes that occur in the spine over time and to adopt appropriate prevention and management strategies.

- A disruption of the normal architecture of the disc (drying out) will eventually cause a crack.
- This crack weakens the annulus fibrosus (which has the role of retaining the nucleus)
- A severe fissure will result in migration of the nucleus or protrusion of the internal nucleus pulposus, possibly putting pressure on the spinal cord or nerve root and resulting in radiating pain and specific locations of weakness.
Just over 90% of disc herniations occur in the L4-L5 or L5-S1 disc space, which will impinge on the L4, L5 or S1 nerve root. This compression will produce radiculopathy (radiation) into the posterior leg and dorsal foot.
Factors causing disc deterioration
Drying of the disc with age
At birth, the intervertebral disc is made up of about 80% water, ensuring its flexibility and shock-absorbing function. However, with aging, this disc gradually loses water, which reduces its ability to absorb shocks and makes it less flexible. This loss of fluid also leads to a reduction in the thickness of the disc, thus narrowing the space between the vertebrae.
Over time, the dehydration process can cause microscopic tears or cracks in the outer layer of the disc, also called the annulus or capsule. These small lesions can lead to larger problems. Specifically, the gelatinous material inside the disc, known as the nucleus, can leak out through these tears or cracks in the capsule. This leakage can cause the disc to bulge, open (rupture), or even break into fragments, leading to problems such as herniated discs.
In short, the process of dehydration of the intervertebral disc, accompanied by the appearance of tears in its outer layer, contributes to the loss of its structural integrity and can lead to various complications related to the spine.

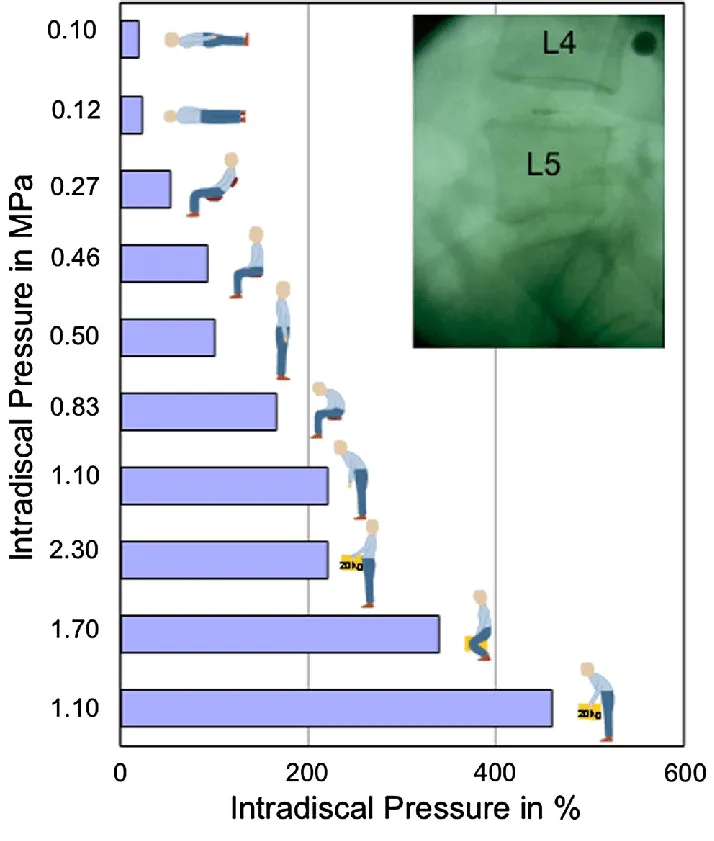
Mechanical load
Excessive or repetitive mechanical loads on the spine, such as lifting heavy loads incorrectly, can contribute to premature disc wear.
The spine, a fundamental pillar of the human body, is subjected to various stresses on a daily basis. One of the main sources of concern is the mechanical load to which it is exposed. Physical activities involving heavy lifting, performed incorrectly, can put excessive pressure on the spine, thus jeopardizing the long-term health of the lumbar region.
Intervertebral discs, crucial structures located between the vertebrae, play a vital role in shock absorption and spinal flexibility. However, when excessive mechanical loads are applied repetitively, these discs can experience unusual stresses. Improper lifting of heavy loads, for example, can cause excessive compression of the discs, putting them at increased risk of premature wear.
Wear and tear of the intervertebral discs can lead to various health problems, such as herniated discs, chronic lower back pain, and even neurological disorders in some severe cases. It is imperative to raise awareness of the importance of proper technique when lifting and to promote ergonomic practices to reduce the risk of mechanical load-related injuries.
Training programs on workplace safety and load handling can play a crucial role in preventing spinal health problems. Workers should be informed about good lifting practices, correct posture and the use of appropriate lifting equipment to minimize the risk of injury.
Bad posture
Prolonged poor posture, whether sitting or standing, can put excess pressure on the discs and contribute to their deterioration.
Posture plays a fundamental role in spinal health, and maintaining an incorrect position for long periods of time can have detrimental consequences on the spinal structure. When sitting, for example, a hunched forward posture can cause the lumbar vertebrae to become misaligned, putting increased pressure on the intervertebral discs.
When the spine is under constant pressure due to poor posture, the intervertebral discs can experience inappropriate stress. The excessive pressure can cause the discs to compress unevenly, promoting their premature deterioration. Similarly, poor posture while standing, such as leaning back excessively, can also contribute to similar problems.
The effects of poor posture are not limited to the intervertebral discs. They can also lead to muscle tension, chronic back pain and joint problems. It is essential to raise awareness about the importance of maintaining proper posture, whether at work, at home or in other daily contexts.
Using ergonomics, such as appropriate office chairs and adjustable workstations, can help promote proper posture. Taking regular breaks to stretch and adjust position can also help prevent the negative effects of prolonged posture.
In summary, poor posture, whether adopted while sitting or standing, can put excessive pressure on the intervertebral discs, contributing to their deterioration. Being aware of postural habits, using ergonomic equipment and taking regular breaks to encourage proper movement are important measures to maintain long-term spinal health.
Smoking
Smoking is closely associated with adverse effects on spinal health, particularly in relation to the deterioration of intervertebral discs. One of the mechanisms by which smoking exerts its negative impact is related to a decrease in blood flow to the discs.
The nicotine in tobacco acts as a vasoconstrictor, meaning it causes blood vessels to narrow. As a result, this vasoconstriction reduces blood flow to the structures of the spine, including the intervertebral discs. These discs depend on adequate blood flow to receive essential nutrients and oxygen needed for their health and optimal function.

Decreased blood flow compromises the discs’ ability to maintain hydration and elasticity. These factors are crucial for ensuring shock absorption and spinal flexibility. Without adequate nutrition, discs can become more vulnerable to premature wear and deterioration.
Therefore, individuals who smoke are more likely to experience intervertebral disc problems, such as herniated discs, chronic lower back pain, and other spinal complications. Smoking cessation can play a crucial role in maintaining disc health by improving blood flow and promoting better nutrition to these essential spinal structures.
Specific professional activities
- Jobs involving repetitive motions: Example: Supermarket checkout operator Why: Checkout operators perform repetitive motions of scanning, scanning, and bagging items. This constant repetition can lead to premature wear of the discs by putting continuous pressure on the spine, especially in the lumbar region.
- Jobs with constant vibration: Example: Construction equipment operator Why: Construction equipment operators are exposed to constant vibrations from the heavy machinery they operate. These vibrations can put stress on the spine, contributing to disc deterioration over time.
- Jobs involving awkward positions: Example: Plumber working in tight spaces Why: Plumbers may be required to work in awkward or awkward positions, such as bending or twisting to access pipes in tight spaces. These prolonged positions can put uneven pressure on the spinal discs, increasing the risk of damage.

Each of these examples highlights how specific occupational activities can contribute to disc deterioration due to repetitive movements, constant vibration, or awkward positions that place excessive stress on the spine. It is essential for workers in these occupations to take ergonomic precautions, take regular breaks to change posture, and use appropriate protective equipment to minimize the risk of spinal problems.
Psychological Stress
Psychological stress, whether related to work, personal relationships, or other aspects of life, can have a significant impact on spinal health, particularly when it comes to spinal disc problems. The link between stress and disc deterioration can be explained in several ways:
- Increased muscle tension: Chronic stress can cause increased muscle tension, especially in the back area. Tight muscles can put extra pressure on the spine, including the intervertebral discs, contributing to their premature wear.
- Changes in pain perception: Stress and anxiety can influence how a person perceives pain. High levels of stress can make a person more sensitive to pain, even at normally tolerable levels. This can worsen the perception of symptoms related to spinal disc problems.
- Increased inflammation: Chronic stress can trigger inflammatory responses in the body. Increased inflammation can negatively affect the tissues surrounding the intervertebral discs, increasing the risk of complications and deterioration.
- Bad habits related to stress: In response to stress, some people adopt unhealthy habits such as prolonged sitting in uncomfortable positions or lack of exercise. These habits can contribute to disc deterioration.
- Impact on sleep behaviors: Stress can also influence sleep patterns, sometimes leading to poor quality sleep. Insufficient rest can compromise the ability of discs to regenerate during the night.
Thus, stress management can play a crucial role in preventing spinal disc problems. Stress management techniques, such as meditation, relaxation, exercise, and psychological support, can help reduce the impact of stress on spinal health and help maintain disc functionality.
Aging
Aging is an inevitable factor that has a significant impact on the health of the intervertebral discs, essential structures of the spine. This natural process is characterized by a progressive degeneration of the discs over time. Several changes associated with aging contribute to the deterioration of the intervertebral discs:
- Loss of elasticity: With age, the intervertebral discs lose their natural elasticity. This loss of elasticity compromises their ability to absorb shocks and stresses exerted on the spine on a daily basis.
- Decreased water content: Intervertebral discs are composed primarily of water. Over the years, this water content tends to decrease, leading to dehydration of the discs. Less hydration reduces their ability to maintain the suppleness and flexibility needed to ensure adequate spinal mobility.
- Disc collapse and loss of height: Disc degeneration can lead to collapse and loss of height. This can cause adjacent vertebrae to move closer together, increasing the risk of disc friction and compression.
- Formation of cracks and tears: Over time, cracks and tears can form in the structure of the discs, compromising their integrity and ability to function optimally.
- Decreased regenerative capacity: The cells in the intervertebral discs have a limited ability to regenerate. With age, this regenerative capacity decreases, making the discs more vulnerable to damage and deterioration.
These aging-related changes are normal, but they can contribute to a variety of spinal health issues, such as herniated discs, lower back pain, and decreased mobility. While aging is inevitable, adopting healthy lifestyle habits, maintaining regular physical activity, and following back care practices can help mitigate some of the negative effects of aging on spinal disc health.
Bad Lifting Habits
Poor lifting habits are a significant risk factor for spinal health, particularly when it comes to disc deterioration. Lifting objects incorrectly, without using proper techniques, can put excessive pressure on the spine, putting disc health at risk. Here’s how these habits can contribute to disc deterioration:
- Improper load on the spine: Lifting objects incorrectly can result in uneven distribution of the load on the spine. This can lead to excessive compression of the intervertebral discs, especially in the lumbar region, increasing the risk of injury and deterioration.
- Stress on muscles and ligaments: Improper lifting technique can place excessive stress on the muscles and ligaments that support the spine. This can lead to muscle strains, microtraumas and ligament tears, affecting spinal stability.
- Spinal Twisting: Twisting your body improperly while lifting an object exposes your spine to unwanted twisting. This twisting can increase pressure on the discs and surrounding structures, contributing to their deterioration.
- Lack of adequate support: Not using adequate support, such as leg muscles, when lifting can lead to overload on the spine. Leg muscles are essential to share the load and reduce pressure on the spine.
- Impact on posture: Poor lifting technique can compromise posture, putting additional strain on the spine. Improper posture can contribute to disc deterioration over time.

To prevent disc damage from poor lifting habits, proper lifting techniques are essential. This includes bending with your knees rather than your back, maintaining a neutral posture, using leg muscles to lift, and avoiding twisting your body while lifting heavy objects. Awareness and education on proper lifting practices are crucial to reducing the risk of injury and promoting long-term spinal health.
List of Factors causing Disc Deterioration
Here are some of the main factors causing intervertebral disc deterioration:
List:
- Excessive mechanical load: Excessive mechanical loads on the spine, including lifting heavy loads incorrectly, can contribute to premature disc wear.
- Poor posture: Maintaining poor posture, whether sitting or standing for long periods of time, can put inappropriate pressure on the discs, promoting their deterioration.
- Aging: The natural aging process causes degeneration of the intervertebral discs. Over time, the discs lose their elasticity and shock absorption capacity.
- Sedentary Lifestyle: A sedentary lifestyle can weaken back muscles and contribute to disc deterioration. Regular physical activity is essential to maintain spinal health.
- Trauma: Trauma such as car accidents, falls or sports injuries can damage the intervertebral discs, causing them to deteriorate.
- Disc Dehydration: Disc dehydration due to fluid loss can cause a decrease in their cushioning capacity and contribute to disc wear.
- Genetic factors: Some individuals may be genetically predisposed to health problems related to the intervertebral discs, increasing the risk of deterioration.
- Smoking: Smoking has been linked to decreased blood flow to the discs, which can compromise their nutrition and contribute to their deterioration.
- Obesity: Excess weight can put additional strain on the spine, increasing pressure on the discs and contributing to their deterioration.
- Specific occupations: Certain jobs involving repetitive movements, constant vibrations or awkward positions can increase the risk of disc damage.
- Degenerative diseases: Certain degenerative medical conditions, such as degenerative disc disease (DD) or osteoarthritis, can accelerate the process of disc deterioration.
- Muscle Deficits: Weakened core and back muscles can compromise spinal stability, contributing to disc deterioration.
- Psychological stress: Stress and anxiety can influence pain perception and worsen problems with intervertebral discs.
- Insufficient hydration: Insufficient fluid intake can affect the quality of the discs, as water is essential to maintain their structure and optimal functioning.
- Environmental Factors: Certain environmental conditions, such as constant vibration or harsh working conditions, can contribute to disc deterioration.
- Poor lifting habits: Lifting objects incorrectly, without using proper techniques, can put excess pressure on the spine and contribute to disc deterioration.
- Excessive use of electronic devices: Prolonged use of electronic devices, such as smartphones or laptops, with poor ergonomics can cause increased stress on the spine and affect disc health.
- Pre-existing medical conditions: Certain pre-existing medical conditions, such as scoliosis or other spinal abnormalities, can increase the vulnerability of discs to deterioration.
- Lack of adequate rest: Insufficient sleep or inadequate rest can compromise the discs’ ability to regenerate and recover, contributing to their wear and tear.
- Anatomical defects: Some individuals may have anatomical defects that make their discs more prone to deterioration, regardless of their lifestyle or habits.
- High-impact sports activities: Certain sports activities, especially those involving sudden movements or repetitive impacts, can increase stress on the discs and contribute to their deterioration.
- Poor stress management: Chronic stress can negatively impact the overall health of the body, including the spine and intervertebral discs.
- Nutritional factors: A diet poor in essential nutrients, such as calcium and vitamin D, can affect disc health by compromising their structure and function.
- Post-surgical changes: Previous surgeries on the spine can cause structural changes that contribute to disc deterioration over time.
- Excessive use of high heels: Frequent wearing of high heels can alter the natural curvature of the spine, affecting weight distribution and potentially contributing to disc deterioration.
- Hormonal factors: Certain hormonal changes, such as those associated with menopause in women, can influence bone density and indirectly contribute to disc problems.
- Prolonged exposure to vibration: Certain occupations, such as those involving prolonged exposure to vibration, can increase the risk of disc damage.
- Weather conditions: Extreme weather conditions, such as changes in atmospheric pressure, can affect disc sensitivity and contribute to painful symptoms.
- Poor sleeping habits: Adopting uncomfortable sleeping positions or using an improper mattress can affect the health of your intervertebral discs over time.
- Excessive use of automated lifting devices: Frequent use of automated lifting devices can lead to decreased physical activity, weakening back muscles and increasing the risk of disc damage.
- Psychological conditions: Psychological disorders such as depression or anxiety can influence pain perception and impact overall spinal health.
- Congenital Postural Defects: Some individuals may have congenital postural defects that make their spine more vulnerable to disc deterioration.
- Excessive use of portable electronic devices: Prolonged use of portable electronic devices with frequent head tilt can cause strain on the spine and contribute to disc problems.
It is important to note that most people will experience some deterioration of their discs as they age, but not all will necessarily experience pain or other associated symptoms.

Unlike other tissues in the body, there is very little blood supply to the disc, so once a disc is injured it cannot repair itself and the disc will begin to deteriorate.
Long-term outcomes of degenerative disc disease
Disc disease is not the only sign of spinal wear. The following conditions often occur in parallel:
- Spinal osteoarthritis.When the disc loses its structure, the intervertebral space decreases. This causes greater pressure on the facet joints and they will eventually wear out prematurely.
- Osteoporosis.Degeneration of bone structure can increase the risk of vertebral bone fractures, contributing to overall instability and aging of the spine.
- Spinal stenosisA narrowed spinal canal can occur when the discs flatten, stiffen, bulge into the canal, or strain the facet joints.
- Degenerative spondylolisthesis.Facet degeneration can cause spondylolisthesis.
Differential diagnoses
- Cauda Equina Syndrome – Medical Emergency
- Urinary retention or incontinence, decreased
sexual function - Numbness or paresthesia around the perineum
- Saddle distribution of sensory loss
- Loss of anal sphincter tone (~80% sensitivity)
- Urinary retention or incontinence, decreased
- Lumbar sprain or strain, SI syndrome
- Spondylolisthesis or instability
- Spinal stenosis
- Piriformis syndrome
- Tumor (multiple myeloma or metastases)
- Infection (meningitis)
- Osteoarthritis (rheumatoid or ankylosing spondylitis)
Degenerative cascade
Kirkaldy-Willis describes the degenerative cascade as the necessary reaction of the vertebral body to a degenerated disc.
In front of a twisted disc injury. His environment responds in 3 steps.
- Dysfunction: Small circumferential tears in the outer layer of the disc grow inward. After injury, mobility may be limited.
- Relative instability : The inner material of the disc begins to protrude outward through the tears, causing the disc height to decrease.
- Recovery: Osteophytes form on the edges of the disc and disc changes become fixed. The vertebral segment stabilizes and dysfunction improves.
Symptoms
- Low back pain : Back pain is common in the second decade, discopathy and herniated discs in the third or fourth decade. The usual history of a lumbar disc herniation is repetitive low back pain, radiating to the buttocks and relieved by rest . The pain is increased by episodes of bending, sitting, straining, sneezing, coughing, etc. The pain is decreased by rest and fetal position.
- Radiculopathy : This refers to pain in the distribution of the sciatic nerve and is invariably due to a herniated disc. This is called sciatica. Leg pain equal to or greater than back pain highlights radicular pain due to compression of the nerve root due to a herniated disc. The pain usually begins in the lower back and radiates to the sacroiliac regions, buttocks, and thigh. Radicular pain usually extends below the knee.
- Nerve Root Compression : About 95% of disc prolapse occurs in the L4-5 region, compressing the L5 nerve root. Other commonly involved nerve roots are L4 and S1 due to disc prolapse between L3-4 and L5-S1 respectively showing different clinical manifestations following nerve root compression.

- Osteoarthritis refers to degenerative changes in synovial joints .
- Discopathy refers to degenerative changes in the intervertebral disc.
- Spondylosis is a degenerative process of the spine involving mainly the annulus fibrosus and characterized by anterior and lateral marginal osteophytes arising from the processes of the vertebral body, while the height of the intervertebral disc is normal or only slightly decreased .
References
- Bozzio AE, Johnson CR, Fattor JA, Kleck CJ, Patel VV, Burger EL, Noshchenko A, Cain CMJ. Stand-alone Anterior Lumbar Interbody, Transforaminal Lumbar Interbody, and Anterior/Posterior Fusion: Analysis of Fusion Outcomes and Costs. Orthopedics. 2018 Sep 01;41(5):e655-e662. [ PubMed ]2.
- Mostofi K, Gharaie Moghaddam B, Karimi Khouzan R, Daryabin M. The reliability of LERI’s sign in L4 and L3 radiculalgia. J Clin Neurosci. 2018 Apr;50:102-104. [ PubMed ]3.
- Paul CPL, Emanuel KS, Kingma I, van der Veen AJ, Holewijn RM, Vergroesen PA, van de Ven PM, Mullender MG, Helder MN, Smit TH. Changes in Intervertebral Disk Mechanical Behavior During Early Degeneration. J Biomech Eng. 2018 Sep 01;140(9) [ PubMed ]4.
- Solomou A, Kraniotis P, Rigopoulou A, Petsas T. Frequent Benign, Nontraumatic, Noninflammatory Causes of Low Back Pain in Adolescents: MRI Findings. Radiol Res Pract. 2018;2018:7638505. [ PMC free article ] [ PubMed ]5.
- Abi-Hanna D, Kerferd J, Phan K, Rao P, Mobbs R. Lumbar Disk Arthroplasty for Degenerative Disk Disease: Literature Review. World Neurosurg. 2018 Jan;109:188-196. [ PubMed ]6.
- Martínez-Quiñones JV, Aso-Escario J, González-García L, Consolini F, Arregui-Calvo R. Are Modic Changes Able to Help Us in Our Clinical Practice? A Study of the Modic Changes in Young Adults During Working Age. Clin Spine Surg. 2017 Jul;30(6):259-264. [ PubMed ]7.
- Anderson JT, Haas AR, Percy R, Woods ST, Ahn UM, Ahn NU. Lumbar Diskography and Failed Back Syndrome in Patients Receiving Workers’ Compensation. Orthopedics. 2015 Nov;38(11):e951-8. [ PubMed ]8.
- Mijiyawa M, Oniankitan O, Kolani B, Koriko T. Low back pain in hospital outpatients in Lomé (Togo). Joint Bone Spine. 2000;67(6):533-8. [ PubMed ]9.
- Yao Q, Wang S, Shin JH, Li G, Wood KB. Lumbar facet joint motion in patients with degenerative spondylolisthesis. J Spinal Disord Tech. 2013 Feb;26(1):E19-27. [ PMC free article ] [ PubMed ]10.
- Dydyk AM, Khan MZ, Singh P. StatPearls [Internet]. Stat Pearls Publishing; Treasure Island (FL): Oct 24, 2022. Radicular Back Pain. [ PubMed ]11.
- Shah LM, Ross JS. Imaging of Degenerative and Infectious Conditions of the Spine. Neurosurgery. 2016 Sep;79(3):315-35. [ PubMed ]12.
- Fritzell P, Hägg O, Wessberg P, Nordwall A., Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine (Phila Pa 1976). 2001 Dec 01;26(23):2521-32; discussion 2532-4. [ PubMed ]13.
- Lee YC, Zotti MG, Osti OL. Operative Management of Lumbar Degenerative Disc Disease. Asian Spine J. 2016 Aug;10(4):801-19. [ PMC free article ] [ PubMed ]14.
- Lu SB, Hai Y, Kong C, Wang QY, Su Q, Zang L, Kang N, Meng XL, Wang Y. An 11-year minimum follow-up of the Charite III lumbar disc replacement for the treatment of symptomatic degenerative disc disease . Eur Spine J. 2015 Sep;24(9):2056-64. [ PubMed ]15.
- Siepe CJ, Mayer HM, Heinz-Leisenheimer M, Korge A. Total lumbar disc replacement: different results for different levels. Spine (Phila Pa 1976). 2007 Apr 01;32(7):782-90. [ PubMed ]16.
- Mostofi K, Khouzani RK. Preliminary results of lumbar disk herniation surgery by Endoscopic Destandau Method. J Clin Orthop Trauma. 2018 Mar;9(Suppl 1):S149-S151. [ PMC free article ] [ PubMed ]17.
- Hsu WK, Jenkins TJ. Management of Lumbar Conditions in the Elite Athlete. J Am Acad Orthop Surg. 2017 Jul;25(7):489-498. [ PubMed ]18.
- Joswig H, Stienen MN, Smoll NR, Corniola MV, Chau I, Schaller K, Hildebrandt G, Gautschi OP. Effects of Smoking on Subjective and Objective Measures of Pain Intensity, Functional Impairment, and Health-Related Quality of Life in Lumbar Degenerative Disk Disease. World Neurosurg. 2017 Mar;99:6-13. [ PubMed ]
























{kind=link}