

Introduction
Lateral patellar compression syndrome is a painful knee condition that results from a disruption of the normal movement of the patella along the groove of the femur. This condition, also known as patellofemoral syndrome, is characterized by excessive compression of the patella on the outer side of the joint.
The complex pathophysiology involves anatomical, muscular and biomechanical factors, creating an imbalance which can lead to irritation or even wear of the articular cartilage. Symptoms include pain around the anus or rectum, muscle spasms, difficulty defecating, and rectal pressure. This condition requires a multidisciplinary treatment approach, including physical therapy, targeted exercises, and in some cases, more advanced interventions to restore stability and normal movement of the kneecap.
Understanding the causes, symptoms and treatment options is essential for effective management of this common knee syndrome. The patella is displaced laterally and its medial facet rubs excessively on the lateral condyle of the femur. Without correction, the cartilage on the lateral facet will be worn prematurely. It’s a common complaint among runners, jumpers and other athletes such as skiers, cyclists and football players.
Causes
Lateral compression patella syndrome, also known as patellofemoral syndrome, is often attributed to a combination of anatomical, biomechanical, and environmental factors. This condition is characterized by irritation and pain around the kneecap, usually aggravated by activities involving the knee, such as running, going up and down stairs, and repeated bending. A muscular imbalance between the quadriceps and hip muscles, influencing the path of the kneecap during movement, is a common cause.
Additionally, anatomical abnormalities such as malalignment of the patella or variations in the bony morphology of the femur or patella may contribute to the development of the syndrome. Sports or occupational activities involving repetitive knee movements, as well as acute trauma or repetitive strain injuries, can also overload and irritate the structures around the patella. Muscular imbalances and anatomical abnormalities can lead to poor joint mechanics, increasing stress on the patella and contributing to the syndrome. Other factors such as excess weight, improper footwear, or poor training technique can worsen symptoms. In the treatment of lateral compression patella syndrome, osteopaths can play an important role in assessing and correcting structural imbalances and improving overall musculoskeletal function. Osteopathic interventions may include joint manipulation techniques, muscle stretching, and advice on ergonomics and activity modifications to reduce stress on the patella and promote healing. An individualized approach that addresses the specific needs of each patient is essential to optimize the results of osteopathic treatment of lateral patellar compression syndrome and improve the quality of life of patients.
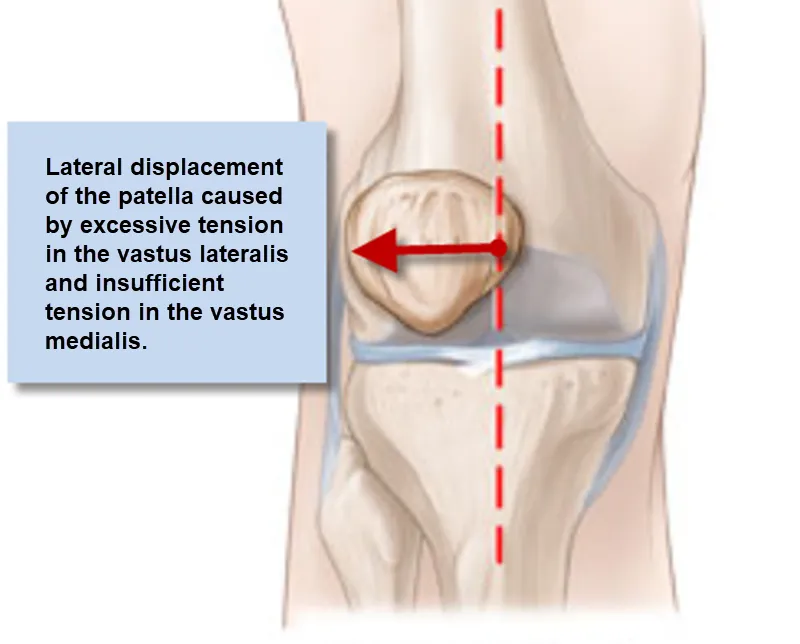
The alignment of the knee, symbolized by the red dotted line, shows the lateral deviation of the patella outward, away from its optimal central alignment. This type of issue can occur due to factors such as overuse, anatomical abnormalities, or poor biomechanics.
Treatment generally includes strengthening exercises to correct the muscle balance, particularly by reinforcing the vastus medialis oblique (VMO) and stretching the lateral muscles, along with manual therapies to improve joint mobility and reduce muscle tension.
- Muscle dysfunction: Muscle imbalance or weakness, particularly in the quadriceps muscles and hip group muscles, can influence the movement of the patella. If the muscles don’t work together properly to guide the kneecap into the proper path, it can lead to lateral compression.
- Poor biomechanics: Biomechanical abnormalities such as poor alignment of the lower limbs, joint instability or deviation from the normal trajectory of the patella can contribute to lateral compression.
- Anatomical factors: Some individuals may have anatomical characteristics that predispose to this syndrome, such as an unusual shape of the patella or an abnormal angle between the femur and the patella.
- Overuse: Activities that frequently put stress on the knees, such as running, repeated jumping, or frequent flexion and extension movements, can contribute to irritation and lateral compression of the kneecap.
- Joint instability: A lack of stability in the knee joint can lead to abnormal movements of the patella, thereby promoting lateral compression.
- Postural defects: Poor posture, particularly during physical activities, can influence the trajectory of the patella and lead to lateral compression.
- Inappropriate footwear: Footwear that does not provide adequate support or is not adapted to individual biomechanics can contribute to lateral compression of the patella.
- Trauma: Previous knee injuries, such as sprains or fractures, can affect the normal trajectory of the patella, increasing the risk of lateral compression.
- Hyperpronation: Excessive pronation of the foot can influence the rotation of the tibia, thus affecting the trajectory of the patella.
- Uneven muscle tension: Uneven tension between the inner and outer thigh muscles can lead to unbalanced forces on the kneecap, promoting lateral compression.

Lateral patellar compression occurs when the patella is pulled toward the outside of the femoral trochlea, which can result in premature wear of the cartilage, commonly known as patellofemoral pain syndrome. Osteopathic treatment and muscle-strengthening exercises, particularly focusing on the vastus medialis oblique (VMO), are often recommended to restore alignment and reduce symptoms.
This X-ray clearly illustrates the patellar misalignment, aiding in accurate diagnosis and guiding therapeutic interventions to improve knee function and alleviate pain.
- Poor tracking results in a concentration of pressure on the external part of the patella (lateral facet).
- The retinaculum on the inner part of the knee is stretched while the retinaculum on the outer part of the knee shortens over time.
- The pain is worse when the knee is bent or when the quadriceps muscle is active or both (each causing a force on the kneecap).
Pathophysiology
The pathophysiology of lateral patellar compression syndrome involves a disruption in the normal movement of the patella along the groove of the femur, with a tendency for compression on the lateral side of this joint. Several underlying mechanisms may contribute to this condition, including anatomical, muscular, and biomechanical factors. Here is a more detailed explanation of the pathophysiology:
- Anatomy of the Patella: The patella (patella) is a diamond-shaped bone located at the front of the knee. It articulates in a groove in the femur called the femoral trochlea. Movement of the patella within this groove is essential to allow normal extension and flexion of the knee.
- Muscle Dysfunction: The quadriceps muscles, particularly the vastus medialis and vastus lateralis, play a crucial role in the movement of the patella. A muscular imbalance, weakness of the vastus medialis or hyperactivity of the vastus lateralis can lead to uneven traction of the patella, thus promoting lateral compression.
- Biomechanical Instability: Biomechanical instability of the knee can lead to abnormal movements of the patella. This may include poor alignment of the lower extremities, excessive pronation of the foot, abnormal rotation of the tibia, or lateral deviation of the patella during movement.
- Articular Cartilage Irritation: Constant lateral compression can lead to irritation of the articular cartilage of the patella and femoral trochlea. This can lead to degenerative changes, such as cartilage wear and tear, contributing to pain and inflammation.
- Anatomical Factors: Some individuals may have anatomical characteristics predisposing to lateral compression of the patella, such as abnormal tilt or rotation of the patella.
- Overuse: Repetitive activities involving flexion and extension of the knee, such as running or jumping, can lead to overuse and contribute to lateral compression.
- Inflammation and Swelling: Chronic lateral compression can cause inflammation of surrounding structures, including tendons, ligaments and joint capsules, leading to swelling.
- Role of Neuropathic Pain: In some cases, components of neuropathic pain may be present, where surrounding nerves are affected, contributing to the amplification of pain.
Symptoms
- Pain on the outer side of the knee: Pain is often felt on the outer side of the kneecap, near the knee joint line. This pain may be intermittent or constant.
- Pain worse with activity: Pain tends to get worse during or after activities that put strain on the knees, such as walking, running, going up or down stairs, jumping, or even prolonged sitting .
- Grinding or cracking sensation: Some individuals may feel a grinding, cracking, or rubbing sensation in the kneecap when they bend or extend the knee.
- Difficulty fully bending or extending the knee: Limitations in full knee flexion or extension may occur due to lateral compression of the patella.
- Joint instability: Some individuals may experience a feeling of instability or weakness in the knee, especially when trying to bear weight on the affected leg.
- Tenderness to touch: The area around the kneecap may be tender to touch, and light pressure may trigger or worsen the pain.
- Swelling: In some cases, slight swelling may develop around the kneecap due to irritation and inflammation.
- Pain with prolonged sitting: Symptoms can be exacerbated when a person sits for a prolonged period of time, putting constant pressure on the kneecap.
Correction
Correction of lateral patellar compression syndrome generally involves a multidisciplinary approach, combining interventions aimed at reducing pain, restoring muscular balance, improving knee biomechanics, and preventing recurrence. Here are some commonly used strategies to correct this condition:
- Osteopathy: Osteopathy sessions are essential to strengthen the quadriceps muscles, with emphasis on the vastus medialis. Targeted exercises may be prescribed to improve muscle stability and balance, helping to guide the kneecap into a more central path.
- Stretching: Regular stretching can help improve the flexibility of the muscles around the knee, thereby reducing muscle tension and promoting smoother movement of the kneecap.
- Orthotics: The use of orthotics, such as orthotic insoles, can help correct biomechanical abnormalities in the foot, contributing to better knee alignment.
- Taping: Taping can be used to provide temporary support by guiding the kneecap into a more central path. Taping techniques can be taught by a healthcare professional.
- Activity Changes: It may be necessary to temporarily modify or reduce activities that exacerbate symptoms, such as running or jumping exercises, until stability and muscle strength are improved.
- Weight Control: Maintaining a healthy body weight can reduce the load on the knees, helping to relieve pressure on the kneecap.
- Anti-inflammatories: Anti-inflammatory medications may be prescribed to reduce inflammation and relieve pain.
- Intra-Articular Injections: In some cases, injections of anti-inflammatories or corticosteroids directly into the joint may be considered to relieve inflammation.
Exercise
It is important to note that specific exercise prescription should be tailored to each individual based on their health, fitness level and the recommendations of their healthcare professional. However, here are some examples of exercises that may be beneficial for strengthening the vastus medialis, stretching the vastus lateralis, and working on the musculature surrounding the knee in the context of lateral patellar compression syndrome:
1. Strengthening the Vastus Medialis:
- Decline Quadriceps Extensions: Lie on your stomach with a rolled-up towel under your knee. Squeeze your buttocks and gently lift your leg, extending your knee. Hold the position for a few seconds and come back down.
- Mini Decline Squats: Standing with feet shoulder-width apart, perform mini squats keeping the weight centered in the heels. Make sure your knees do not extend past your toes.
2. Vastus Lateralis Stretch:
- Standing Vastus Lateralis Stretch: In a standing position, cross the leg to be stretched behind the other leg. Gently tilt the torso away from the crossed leg until you feel a stretch along the side of the hip and knee.
- Quadriceps Stretch with Rotation: In a standing position, bend the leg to be stretched, grab your ankle with the hand on the same side, and bring the heel towards the buttocks. Add an outward knee rotation to target the vastus lateralis.
3. General Strengthening of the Muscles Around the Knee:
- Hip Extensions: Lie on your back with your knees bent. Lift the hips by contracting the buttocks and thigh muscles to create a straight line from shoulders to knees.
- Balance Exercises: Standing on one leg, engage your core and maintain balance for 30 seconds to 1 minute. Vary by adding arm movements or closing your eyes.
Conclusion
In conclusion, lateral patellar compression syndrome presents a significant challenge to those who suffer from it, affecting quality of life and daily mobility. This often underdiagnosed condition requires a proactive approach to alleviate pain and restore normal knee function. Physiotherapy plays a vital role in strengthening the vastus medialis, stretching the vastus lateralis, and rebalancing the muscular forces around the knee. Biomechanical adjustments, specific exercises, and sometimes surgical interventions are key elements of treatment.
It is imperative that individuals experiencing potential symptoms of lateral patellar compression syndrome promptly consult a healthcare professional. Early diagnosis and appropriate intervention can often prevent symptoms from getting worse and help avoid long-term complications.
By continuing to raise awareness of this condition and encouraging a holistic approach to management, we can improve the understanding and treatment of lateral patellar compression syndrome. This will allow individuals to regain normal knee function and return to an active, pain-free life.
References
- Sanchis-Alfonso V. Springer; London: 2006. Anterior knee pain and patellar instability.
- Post W.R. Anterior knee pain: Diagnosis and treatment. J Am Acad Orthop Surg. 2005;13:534–543. – PubMed
- Witvrouw E., Callaghan M.J., Stefanik J.J. Patellofemoral pain: Consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver, September 2013. Br J Sports Med. 2014;48:411–414. – PubMed
- Zaffagnini S., Dejour D., Arendt E. Springer Verlag; Berlin: 2010. Patellofemoral pain, instability, and arthritis.
- Larson R.L., Cabaud H.E., Slocum D.B., James S.L., Keenan T., Hutchinson T. The patellar compression syndrome: Surgical treatment by lateral retinacular release. Clin Orthop Relat Res. 1978;134:158–167. – PubMed



 Weakness: Causes, Implications, and Solutions")










 of the knee")

 Injuries in Athletes")

{kind=link}