

Intercostal neuralgia, a disorder characterized by sharp pain along the intercostal nerves between the ribs, can lead to significant deterioration in quality of life.
Introduction
For those who suffer from it, finding effective solutions to relieve this throbbing pain is often a complex quest. In this context, osteopathy emerges as a promising approach that aims to treat intercostal neuralgia by addressing its underlying physiological aspects.
Osteopathy, as an alternative medical discipline, is distinguished by its holistic approach focused on the gentle manipulation of tissues, joints and muscles to restore the structural and functional balance of the body. In the specific case of intercostal neuralgia, osteopathic practitioners undertake a careful assessment to identify possible imbalances, movement restrictions and tension in the affected areas, particularly in the vertebrae, ribs and surrounding tissues.
Osteopathic techniques often include precise joint manipulations, targeted muscle stretching, and gentle mobilizations. These interventions aim to promote blood and lymphatic circulation, reduce local inflammation, and relieve pressure on the intercostal nerves. By acting in a non-invasive manner, osteopathy offers a complementary approach that can help relieve the symptoms of intercostal neuralgia.
Many patients report significant improvement in their condition after regular osteopathy sessions. It is important to emphasize that osteopathy does not just treat symptoms in isolation, but also focuses on identifying and treating the underlying causes of intercostal neuralgia. This comprehensive approach helps to provide lasting results and improve the quality of life of affected individuals.
However, it is important to emphasize that each case of intercostal neuralgia may present unique particularities, and consultation with a qualified health professional is recommended to assess the suitability of osteopathy as a complement or alternative to conventional treatments. By collaborating with other health professionals, osteopathic practitioners can play a crucial role in the integrated management of intercostal neuralgia.
Definition
Intercostal neuralgia is characterized by neuropathic pain along the affected intercostal nerves, which may present as sharp, shooting, burning, or stabbing pain in the ribs, chest, or abdomen. Often associated with abnormal sensations such as numbness and tingling, this pain may be intermittent or constant. It usually presents as a band of pain enveloping the chest and back or follows a thoracic dermatomal pattern. Even after resolution of the underlying condition, the pain may persist for an extended period of time.
Symptoms are primarily sensory, although motor function impairment may occur in severe cases. Although the causal mechanisms of the disease vary, the pathways of pain transmission remain the same, resulting in similarities in treatment approaches.
Pathophysiology of intercostal neuralgia
- Nerve irritation or compression: Intercostal neuralgia is often triggered by irritation or compression of the intercostal nerves. This irritation can result from a variety of causes such as a herniated disc, inflammation due to a viral infection such as herpes zoster, tumors, trauma, or age-related degenerative changes.
- Inflammatory response: When there is irritation or compression of the nerves, an inflammatory response may occur. This inflammation can increase the sensitivity of the nerves, contributing to the pain and other symptoms associated with intercostal neuralgia.
- Neuropathic pain: Intercostal neuralgia is often characterized by neuropathic pain, which is pain associated with the nervous system. Irritation of the nerves can lead to abnormal activation of pain pathways, sending pain signals to the brain even in the absence of external painful stimuli.
- Impaired nerve transmission: Irritation of the nerves can impair the normal transmission of nerve signals. This can result in abnormal sensations such as tingling, numbness, or skin hypersensitivity in the affected area.
- Pain Reference: Intercostal neuralgia pain may be felt along the affected intercostal nerves, but it may also be referred to other areas of the body. For example, irritation in a specific area may cause pain to radiate along the nerves, affecting areas far from the original area.
- Muscle reaction: In response to pain, the intercostal muscles and surrounding muscles may contract or spasm, which can worsen pain and contribute to decreased thoracic mobility.
- Impact on quality of life: Persistent pain and symptoms associated with intercostal neuralgia can have a significant impact on quality of life, often resulting in limitation of daily activities, breathing difficulties and sleep disturbances.
Causes of Intercostal Neuralgia
- Herpes Zoster (Shingles): A common cause of intercostal neuralgia is the herpes zoster virus, which causes shingles. After infection with the virus, persistent pain may develop along the affected intercostal nerves.
- Nerve Compression: Compression of the intercostal nerves can occur due to a variety of conditions, including:
- Herniated disc: A displaced spinal disc can put pressure on the intercostal nerves.
- Chest trauma: Physical injuries, such as fractures or bruises, can cause nerve compression.
- Tumors: Thoracic tumors can compress the intercostal nerves and cause pain.
- Thoracic surgery: Surgical procedures performed on the chest, such as heart surgery or thoracotomy, can cause irritation of the intercostal nerves.
- Respiratory infections: Respiratory tract infections, such as bronchitis or pneumonia, can sometimes lead to intercostal neuralgia.
- Floating Rib Syndrome: This syndrome occurs when the lower rib is not attached to the sternum, which can cause irritation of the intercostal nerves.
- Thoracic spondylosis: Degeneration of the thoracic vertebrae can lead to structural changes that compress the intercostal nerves.
- Repetitive activities: Certain repetitive activities or excessive movements of the torso can cause irritation of the intercostal nerves.
Symptom of Intercostal Neuralgia
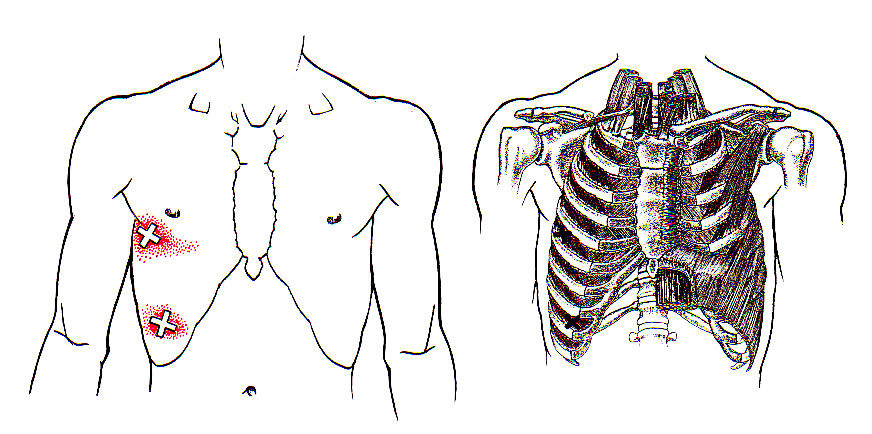
Intercostal neuralgia is characterized by sharp, stabbing pain that radiates around the ribcage, often wrapping from the back to the front of the chest. This pain can be sudden and intense, resembling an electric shock, or it may present as a deep, persistent ache. The discomfort is typically exacerbated by movements such as twisting, bending, or taking deep breaths, and can be triggered by simple activities like coughing, sneezing, or even laughing. Some individuals also experience tingling, numbness, or a burning sensation in the affected area. The pain can be constant or intermittent, but it is usually severe enough to interfere with daily activities and quality of life.
- Chest pain: Pain is the main symptom of intercostal neuralgia. It can be sharp, throbbing or burning and is often described as an electric pricking sensation.
- Location of pain: The pain follows the course of the intercostal nerves and is usually located on the side of the torso. It may radiate forward or backward.
- Worse with movement: Movements of the torso, such as coughing, sneezing, rotating the trunk, or even deep breathing, can make the pain worse.
- Skin hypersensitivity: The skin over the affected area may become more sensitive to touch. Tight clothing or direct contact with the skin may be uncomfortable.
- Belt-like pain: Pain can sometimes surround the chest like a belt, following the course of the intercostal nerves.
- Tingling or Numbness: Some individuals may experience tingling or a numb sensation in the affected area.
- Burning sensations: The pain may be accompanied by burning sensations, adding to the discomfort felt by the person.
- Difficulty breathing deeply: Due to the pain associated with breathing movements, some people may avoid taking deep breaths, which can lead to shallow breathing.
- Muscle cramps: The intercostal muscles may contract in response to pain, causing cramps or spasms.
- Muscle tension: The affected area may have increased muscle tension in response to pain.
A Day in the Life of Someone Suffering from Intercostal Neuralgia
The day begins early, often before the first light of dawn. The sharp, stabbing pain radiating around the ribcage has become an unwelcome alarm clock, rousing the sufferer from sleep. Intercostal neuralgia, a condition characterized by nerve pain along the intercostal nerves, has a way of making its presence known at the most inconvenient times.
Getting out of bed is a careful process, requiring a slow, deliberate movement to avoid aggravating the nerves. The pain, which may feel like a persistent, deep ache or a sudden electric shock, can be triggered by the slightest twist or bend. As the individual sits on the edge of the bed, taking a moment to steady their breathing, they mentally prepare for the day ahead, knowing that each activity will need to be approached with caution.
Mornings are the most challenging. Basic tasks such as brushing teeth or getting dressed become Herculean efforts. Lifting the arms to pull on a shirt can send waves of pain across the chest and back, making the person hyper-aware of every movement. The pain is relentless, sometimes sharp and burning, other times dull and throbbing, but always there, a constant companion.
Breakfast, a simple affair, is often more about convenience than enjoyment. Sitting in a rigid chair exacerbates the discomfort, so the sufferer opts for a cushioned seat, though even that provides only minimal relief. As they sip on a cup of coffee, they might feel a fleeting sense of normalcy, but it’s short-lived. The act of eating or drinking can sometimes intensify the pain, particularly if it causes a slight hiccup or the need to take a deep breath.
Work, whether at home or in an office, presents its own set of challenges. If the person works at a desk, sitting for prolonged periods can be excruciating. Every hour, they stand up, stretch carefully, and walk around, trying to alleviate the pressure on their ribs and back. Concentration is difficult when each breath reminds them of the pain.
Tasks that require physical exertion, like lifting or carrying, are nearly impossible. Even holding a phone to the ear for too long can trigger a spasm. The sufferer becomes adept at finding ways to minimize movement—using hands-free devices, adjusting their posture frequently, and avoiding actions that require twisting or bending.
By midday, fatigue sets in. The constant battle with pain is draining, both physically and mentally. A nap might provide some respite, but even rest is elusive when lying down brings little comfort. Afternoon activities are approached with a mixture of determination and dread, knowing that each one could set off another bout of pain.
Evenings are spent in quiet activities—reading, watching television, anything that allows the person to stay still. Social interactions are limited; laughter, which once brought joy, now brings sharp stabs of pain if it forces deep breaths. By the time night falls, the person is exhausted, though sleep is not guaranteed. They go to bed hoping for a few hours of uninterrupted rest, knowing that another painful day awaits.
Living with intercostal neuralgia is a constant balancing act, where each movement must be measured, each task carefully considered. The pain is always there, shaping every moment of the day, reminding the sufferer of the fragility of their own body.
Biomechanics of intercostal neuralgia
- Nerve Compression: One of the most common causes of intercostal neuralgia is compression of the intercostal nerves. This compression can result from a variety of conditions, such as a herniated disc, muscle compression, inflammation, or even a tumor. The biomechanics of the spine and surrounding structures can influence the pressure placed on the intercostal nerves.
- Posture: Poor posture, especially if it places excessive pressure on the spine or nerves, can contribute to intercostal neuralgia. Incorrect posture can create biomechanical imbalances that affect the distribution of loads on the spine and adjacent structures.
- Spinal mobility: Reduced mobility or stiffness in the spine, particularly in the thoracic region, may increase the risk of intercostal neuralgia. Normal spinal biomechanics require adequate range of motion to avoid excessive pressure on the nerves.
- Muscle Dysfunction: The intercostal muscles and surrounding muscles play a critical role in thoracic biomechanics. Excessive muscle tension, spasms, or imbalances can contribute to compression of the intercostal nerves.
- Repetitive activities: Repetitive movements or activities that place excessive strain on the thoracic region can lead to biomechanical stresses, increasing the risk of intercostal neuralgia. This may include specific occupational or sporting activities.
- Trauma: Physical trauma, such as car accidents or falls, can disrupt the normal biomechanics of the spine and intercostal nerves, contributing to the development of intercostal neuralgia.
Myofascial Trigger Points and Intercostal Neuralgia
Myofascial trigger points and intercostal neuralgia are two interconnected concepts in muscle and nerve health. Myofascial trigger points, often referred to as “knot points,” are specific areas of muscle tension and contraction that can cause local or referred pain. Intercostal neuralgia, on the other hand, involves irritation or compression of the intercostal nerves located between the ribs.
In the context of intercostal neuralgia, myofascial trigger points may play a significant role. These tender points in the intercostal muscles or surrounding muscles can contribute to irritation of the intercostal nerves. When activated, these trigger points can cause local pain as well as referred pain along the intercostal nerves, thereby exacerbating the symptoms of intercostal neuralgia.
Treatment of myofascial trigger points can be an important component of managing intercostal neuralgia. Treatment approaches may include manual techniques, such as myofascial release and trigger point release, as well as strengthening and stretching exercises targeting the involved muscles.
Osteopathy and intercostal neuralgia
Osteopathic treatment of intercostal neuralgia may involve a variety of techniques to relieve muscle tension, improve thoracic mobility, and reduce irritation of the intercostal nerves. The use of trigger points (or trigger points) in the intercostal muscles is a specific osteopathic approach that may be beneficial. Here is how osteopathy may approach the treatment of intercostal neuralgia, highlighting the use of trigger points and mentioning another technique:

- Trigger Point Release: The osteopath can apply myofascial release techniques to identify and release trigger points in the intercostal muscles. These tender, tight points can be a source of pain and contribute to nerve irritation. By applying specific pressure and releasing these points, the osteopath can promote muscle relaxation and relieve the pain associated with intercostal neuralgia.
- Holistic Approach: Osteopathy takes a holistic approach, considering the body as a whole. The osteopath may assess other structures such as the diaphragm, abdominal muscles and adjacent structures to ensure that overall musculoskeletal balance is preserved. Adjustments may be made to improve the patient’s overall biomechanics.
- Postural Exercises and Advice: In addition to manipulations and manual techniques, the osteopath can recommend specific exercises and provide postural advice. These measures aim to strengthen the muscles involved, prevent recurrence and promote healthy posture to reduce pressure on the intercostal nerves.
References
- Williams EH, Williams CG, Rosson GD, Heitmiller RF, Dellon AL. Neurectomy for treatment of intercostal neuralgia . Ann Thorac Surg. 2008 May;85(5):1766-70. [ PubMed ]2.
- Samlaska S, Dews TE. Long-term epidural analgesia for pregnancy-induced intercostal neuralgia . Bread. 1995 Aug;62(2):245-248. [ PubMed ]3.
- Keller SM, Carp NZ, Levy MN, Rosen SM. Chronic post thoracotomy pain. J Cardiovasc Surg (Torino). 1994 Dec;35(6 Suppl 1):161-4. [ PubMed ]4.
- Santos PS, Resende LA, Fonseca RG, Lemônica L, Ruiz RL, Catâneo AJ. Intercostal nerve mononeuropathy: study of 14 cases. Arq Neuropsiquiat. 2005 Sep;63(3B):776-8. [ PubMed ]5.
- Gerner P. Postthoracotomy pain management problems. Anesthesiol Clin. 2008 Jun;26(2):355-67, vii. [ PMC free article ] [ PubMed ]6.
- Peng Z, Li H, Zhang C, Qian PLoS One. 2014;9(2):e90014. [ PMC free article ] [ PubMed ]7.
- Maguire MF, Ravenscroft A, Beggs D, Duffy JP. A questionnaire study investigating the prevalence of the neuropathic component of chronic pain after thoracic surgery. Eur J Cardiothorac Surg. 2006 May;29(5):800-5. [ PubMed ]8.
- Dajczman E, Gordon A, Kreisman H, Wolkove N. Long-term postthoracotomy pain. Chest. 1991 Feb;99(2):270-4. [ PubMed ]9.
- Perttunen K, Tasmuth T, Kalso E. Chronic pain after thoracic surgery: a follow-up study. Acta Anaesthesiol Scand. 1999 May;43(5):563-7. [ PubMed ]10.
- Steegers MA, Snik DM, Verhagen AF, van der Drift MA, Wilder-Smith OH. Only half of the chronic pain after thoracic surgery shows a neuropathic component. J Pain. 2008 Oct;9(10):955-61. [ PubMed ]11.
- Kalso E, Perttunen K, Kaasinen S. Pain after thoracic surgery. Acta Anaesthesiol Scand. 1992 Jan;36(1):96-100. [ PubMed ]12.
- Gotoda Y, Kambara N, Sakai T, Kishi Y, Kodama K, Koyama T. The morbidity, time course and predictive factors for persistent post-thoracotomy pain. Eur J Pain. 2001;5(1):89-96. [ PubMed ]13.
- Rogers ML, Duffy JP. Surgical aspects of chronic post-thoracotomy pain. Eur J Cardiothorac Surg. 2000 Dec;18(6):711-6. [ PubMed ]14.
- Bayman EO, Brennan TJ. Incidence and severity of chronic pain at 3 and 6 months after thoracotomy: meta-analysis. J Pain. 2014 Sep;15(9):887-97. [ PubMed ]15.
- Beuerlein KG, Strowd LC. Multidermatomal herpes zoster: a pain in the neck? Dermatol Online J. 2019 Nov 15;25(11) [ PubMed ]16.
- Gershon AA, Gershon MD, Breuer J, Levin MJ, Oaklander AL, Griffiths PD. Advances in the understanding of the pathogenesis and epidemiology of herpes zoster. J Clin Virol. 2010 May;48 Suppl 1(Suppl 1):S2-7. [ PMC free article ] [ PubMed ]17.
- Forbes HJ, Thomas SL, Smeeth L, Clayton T, Farmer R, Bhaskaran K, Langan SM. A systematic review and meta-analysis of risk factors for postherpetic neuralgia . Bread. 2016 Jan;157(1):30-54. [ PMC free article ] [ PubMed ]18.
- Gauthier A, Breuer J, Carrington D, Martin M, Rémy V. Epidemiology and cost of herpes zoster and post-herpetic neuralgia in the United Kingdom. Epidemiol Infect. 2009 Jan;137(1):38-47. [ PubMed ]19.
- Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007 Nov;82(11):1341-9. [ PubMed ]




")





















{kind=link}