

Introduction
Cluster Headaches: A Surging Pain to Decode
Horton’s headaches, also known as trigeminal autonomic cephalgias (TACs), are classified as one of the most uncommon primary headaches, affecting a mere 0.1% of the population. The rarity of these headaches poses a challenge in comprehending the intricacies of their underlying mechanisms, making the study of this condition notably intricate. Despite their infrequency, Horton’s headaches are acknowledged as one of the most severe types of headaches, emphasizing the critical importance of their accurate identification and effective management.
Also referred to as Cluster headache AVF, Horton’s headaches manifest as unilateral headaches with a relatively short duration, ranging from 15 minutes to 3 hours. What sets them apart is their association with at least one autonomic symptom occurring on the same side as the headache. These autonomic symptoms include watery eyes, nasal congestion, conjunctival injection, or a sensation of auditory fullness. The interplay of these symptoms contributes to the distinct clinical profile of Horton’s headaches.
Nasal congestion is a notable feature of Horton’s headaches, and it can lead to misdiagnosis, often being confused with a “sinus headache.” Unfortunately, such misdiagnoses may result in ineffective treatments, as decongestants commonly prescribed for sinus headaches prove futile in alleviating the intensity of Horton’s headaches. A characteristic pattern emerges as these headaches occur either every other day or up to eight times a day. Additionally, they exhibit a specific temporal pattern, predominantly presenting during the night. The regularity of these headaches becomes evident, often at the same time each day.
An intriguing aspect of Horton’s headaches is their episodic nature. Most individuals experience daily episodes that persist for weeks or even months, creating a considerable impact on their daily lives. However, these intense phases are interspersed with prolonged periods of remission, providing some respite from the debilitating symptoms.
Given the severity and unique characteristics of Horton’s headaches, accurate diagnosis and appropriate management become paramount. The distinction between these headaches and other types, such as sinus headaches, is crucial to ensure effective therapeutic interventions. Healthcare professionals must be attentive to the specific autonomic symptoms accompanying these headaches, steering clear of potential misdiagnoses that could lead to ineffective treatments. As research endeavors continue to unravel the complexities of Horton’s headaches, enhancing our understanding of their mechanisms, the emphasis on timely and accurate identification remains fundamental for optimizing patient outcomes.
Who Are Most Affected? Prevalence and Patient Profile
Cluster headaches, also known as cluster headaches (CH), represent a rare but extremely disabling form of primary headache disorder. Understanding their epidemiology is essential for assessing their impact on populations and guiding clinical management. These data provide insight into the most affected populations and help contextualize the importance of the topic.
General Prevalence
The prevalence of cluster headaches in the general population is estimated at between 0.1% and 0.4% , making it a relatively rare condition. However, its severity and impact on quality of life make it a research priority in the field of primary headache disorders.
Variations by Sex
- Cluster headaches predominantly affect men , with a male to female ratio of approximately 3:1 .
- However, some recent studies show a slight increase in diagnoses in women, possibly due to better recognition of symptoms and more frequent medical follow-up.
Age Distribution
- The average age of onset of cluster headaches is between 20 and 40 years , although cases have been reported in children and the elderly.
- Diagnosis is often delayed due to the rarity of the condition and its atypical clinical presentation, particularly in young or elderly patients.
Ethnic and Geographic Variations
- Epidemiological data indicate a slightly higher prevalence in populations of European origin compared to Asian or African populations.
- The geographic difference could be due to genetic or environmental factors, although further studies are needed to confirm these observations.
Family Risk and Heredity
- Family histories of cluster headaches are rare but documented, suggesting a potential genetic component. Some studies have identified mutations in genes related to neurotransmitters and vascular circuits in the brain.
Societal Impact and Under-Diagnosis
AVFs affect individuals in the midst of their professional and social activity, amplifying their economic and societal impact.
Due to their rarity and the disabling nature of attacks, cluster headaches are often underdiagnosed or misdiagnosed. Patients may be mistaken for migraines or tension-type headaches, delaying appropriate treatment.
What Promotes Their Appearance: Risk Factors and Triggers
Cluster headaches, also known as cluster headaches (CH), are a rare but extremely disabling form of primary headache disorder. Although the exact causes remain uncertain, several risk factors have been identified that may increase the likelihood of developing this condition. These factors, whether genetic, environmental, or lifestyle-related, provide insight into individual susceptibility and guide preventive and therapeutic approaches.
Family History
Studies have shown a genetic component in the development of cluster headaches. A positive family history, particularly among first-degree relatives, is associated with an increased risk. Research suggests that mutations in certain genes involved in the regulation of vascular and neural circuits may play a role.
- Genetic transmission : Although the exact mechanisms are not fully understood, a family history significantly increases the risk of developing CH. This indicates a genetic predisposition that could explain some recurrent forms.
Smoking
Smoking is one of the main environmental risk factors associated with cluster headaches. Studies show that more than 80% of patients with CH are current or former smokers.
- Impact of nicotine : Nicotine acts on blood vessels, increasing their sensitivity and contributing to excessive vasodilation, a key element in the pathophysiological mechanisms of AVF.
- Correlation with severity : Patients who actively smoke often have more frequent and more severe attacks.
Sex and Hormones
Cluster headaches predominantly affect men, with a ratio of approximately 3:1 to women. However, the gender gap appears to be narrowing slightly in recent studies, suggesting a complex role for hormones.
- Hormonal influence : In women, hormonal variations, particularly those linked to the menstrual cycle, could have a modulating effect on seizures.
Lifestyle Habits and Triggers
Certain lifestyles and specific triggers increase the risk of seizures occurring or worsening.
- Alcohol consumption : Alcohol is a common trigger, even in small amounts. It acts as a vasodilator, often causing immediate attacks.
- Stress and sleep disturbances : Chronic stress and lack of sleep are aggravating factors that can influence the frequency and intensity of attacks.
- Exposure to certain stimuli : Strong odors, bright lights, and sudden changes in temperature are among common triggers.
Other Comorbidities
Patients with certain conditions, such as vascular disorders or chronic migraines, are at increased risk of developing cluster headaches. Although these comorbidities are not direct causes, they share common pathophysiological mechanisms.
What We Know (And Still Don’t Know) About the Causes
List of causes:
- Nervous system dysfunction : Dysfunctions in the nervous system, particularly in the hypothalamus, have been associated with cluster headaches. The hypothalamus plays a key role in regulating circadian rhythms, which may explain why attacks often occur at specific times of the day.
- Vascular factors : Changes in blood flow and dilation of blood vessels around the brain and eyes may play a role in cluster headaches. However, the exact relationship between blood vessels and cluster headaches remains unclear.
- Genetic factors : There is evidence suggesting that there may be a genetic component to cluster headaches. A family history of cluster migraines increases the risk of developing the condition.
- Environmental factors : Certain environmental factors, such as smoking, can trigger or worsen cluster headache attacks. Similarly, seasonal changes, temperature fluctuations, and other environmental factors can influence the frequency and severity of attacks.
- Hormones : Hormonal changes, such as those associated with menopause in women, can influence the frequency and severity of attacks.
- Head trauma : Head injuries can trigger cluster headaches in some people, although this relationship is not always clear.
- Inflammation : Inflammatory processes in nerve or vascular pathways may contribute to the symptoms of cluster headaches.
- Sleep disturbances : Sleep disturbances, such as insomnia or sleep-disordered breathing, may increase the risk of cluster headache attacks.
- Alcohol and nicotine : Alcohol and nicotine use, especially smoking, are known triggers of cluster headache attacks.
- Psychological stress : Emotional and psychological stress can trigger or worsen cluster headache symptoms in some people.
- Exposure to bright light : Prolonged exposure to bright light or intense visual stimuli can trigger seizures in some people.
- Certain medications : Certain medications, such as vasodilators, can worsen cluster headache symptoms in some people.
- High Altitude : Some people may develop cluster headaches when exposed to high altitudes due to changes in atmospheric pressure.
- Dietary factors : Certain foods and beverages, such as foods high in histamine or foods containing nitrates, can trigger cluster headache attacks in some susceptible individuals.
- Vascular disorders : Conditions such as atherosclerosis or other vascular disorders may increase the risk of developing cluster headaches.
- Endocrine Disorders : Hormonal imbalances or endocrine disorders may be associated with the onset of cluster headaches in some people.
- Chemical exposure : Certain environmental or occupational chemicals can trigger cluster headache attacks in susceptible individuals.
- Underlying medical conditions : Certain underlying medical conditions, such as arthritis, autoimmune diseases, or infections, may be associated with cluster headaches.
- Blood clotting disorders : Abnormalities in blood clotting can affect cerebral blood flow and contribute to cluster headaches.
- Altered gut microbiota : Research suggests a link between gut microbiota and neurological disorders, including cluster headaches.
- Psychological factors : Psychological disorders such as anxiety, depression, or post-traumatic stress disorder may be associated with cluster headaches.
- Swallowing problems : Swallowing abnormalities or chewing problems may be associated with cluster headaches in some people.
- High blood pressure : High blood pressure can affect blood flow to the brain and increase the risk of cluster headache attacks.
- Dehydration : A state of dehydration can lead to changes in blood pressure and circulation, which can trigger cluster headache attacks in some people.
Recognizing the Signs: Typical Symptoms of a Crisis
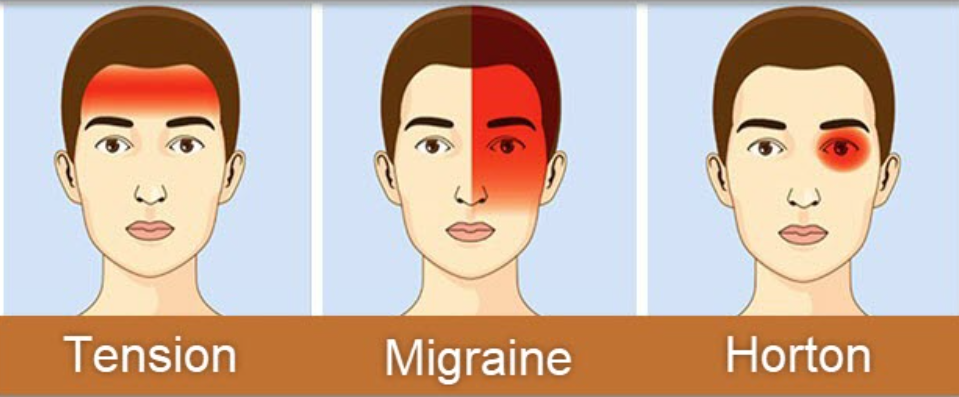
Migraine Pattern: Identified by intense, throbbing pain usually on one side of the head, accompanied by nausea, and sensitivity to light (photophobia) and sound (phonophobia).
Cluster Headache Pattern: Known for severe, burning or piercing pain around one eye, often associated with redness, tearing, and nasal congestion on the same side
- Sudden, intense pain: The main characteristic of Horton’s headaches is extremely intense, sudden pain, often described as a burning, stinging, or stabbing sensation. The pain is usually localized on one side of the head, around the eye, temple or forehead.
- Short duration of attacks: Horton’s headache attacks tend to be very short but very painful. Each episode can last from 15 minutes to three hours, although some individuals may experience several attacks in a day.
- Frequency of Attacks: Horton’s headaches can occur very regularly during a specific period of time, called the “cluster period.” During this time, people may have several seizures per day, often at specific times.
- Sensitivity to light and sound: During an attack, people with Horton’s headaches may be sensitive to light (photophobia) and sound (phonophobia).
- Restlessness or restlessness during attacks: Some people may feel restless or restless during a Horton’s headache attack, moving around frequently or actively expressing their pain.
- Symptoms associated with the affected side: The pain is usually localized to one side of the head, and symptoms such as redness or watering of the eye, runny nose, or nasal congestion on the affected side may also occur.
It is important to note that Horton’s headaches are a serious medical condition and require medical evaluation and management. If you suspect that you or someone you know is suffering from Horton’s headaches, consult a healthcare professional to get an accurate diagnosis and discuss treatment options.
Inside the Mechanism: What Happens in the Brain
The pathophysiology of Horton’s headache is not completely understood, but some hypotheses have been put forward to explain the mechanisms underlying this painful condition. Here are some aspects of the pathophysiology of Horton’s headaches:
- Hypothalamus: It is suggested that the suprachiasmatic nucleus of the hypothalamus, which is involved in the regulation of circadian rhythms, may play a central role in Horton’s headaches. Dysfunctions in the hypothalamus could contribute to the onset of seizures.
- Vascular dysregulation: Changes in blood circulation and vasomotor function have been observed during Horton’s headache attacks. Some researchers believe that abrupt changes in the caliber of blood vessels, particularly those located around the periorbital region, could contribute to the severe pain.
- Activation of the trigeminal nerve: The trigeminal nerve, which is responsible for facial sensation, may be involved in Horton’s headaches. Abnormal activation of this nerve could contribute to pain and associated symptoms, such as nasal congestion and watery eyes.
- Release of chemicals: Certain neurotransmitters and chemicals, such as serotonin, have been implicated in Horton’s headaches. Abnormal release of these substances could play a role in vasodilation and pain.
- Role of the immune system: There are indications that the immune system may be involved in Horton’s headaches. Inflammatory markers may be present, and some patients have shown a positive response to certain immunosuppressive medications.
- Genetic Factors: There is a familial trend in some cases of Horton’s headache, suggesting a possible genetic component in the predisposition to this condition.
The complexity of the pathophysiology of Horton’s headache requires continued research to better understand the underlying mechanisms. Advances in this area could lead to more targeted and effective treatments to relieve symptoms of this debilitating condition. It is important to note that the pathophysiology may vary between individuals, and the precise understanding of this condition may evolve over time as more research is conducted.
Common Triggers: What Can Cause a Crisis
Here are some potential triggers:
- Alcohol: Consumption of alcohol, particularly beer, red wine or hard liquor, has been linked to triggering seizures in some people.
- Smoking: Smoking, especially regular smoking, is a potential risk factor.
- Heat: Some patients report that heat can trigger or worsen seizures.
- Physical activity: Intense physical exercise can trigger seizures in some people.
- Circadian rhythms: Horton’s headaches may be associated with disruptions in the circadian rhythm, and some people may be more likely to experience attacks at specific times of the day.
- Certain foods: Certain foods, such as foods high in histamine (aged cheeses, certain seafood, etc.), have been suggested as potential triggers.
- Stress: Although the link between stress and Horton’s headaches is unclear, stress can make symptoms worse in some people.
It is important to note that these triggers do not necessarily trigger attacks in all people with Horton’s headaches, and some individuals may not have obvious triggers. Everyone reacts differently, and it can be helpful to keep a seizure diary to identify individual triggers.
When Pain Invades Life: Daily and Social Impacts
Cluster headaches (CH) are recognized as one of the most painful forms of headache. This condition, although rare, has a significant impact on patients’ quality of life, affecting their daily activities, work life, and social relationships. Understanding these impacts is essential to raise awareness among patients, families, and healthcare professionals, and to better guide management strategies.
Impact on Daily Activities
Cluster headache attacks are characterized by acute, one-sided pain, often described as unbearable. These attacks, which can occur several times a day and last from 15 minutes to 3 hours, make daily activities nearly impossible.
- Basic functions :
- During attacks, patients are often unable to concentrate, read, cook, or even walk. The intensity of the pain forces them to stop any activity they are currently doing.
- Associated symptoms, such as watery eyes, nasal congestion, or facial sweating, amplify the discomfort and make it difficult to manage simple tasks.
- Disruption of sleep cycles :
- Nighttime attacks are common, causing sudden awakenings and severely disrupting sleep quality. This chronic sleep deprivation increases fatigue and irritability, exacerbating daytime difficulties.
Professional Impacts
Cluster headaches primarily affect individuals between the ages of 20 and 40, an age group often associated with intense professional activity. The effects on work are significant:
- Absenteeism and drop in productivity :
- Severe and unpredictable pain forces many patients to regularly miss work. Even during periods when attacks are not occurring, the fear of further attacks creates constant anxiety, reducing the ability to concentrate.
- According to studies, one in three patients report job loss or reduced professional activity due to disabilities related to AVF.
- Career changes :
- Some patients choose less demanding jobs or positions with flexible hours to better manage their symptoms. This can lead to lower income and limited career opportunities.
- Stigma and misunderstanding :
- The invisible nature of cluster headaches often leads to misunderstanding from colleagues and employers, exacerbating stress and feelings of isolation.
Impacts on Social and Family Life
The repercussions of cluster headaches extend far beyond the individual sphere, also affecting social and family relationships.
- Social isolation :
- Patients often avoid social interactions for fear of a seizure occurring in public. This constant fear can lead to progressive isolation and decreased participation in social events.
- Activities involving potential triggers (alcohol, bright light, stress) are particularly feared, further limiting outings and leisure activities.
- Family relationships :
- Patients’ loved ones, while often empathetic, may struggle to understand the extent of the pain and the impact of the attacks. This can lead to strained relationships.
- Family responsibilities, such as caring for children or managing household chores, become a burden, adding to the stress for patients and their partners.
- Effects on mental health :
- Chronic pain and loss of control over daily life are strongly correlated with mental health disorders, including anxiety and depression. One study shows that more than 40% of cluster headache patients experience depressive symptoms.
Patient Testimonials
Julie, 29, stay-at-home mom :
“The fear of triggering a crisis prevents me from enjoying simple moments, like taking my children to the park. The guilt is constant.”
Marc, 35, engineer :
“During a seizure, I feel like a knife is being stabbed into my eye. I’m unable to work or even think. It’s a pain that isolates me from everything, even my family.”
Naming Pain: How to Diagnose the Condition
The diagnostic criteria for cluster headache according to the International Classification of Headache Disorders, 3rd edition (ICHD-3) are as follows.
Cluster Headaches
Diagnostic criteria:
- At least five painful attacks: The attacks must meet criteria B to D.
- Severe, one-sided headache attacks: Attacks usually occur around the eye or temple.
- Characteristics of pain: Pain has at least two of the following characteristics:
- Reaches maximum intensity in just a few minutes.
- The pain is throbbing or throbbing.
- The pain is severe or unbearable in intensity.
- Frequency of attacks: The frequency of attacks is at least one every two days to eight per day.
Associated characteristics that may be present:
- Conjunctival injection or tear: Possible presence on affected side.
- Nasal congestion or runny nose: The nostril on the affected side may be congested or runny.
- Eyelid Edema: The eyelid on the affected side may be edematous.
- Forehead and facial sweat: The forehead and face on the affected side may be sweaty.
- Restlessness or need to move: Often seen during seizures.
Cluster headaches can be classified into two subtypes:
- Episodic: Attacks occur in series (clusters) followed by periods of complete remission.
- Chronic: Attacks occur without a complete remission period or with very short remission periods (less than 3 months).
These diagnostic criteria are intended to be evaluated by qualified healthcare professionals to confirm the diagnosis of cluster headaches. If you or someone you know is experiencing similar symptoms, it is recommended that you consult a healthcare professional for a proper evaluation.
Living with Cluster Headaches: A Typical Day
Horton’s headaches, also known as cluster headaches, are among the most excruciating types of pain a person can experience. This neurological condition is characterized by severe, debilitating pain typically around one eye, with episodes lasting from minutes to hours. Here’s a glimpse into a typical day in the life of someone suffering from Horton’s headache.
Morning: A Brutal Awakening
The day often starts abruptly for those with Horton’s headaches. These headaches frequently occur during sleep, causing a sudden and painful awakening. The pain is described as a burning or piercing sensation, usually concentrated around one eye, accompanied by symptoms like redness, tearing, and nasal congestion on the same side.
After taking an abortive treatment, such as a triptan medication or inhaling pure oxygen, the person tries to fall back asleep. However, the fear of another attack can make sleep difficult to regain. For those who wake up without pain, the morning is marked by heightened alertness and mental preparation for the possibility of an attack.
Mid-Morning: Avoiding Triggers
The mid-morning period is critical for avoiding potential triggers. Horton’s headaches can be triggered by factors such as alcohol, certain foods (like chocolate or aged cheeses), strong odors, and even temperature changes. Morning routines are carefully designed to minimize exposure to these triggers.
In addition to preventive measures, people with Horton’s headaches often have to juggle work or family obligations. Concentrating on work can be a constant challenge, especially with the looming threat of an attack. Informed colleagues and family members can offer crucial support, but maintaining normal productivity remains difficult.
Afternoon: Managing the Attacks
Attacks can occur at any time of the day. When an attack strikes, the pain is so intense that the person is often incapacitated. These episodes typically last between 15 minutes and 3 hours, but the pain can be so unbearable that immediate intervention with specific treatments, such as high-flow oxygen or injectable medications, is necessary.
During an attack, the environment must be as quiet and dark as possible. The person may need to retreat to an isolated room to manage the pain. Relaxation techniques, such as deep breathing and meditation, can help, although their effectiveness varies from person to person.
Evening: Anticipating the Night
Evenings are a time for preparing for the night ahead. Horton’s headaches often follow regular cycles, making attacks somewhat predictable. The person may avoid known evening triggers, such as alcohol, and ensure that emergency treatments are readily accessible.
Sleep is crucial, but the fear of nighttime attacks can make falling asleep difficult. Some people find it helpful to sleep in a semi-upright position to reduce the frequency of attacks. Others adopt soothing rituals, such as reading or listening to soft music, to facilitate a more peaceful transition to sleep.
Conclusion: A Daily Struggle
Living with Horton’s headaches is a daily struggle marked by intense pain and constant adaptation. Every aspect of the day, from diet to sleep routines, is influenced by the need to avoid triggers and manage attacks. Despite these challenges, those with this condition develop incredible resilience and coping strategies to navigate their daily lives.
For those unfamiliar with this condition, understanding the challenges faced by people with Horton’s headaches can foster empathy and support. Recognizing the invisible pain and the strength required to manage it can help create a more compassionate and supportive environment for everyone.
L’Ostéopathie en Renfort : Une Approche Globale et Manuelle
Cluster headaches, due to their intensity and recurrence, lead many patients to seek complementary approaches to relieve pain and improve their quality of life. Osteopathy, thanks to its holistic approach to the body and its arsenal of non-invasive manual techniques, constitutes a relevant therapeutic avenue, complementing conventional neurological care.
Without claiming to cure cluster headaches, osteopathy proposes to intervene on the mechanical, vascular and neurological imbalances likely to influence the frequency and intensity of attacks.
Understanding the osteopathic terrain of cluster headaches
The osteopath does not only treat pain located around the eye or temple. He seeks to understand the entire chain of myofascial tension , cranial or cervical mobility restrictions , postural asymmetries and physiological stress factors that can maintain a breeding ground for attacks.
Indeed, the craniocervical region constitutes an important neurovascular crossroads. The brainstem, cranial nerves, carotid vascular axis, intracranial venous plexuses, and reciprocal tension membranes may all be involved, directly or indirectly, in the triggering or amplifying mechanisms of cluster headaches.
The main areas of osteopathic intervention
1. The skull and intracranial membranes
Cranial work in osteopathy aims to release tension in the cranial sutures , reciprocal tension membranes and to improve the mobility of the skull bones. This approach is particularly useful in cases where the pain is localized around the eye or temple.
👉 Techniques used :
- Functional techniques on the base of the skull (occiput, temporals, sphenoid)
- Membrane techniques (relaxation of intracranial membrane tension)
- Techniques for decompression of the foramens (through which the cranial nerves, including the trigeminal nerve, pass)
2. The upper cervical spine
The occipito-atlanto-axial junction (C0-C1-C2) is a key area. It is directly related to the trigemino-cervical system , which is involved in the transmission of facial and orbital pain. Restricted mobility in this area can maintain a tonic postural and neurological imbalance.
👉 Techniques used :
- Muscle Energy Techniques for C1/C2
- Gentle mobilization of the upper cervical vertebrae
- Suboccipital decompression
3. The upper thorax and the base of the neck
Vascular congestion and myofascial tension in the upper thoracic region (clavicles, first rib, sternum) can interfere with cranial venous return . Intracranial venous stagnation is sometimes found in patients with migraine or cluster headaches, and can worsen symptoms.
👉 Techniques used :
- Release of the first rib
- Sternal mobilization
- Opening of the upper thoracic outlet
4. The autonomic nervous system
The involvement of the autonomic nervous system is well documented in cluster headaches (watering eyes, nasal congestion, red eyes, facial sweating). Osteopathy seeks to balance the ortho- and parasympathetic tone , working in particular on the reflex centers of the brainstem, the cervical ganglia and the diaphragm.
👉 Techniques used :
- Vagal techniques (release of the thoracic inlet, work around the vagus nerve)
- Craniosacral techniques
- Normalization of the diaphragm (influence on the phrenic nerve and the vagal axis)
5. The Skull-Sacré Axe
The connection between the skull and sacrum is fundamental to the osteopathic approach. Tensions in the pelvis, pelvic floor, or sacrum can create upward compensations that impact the base of the skull and the central nervous system.
👉 Techniques used :
- Work on the sacrum and sacroiliac joints
- Release of fascial tension in the lumbopelvic region
- Fluidic techniques on the craniosacral axis
What the Science Says: Data and Studies on Osteopathic Effectiveness
Several studies have explored the effectiveness of osteopathic treatments for various types of headaches, including migraines and tension-type headaches. Although specific research on osteopathy for cluster headaches is limited, the results of related studies are promising:
Studies on migraines
- A 2011 study published in “The Journal of Headache and Pain” found that osteopathic manipulative treatment (OMT) significantly reduced the frequency and intensity of migraine attacks. The study, titled “Efficacy of osteopathic manipulative treatment of female patients with migraine: results of a randomized controlled trial,” was published in the Journal of Alternative and Complementary Medicine . It involved 42 participants, with 21 in the intervention group receiving OMT and 21 in the control group receiving no additional treatment beyond their usual medication. Results showed significant improvements in the intervention group in several domains of health-related quality of life, a reduction in pain intensity, and a decrease in the number of days affected by migraines. The control group did not show such significant improvements, supporting the potential benefits of OMT in managing migraines. ( Journal of Alternative and Complementary Medicine )
- Another study from the same year, titled “Migraine without aura and osteopathic medicine, a non-pharmacological approach to pain and quality of life: open pilot study,” published in The Journal of Headache and Pain , also suggested that osteopathic manipulative treatment (OMT) has positive effects on reducing pain and improving quality of life for patients with migraine. This study involved patients with migraine without aura and evaluated the impact of OMT on pain and quality of life. The results showed a significant reduction in the intensity and frequency of migraine attacks in participants receiving OMT. Additionally, these patients reported an improvement in their overall quality of life, including aspects such as emotional and physical well-being. The researchers observed that OMT may help modulate the autonomic nervous system, improve blood flow, and correct musculoskeletal misalignments, which may contribute to the reduction of migraines. However, the study authors stressed the need for further research with larger samples and more robust methodologies to confirm these promising results and better understand the mechanisms of action of OMT in the treatment of migraines ( The Journal of Headache and Pain )
Tension-type headaches
- A study published in the European Journal of Pain in 2014 explored the effectiveness of osteopathic manipulative treatment (OMT) for tension-type headaches. This research found that OMT can relieve these headaches through muscle relaxation and improved blood flow. The study involved patients with chronic tension-type headaches (CTTH). Participants were divided into two groups: one group receiving OMT sessions and a control group treated with amitriptyline, a medication commonly used for chronic pain. The results showed that patients in the OMT group experienced significant reductions in pain intensity, headache frequency, and headache duration, compared to the control group. Specifically, pain intensity in the OMT group decreased from 4.9 to 3.1 on a 10-point scale, headache frequency decreased from 19.8 to 8.3 days per month, and headache duration was reduced from 10 to 6 hours. These improvements were statistically significant and suggest that OMT may be an effective treatment for tension-type headaches by improving head posture and reducing muscle tension. However, the study also highlighted the need for further research with larger sample sizes to confirm these findings and better understand the mechanisms underlying OMT’s effectiveness for this type of headache. ( Journal of Osteopathic Medicine )
Towards a Complete Approach: Relieve, Understand, Support
In conclusion, osteopathy presents itself as a promising and holistic approach in the management of Horton’s headaches, also known as “cluster migraines”. By focusing on the structural and functional balance of the body, osteopaths aim to relieve pain, reduce the frequency of attacks and restore the overall well-being of patients.
Osteopathy is distinguished by its consideration of the patient’s posture, mobility and blood circulation to identify physical imbalances. The gentle manual techniques used in osteopathy aim to release muscle tension and joint restrictions, thereby helping to reduce pressure on nerves and blood vessels.
This approach not only treats local symptoms, but also focuses on identifying underlying factors such as stress and other lifestyle elements that could be contributing to headaches. By taking a holistic perspective, osteopathy offers a complementary alternative for those seeking non-invasive solutions in the management of these debilitating headaches.
Thus, osteopathy represents a promising avenue for providing relief to those suffering from Horton’s headaches, highlighting the importance of treating both symptoms and underlying causes for a comprehensive approach to neurovascular health.
References
- Drummond PD. Mechanisms of autonomic disturbance in the face during and between attacks of cluster headache . Cephalalgia. 2006 Jun;26(6):633-41. [ PubMed ]
- Hoffmann J, May A. Diagnosis, pathophysiology, and management of cluster headache . Lancet Neurol. 2018 Jan;17(1):75-83. [ PubMed ]
- Weaver-Agostoni J. Cluster headache . Am Fam Physician. 2013 Jul 15;88(2):122-8. [ PubMed ]
- Láinez MJ, Guillamón E. Cluster headache and other TACs: Pathophysiology and neurostimulation options. Headache . 2017 Feb;57(2):327-335. [ PubMed ]
- Harder AVE, Winsvold BS, Noordam R, Vijfhuizen LS, Børte S, Kogelman LJA, de Boer I, Tronvik E, Rosendaal FR, Willems van Dijk K, O’Connor E, Fourier C, Thomas LF, Kristoffersen ES, Cluster Headache Genetics Working Group. Fronczek R, Pozo-Rosich P, Jensen RH, Ferrari MD, Hansen TF, Zwart JA, Terwindt GM, van den Maagdenberg AMJM. Genetic Susceptibility Loci in Genomewide Association Study of Cluster Headache . Ann Neurol. 2021 Aug;90(2):203-216. [ PMC free article ] [ PubMed ]
- O’Connor E, Fourier C, Ran C, Sivakumar P, Liesecke F, Southgate L, Harder AVE, Vijfhuizen LS, Yip J, Giffin N, Silver N, Ahmed F, Hostettler IC, Davies B, Cader MZ, Simpson BS, Sullivan R, Efthymiou S, Adebimpe J, Quinn O, Campbell C, Cavalleri GL, Vikelis M, Kelderman T, Paemeleire K, Kilbride E, Grangeon L, Lagrata S, Danno D, Trembath R, Wood NW, Kockum I, Winsvold BS , Steinberg A, Sjöstrand C, Waldenlind E, Vandrovcova J, Houlden H, Matharu M, Belin AC. Genome-Wide Association Study Identifies Risk Loci for Cluster Headache . Ann Neurol. 2021 Aug;90(2):193-202. [ PubMed ]
- Shin YW, Park HJ, Shim JY, Oh MJ, Kim M. Seasonal Variation, Cranial Autonomic Symptoms, and Functional Disability in Migraine: A Questionnaire-Based Study in Tertiary Care. Headache . 2015 Sep;55(8):1112-23. [ PubMed ]
- Waldenlind E, Gustafsson SA, Ekbom K, Wetterberg L. Circadian secretion of cortisol and melatonin in cluster headache during active cluster periods and remission. J Neurol Neurosurg Psychiatry. 1987 Feb;50(2):207-13. [ PMC free article ] [ PubMed ]
- Akerman S, Holland PR, Summ O, Lasalandra MP, Goadsby PJ. A translational in vivo model of trigeminal autonomic cephalalgias: therapeutic characterization. Brain. 2012 Dec;135(Pt 12):3664-75. [ PubMed ]
- Waung MW, Taylor A, Qualmann KJ, Burish MJ. Family History of Cluster Headache : A Systematic Review. JAMA Neurol. 2020 Jul 01;77(7):887-896. [ PMC free article ] [ PubMed ]
- Fischera M, Marziniak M, Gralow I, Evers S. The incidence and prevalence of cluster headache : a meta-analysis of population-based studies. Cephalalgia. 2008 Jun;28(6):614-8. [ PubMed ]
- Rozen TD. Cluster Headache Clinical Phenotypes: Tobacco Nonexposed (Never Smoker and No Parental Secondary Smoke Exposure as a Child) versus Tobacco-Exposed: Results from the United States Cluster Headache Survey. Headache . 2018 May;58(5):688-699. [ PubMed ]
- Leone M, Russell MB, Rigamonti A, Attanasio A, Grazzi L, D’Amico D, Usai S, Bussone G. Increased familial risk of cluster headache . Neurology. 2001 May 08;56(9):1233-6. [ PubMed ]
- Barloese MCJ, Beske RP, Petersen AS, Haddock B, Lund N, Jensen RH. Episodic and Chronic Cluster Headache : Differences in Family History, Traumatic Head Injury, and Chronorisk. Headache . 2020 Mar;60(3):515-525. [ PubMed ]
- Drummond PD. Dysfunction of the sympathetic nervous system in cluster headache . Cephalalgia. 1988 Sep;8(3):181-6. [ PubMed ]
- Wilbrink LA, Louter MA, Teernstra OPM, van Zwet EW, Huygen FJPM, Haan J, Ferrari MD, Terwindt GM. Allodynia in cluster headache . Bread. 2017 Jun;158(6):1113-1117. [ PubMed ]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1-211. [ PubMed ]
- Long RJ, Zhu YS, Wang AP. Cluster headache due to structural lesions: A systematic review of published cases. World J Clin Cases. 2021 May 16;9(14):3294-3307. [ PMC free article ] [ PubMed ]
- Grangeon L, O’Connor E, Danno D, Ngoc TMP, Cheema S, Tronvik E, Davagnanam I, Matharu M. Is pituitary MRI screening necessary in cluster headache ? Cephalalgia. 2021 Jun;41(7):779-788. [ PMC free article ] [ PubMed ]

























{kind=link}