

Introduction to Lumbar Facet Syndrome
Lumbar facet syndrome is a leading cause of chronic low back pain, often underdiagnosed due to its symptoms being mistaken for other spinal conditions, such as herniated discs or muscular pain. This condition, stemming from dysfunction or degeneration of the facet joints, significantly impacts patients’ quality of life by restricting mobility and causing persistent discomfort. A comprehensive and individualized therapeutic approach is essential to alleviate symptoms and prevent long-term complications. Osteopathy, with its holistic and manual approach, offers an effective and well-suited solution to this issue.
Facet joints play a vital role in the stabilization and mobility of the spine. Located at the posterior of each vertebra, they facilitate flexion, extension, and rotation while distributing mechanical loads. However, when subjected to repetitive strain, poor posture, or degenerative processes, these joints can become a source of significant pain and stiffness. Lumbar facet syndrome typically presents as localized pain in the lower back, often exacerbated by specific movements such as extension or twisting, and may radiate to the buttocks or thighs.
Osteopathy stands out for its ability to address lumbar facet syndrome comprehensively, targeting not just the symptoms but also the underlying causes of dysfunction. Through a detailed assessment of posture, joint mobility, and muscular tension, the osteopath develops a personalized treatment plan aimed at restoring mechanical and functional balance to the lumbar spine. Techniques such as gentle joint mobilization, myofascial release, and postural corrections are central to this approach. These interventions help reduce pain, enhance mobility, and prevent recurrence.
Furthermore, osteopathy emphasizes preventive care, which is crucial for achieving long-term results. Key aspects include postural education, ergonomic adjustments for work environments, and incorporating specific strengthening and stretching exercises. By guiding patients toward better management of their condition, osteopathy not only improves their quality of life but also minimizes the impact of lumbar facet syndrome.
Warning: The information presented in this article is for informational and educational purposes only. It is not a substitute for professional medical advice. Lumbar facet syndrome is a complex condition that can cause chronic lower back pain, and its diagnosis and management require individualized assessment and care. If you experience similar pain, stiffness, or other symptoms described in this article, it is recommended that you consult a qualified healthcare professional, such as an osteopath or physician, for appropriate care. Self-diagnosis or self-treatment may lead to complications or worsen symptoms.
Definition and Description of Lumbar Facet Syndrome
Lumbar facet syndrome is a prevalent musculoskeletal condition characterized by pain and dysfunction of the facet joints in the lumbar region of the spine. These zygapophyseal joints are essential for spinal stability and mobility. Damage, overuse, or degeneration of these joints can lead to significant pain and restricted function. This condition highlights the critical role of facet joints in maintaining spinal health and mobility.
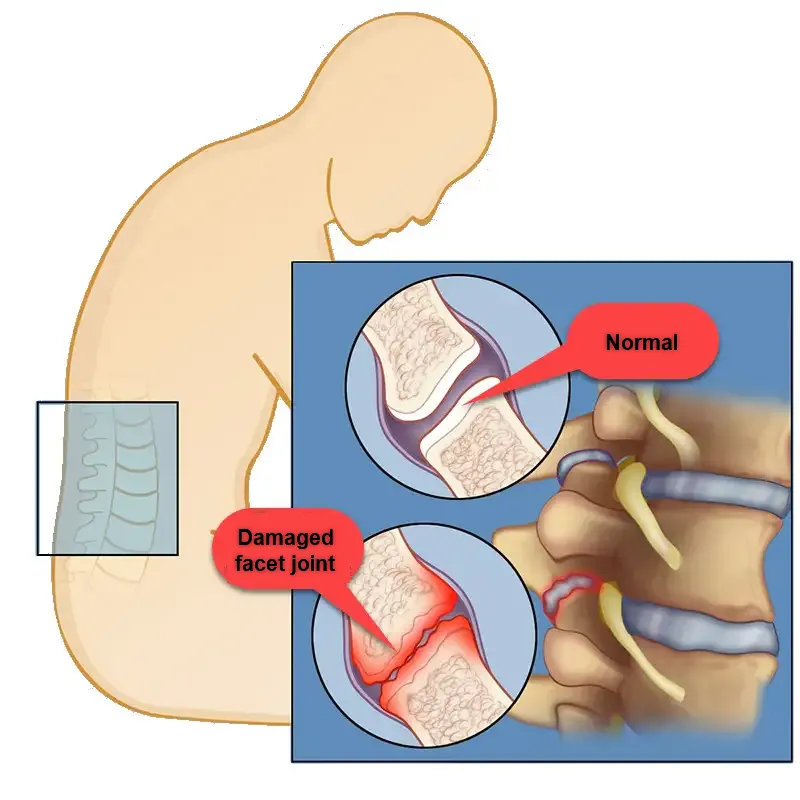
Facet joints connect the vertebrae, providing both stability and flexibility. They are covered in cartilage and encapsulated by a fluid-filled membrane that facilitates smooth motion. Lumbar facet syndrome emerges when wear and tear thin the protective capsule and erode the cartilage. Without adequate lubrication and cushioning, the joints rub against each other, causing inflammation and irritation. This process not only contributes to pain but also promotes further degeneration.
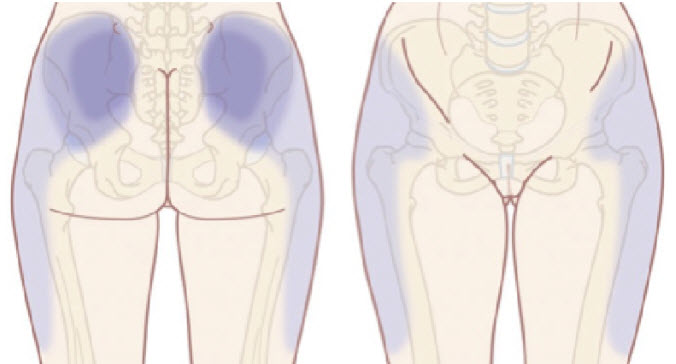
The hallmark of lumbar facet syndrome is pain originating from the facet joints in the lower back. This pain often radiates to the buttocks and thighs. The syndrome can develop acutely, for instance, after trauma or sudden movements, or manifest chronically due to gradual degeneration. Patients frequently report deep, localized pain and stiffness, especially during spine movements such as extension, rotation, or twisting. These movements exacerbate the stress on the inflamed joints, intensifying discomfort.
A distinguishing feature of facet syndrome is its origin in the joints, unlike disc-related pain, which involves intervertebral discs. Facet joints are designed to stabilize the spine and limit excessive movement. When subjected to repetitive mechanical stress, they can lose proper alignment and glide, leading to inflammation and irritation of surrounding sensory nerves. This joint dysfunction disrupts the normal biomechanics of the spine, contributing to chronic pain and stiffness.
It is essential to recognize that lumbar facet syndrome is not exclusive to older individuals. While degenerative changes are more common with aging, repetitive stress, poor posture, and certain occupations can predispose younger individuals to this condition. For example, athletes or individuals with physically demanding jobs may experience premature wear and tear of their facet joints.
Early diagnosis and targeted treatment are crucial for managing lumbar facet syndrome effectively. Non-invasive options like physical therapy, anti-inflammatory medications, and lifestyle modifications can alleviate symptoms and restore function. In more severe cases, interventions such as facet joint injections or radiofrequency ablation may be recommended.
Location and Role of Facet Joints
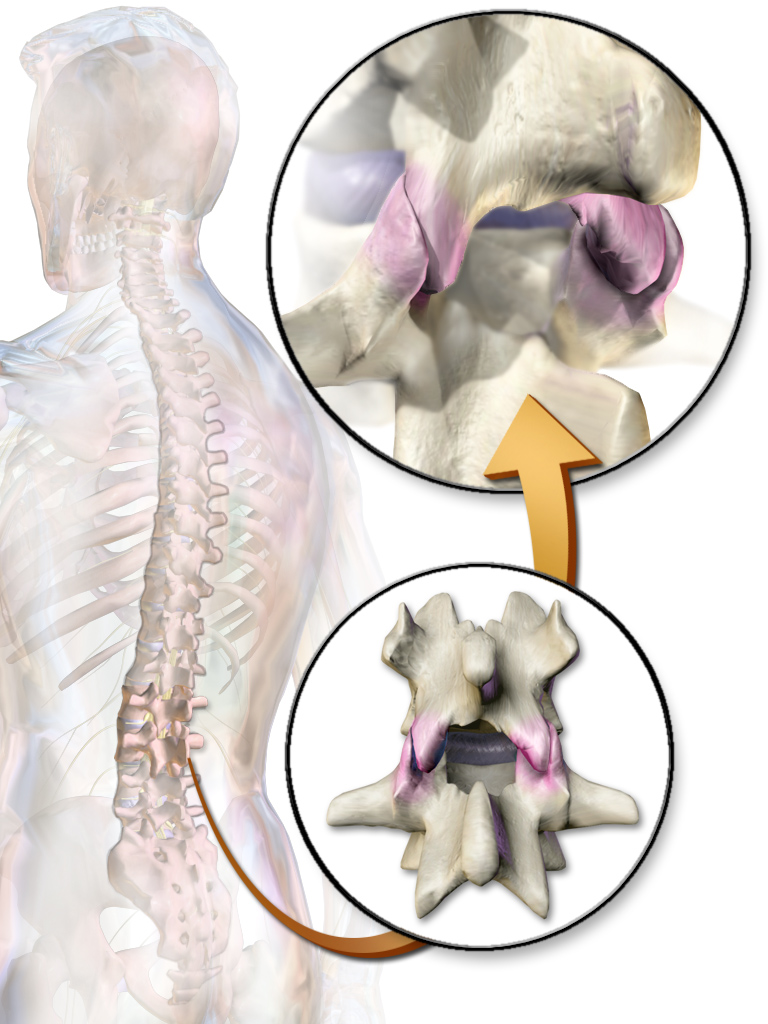
The facet joints, or zygapophyseal joints, are located at the back of each vertebra and are found on either side of the spine. Each vertebra has two pairs of facet joints: an upper pair, which articulates with the vertebra above it, and a lower pair, which articulates with the vertebra below it. The lumbar facet joints play a crucial role in the stability and mobility of the spine. They allow for flexion, extension, and rotation while maintaining spinal alignment and limiting excessive movement that can cause injury.
Structure of Facet Joints
The facet joints, also known as zygapophyseal joints, are essential anatomical structures in the spine that provide stability and enable controlled motion. These joints are found on the posterior side of each vertebra and connect adjacent vertebrae, forming a key part of the vertebral column.
Anatomically, each facet joint comprises two articular surfaces: one from the superior articular process of the lower vertebra and the other from the inferior articular process of the vertebra above. These surfaces are coated with a smooth, protective layer of hyaline cartilage, which minimizes friction and allows for fluid motion. Encasing the joint is a fibrous capsule lined with synovial membrane, which secretes synovial fluid. This fluid lubricates the joint, reducing wear and ensuring smooth articulation during movements such as bending, twisting, or extending the back.
Facet joints are designed to withstand significant loads and provide stability, particularly in the lumbar spine, where they bear much of the body’s weight. They function in conjunction with intervertebral discs to limit excessive movements, such as twisting or shearing, that could compromise the integrity of the spinal column. By distributing mechanical stress, these joints also protect other spinal structures, including discs and ligaments, from damage.
Despite their robust design, facet joints are not immune to degeneration. Over time, the cartilage that cushions the articular surfaces may deteriorate due to aging, repetitive stress, or trauma. This process, known as facet joint osteoarthritis, leads to reduced joint space, increased friction, and the development of bony growths or spurs. These changes can cause pain, stiffness, and a loss of flexibility in the spine. Degeneration in the lumbar region often results in symptoms that interfere with daily activities, such as difficulty bending or twisting.
When facet joints are impaired, they can also trigger reflex pain that radiates to other parts of the body. For example, dysfunction in the lumbar facets may cause pain to spread to the hips, buttocks, or lower limbs. This condition, often referred to as facet joint syndrome, is commonly exacerbated by specific movements, including back extension or lateral rotation.
Causes and Predisposing Factors of Lumbar Facet Syndrome
Aging and Joint Degeneration
One of the most significant factors in the development of lumbar facet syndrome is the age-related process of joint degeneration. As we age, the facet joints undergo progressive wear of cartilage, resulting in loss of flexibility and decreased joint space. This degeneration is often accompanied by inflammation of the facets, the formation of osteophytes (bony growths), and thickening of the joint capsule.
Over time, cartilage loss can cause increased friction between joint surfaces, leading to increased inflammation and pain. Osteophytes can also compress surrounding nerves, causing radiating pain and neurological symptoms. This degenerative process is inevitable with age, but it can be delayed or mitigated by preventive measures, such as correcting posture and maintaining good physical condition.
Bad Posture and Overuse
Poor posture is a major risk factor in the development of lumbar facet syndrome. The spine is designed to be maintained in a natural curvature (lumbar lordosis) to evenly distribute loads and reduce stress on joint structures. However, improper postural habits, such as prolonged sitting or excessive back flexion, can lead to facet misalignment and increase mechanical stress.
Office workers, truck drivers, and people in jobs that involve repetitive movements or prolonged standing are particularly at risk. Athletes, including weightlifters, gymnasts, and tennis players, also put repeated stress on their spine, which can lead to overuse of the facet joints and cause chronic inflammation.
Trauma and Sudden Movements
Direct trauma, such as falls or car accidents, is another common cause of lumbar facet syndrome. A violent impact can cause joint misalignment, tearing of the joint capsule, or cartilage damage, which causes immediate inflammation of the facets. Sudden movements or false movements, especially those involving excessive extension or twisting of the back, can also damage the facets and trigger acute lower back pain.
In conclusion, the facet joints play a pivotal role in both stabilizing the spine and enabling its flexibility. While their structure is well-adapted to resist stress and facilitate movement, these joints are susceptible to wear and tear over time. Understanding their anatomy and function is key to diagnosing and managing conditions like facet joint syndrome and osteoarthritis effectively.
Contact sports, such as rugby or football, put athletes at increased risk of facet injuries due to repeated impacts and unpredictable movements. Similarly, individuals who engage in activities that require heavy lifting without proper technique may be at increased risk of facet dysfunction.
Muscular Imbalances and Postural Compensations
Muscle imbalances are an often underestimated factor in the development of facet dysfunction. When certain stabilizing muscles of the lumbar spine are weakened or contracted, other muscles must compensate, resulting in mechanical overload on the facet joints. For example, weakened abdominal muscles and paravertebral muscles can cause lumbar hyperlordosis, increasing pressure on the posterior facets.
Additionally, tight muscles such as the erector spinae, psoas, or quadratus lumborum can limit lumbar mobility and disrupt spinal alignment. These imbalances and compensations, if left uncorrected, create a vicious cycle of pain and joint dysfunction.
Obesity and Increased Mechanical Stress
Obesity is a significant risk factor for lumbar facet syndrome because excess weight increases the mechanical stresses on the spine. Each additional kilogram adds additional pressure to the lumbar facets, increasing their premature wear. Obese individuals also tend to adopt compensatory postures to support their weight, which further accentuates facet misalignments and dysfunction.
Abdominal fat accumulation can also alter the center of gravity and lead to increased lumbar lordosis, which increases the pressure on the posterior facets. Proper management of body weight through a healthy diet and regular physical activity is crucial to reduce the risk of developing this syndrome.
Genetic Factors and Family Predisposition
Some studies have shown a genetic predisposition to degenerative joint diseases, including facet pathologies. Individuals with a family history of osteoarthritis, spondylitis, or degenerative spinal diseases are at increased risk of developing lumbar facet syndrome. Anatomical features, such as a pronounced lumbar curve or excessive pelvic tilt, may also be inherited and influence the predisposition to facet syndrome.
Risk Factors for Lumbar Facet Syndrome
Lumbar facet syndrome, a common cause of lower back pain, arises from dysfunction or degeneration of the facet joints in the lumbar spine. A variety of factors can increase the risk of developing this condition, many of which are related to lifestyle, occupational habits, and underlying health conditions.
Aging and Degeneration
One of the primary risk factors for lumbar facet syndrome is aging. Over time, the cartilage within the facet joints naturally deteriorates, leading to osteoarthritis. This degenerative process reduces the joints’ flexibility and ability to bear mechanical loads, making them more susceptible to injury and pain. Age-related changes also include the formation of bone spurs, which can further exacerbate joint dysfunction and contribute to nerve irritation.
Repetitive Movements and Poor Posture
Occupational and lifestyle habits significantly influence the health of lumbar facet joints. Jobs or activities that require repetitive bending, twisting, or heavy lifting place considerable strain on the lower back. Poor posture, whether during prolonged sitting, standing, or performing physical tasks, can lead to uneven distribution of weight across the spinal joints, increasing stress on the facets. Over time, these repetitive stresses can cause microtrauma, accelerating the wear-and-tear process.
Trauma and Injury
Sudden trauma, such as from a fall, sports injury, or car accident, can directly damage the facet joints or surrounding structures. The resulting inflammation and instability may contribute to the development of lumbar facet syndrome. Even minor injuries, if left untreated, can lead to chronic joint dysfunction.
Excess Weight and Obesity
Carrying excess body weight places additional pressure on the lumbar spine, particularly the facet joints. This increased mechanical load accelerates joint degeneration and heightens the risk of developing pain and stiffness. Obesity is also associated with systemic inflammation, which may exacerbate joint deterioration.
Sedentary Lifestyle
A lack of regular physical activity contributes to weak core and back muscles, which are essential for supporting the spine. Poor muscle tone can result in greater reliance on the facet joints for stability, leading to increased wear. Prolonged periods of inactivity, such as sitting for hours without breaks, also contribute to joint stiffness and discomfort.
Genetic and Structural Factors
Individuals with a genetic predisposition to conditions like osteoarthritis or abnormalities in spinal alignment, such as scoliosis or lordosis, are at higher risk for lumbar facet syndrome. These structural variations may lead to uneven joint loading and faster cartilage wear.
Mechanisms of Facet Degeneration
Facet joints are synovial joints that stabilize the spine while allowing flexion, extension, and rotation movements. They consist of surfaces covered with hyaline cartilage, surrounded by a joint capsule containing synovial fluid. This fluid lubricates the joint surfaces and protects them against wear. However, several mechanisms can lead to progressive degeneration of the lumbar facets.
1. Cartilaginous Wear
One of the main mechanisms of facet degeneration is the progressive wear of the cartilage covering the articular surfaces. With age, the hyaline cartilage gradually loses its ability to absorb shocks and reduce friction between the articular surfaces. This loss of flexibility and elasticity leads to erosion of the cartilage, exposing the underlying bones to direct friction. This cartilage wear is accelerated by repetitive mechanical stresses, such as twisting, flexion and extension movements, as well as by poor posture.
Cartilage erosion can cause chronic inflammation of the joint, due to the release of inflammatory mediators such as cytokines and prostaglandins. This inflammation contributes to the pain and stiffness experienced by patients with lumbar facet syndrome.
2. Formation of Osteophytes
In response to cartilage wear, the body attempts to compensate for this loss by forming osteophytes, which are bony growths that develop around the facet joints. Osteophytes are intended to stabilize the damaged joint, but their presence can cause compression of surrounding structures, such as sensory nerves and ligaments. Osteophyte formation is a sign of advanced degeneration and can lead to radiating pain and significant functional limitations.
Osteophytes can also reduce joint space and limit facet mobility, further exacerbating the stiffness and pain patients experience. In addition, osteophytes can put pressure on nearby nerve roots, causing radiating pain or neurological symptoms.
3. Lumbar Hyperlordosis and Joint Instability
Lumbar facet degeneration can also be promoted by postural changes, such as lumbar hyperlordosis. Hyperlordosis is an excessive accentuation of the natural curvature of the lumbar spine, which places increased pressure on the posterior facets. This posture increases the compressive forces on the facets and accelerates their wear. In the long term, this wear can lead to joint instability, making the facets more susceptible to repeated injury or inflammation.
Joint instability is often aggravated by muscular imbalances or weakness in the stabilizing muscles of the spine. As a result, the facets are put under increased strain to compensate for this lack of stability, which accelerates their degeneration.
Pathophysiology of Lumbar Facet Syndrome
The pathophysiology of lumbar facet syndrome is characterized by complex mechanisms of joint degeneration that affect the lumbar facets and their impact on surrounding nervous and muscular structures. Understanding these mechanisms is essential to guide management strategies and improve the quality of life of patients. In this section, we will review the processes of facet degeneration and their impact on surrounding nervous and muscular structures.
Mechanisms of Facet Degeneration
Facet joints are synovial joints that stabilize the spine while allowing flexion, extension, and rotation movements. They consist of surfaces covered with hyaline cartilage, surrounded by a joint capsule containing synovial fluid. This fluid lubricates the joint surfaces and protects them against wear. However, several mechanisms can lead to progressive degeneration of the lumbar facets.
1. Cartilaginous Wear
One of the main mechanisms of facet degeneration is the progressive wear of the cartilage covering the articular surfaces. With age, the hyaline cartilage gradually loses its ability to absorb shocks and reduce friction between the articular surfaces. This loss of flexibility and elasticity leads to erosion of the cartilage, exposing the underlying bones to direct friction. This cartilage wear is accelerated by repetitive mechanical stresses, such as twisting, flexion and extension movements, as well as by poor posture.
Cartilage erosion can cause chronic inflammation of the joint, due to the release of inflammatory mediators such as cytokines and prostaglandins. This inflammation contributes to the pain and stiffness experienced by patients with lumbar facet syndrome.
2. Formation of Osteophytes
In response to cartilage wear, the body attempts to compensate for this loss by forming osteophytes, which are bony growths that develop around the facet joints. Osteophytes are intended to stabilize the damaged joint, but their presence can cause compression of surrounding structures, such as sensory nerves and ligaments. Osteophyte formation is a sign of advanced degeneration and can lead to radiating pain and significant functional limitations.
Osteophytes can also reduce joint space and limit facet mobility, further exacerbating the stiffness and pain patients experience. In addition, osteophytes can put pressure on nearby nerve roots, causing radiating pain or neurological symptoms.
3. Lumbar Hyperlordosis and Joint Instability
Lumbar facet degeneration can also be promoted by postural changes, such as lumbar hyperlordosis. Hyperlordosis is an excessive accentuation of the natural curvature of the lumbar spine, which places increased pressure on the posterior facets. This posture increases the compressive forces on the facets and accelerates their wear. In the long term, this wear can lead to joint instability, making the facets more susceptible to repeated injury or inflammation.
Joint instability is often aggravated by muscular imbalances or weakness in the stabilizing muscles of the spine. As a result, the facets are put under increased strain to compensate for this lack of stability, which accelerates their degeneration.
Impact on Nervous and Muscular Structures
The mechanisms of facet degeneration are not limited to the joints themselves, but also have a significant impact on the surrounding nerve and muscle structures. The pain and dysfunction resulting from this degeneration can lead to compensatory reactions and irritation of the surrounding tissues.
1. Irritation of Sensory Nerves
The facet joints are rich in sensory nerve endings, called nociceptors, which transmit pain signals to the central nervous system. When the facets become inflamed or compressed by osteophytes, these nociceptors are activated and send persistent pain signals. This nerve irritation contributes to the deep, shooting pain felt in the lower back, and can also cause pain to radiate to the buttocks or thighs.
Due to their proximity to the lumbar nerve roots, degenerated facets can also cause compression or irritation of the nerves, resulting in radiating pain similar to sciatica. However, unlike disc compression, facet pain is usually limited to the lumbar region and is not accompanied by marked neurological symptoms, such as numbness or muscle weakness.
2. Muscle Reactions and Contractures
Lumbar facet degeneration can also have a significant impact on surrounding muscles. In response to pain and inflammation, the paraspinal muscles and erector spinae may reflexively contract to protect the damaged facets. These prolonged muscle contractions lead to increased stiffness and reduced lumbar mobility, further exacerbating functional limitations.
Muscle contractures can also lead to secondary pain and myofascial tension points, which manifest as local and referred pain. The muscles involved in these compensations are often hypertonic and may be tender to palpation. In addition, these prolonged muscle reactions can create a vicious cycle of pain and joint dysfunction, by increasing stress on already degenerated facets.
3. Postural Imbalances and Compensatory Adaptations
Facet degeneration can also lead to postural imbalances and compensatory adaptations throughout the lumbar spine. Patients with lumbar facet syndrome often adopt protective postures to avoid painful movements, which alters their spinal alignment and places stress on other joint structures. For example, a patient may adopt a slight flexion posture to relieve pressure on the posterior facets, which leads to increased stress on the intervertebral discs and ligaments.
These postural adaptations can worsen existing muscle imbalances and create new areas of joint dysfunction. In the long term, these imbalances can lead to chronic pain and increased functional limitations, requiring comprehensive, multidisciplinary management.
Symptoms and Clinical Manifestations of Lumbar Facet Syndrome
Lumbar facet syndrome presents with a spectrum of clinical symptoms that can vary in intensity and location among individuals. Patients with this syndrome typically report low back pain that is chronic or recurrent, often exacerbated by specific spinal movements. A good understanding of the characteristic symptoms is essential to differentiate this syndrome from other possible causes of low back pain, such as disc or muscle pathologies. In this section, we will review the main symptoms and clinical manifestations associated with lumbar facet syndrome.
Localized Pain in the Lumbar Area
The predominant symptom of lumbar facet syndrome is pain localized to the lower back. This pain is often described as deep, dull, and persistent. Unlike disc pain, which can be sharp and stabbing, facet pain tends to be more diffuse and is often felt on both sides of the spine. It may radiate laterally to the buttocks and sometimes down to the upper thighs, not extending beyond the knees.
Patients frequently report an increase in pain intensity during lateral flexion or extension movements of the back. For example, leaning backward or rotating the trunk can cause an exacerbation of symptoms. This is because these movements place greater strain on the posterior facets, thereby increasing pressure and irritation on already inflamed structures.
Morning Stiffness and Decreased Mobility
Another common symptom in patients with lumbar facet syndrome is morning stiffness. After a period of prolonged rest, especially after waking up, patients may experience significant stiffness in the lower back, accompanied by a sensation of joint locking. This stiffness may improve after a few minutes of movement or stretching, but it tends to recur after prolonged periods of immobility, such as prolonged sitting.
This decrease in lumbar mobility affects everyday movements, such as bending to pick up an object, turning in bed, or getting up from a chair. Patients may also have difficulty performing physical activities, especially those that require flexion or extension of the spine.
Pain radiating to the buttocks and thighs
In some cases, facet pain may extend beyond the lumbar region and radiate to the buttocks or upper thighs. Although this radiation is usually limited to the buttocks, it can sometimes extend to the thighs without ever going beyond the knees, unlike sciatica of disc origin. This radiating pain is often the result of irritation of the sensory nerves near the facet joints, and may be confused with neuropathic pain.
This feature can make the diagnosis more complex, since many lumbar pathologies have similar irradiations. However, the essential difference lies in the absence of neurological symptoms such as numbness, tingling or muscle weakness, which are more common in cases of disc compression.
Pain on Palpation of Facet Joints
During clinical assessment, pain on palpation of the facet joints is a characteristic sign of lumbar facet syndrome. A qualified health professional, such as an osteopath, can apply gentle pressure to the facet joints by locating them on the posterior aspect of the lumbar spine. Pain reproduced during this palpation indicates possible involvement of the facets in the patient’s symptomatology.
It is also common for patients to report increased sensitivity during joint mobilization tests, such as lumbar extension or lateral rotation movements. These tests help assess the response of the facets to movement and confirm the involvement of these joint structures.
Worsening of Pain with Activity and Prolonged Maintenance of Certain Postures
Patients with lumbar facet syndrome frequently report worsening pain with prolonged physical activity or maintaining certain postures. For example, prolonged sitting or standing can cause increased discomfort, due to the continued pressure on the lumbar facets. Similarly, activities requiring twisting or heavy lifting tend to exacerbate symptoms.
This postural and dynamic worsening is a key feature that distinguishes facet syndrome from other sources of low back pain, such as disc pathologies, which are often exacerbated by forward bending movements.
Absence of marked neurological signs
It is important to emphasize that in most cases of lumbar facet syndrome, patients do not present with marked neurological signs, such as numbness, tingling, or muscle weakness in the lower extremities. This absence of neurological signs helps differentiate facet syndrome from disc pathologies, such as disc herniation, which can compress nerve roots and cause significant neurological symptoms.
Neurological symptoms are usually absent because facet syndrome does not directly involve the nerve roots, but rather the posterior joints of the spine. However, it is possible for osteophytes or bony growths formed at the facets to exert partial compression on nearby nerves, resulting in radiating pain.
In summary, the symptoms of lumbar facet syndrome are mainly characterized by local or radiated pain, morning stiffness, tenderness on palpation and aggravation during specific movements or prolonged maintenance of certain postures. These clinical manifestations must be taken into account during the evaluation and management of patients, in order to differentiate this condition from other lumbar pathologies and to implement an appropriate therapeutic strategy.
Diagnosis of Lumbar Facet Syndrome
Diagnosis of lumbar facet syndrome requires a clinical approach and appropriate additional testing to distinguish this condition from other potential causes of low back pain. A complete evaluation, including a detailed history, targeted clinical testing, and imaging studies if necessary, is essential. The diagnostic approach must be rigorous to accurately guide treatment and avoid diagnostic errors. In this section, we will explore in detail the clinical assessment and mobility testing as well as the use of imaging studies to confirm the presence of this syndrome.
Clinical Assessment and Mobility Tests
Clinical evaluation is a crucial step in the diagnosis of lumbar facet syndrome. It consists of a series of questions and physical tests to assess the nature of the pain, aggravating factors, and functional limitations. A complete clinical evaluation begins with a detailed history, followed by mobility and palpation tests to confirm facet involvement.
Complete Anamnesis
The history is the starting point for the clinical assessment. The healthcare professional asks the patient about the history of the pain, its onset, location, and progression over time. Patients with lumbar facet syndrome typically describe pain localized to the lumbar region, often felt on both sides of the spine. This pain is typically aggravated by back extension, rotation, or lateral flexion.
Questions should also include the patient’s lifestyle habits, such as posture at work, physical activities performed, and history of trauma or sudden movements. These elements help identify potential risk factors and guide the clinical evaluation toward a diagnosis of lumbar facet syndrome.
Mobility Tests
Once the anamnesis has been taken, the clinical assessment continues with targeted mobility tests, which aim to reproduce the pain felt by the patient. Mobility tests are used to assess the function of the facet joints and confirm their involvement in the symptomatology. Among the most commonly used tests are:
- Lumbar extension test: This test involves asking the patient to lean back while observing the reactions. The pain triggered during this extension often indicates irritation of the posterior facets, due to the compression exerted on the joints.
- Lateral rotation test: This test assesses pain during trunk rotation. The patient is asked to rotate the torso to the left and then to the right. Pain localized in the lumbar region during these movements indicates possible facet joint involvement.
- Palpation of the facets: During the physical examination, the health professional performs a palpation of the lumbar facets to assess their sensitivity. The reproduction of pain during this palpation is a characteristic clinical sign of lumbar facet syndrome.
These clinical tests are essential to differentiate facet syndrome from other possible causes of lower back pain, such as disc pathologies, muscle pain or ligament damage.
Use of Medical Imaging and Additional Tests
When clinical tests indicate a suspicion of lumbar facet syndrome, medical imaging tests may be necessary to confirm the diagnosis and rule out other pathologies. Imaging tests allow visualization of the bony structures, joints and soft tissues of the lumbar spine. They provide valuable information on the condition of the facet joints, the presence of lesions or signs of degeneration.
Lumbar X-ray
X-rays are often the first imaging test used to evaluate the bony structure of the lumbar spine. Although this test cannot directly visualize the facet joints, it can reveal signs of joint degeneration such as osteophytes, joint space narrowing, or hyperlordosis. X-rays are particularly useful in ruling out other bony causes of low back pain, such as fractures or spinal deformities.
Computed tomography (CT) scan
Computed tomography, or CT scan, is an imaging test that allows detailed visualization of the bony and joint structures of the lumbar spine. Unlike X-rays, CT scans provide a cross-sectional image of the facet joints, which can detect abnormalities such as fractures, joint deformities, or facet hypertrophy. This test is indicated when signs of advanced degeneration are suspected or when nerve compression by osteophytes is considered.
Magnetic Resonance Imaging (MRI)
MRI is the test of choice to evaluate the joint structures and soft tissues of the lumbar spine. This noninvasive test allows visualization of the facet joints, intervertebral discs, ligaments, and surrounding muscles. MRI can reveal facet inflammation, cartilage deformities, or intra-articular effusions. In addition, MRI can rule out other conditions that can cause similar pain, such as herniated discs, lumbar spinal stenosis, or muscle conditions.
Osteopathic Approach
Osteopathy offers a holistic, hands-on approach to the management of lumbar facet syndrome. By addressing the structural and functional imbalances contributing to the condition, osteopathic treatment aims to restore mobility, reduce pain, and improve overall spinal health. Using manual techniques tailored to the patient’s needs, the osteopath seeks to enhance facet joint function while alleviating associated muscular tension and postural issues.
Joint Mobilization Techniques
One of the primary tools in osteopathy for managing lumbar facet syndrome is joint mobilization. This technique involves the application of gentle pressure and rhythmic movements to the affected joints. The goal is to facilitate the gliding of joint surfaces, reduce joint stiffness, and relieve tension around the facets. By carefully mobilizing the lumbar spine, the osteopath helps restore the range of motion to the facet joints without causing excessive strain or discomfort. Joint mobilization is particularly effective in addressing joint locks or restrictions, which are common contributors to facet-related pain.
Myofascial Release
Myofascial release is another key technique used in osteopathic care for lumbar facet syndrome. This method focuses on releasing tension in the myofascial tissues, which include the muscles and the surrounding connective tissues (fascia). Pain from facet joint dysfunction often causes these tissues to become tight or rigid, leading to further discomfort and limited mobility.
Through slow, deliberate movements and sustained pressure, myofascial release helps to ease muscle tightness, improve blood flow, and enhance tissue elasticity. This technique not only alleviates muscle spasms and contractures but also promotes relaxation and a sense of well-being. By addressing the tension in the soft tissues surrounding the lumbar spine, myofascial release contributes to overall spinal health and facilitates better movement patterns.
Gentle Osteopathic Manipulation Techniques
Gentle osteopathic manipulation techniques, such as indirect manipulation and functional methods, are particularly beneficial for patients with lumbar facet syndrome. These techniques focus on releasing joint restrictions and optimizing facet joint function without resorting to high-velocity adjustments that may be inappropriate for some individuals.
Indirect manipulation involves guiding the joint into a position of ease, allowing the body’s natural healing mechanisms to restore balance. Functional techniques, on the other hand, employ controlled, subtle movements to encourage proper alignment and reduce joint tension. Both methods prioritize patient comfort and safety while achieving the therapeutic goal of improving spinal mobility and alleviating pain.
Scientific Evidence on the Benefits of Osteopathic Care for Lumbar Facet Syndrome
Prevalence and Recovery Rate of Low Back Pain and Leg Pain in Osteopathic Practice
N. Chemeris (2007)
This paper highlights the recovery rates for low back and leg pain with osteopathic care, including its effects on lumbar facet issues.
Full Text (PDF)
Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain
S. P. Cohen, S. N. Raja (2007)
This article explores the complexity of lumbar facet joint pain and potential treatments, emphasizing osteopathic approaches.
Full Text (PDF)
The Comparative Efficacy of Spinal Manipulative Therapy and Extracorporeal Shockwave Therapy in the Treatment of Chronic Lumbar Facet Syndrome
L. Khesa (2019)
This study compares osteopathic manipulative therapy with alternative methods for treating lumbar facet syndrome.
Full Text
American Osteopathic Association Guidelines for Osteopathic Manipulative Treatment (OMT) for Patients with Low Back Pain
Guideline Subcommittee (2010)
This document offers guidelines for using osteopathic treatments for low back pain, including facet-related conditions.
Full Text (PDF)
Osteopathic Manipulative Medicine: A Brief Review of the Hands-on Treatment Approaches and Their Therapeutic Uses
A. Roberts et al. (2022)
Reviews osteopathic interventions and their efficacy in treating musculoskeletal conditions, including lumbar facet syndrome.
Full Text (PDF)
Back Pain: Facet Syndrome
P. Rana (2022)
Discusses both osteopathic and acupuncture treatments for axial back pain caused by facet syndrome.
Full Text (Springer)
Immediate Alteration of the Lumbar Intervertebral Foramen During Osteopathic Locking Technique
P. M. Dugailly, W. Salem (2021)
Examines immediate structural changes in the spine from osteopathic techniques.
Full Text (PDF)
Manual Versus Mechanical Force Manipulation in the Treatment of Lumbar Facet Syndrome
J. Liepner (2012)
Compares manual osteopathic manipulative treatments with mechanical alternatives.
Full Text
Foundations of Osteopathic Medicine
American Osteopathic Association (2010)
Comprehensive textbook discussing osteopathic treatments, including applications for lumbar facet syndrome.
Google Books Preview
Therapeutic Effects of Chinese Osteopathy in Patients with Lumbar Disc Herniation
W. Zhang et al. (2013)
Discusses traditional osteopathic methods that are applicable to lumbar facet syndrome.
Full Text (World Scientific)
The Relative Effectiveness of Non-Steroidal Anti-Inflammatory Medication Compared to a Homeopathic Complex in Treating Cervical Facet Syndrome
SE Hepburn (2000)
Compares various treatment approaches, including osteopathic care, for managing facet syndromes.
Full Text (PDF)
Back Pain: Facet Syndrome
P. Rana (2022)
Explores the role of osteopathic manipulation and acupuncture in managing axial low back pain from facet syndrome.
Full Text (Springer)
An Osteopathic Approach to Patients with Degenerative and Herniated Discs
R. Kessler, C. Haase, D. Dean III (2021)
Examines osteopathic care strategies for spinal conditions, including lumbar facet syndrome.
Article Link
American Osteopathic Association Guidelines for Osteopathic Manipulative Treatment (OMT) for Patients with Low Back Pain
Guideline Subcommittee on Low Back Pain (2010)
Outlines osteopathic treatment recommendations for managing lumbar conditions.
Full Text (PDF)
Physiotherapy and Lumbar Facet Joint Injections as a Combination Treatment for Chronic Low Back Pain
H. Chambers (2013)
Discusses the combination of osteopathy with other therapeutic methods for lumbar facet pain.
Article Link
Prevention and Management of Lumbar Facet Syndrome
Prevention and management of lumbar facet syndrome is based on a multidimensional approach aimed at reducing the risks of joint degeneration, relieving symptoms and improving the overall function of the lumbar spine. A combination of postural advice, specific exercises and osteopathic interventions is essential to achieve these goals. In this section, we will examine in detail the strategies for prevention and management of this condition, focusing on postural advice, strengthening exercises and the osteopathic approach.
Postural Advice and Prevention of Overloads
Good posture is essential to maintain the alignment and health of the facet joints. Proper posture helps distribute loads evenly across the spinal structures, reducing mechanical stress on the lumbar facets. In contrast, poor posture, especially prolonged flexion or excessive extension, increases compressive forces on the posterior facets and accelerates their wear.
Postural Education
Postural education aims to make patients aware of the correct positions to adopt in daily activities and at work. Basic advice includes:
- Maintaining a natural lumbar lordosis: It is essential to maintain a neutral lumbar curve when sitting or standing. To achieve this, patients should avoid hunching the lower back forward or arching excessively backward.
- Adopt an ergonomic sitting position: Using ergonomic chairs with good lumbar support can help prevent facet strain. Patients are encouraged to adjust their office chair so that the feet are flat on the floor and the knees are slightly below the hips.
- Avoid sudden twisting movements: Sudden rotational movements of the back should be avoided, especially when lifting weights. Patients should be taught to turn their entire body by pivoting the feet rather than using only the spine.
Reduction of Loads and Lifting Techniques
Preventing overload is also crucial to reducing stress on the lumbar facets. This includes learning proper lifting techniques and avoiding heavy loads or prolonged positions.
- Safe lifting technique: When lifting objects, patients should bend their knees and use their leg muscles to lift the load, while keeping their back straight. This technique reduces pressure on the lumbar facets and limits the risk of injury.
- Alleviation of repetitive loads: For workers performing repetitive tasks, it is recommended to split the loads or take regular breaks to avoid prolonged stress on the spine.
Lumbar Strengthening and Stretching Exercises
Strengthening and stretching exercises are essential to improve lumbar spine stability and flexibility, while reducing stress on the facets. A targeted exercise program helps maintain optimal alignment and prevent muscle imbalances.
Muscle strengthening
Strengthening exercises aim to stabilize the spine by strengthening the paraspinal muscles, abdominals and deep back muscles.
- Strengthening Stabilizer Muscles: Exercises such as abdominal planks, core exercises, and lumbar extensions are particularly effective for strengthening the stabilizing muscles of the spine.
- Deep Abdominal Strengthening Exercises: Exercises targeting the deep abdominal muscles, such as the transverse abdominis, effectively support the lumbar spine and reduce stress on the facets.
Specific Stretches
Stretching aims to improve the flexibility of the muscles and structures around the spine, thereby reducing tension on the facets.
- Erector spinae and quadriceps stretches: The erector spinae and quadriceps muscles, often tight due to poor posture or lumbar hyperlordosis, must be stretched regularly to maintain optimal flexibility.
- Psoas and Hamstring Stretches: The psoas and hamstring muscles are commonly tight in patients with lower back pain. Regular stretching of these muscles can help relieve pressure on the facets and improve mobility.
Osteopathic Treatments for Lumbar Facet Syndrome
Osteopathic treatments are an effective approach to the management of lumbar facet syndrome. Osteopathy, as a holistic manual therapy, aims to restore joint mobility, reduce muscle tension, and improve the function of spinal structures. Specific techniques of gentle joint mobilization, myofascial release, and manual therapy to relieve tension points play a key role in this approach. In this section, we will explore these techniques and their effects on the affected structures.
Gentle Joint Mobilization Techniques
Gentle joint mobilization is an osteopathic technique that aims to restore the range of motion of the facet joints without causing excessive stress. Unlike high-velocity manipulation (HVLA), gentle mobilization techniques involve slow, controlled movements to mobilize the facet joints in a progressive manner.
1. Objectives of Gentle Joint Mobilizations
The main goal of these mobilizations is to reduce the motion restrictions and pain associated with the lumbar facets. The facets are often inflamed or degenerated due to repetitive mechanical stress or cartilaginous degeneration. Gentle mobilizations help improve facet mobility by promoting better gliding between the articular surfaces and reducing friction.
These techniques also help increase the supply of synovial fluid to the joint, which helps lubricate the facets and reduce inflammation. In addition, they stimulate proprioceptive receptors, which improves the perception of spinal alignment and helps correct maladaptive postures.
2. Application of Mobilization Techniques
Gentle joint mobilization techniques are performed with light pressure and oscillatory movements. The practitioner first identifies areas of joint restriction by palpation and observation of the patient’s movements. Then, he or she applies repetitive, low-amplitude movements to the affected facets, targeting the specific restrictions.
Mobilizations are usually performed in the direction of the restriction, with an amplitude and speed adapted to the patient’s tolerance. These techniques are particularly recommended for patients who are sensitive to pain or have contraindications to more invasive spinal manipulations.
Myofascial Release of Surrounding Structures
Myofascial release is a manual technique to relax the muscles and fascia surrounding the lumbar facet joints. The paraspinal muscles, erector spinae, and deep back muscles, such as the multifidus, are often tight or contracted in response to facet inflammation. Myofascial release helps release these muscle tensions and improve blood flow to the affected tissues.
1. Mechanisms and Objectives of Myofascial Release
Fascia is a connective tissue that surrounds muscles, ligaments, and joints. When tight or stiff, it puts pressure on the underlying structures and reduces the mobility of the facets. Myofascial release aims to release this fascia by applying sustained pressure and slow stretches to the tight areas.
The goal of this technique is to reduce muscle stiffness and restore elasticity to the surrounding soft tissues. By releasing fascia and contracted muscles, the flexibility and mobility of the facets is improved, while reducing painful tension points.
2. Myofascial Release Techniques
Myofascial release techniques involve using the hands or forearms to apply sustained pressure to areas of tension. The practitioner first identifies areas of fascial restriction through palpation, then applies gentle, gradual pressure to relax the tissues.
The movements are slow and aim to stretch the fascia in different directions. Myofascial release can be applied directly to the paravertebral muscles or indirectly to surrounding muscles, such as the psoas muscles or quadratus lumborum. These techniques help improve blood circulation and reduce inflammation around the degenerated facets.
Manual Therapy to Relieve Tension Points
Myofascial tension points are hyperirritable areas in the muscles and fascia, often referred to as “trigger points.” These points may be tender to palpation and cause local or referred pain in the lumbar region. Manual therapy aims to relieve these tension points through the application of various release techniques.
1. Identification of Tension Points
Tension points are often the result of prolonged muscle contractions or postural imbalances. They usually form in response to repetitive mechanical stress or chronic inflammation of the facets. During the assessment, the osteopath uses palpation techniques to locate areas of increased sensitivity and muscle stiffness.
2. Ischemic Pressure Techniques
One of the most commonly used techniques to relieve tension points is ischemic pressure. This technique involves applying direct, sustained pressure to the tension point until the pain begins to diminish. Ischemic pressure works by temporarily inhibiting blood flow to the area, which then allows for reoxygenation and relaxation of the muscle fibers.
This technique should be applied gradually, slowly increasing the pressure to avoid aggravating the pain. The patient is encouraged to breathe deeply while the pressure is being applied, to promote muscle relaxation and release of tension points.
3. Post-Isometric Stretching and Release Techniques
Post-isometric stretching is another effective technique for reducing tension points. This method involves gently contracting the muscle in question for a few seconds, then releasing it while gently stretching it. This technique helps to relax the muscle fibers and improve range of motion.
Muscle relaxation techniques, such as contraction-release or functional mobilization techniques, are also used to relieve tension and restore optimal muscle function. These techniques are suitable for patients with chronic pain or significant stiffness.
Beneficial Effects of Osteopathic Treatments
Gentle joint mobilization, myofascial release, and stress point relief techniques offer many benefits for patients with lumbar facet syndrome. They help to:
- Reduce Pain and Inflammation: Gentle mobilizations and myofascial release help improve blood circulation and reduce inflammation around degenerated facets.
- Improve joint mobility: By releasing joint and fascial restrictions, these techniques increase the range of motion of the lumbar facets.
- Correct postural imbalances: Osteopathic interventions target muscular imbalances and postural compensations, thus promoting better stability of the spine.
- Reduce Muscle Tightness: Myofascial release and tension point therapy help release tight muscles and relieve radiating pain.
Complications and Prognosis of Lumbar Facet Syndrome
Lumbar facet syndrome is a common condition that, if not treated appropriately, can lead to significant complications and impair patients’ quality of life. Early and appropriate management is essential to avoid worsening of symptoms and long-term complications. In this section, we will review the possible consequences of lack of treatment and the long-term prognosis of patients with this syndrome.
Possible Evolution Without Treatment
When not adequately managed, lumbar facet syndrome can progress progressively and cause a deterioration in joint and muscle function. This progression is marked by an exacerbation of pain and an increase in functional limitations. Failure to treat can lead to joint, muscle and postural complications.
1. Worsening of Chronic Lower Back Pain
Pain is the most common symptom of lumbar facet syndrome. Without proper management, pain can intensify over time and become chronic. Inflammation and repeated stress on the degenerated facets cause continued irritation of the nerve endings, leading to hypersensitivity and persistent pain.
Worsening pain can impact patients’ daily activities. They may have difficulty sitting, standing, walking, or rotating. These limitations increase the risk of a sedentary lifestyle, which in turn can contribute to muscle deconditioning and worsening of symptoms.
2. Development of Postural Compensations and Muscular Imbalances
If left untreated, patients with lumbar facet syndrome often develop compensatory strategies to avoid painful movements. These compensations may include protective postures, such as adopting constant back flexion or lateral tilt to relieve the affected facets. These postural changes contribute to muscle imbalances and increased stress on other spinal structures.
Prolonged compensations can also lead to pain in other areas, such as the hips, thighs or shoulders. The muscular imbalances created by these maladaptive postures increase the load on the surrounding joints and can promote the appearance of new pathologies, such as chronic muscle pain, myofascial contractures or tendonitis.
3. Progressive Joint Degeneration and Stiffness
Lack of adequate treatment can accelerate the degeneration of the lumbar facets and lead to progressive loss of mobility. Erosion of articular cartilage and the formation of osteophytes limit the normal movements of the spine, causing increasing stiffness and rigidity. In the long term, this loss of mobility can worsen pain and alter overall posture.
Joint degeneration can also lead to spinal instability, due to the loss of the supporting function of the facets. This instability increases the risk of spinal deformities, such as scoliosis or hyperlordosis, which increases the stress on adjacent structures.
Long-Term Prognosis and Quality of Life of Patients
The prognosis of patients with lumbar facet syndrome depends largely on the early diagnosis, the severity of the degeneration, and the therapeutic management implemented. Proactive and appropriate management can prevent long-term complications and improve the quality of life of patients.
1. Improved Joint Pain and Function
When properly managed, lumbar facet syndrome can be stabilized and pain can be effectively relieved. Osteopathic treatments, combined with muscle strengthening exercises and postural adjustments, can reduce stress on the facets and restore joint mobility. Reducing inflammation and muscle tension also helps improve patient comfort.
Patients who adhere to a comprehensive care program, including manual interventions, postural advice and specific exercises, can expect a significant improvement in their quality of life. Acute pain can be controlled and chronic pain reduced, allowing patients to resume their daily activities.
2. Recurrence Prevention and Long-Term Management
The long-term prognosis of lumbar facet syndrome also depends on the ability of patients to adopt strategies to prevent recurrence. Adequate postural education and regular muscle strengthening are essential to maintain spinal alignment and reduce the risk of excessive stress on the facets.
Patients should be encouraged to practice spinal stabilizing muscle strengthening exercises and to adopt ergonomic postures at work and at home. Body weight management and avoidance of sudden twisting movements are also key elements of prevention.
3. Impact on Quality of Life
Untreated lumbar facet syndrome can have a significant impact on patients’ quality of life. Chronic pain and functional limitations often lead to mental health implications, including anxiety and depression. Fear of pain can cause patients to avoid social and physical activities, contributing to isolation and decreased overall life satisfaction.
In contrast, proactive and tailored management can restore joint function, reduce pain and prevent complications. Patients can thus regain their functional independence and fully participate in their daily activities.
Case Studies and Testimonials: Effectiveness of Osteopathic Treatments for Lumbar Facet Syndrome
Case studies and patient testimonials provide concrete evidence of the effectiveness of osteopathic treatments in the management of lumbar facet syndrome. These stories help illustrate how osteopathy can improve patients’ quality of life by relieving pain, restoring mobility, and promoting better joint function. In this section, we will discuss some successful clinical cases and share testimonials from patients who have benefited from osteopathic care.
Presentation of Successful Clinical Cases
Case 1: Reduction of Chronic Pain in an Elderly Patient
Background: A 70-year-old patient had chronic low back pain for several years. The pain, located in the lower lumbar region, was exacerbated by extension movements and prolonged standing. Analgesics provided limited relief, and corticosteroid injections had only a temporary effect.
Clinical assessment: Evaluation revealed significant stiffness of the lumbar facets and muscle tension in the paravertebral muscles. Mobility testing showed restriction during trunk extension and rotation, which reinforced the hypothesis of lumbar facet syndrome.
Intervention: Osteopathic treatment focused on gentle joint mobilization techniques to improve facet mobility, combined with myofascial release of the paravertebral and psoas muscles. Gentle strengthening exercises were also incorporated.
Results: After six sessions, the patient experienced a significant reduction in his lower back pain and an improvement in his ability to stand and walk. Myofascial release techniques reduced muscle tension, improving the patient’s quality of life.
Case 2: Recovery of Mobility after Trauma
Background: A 45-year-old active tennis player injured herself while performing a sudden rotational movement. Since the accident, she had been experiencing severe lower back pain, aggravated by rotation and physical exertion. Prescribed anti-inflammatory medications provided only partial relief, and the pain limited her sports activities.
Clinical assessment: Clinical tests showed restricted mobility of the L3-L5 facets, as well as significant tension points in the erector spinae muscles. The patient also had mild lumbar hyperlordosis, which increased pressure on the posterior facets.
Intervention: Osteopathic treatment consisted of using gentle joint mobilization techniques to restore facet mobility, as well as myofascial release techniques for the erector spinae muscles. Specific stretching and corrective exercises were recommended.
Results: After four sessions, the patient regained much of her mobility and was able to resume playing tennis without pain. The preventive exercises helped improve her postural alignment and prevent recurrences.
Case 3: Management of Work-Related Pain in an Office Worker
Background: A 50-year-old man, who worked mainly in a sitting position, suffered from chronic low back pain. The pain intensified at the end of the day and continued even after his working hours. He had tried to modify his posture and use a lumbar cushion, but the pain persisted.
Clinical assessment: Assessment revealed L4-L5 facet restrictions and myofascial tension in the quadratus lumborum muscles. Extension testing reproduced the patient’s pain. Postural imbalances were also identified, due to long hours spent sitting.
Intervention: Osteopathic treatment focused on myofascial release of tight muscles and gentle lumbar facet joint mobilizations. Ergonomic advice was provided to adjust her posture at the office, and stretching exercises were recommended to improve her flexibility.
Results: After five sessions, the patient noted a significant reduction in his pain, better tolerance to sitting and an improvement in his general comfort at work.
Long-Term Prognosis and Quality of Life of Patients
The prognosis of patients with lumbar facet syndrome depends largely on the early diagnosis, the severity of the degeneration, and the therapeutic management implemented. Proactive and appropriate management can prevent long-term complications and improve the quality of life of patients.
1. Improved Joint Pain and Function
When properly managed, lumbar facet syndrome can be stabilized and pain can be effectively relieved. Osteopathic treatments, combined with muscle strengthening exercises and postural adjustments, can reduce stress on the facets and restore joint mobility. Reducing inflammation and muscle tension also helps improve patient comfort.
Patients who adhere to a comprehensive care program, including manual interventions, postural advice and specific exercises, can expect a significant improvement in their quality of life. Acute pain can be controlled and chronic pain reduced, allowing patients to resume their daily activities.
2. Recurrence Prevention and Long-Term Management
The long-term prognosis of lumbar facet syndrome also depends on the ability of patients to adopt strategies to prevent recurrence. Adequate postural education and regular muscle strengthening are essential to maintain spinal alignment and reduce the risk of excessive stress on the facets.
Patients should be encouraged to practice spinal stabilizing muscle strengthening exercises and to adopt ergonomic postures at work and at home. Body weight management and avoidance of sudden twisting movements are also key elements of prevention.
3. Impact on Quality of Life
Untreated lumbar facet syndrome can have a significant impact on patients’ quality of life. Chronic pain and functional limitations often lead to mental health implications, including anxiety and depression. Fear of pain can cause patients to avoid social and physical activities, contributing to isolation and decreased overall life satisfaction.
In contrast, proactive and tailored management can restore joint function, reduce pain and prevent complications. Patients can thus regain their functional independence and fully participate in their daily activities.
In the Shoes of a Patient: Living a Day with Lumbar Facet Syndrome
For people with lumbar facet syndrome, every day can be a challenge. This joint pain located in the lower back can be constant or recurring, disrupting simple daily activities and limiting mobility. Understanding what someone with this syndrome goes through can help you better understand the scope of this condition and the importance of its treatment.
Morning: A Difficult Wake-Up
The day often begins with a painful awakening. After a night of sleep, morning stiffness in the lower back is a constant for many patients. This phenomenon is due to prolonged immobility, which leads to increased inflammation around the facets. Getting out of bed can sometimes require considerable effort, with the need to move slowly and take breaks before standing up completely. The feeling of blocking or stiffness can last for several minutes, making simple actions such as getting out of bed or putting on clothes difficult.
Commuting to Work: A Seated Challenge
For those who work outside the home, commuting by car or public transit is an added challenge. Prolonged sitting can exacerbate pain. Compression of the lumbar facets when sitting, especially without adequate lumbar support, is often the cause of discomfort. Patients report that even short periods of time spent in a car or sitting on a hard seat can trigger sharp pain or a feeling of deep tension in the lower back. The need to stand up regularly or stretch becomes a necessity to prevent the pain from worsening.
At the office: Ergonomics at the heart of concerns
For people with sedentary jobs, the day at the office is punctuated by periods of increasing pain. Sitting in front of a computer for long hours, with an incorrect posture, can lead to intense pain. Patients often try to adopt compensatory positions to avoid the movements that trigger the pain, which in the long term leads to muscle tension and postural imbalances. The need to constantly adjust the chair, take regular breaks and get up to walk becomes crucial. Prolonged meetings or tasks that require remaining static are particularly difficult to endure.
End of the Day: Increased Fatigue and Pain
At the end of the day, fatigue sets in and with it, an increase in pain. The back muscles, often tight in response to facet pain, become even stiffer. Walking becomes painful, rotational movements of the torso are limited, and bending to pick up an object can be extremely difficult. For many patients, the end of the day means returning home feeling heavy and extremely tired, which can also affect mood and the quality of social and family interactions.
Daily activities and leisure activities: A constant adaptation
People with lumbar facet syndrome often have to give up certain activities or significantly modify them. For example, simple housework can be difficult to do. Bending down to clean, lifting heavy objects or even vacuuming becomes a challenge. Leisure activities, such as sports or walking, are also limited. Many patients have to reduce their level of physical activity, which has an impact on their general well-being and morale. The stress associated with the fear of triggering severe pain often limits outings and moments of relaxation.
Evening: The Need for Recovery
At the end of the day, finding comfort is a priority. People with lumbar facet syndrome often spend their evenings finding positions that relieve pain. Using support cushions, practicing light stretches, or applying warm compresses become end-of-day rituals. Sleep can be difficult to come by, due to the pain and anxiety associated with recurring painful episodes.
Living with lumbar facet syndrome involves constant adaptation and increased vigilance to avoid painful movements. Pain affects not only daily tasks, but also mood and quality of life. Understanding the daily lives of people suffering from this syndrome helps to realize the importance of adequate care to improve their comfort and autonomy.
10 Q&A on osteopathy benefit of chronic facet irritation
1. What is chronic facet irritation?
Chronic facet irritation is a condition involving persistent inflammation or degeneration of the facet joints in the spine. These joints are responsible for stabilizing the spine and facilitating movement. Chronic irritation can lead to long-term pain and stiffness.
2. What are the common causes of chronic facet irritation?
The main causes include repetitive strain, poor posture, spinal arthritis, disc degeneration, trauma, and aging. These factors can result in joint wear and tear, leading to inflammation and irritation.
3. How does chronic facet irritation manifest?
Symptoms include localized pain in the back, stiffness, reduced range of motion, and pain that worsens with certain movements like twisting or bending. Pain may radiate to surrounding areas, such as the buttocks or shoulders, depending on the location.
4. How is chronic facet irritation diagnosed?
Diagnosis involves a combination of patient history, physical examination, and imaging studies such as X-rays, CT scans, or MRIs. In some cases, diagnostic injections into the affected joint may help confirm the condition.
5. How can osteopathy help with chronic facet irritation?
Osteopathy offers a holistic approach by using manual techniques to relieve pain, improve joint mobility, and restore alignment. It also addresses muscle imbalances and promotes overall spinal health.
6. What osteopathic techniques are commonly used for chronic facet irritation?
Techniques include:
- Soft tissue massage to release muscle tension.
- Joint mobilization to restore motion and reduce stiffness.
- Myofascial release to improve connective tissue flexibility.
- High-velocity, low-amplitude (HVLA) adjustments for spinal alignment.
7. Is osteopathy effective for long-term management of chronic facet irritation?
Yes, osteopathy is effective for long-term management by addressing the root causes of the irritation, improving posture, and teaching patients exercises to maintain spinal health and prevent recurrence.
8. Are there any risks associated with osteopathic treatment?
Osteopathic treatment is generally safe when performed by a qualified professional. Minor risks include temporary soreness or discomfort. Techniques like HVLA adjustments should be used cautiously in patients with advanced spinal degeneration or osteoporosis.
9. How does osteopathy compare to other treatments for chronic facet irritation?
Unlike conventional treatments like medication or injections, osteopathy focuses on the underlying mechanical and structural issues. It offers a natural and non-invasive alternative or complement to traditional approaches.
10. Can lifestyle changes enhance the benefits of osteopathy for chronic facet irritation?
Absolutely. Regular exercise, core strengthening, maintaining a healthy weight, and proper ergonomics can significantly improve outcomes when combined with osteopathic care.
Conclusion
Lumbar facet syndrome is a common cause of lower back pain, often confused with other back pathologies, such as muscle pain or herniated discs. As a degenerative condition affecting the facet joints, this syndrome can significantly affect the quality of life of those affected, making it difficult to perform daily tasks and compromising general well-being. The importance of its management lies in the need for an early and multidisciplinary approach, integrating both lifestyle modifications and appropriate therapeutic interventions, such as those offered by osteopathy.
Osteopathy plays a key role in the management of lumbar facet syndrome, focusing on restoring joint mobility, reducing surrounding muscle tension and improving postural alignment. Osteopathic techniques, such as gentle mobilisation and myofascial release, allow dysfunctions to be treated in a targeted manner, while respecting the integrity of the affected structures. In addition, postural advice and strengthening exercises are crucial elements to prevent recurrence and maintain optimal lumbar balance.
Proactive management of lumbar facet syndrome, based on a comprehensive clinical assessment and preventive strategies, offers patients the opportunity to improve their comfort and independence in daily life. It is essential that people suffering from this syndrome understand the importance of regular and appropriate care, which involves a trusting relationship with qualified health professionals. In addition, adopting healthy habits, such as weight management, ergonomic adjustment at work, and regular physical activity, is an important part of preventing this condition and its progression.
In summary, although lumbar facet syndrome can be a significant challenge for those who suffer from it, therapeutic solutions exist to relieve symptoms and improve joint function. With appropriate follow-up, patients can regain a satisfactory quality of life and minimize the impacts of this condition. By keeping in mind the importance of an accurate diagnosis and comprehensive management, it is possible to limit long-term complications and promote better lumbar health.
References
- Bogduk N. Degenerative joint disease of the spine. Radiol Clin North Am. 2012 Jul;50(4):613-28. [ PubMed ]
- Grgić V. [Lumbosacral facet syndrome: functional and organic disorders of lumbosacral facet joints]. Lijec Vjesn. 2011 Sep-Oct;133(9-10):330-6. [ PubMed ]
- Marcia S, Masala S, Marini S, Piras E, Marras M, Mallarini G, Mathieu A, Cauli A. Osteoarthritis of the zygapophysial joints: efficacy of percutaneous radiofrequency neurotomy in the treatment of lumbarfacet joint syndrome. Clin Exp Rheumatol. 2012 Mar-Apr;30(2):314. [ PubMed ]
- Manchikanti L, Boswell MV, Singh V, Pampati V, Damron KS, Beyer CD. Prevalence of facet joint pain in chronic spinal pain of cervical, thoracic, and lumbar regions. BMC Musculoskelet Disord. 2004 May 28;5:15. [ PMC free article ] [ PubMed ]
- Kozera K, Ciszek B, Szaro P. Posterior Branches of Lumbar Spinal Nerves – part II: Lumbar Facet Syndrome – Pathomechanism, Symptomatology and Diagnostic Work-up. Ortop Traumatol Rehabil. 2017 Apr 12;19(2):101-109. [ PubMed ]
- Bogduk N. Functional anatomy of the spine. Handb Clin Neurol. 2016;136:675-88. [ PubMed ]
- Falco FJ, Manchikanti L, Datta S, Sehgal N, Geffert S, Onyewu O, Singh V, Bryce DA, Benyamin RM, Simopoulos TT, Vallejo R, Gupta S, Ward SP, Hirsch JA. An update of the systematic assessment of the diagnostic accuracy of lumbar facet joint nerve blocks. Pain Physician. 2012 Nov-Dec;15(6):E869-907. [ PubMed ]
- Boswell MV, Manchikanti L, Kaye AD, Bakshi S, Gharibo CG, Gupta S, Jha SS, Nampiaparampil DE, Simopoulos TT, Hirsch JA. A Best-Evidence Systematic Appraisal of the Diagnostic Accuracy and Utility of Facet (Zygapophysial) Joint Injections in Chronic Spinal Pain. Pain Physician. 2015 Jul-Aug;18(4):E497-533. [ PubMed ]
- Smuck M, Crisostomo RA, Trivedi K, Agrawal D. Success of initial and repeated medial branch neurotomy for zygapophysial joint pain: a systematic review. PM R. 2012 Sep;4(9):686-92. [ PubMed ]
- Bogduk N. On diagnostic blocks for lumbar zygapophysial joint pain. F1000 Med Rep. 2010 Aug 09;2:57. [ PMC free article ] [ PubMed ]
























{kind=link}