

Introduction
Lumbar stenosis is a degenerative spinal condition characterized by narrowing of the spinal canal in the lumbar region. This condition can have significant implications on a person’s quality of life, affecting their mobility and causing various symptoms.
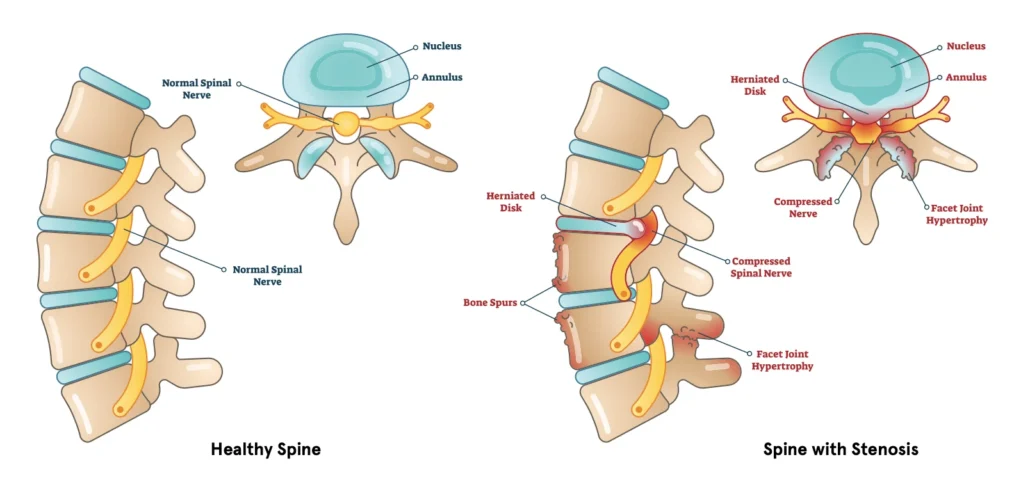
One of the main causes of lumbar stenosis is the natural aging process. Over the years, the intervertebral discs lose height due to compression and dehydration. This decrease in disc height can lead to increased pressure on surrounding structures. In response to this phenomenon, the vertebral body reacts by developing additional edges at the periphery of the vertebral endplates. This is done in an attempt to absorb shock and stabilize the spine, but sometimes this reaction can lead to narrowing of the spinal canal.
The ligamentum flavum, a ligament located at the back of the spine, also tends to undergo degenerative changes. It may thicken or become enlarged, contributing to narrowing of the spinal canal. Additionally, osteophytes, also known as bone spurs, may form. These bony growths can compress the spinal cord and nerve roots, causing symptoms such as pain, numbness, and weakness in the lower extremities.
In degenerative disease, the facet joints, also called apophyseal joints, may undergo changes. These joints, responsible for flexion and extension of the spine, can become flattened or deformed, contributing to the narrowing of the spinal canal.
Symptoms of lumbar stenosis can vary from person to person, but they often include lower back pain, cramps, numbness, muscle weakness, and difficulty walking. These symptoms may be exacerbated while walking or standing, and relieved by rest or leaning forward.
Treatment for lumbar stenosis depends on the severity of symptoms and may include non-surgical approaches such as physical therapy, pain-relieving medications, and corticosteroid injections. In more severe cases or when symptoms do not respond to conservative treatments, surgery may be considered to relieve compression of nerve structures.
Understanding What Causes Lumbar Stenosis.
Lumbar spinal stenosis, a condition characterized by the narrowing of the spinal canal in the lower back, can stem from various causes. One primary factor is the natural aging process, which often leads to degenerative changes in the spine. Over time, the discs between the vertebrae may lose water content and height, resulting in a collapse of the disc spaces and the development of bone spurs, known as osteophytes. These changes contribute to the narrowing of the spinal canal, exerting pressure on the spinal cord and nerves. Another common cause is osteoarthritis, which leads to the breakdown of the cartilage that cushions the joints in the spine. As the cartilage wears away, the bones may rub against each other, causing inflammation and further narrowing of the spinal canal. Additionally, thickening of the ligaments in the spine, a condition known as ligamentum flavum hypertrophy, can contribute to lumbar spinal stenosis by encroaching upon the spinal canal space. Other factors that may contribute to the development or worsening of lumbar stenosis include spinal injuries, genetic predispositions, and congenital abnormalities of the spine. Understanding the underlying causes of lumbar stenosis is crucial for accurate diagnosis and effective management of this condition. By addressing the root causes and associated risk factors, healthcare providers can tailor treatment plans to alleviate symptoms and improve patients’ quality of life.
The aging process is the main cause of degenerative changes seen in the spine, eventually leading to spinal stenosis. Here are some factors associated with this development:
- Loss of Disc Height: With age, intervertebral discs lose height due to dehydration and reduced protein mass. This contributes to compression of the vertebral body.
- Rim Formation: In response to decreased disc height, the vertebral body may form an additional lip or rim to cushion shock and maintain stability.
- Compression of the Vertebral Canal: The extension of the lip formed by the vertebral body can, in some cases, partially obstruct the opening of the vertebral canal, leading to compression of the nerve structures.
- Ligamentum Flavum Hypertrophy: The ligamentum flavum, which helps stabilize the spine, tends to hypertrophy or thicken with age, contributing to stenosis.
- Formation of Osteophytes: Bone spurs, or osteophytes, also form in response to aging. These growths can reduce the space available in the spinal canal.
- Facet Deformation: Apophyseal joints, also called facets, can undergo degenerative changes, becoming flattened or distorted over time.
These degenerative changes in the spine, often related to age, can contribute to spinal stenosis, leading to symptoms such as nerve compression, pain, and loss of function.
History of Lumbar Stenosis
The history of spinal stenosis dates back centuries, but its identification and understanding have evolved significantly over time. Here is a brief historical overview of spinal stenosis:
- Antiquity: The first descriptions of symptoms that could be linked to spinal stenosis date back to ancient times. However, in the absence of advanced anatomical knowledge, observations were often limited to descriptions of back pain and difficulty moving.
- Renaissance and Development of Anatomy: During the Renaissance, significant advances were made in the field of anatomy. Scientists like Andreas Vesalius have contributed to a better understanding of the structure of the human body, including the spine and spinal canal.
- Beginning of Modern Medicine: Over the centuries, modern medicine emerged, and with it, a better ability to diagnose spinal conditions. However, spinal stenosis as a distinct entity was not fully recognized until later.
- Identifying Spinal Stenosis: The term “spinal stenosis” became common in the 20th century. With the advent of radiography and other medical imaging techniques, doctors were able to more precisely identify and characterize structural changes in the spinal canal.
- Research and Treatments: Advances in medical research have led to a deeper understanding of the mechanisms underlying spinal stenosis, including its links to aging, osteoarthritis, and other degenerative conditions. Multiple treatment options, ranging from conservative management to surgery, have been developed.
- Evolution of Surgical Techniques: Surgical techniques to treat spinal stenosis have evolved considerably. Procedures such as laminectomy and spinal fusion were developed to relieve nerve compression.
- Interventional Approaches: In addition to surgical treatments, interventional approaches, such as epidural injections and minimally invasive decompression, have been developed to relieve the symptoms of spinal stenosis.
Today, spinal stenosis is a well-recognized medical condition, diagnosed using advanced medical imaging and treated through various modalities depending on the severity of symptoms and the specific condition of the patient.
Recognizing Symptoms Early
Early recognition of lumbar stenosis symptoms is critical for effective management and prevention of complications. Understanding the signs of pain, numbness, and weakness, as well as the differences between neurogenic and vascular claudication, can help individuals seek appropriate care promptly. Below, we explore the key indicators, how to differentiate claudication types, and when it is time to consult a healthcare provider.
Signs of Pain, Numbness, and Weakness
Lumbar stenosis often manifests through pain, numbness, and weakness, primarily affecting the lower back and lower extremities. These symptoms arise due to the narrowing of the spinal canal and subsequent compression of nerve roots.
- Pain
- Location: Lower back pain is the most common initial symptom, which may radiate to the buttocks, thighs, or calves.
- Nature: The pain can vary from dull and aching to sharp and severe, often worsening with prolonged standing or walking.
- Relief: Leaning forward or sitting often alleviates the pain by increasing space in the spinal canal and reducing nerve compression.
- Numbness and Tingling
- Affected Areas: Sensations of numbness or tingling are often felt in the buttocks, legs, or feet.
- Pattern: These sensations may follow a specific nerve root distribution, known as dermatomes, and often occur bilaterally.
- Impact: Numbness can impair balance and coordination, increasing the risk of falls.
- Weakness
- Muscle Involvement: Weakness, especially in the legs, is a hallmark sign of nerve compression. It may present as difficulty lifting the feet (foot drop) or maintaining balance.
- Functional Limitations: Tasks like climbing stairs, walking long distances, or standing for extended periods become challenging.
Recognizing these symptoms early and monitoring their progression is essential for timely diagnosis and intervention.
How to Identify Neurogenic Claudication
Neurogenic claudication is a hallmark symptom of lumbar stenosis, characterized by pain, numbness, and weakness in the legs during walking or standing. It is crucial to distinguish neurogenic claudication from vascular claudication, as they have different causes and management strategies.
- Neurogenic Claudication
- Cause: Compression or irritation of spinal nerve roots due to narrowing of the spinal canal or foramina.
- Symptoms:
- Pain, numbness, or weakness in the buttocks, thighs, or calves.
- Symptoms worsen with standing or walking and improve with sitting or bending forward.
- Patients may adopt a forward-leaning posture or use support to reduce symptoms.
- Pain Distribution: Often bilateral, with a “heaviness” or “burning” sensation.
- Provocation and Relief: Activities requiring lumbar extension (e.g., walking downhill) worsen symptoms, while flexion (e.g., sitting or leaning forward) provides relief.
- Vascular Claudication
- Cause: Insufficient blood flow to the leg muscles, typically due to peripheral artery disease (PAD).
- Symptoms:
- Cramping pain, typically in the calves, that worsens with exercise and improves with rest.
- Pain is often unilateral and may be associated with skin changes or hair loss on the legs.
- Pain Distribution: Localized to the muscles, especially the calves, and does not typically involve numbness or tingling.
- Provocation and Relief: Symptoms worsen with walking or climbing uphill and improve rapidly with rest, regardless of posture.
Diagnostic Tools:
- Neurogenic Claudication: Diagnosis often involves imaging (e.g., MRI or CT) to assess spinal narrowing.
- Vascular Claudication: Diagnosis includes vascular tests like ankle-brachial index (ABI) measurements or Doppler ultrasound.
When to Seek Medical Help
While mild symptoms of lumbar stenosis may be managed conservatively, certain signs and circumstances warrant prompt medical attention:
- Persistent Symptoms
- Chronic pain, numbness, or weakness lasting several weeks despite rest or conservative treatments.
- Difficulty performing daily tasks due to pain or functional limitations.
- Progressive Symptoms
- Increasing severity or frequency of symptoms over time.
- Worsening leg weakness or balance issues, raising concerns about nerve damage.
- Severe Pain or Neurological Deficits
- Unbearable pain that disrupts sleep or daily activities.
- Sudden onset of significant leg weakness, numbness, or tingling.
- Signs of Cauda Equina Syndrome
- A rare but serious condition requiring immediate attention. Symptoms include:
- Loss of bladder or bowel control.
- Severe pain in the lower back and legs.
- Numbness in the groin or “saddle” region.
- A rare but serious condition requiring immediate attention. Symptoms include:
- Inability to Walk or Stand
- Individuals who experience severe neurogenic claudication that prevents walking or standing for even short durations should consult a healthcare provider.
- General Health Concerns
- Patients with pre-existing conditions like diabetes, arthritis, or peripheral artery disease should be vigilant about symptoms, as these conditions may exacerbate or mimic lumbar stenosis.


Pathophysiology of lumbar stenosis
The pathophysiology of lumbar stenosis involves several contributing factors, including degenerative changes in the spine, structural abnormalities, and inflammatory processes.
Degenerative changes in the spine play a significant role in the pathogenesis of lumbar stenosis. As people age, the intervertebral discs lose water content and elasticity, leading to decreased disc height and increased susceptibility to bulging or herniation. Additionally, osteoarthritis of the facet joints can occur, causing hypertrophy of the facet joints and thickening of the ligamentum flavum. These degenerative changes contribute to the narrowing of the spinal canal and compression of the neural elements within it.
Structural abnormalities also contribute to the development of lumbar stenosis. Conditions such as spondylolisthesis, where one vertebra slips forward over the one below it, can reduce the space available for the nerves and exacerbate compression. Similarly, congenital anomalies like a narrow spinal canal or abnormal curvature of the spine (scoliosis) can predispose individuals to stenosis.
Inflammatory processes within the spine can exacerbate the narrowing of the spinal canal and contribute to symptom progression in lumbar stenosis. Inflammation may result from the body’s response to degenerative changes, injury, or autoimmune conditions. Inflammatory cytokines released in response to tissue damage can lead to further tissue degeneration and fibrosis, contributing to the narrowing of the spinal canal and compression of neural structures.
The symptoms of lumbar stenosis typically manifest when the narrowed spinal canal compresses the nerves that innervate the lower back and lower extremities. Patients may experience radicular pain, which radiates from the lower back into the buttocks and legs, often exacerbated by standing or walking and relieved by sitting or bending forward. Numbness, tingling, and weakness may also occur in the affected areas, leading to difficulty with walking and balance.
The pathophysiology of lumbar stenosis underscores the complex interplay of degenerative changes, structural abnormalities, and inflammatory processes within the spine. Understanding these mechanisms is crucial for developing effective treatment strategies aimed at relieving symptoms, improving function, and enhancing the quality of life for patients with this debilitating condition.
- Development of osteoarthritis: Lumbar stenosis is often associated with osteoarthritis, a degenerative process of the joints. As we age, the joints in the spine, called facet joints, can experience degeneration, leading to increased friction and wear.
- Osteophyte Formation: In response to osteoarthritis, osteophytes, or bony growths, can form along the edges of the vertebrae and facet joints. These osteophytes contribute to the narrowing of the spinal canal by taking up space inside the spine.
- Ligament hypertrophy: To compensate for increased stress on the spine, the ligaments surrounding the spinal canal may become hypertrophied. This also contributes to the compression of the space available for the spinal cord and nerve roots.
- Herniated disc: An intervertebral disc can herniate, where its gelatinous core protrudes through the outer fiber of the disc. This can cause additional pressure on the nerve structures inside the spinal canal.
- Reduction in spinal canal space: The accumulation of degenerative changes, such as osteophytes, ligament hypertrophy, and herniated discs, results in a significant reduction in the space available in the spinal canal.
- Compression of nerve structures: Compression of the spinal cord and nerve roots from these degenerative changes can lead to symptoms such as pain, numbness, weakness, and difficulty walking.
- Clinical Symptoms: Symptoms of lumbar stenosis can vary depending on the severity of the nerve compression. Patients may experience lower back pain, pain radiating to the buttocks and legs (neurogenic claudication), and in severe cases, muscle weakness.
It is important to note that lumbar stenosis can be caused by other factors such as birth defects, trauma or tumors.
The Science Behind Lumbar Stenosis
Lumbar spinal stenosis is a condition characterized by the narrowing of the spinal canal in the lower back, which can compress the spinal cord and nerves. This condition often develops as part of the natural aging process and involves a combination of structural degeneration and inflammatory mechanisms. Understanding the science behind lumbar stenosis sheds light on how these processes interact, leading to pain, mobility challenges, and functional limitations. This article delves into how degeneration affects the spine and the structural and inflammatory contributors to this condition.
How Degeneration Affects the Spine
Degeneration is a primary driver of lumbar stenosis, involving progressive changes to the structures of the spine over time. These changes primarily affect the intervertebral discs, vertebrae, facet joints, and ligaments, which together form the structural and functional units of the spinal column.
- Intervertebral Disc Degeneration
- The intervertebral discs act as shock absorbers between the vertebrae, providing flexibility and cushioning. With age, these discs lose hydration and elasticity due to a decline in proteoglycan content. This process, known as disc desiccation, reduces the disc’s ability to absorb shock, leading to:
- Disc Height Loss: The thinning of the discs reduces the space between adjacent vertebrae, increasing mechanical stress on the facet joints and ligaments.
- Bulging or Herniation: Degenerated discs may bulge outward or rupture, protruding into the spinal canal and contributing to stenosis.
- Impact: These changes can directly compress nerve roots or the spinal cord, causing symptoms like radiating pain, numbness, or weakness.
- The intervertebral discs act as shock absorbers between the vertebrae, providing flexibility and cushioning. With age, these discs lose hydration and elasticity due to a decline in proteoglycan content. This process, known as disc desiccation, reduces the disc’s ability to absorb shock, leading to:
- Facet Joint Degeneration
- Facet joints, which connect the vertebrae, allow for controlled spinal motion. Over time, these joints experience wear and tear, resulting in cartilage breakdown and osteoarthritis. This degeneration leads to:
- Joint Hypertrophy: The enlargement of the joints due to bony overgrowth, which can encroach on the spinal canal.
- Formation of Osteophytes: Bone spurs develop as a compensatory mechanism, further narrowing the space available for nerves.
- Impact: Facet joint changes exacerbate nerve compression and contribute to mechanical back pain.
- Facet joints, which connect the vertebrae, allow for controlled spinal motion. Over time, these joints experience wear and tear, resulting in cartilage breakdown and osteoarthritis. This degeneration leads to:
- Ligamentous Changes
- The ligaments surrounding the spinal canal, particularly the ligamentum flavum, play a role in stabilizing the spine. With age, these ligaments can thicken or hypertrophy due to chronic stress and degenerative changes. This thickening further narrows the spinal canal.
- Impact: The combination of ligament hypertrophy and other degenerative changes reduces spinal flexibility and increases the likelihood of nerve compression.
- Spinal Instability
- Loss of disc height and facet joint degeneration can lead to vertebral instability. This instability may cause one vertebra to slip forward over another, a condition known as spondylolisthesis. Such misalignment further reduces the available space in the spinal canal and contributes to stenosis.
Structural and Inflammatory Contributors
Beyond mechanical degeneration, structural abnormalities and inflammatory processes play a crucial role in the progression of lumbar stenosis. These factors interact to exacerbate narrowing of the spinal canal and amplify symptoms.
- Structural Contributors
- Congenital Narrowing of the Spinal Canal: Some individuals are born with a naturally narrower spinal canal, which predisposes them to earlier and more severe stenosis when combined with age-related degeneration.
- Spondylolisthesis: As previously mentioned, vertebral slippage exacerbates the narrowing of the spinal canal, further impinging on nerve structures.
- Scoliosis: Abnormal curvature of the spine can alter the alignment of the vertebrae and lead to uneven pressure distribution, accelerating degeneration and contributing to stenosis.
- Osteophytes: These bony outgrowths, while initially stabilizing mechanisms, reduce the available space for nerves and can cause significant nerve root compression.
- Inflammatory Processes
- Inflammation plays a key role in the pathophysiology of lumbar stenosis, often as a response to degenerative changes or mechanical stress.
- Cytokine Release:
- Pro-inflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α), are released in response to disc degeneration and joint damage. These cytokines promote tissue breakdown, pain sensitization, and further degeneration.
- Neuroinflammation:
- Nerve root compression triggers localized inflammation, contributing to radicular pain, numbness, and muscle weakness. Chronic inflammation can also lead to fibrosis, further narrowing the spinal canal.
- Autoimmune Components:
- In some cases, systemic inflammatory conditions, such as ankylosing spondylitis or rheumatoid arthritis, can contribute to spinal stenosis by causing inflammatory changes in the spine’s ligaments and joints.
- Microvascular Changes
- The narrowing of the spinal canal reduces blood flow to the affected nerves, causing ischemia and further exacerbating symptoms. Hypoxia within the compressed neural tissues leads to cellular damage and can amplify pain and functional limitations.
- Biomechanical Stress and Adaptations
- Chronic stress on the lumbar spine from poor posture, repetitive heavy lifting, or prolonged sitting can accelerate degenerative changes. As the spine adapts to these stressors, compensatory mechanisms, such as muscle tightness or altered gait, may develop, further contributing to pain and functional decline.
Clinical Implications
The interplay between structural and inflammatory factors in lumbar stenosis underscores the complexity of this condition. Understanding these mechanisms highlights the importance of a multidisciplinary approach to management, which may include:
- Non-surgical Interventions: Physical therapy, osteopathic care, and medications targeting inflammation and pain.
- Surgical Options: For severe cases, decompression surgeries, such as laminectomy or spinal fusion, can address structural issues and relieve nerve compression.
- Preventative Measures: Weight management, ergonomic adjustments, and strengthening exercises can slow progression and reduce symptoms.
Understanding Lumbar Stenosis: Contraindications and Osteopathic Approaches
Diagnosis: Getting the Right Answers
Accurate diagnosis is essential for effectively managing lumbar spinal stenosis in osteopathic practice. It involves a combination of clinical evaluations, imaging tests, and specific orthopedic assessments to confirm the condition and guide tailored osteopathic treatment.
Clinical Evaluations and Imaging Tests
The diagnostic process for lumbar stenosis begins with a detailed medical history and physical examination. These steps help osteopaths identify symptoms such as back pain, leg numbness, weakness, or difficulty walking, which are hallmarks of lumbar stenosis.
- Medical History:
- A thorough discussion of the patient’s symptoms, including their duration, triggers, and relieving factors.
- Assessment of previous injuries, surgeries, or underlying conditions that could contribute to spinal narrowing.
- Physical Examination:
- Evaluation of reflexes, muscle strength, and sensation in the lower extremities.
- Observation of gait and posture to identify functional impairments that can be addressed through osteopathic techniques.
- Imaging Tests:
- X-rays: Provide a basic overview of the spinal structure, revealing bone spurs, fractures, or alignment issues.
- MRI (Magnetic Resonance Imaging): Offers detailed images of soft tissues, including nerves and intervertebral discs, to identify compression or stenosis severity.
- CT Scan (Computed Tomography): Useful for evaluating bone-related changes, especially when combined with contrast (CT myelogram).
- Electromyography (EMG): Assesses nerve function and helps confirm whether symptoms are due to nerve root compression.
Orthopedic Tests for Osteopathic Diagnosis
Specific orthopedic tests provide valuable insights for an osteopath when planning treatment strategies. These tests help evaluate the functionality and structural involvement of the lumbar spine.

- Stoop Forward Bend Test:
- How to Perform: The patient is asked to walk until their symptoms, such as leg pain or weakness, appear. Once symptoms are present, the patient stops and bends forward at the hips.
- Result: Relief of symptoms during the forward bend indicates lumbar spinal stenosis. This occurs because bending forward increases the space in the spinal canal, reducing nerve compression.
- Single-Leg Lumbar Extension Test:
- How to Perform: The patient stands on one leg and extends the lumbar spine (leans backward). This test is performed on both sides.
- Result: Reproduction of lower back or leg symptoms is a positive result, often indicating facet joint pathology or stenosis.
- Kemp’s Test:
- How to Perform: The patient leans backward while rotating and bending toward the affected side, either seated or standing.
- Result: Pain radiating down the leg suggests nerve root compression, which may guide specific osteopathic approaches.
- Straight Leg Raise (SLR) Test:
- How to Perform: The patient lies supine while the osteopath lifts one leg, keeping the knee straight.
- Result: Pain or tingling radiating down the leg suggests nerve root irritation. This test helps differentiate stenosis from herniated discs.
- Two-Stage Treadmill Test:
- How to Perform: The patient walks on a treadmill at a slight incline and then on a flat surface.
- Result: Symptoms worsening on a flat surface but improving on an incline suggest lumbar stenosis, as the incline promotes a flexed posture and increases spinal canal space.
Differentiating Similar Conditions in Osteopathy
Lumbar stenosis symptoms can overlap with other conditions, requiring an osteopath to carefully differentiate them to ensure appropriate treatment. Conditions to rule out include:
- Herniated Disc:
- Similar radiating leg pain, often with acute onset and specific nerve root impingement.
- MRI helps distinguish disc herniation from stenosis.
- Peripheral Neuropathy:
- Involves widespread nerve damage, often linked to diabetes, presenting as burning or tingling sensations in the legs.
- Nerve conduction studies can confirm this diagnosis.
- Vascular Claudication:
- Mimics stenosis with leg pain during walking, but stems from poor blood flow rather than nerve compression.
- Doppler ultrasound or angiography differentiates this condition.
- Spondylolisthesis:
- Involves slippage of a vertebra, potentially narrowing the spinal canal.
- X-rays and advanced imaging reveal vertebral alignment issues.
- Hip or Knee Disorders:
- Joint issues causing referred pain to the lower back or legs.
- Physical examination and joint-specific imaging help exclude these causes.
By combining clinical evaluation, imaging, and targeted orthopedic tests, osteopaths can develop a comprehensive understanding of lumbar spinal stenosis and implement effective, patient-specific treatment strategies.
The Science Behind Lumbar Stenosis
Lumbar stenosis is a complex condition resulting from structural and inflammatory changes in the spine. Understanding the mechanisms behind these changes helps osteopaths tailor effective treatment strategies for their patients.
How Degeneration Affects the Spine
Degeneration is the most common cause of lumbar stenosis, typically progressing with age and wear-and-tear on spinal structures.
- Disc Degeneration:
- The intervertebral discs lose water content and elasticity over time, becoming less effective in cushioning spinal loads.
- Collapsed discs can reduce the space within the spinal canal and foramina, compressing nerves and causing symptoms like pain, numbness, or weakness.
- Facet Joint Hypertrophy:
- Degenerative changes in facet joints lead to the formation of osteophytes (bone spurs).
- These bony growths encroach on the spinal canal and contribute to nerve compression.
- Ligamentum Flavum Thickening:
- The ligamentum flavum, which stabilizes the spine, can thicken and lose flexibility due to repetitive stress or inflammation.
- This thickening reduces the diameter of the spinal canal, exacerbating stenosis.
- Vertebral Alignment Issues:
- Conditions like spondylolisthesis, where one vertebra slips forward over another, can further narrow the spinal canal.
- Alignment problems often worsen with age and degeneration, compounding stenosis symptoms.
Structural and Inflammatory Contributors
In addition to degeneration, structural abnormalities and inflammatory processes play significant roles in the development and progression of lumbar stenosis.
- Congenital Factors:
- Some individuals are born with a narrower spinal canal (congenital stenosis).
- Although asymptomatic early in life, aging and degeneration can exacerbate this condition, leading to clinical symptoms.
- Inflammatory Processes:
- Chronic inflammation from conditions like osteoarthritis triggers changes in joint structures and soft tissues.
- Inflammation promotes the formation of osteophytes and thickening of the ligamentum flavum, compounding spinal canal narrowing.
- Soft Tissue Contributions:
- Muscular imbalances and tightness in surrounding areas, such as the hip flexors or paraspinal muscles, can place additional strain on the lumbar spine.
- These imbalances may exacerbate postural dysfunction, further compressing neural structures.
- Epidural Fat Hypertrophy:
- Excess fat in the epidural space can encroach on the spinal canal.
- This condition is more common in individuals with obesity or long-standing spinal conditions.
- Vascular Factors:
- Compromised blood flow to neural tissues may contribute to symptom severity in lumbar stenosis.
- Poor circulation can result in ischemia, leading to increased pain and functional deficits.
Osteopathic Insights on Lumbar Stenosis
Osteopaths recognize that lumbar stenosis is not just a structural problem but a multifaceted condition influenced by biomechanical and systemic factors. Addressing these contributors holistically can alleviate symptoms and improve function:
- Postural Corrections:
- Identifying and correcting postural issues reduces stress on spinal structures, easing nerve compression.
- Soft Tissue Techniques:
- Targeting tight muscles and fascia in the lumbar region restores balance and relieves strain on the spine.
- Joint Mobilization:
- Gentle mobilization of adjacent spinal segments can improve range of motion and reduce compensatory stress.
- Inflammation Management:
- Osteopaths may recommend anti-inflammatory strategies, including dietary changes, hydration, and gentle exercises, to support systemic health.
- Patient Education:
- Educating patients about the progression of lumbar stenosis and preventive strategies empowers them to take an active role in their care.
Osteopathic Solutions for Lumbar Spinal Stenosis
Lumbar spinal stenosis, a condition characterized by the narrowing of the spinal canal in the lower back, can lead to significant pain and mobility challenges. Osteopathic care offers non-invasive, personalized approaches to alleviate symptoms, improve mobility, and enhance overall quality of life. By addressing the root causes and compensatory mechanisms, osteopathic solutions focus on restoring balance, reducing discomfort, and promoting long-term well-being. Key interventions include manual techniques, postural corrections, and patient education combined with lifestyle modifications.
Manual Techniques: Myofascial Release and Mobilization
Manual techniques lie at the heart of osteopathic treatment, targeting the physical structures impacted by lumbar stenosis. Myofascial release and mobilization are two core methods employed to address fascial restrictions, reduce muscle tension, and enhance spinal mobility.
- Myofascial Release
- Purpose: This technique aims to release tension in the fascia, the connective tissue that surrounds muscles and other structures. In lumbar stenosis, the fascia often becomes tight or restricted due to compensatory postural changes and chronic pain.
- Method: The osteopath applies gentle, sustained pressure to areas of restriction, promoting blood flow and softening adhesions. For example, tension in the thoracolumbar fascia or iliopsoas muscle, commonly tight in patients with lumbar stenosis, is addressed to restore flexibility and relieve discomfort.
- Benefits: Patients frequently report reduced pain, improved range of motion, and a sensation of lightness in the affected regions after myofascial release.
- Joint Mobilization
- Purpose: Joint mobilization techniques restore the mobility of the spine and surrounding joints that have become stiff due to degenerative changes. These techniques focus on the facet joints, which are often hypertrophic or misaligned in lumbar stenosis.
- Method: The osteopath performs gentle oscillatory movements or traction to specific spinal segments. This relieves pressure on nerve roots, improves spinal alignment, and facilitates movement without pain.
- Benefits: Regular sessions improve flexibility and reduce symptoms such as radiating leg pain and neurogenic claudication.
By addressing both soft tissue and joint dysfunctions, manual techniques enhance the body’s ability to function effectively and manage the stressors associated with lumbar stenosis.
Postural Corrections and Muscle Strengthening
Postural imbalances often exacerbate the symptoms of lumbar spinal stenosis. Poor posture, such as excessive lumbar lordosis or anterior pelvic tilt, increases pressure on the lumbar spine, worsening pain and limiting mobility. Osteopathy incorporates targeted corrections and strengthening exercises to mitigate these effects.
- Postural Assessments
- The osteopath begins with a comprehensive evaluation of the patient’s posture, identifying areas of misalignment or compensatory patterns. For example, a forward-leaning posture may provide temporary relief for lumbar stenosis but leads to additional strain on other body parts.
- Corrective Techniques
- Through guided exercises and manual adjustments, the osteopath helps patients achieve a more neutral spine alignment. These corrections reduce unnecessary mechanical stress on the lumbar region and improve the distribution of forces across the body.
- Muscle Strengthening
- Target Areas: Core stabilizers, including the transverse abdominis, multifidus, and pelvic floor muscles, are a primary focus. Strengthening these muscles supports the spine, reduces pressure on intervertebral discs, and prevents further degeneration.
- Exercise Examples: Planks, pelvic tilts, and gentle bridging exercises help improve core strength. Additionally, gluteal and hamstring muscles are strengthened to enhance overall stability.
- Stretching: Tight muscles, such as the hip flexors and hamstrings, are stretched to restore balance and flexibility.
- Benefits of Postural and Strength Training
- Improved posture decreases nerve compression, while stronger muscles enhance the spine’s stability. This combination helps patients regain confidence in their movement and reduces reliance on pain medications or assistive devices.
Exploring the Benefits of Osteopathy for Lumbar Spinal Stenosis: Evidence-Based Insights
1. Pain Perception and Thermographic Analysis in Chronic Lower Back Pain Patients (2019)
Summary: This study evaluates the effectiveness of osteopathic treatments in reducing pain and improving thermographic markers in patients with chronic lower back pain.
Access Study (PDF)
2. Work Recovery in Response to Osteopathic Treatment After Hemilaminectomy (1995)
Summary: Focuses on the impact of osteopathy in promoting recovery after hemilaminectomy, a surgery often related to lumbar stenosis treatment, showing positive rehabilitation outcomes.
Access Study (PDF)
3. Physiotherapy vs. Alternative Medicine for Lumbar Spinal Stenosis (2024)
Summary: This systematic review compares physiotherapy and alternative treatments, including osteopathy, in improving pain and quality of life in patients with lumbar spinal stenosis.
Access Study (PDF)
4. Immediate Alteration of Lumbar Intervertebral Foramen with Osteopathic Techniques (2021)
Summary: Demonstrates the immediate effects of osteopathic manipulative locking techniques on lumbar intervertebral structures in healthy participants, with implications for lumbar stenosis treatment.
Access Study (PDF)
5. Osteopathic Manipulative Treatment for Chronic Low Back Pain (2003)
Summary: Highlights the benefits of osteopathic manipulative treatment (OMT) in managing chronic low back pain, which often overlaps with lumbar spinal stenosis symptoms.
Access Study
6. Prevalence and Recovery in Low Back Pain and Leg Pain in Osteopathic Practice (2007)
Summary: Analyzes recovery rates in patients receiving osteopathic care for conditions such as low back and leg pain, which are common in lumbar spinal stenosis.
Access Study (PDF)
7. Selected Osteopathic Techniques in Low Back Pain Treatment (2010)
Summary: Explores the application of specific osteopathic methods for managing low back pain, providing insights relevant to stenosis-associated pain management.
Access Study (PDF)
8. Effectiveness of Manual Therapy Techniques for Lumbar Radiculopathy (2020)
Summary: Examines the role of osteopathic techniques in addressing lumbar radiculopathy, a symptom often associated with lumbar spinal stenosis.
Access Study (PDF)
9. An Osteopathic Approach to Degenerative and Herniated Discs (2021)
Summary: Discusses osteopathy’s role in managing degenerative lumbar conditions, including herniated discs and spinal stenosis, improving mobility and reducing pain.
Access Study
10. Successful Osteopathic Treatment for Foot Drop due to Lumbar Stenosis (2022)
Summary: A case study showing the effectiveness of osteopathic manipulative treatment in resolving symptoms of foot drop caused by lumbar spinal stenosis.
Access Study
Is Lumbar Stenosis a Complete or Partial Contraindication to Spinal Manipulation?
Lumbar stenosis is generally a partial contraindication to spinal manipulation, depending on the severity and symptoms. Here’s why:
Why Partial?
- Nature of Lumbar Stenosis:
- The narrowing of the spinal canal or foramina can compress nerve roots or the spinal cord, causing leg pain, numbness, or weakness.
- High-velocity, low-amplitude (HVLA) techniques may worsen symptoms if not carefully applied.
- Individual Assessment:
- The appropriateness of manipulation depends on the degree of stenosis and neurological symptoms.
- Mild cases may benefit from gentle techniques.
- Modified Techniques:
- Low-force or indirect methods like mobilization and muscle energy techniques can improve mobility without stressing the affected area.
When to Avoid Spinal Manipulation
Spinal manipulation should be avoided in cases of:
- Severe neurological symptoms (e.g., motor weakness, bowel/bladder dysfunction).
- High-grade stenosis with critical narrowing.
- Acute or worsening symptoms.
Best Practices for Osteopathic Care
- Conduct a thorough history, examination, and imaging to guide treatment.
- Collaborate with other healthcare professionals when needed.
- Focus on symptom reduction and functional improvement.
Alternative Osteopathic Approaches
Before considering spinal manipulation, prioritize these techniques:
- Soft Tissue Techniques: Reduce muscle tension and improve circulation.
- Myofascial Release: Relieve fascial restrictions.
- Gentle Mobilizations: Improve mobility in non-affected areas.
- Lifestyle Advice: Encourage posture improvement, ergonomics, and core-strengthening exercises.
These approaches often provide relief while minimizing risks.
Important Warning:This section is for educational purposes only and not a substitute for professional medical advice. Lumbar spinal stenosis should never be taken lightly—untreated, it may lead to permanent nerve damage or loss of function.Manual therapy, including spinal manipulation, must only be performed by qualified, licensed professionals adhering to local regulations. Improper techniques can cause injury or complications. Always consult a healthcare provider before attempting any treatment.
Usual Disclaimer:This blog is for educational purposes only and not a substitute for professional advice. Do not attempt maneuvers, exercises, or treatments described here without consulting a qualified healthcare provider. Improper application may cause injury or complications. Seek professional guidance for your health needs.
By adopting a cautious and tailored approach, osteopaths can effectively manage lumbar stenosis while minimizing risks.
Treatment Options for Every Stage of Lumbar Stenosis
Lumbar spinal stenosis is a progressive condition that requires tailored treatment based on its severity and impact on the patient’s quality of life. From conservative therapies to surgical interventions, a range of options is available to manage symptoms and restore function. This article explores non-surgical solutions for relief and when surgery becomes necessary to address more advanced cases.
Non-Surgical Solutions for Relief
For individuals in the early stages of lumbar stenosis or those with mild to moderate symptoms, non-surgical approaches often provide significant relief. These treatments focus on reducing pain, improving mobility, and preventing the condition from worsening.
- Physical Therapy
- Goals: Strengthen the core, improve posture, and increase spinal flexibility.
- Approach: Physical therapists design individualized exercise programs that include stretching, strengthening, and aerobic exercises. Stretching tight muscles, such as the hamstrings and hip flexors, reduces strain on the lower back, while strengthening core muscles provides better spinal support.
- Benefits: Regular physical therapy improves mobility, reduces pain, and may delay the need for surgical intervention.
- Medications
- Pain Relievers: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen help reduce inflammation and alleviate mild to moderate pain.
- Muscle Relaxants: These are prescribed to relieve muscle spasms associated with lumbar stenosis.
- Corticosteroids: Administered orally or through injections, corticosteroids reduce localized inflammation and relieve nerve compression symptoms.
- Caution: Medications are typically short-term solutions and should be used under medical supervision to avoid side effects.
- Osteopathic Manipulation
- Techniques: Osteopathic physicians use myofascial release, spinal mobilization, and gentle manipulations to improve spinal alignment and reduce tension in surrounding tissues.
- Benefits: These hands-on therapies alleviate pain, enhance flexibility, and restore spinal balance without invasive procedures.
- Epidural Steroid Injections
- Purpose: For individuals with more persistent symptoms, epidural steroid injections deliver anti-inflammatory medication directly into the spinal canal.
- Effectiveness: These injections provide temporary relief from nerve compression symptoms, such as radiating leg pain, and may help patients avoid or delay surgery.
- Lifestyle Modifications
- Postural Adjustments: Proper ergonomics at work and home reduce spinal stress. Using lumbar supports while sitting and practicing good posture are simple yet effective measures.
- Weight Management: Maintaining a healthy weight decreases pressure on the spine, preventing further degeneration.
- Activity Modification: Avoiding activities that exacerbate symptoms, such as prolonged standing or heavy lifting, helps manage pain.
- Assistive Devices
- Purpose: Devices like canes or walkers provide stability and reduce the load on the lumbar spine during movement.
- Application: These tools are particularly beneficial for individuals experiencing neurogenic claudication, which causes pain and weakness during walking.
When Surgery Becomes Necessary
While non-surgical treatments are effective for many individuals, surgery becomes a consideration when symptoms are severe, persistent, or unresponsive to conservative measures. Surgical interventions aim to relieve nerve compression, stabilize the spine, and improve overall function.
- Indications for Surgery
- Progressive Neurological Symptoms: Persistent numbness, weakness, or tingling in the lower extremities that impairs daily activities.
- Severe Pain: Pain that significantly reduces quality of life and is unresponsive to medication or physical therapy.
- Loss of Function: Difficulty walking, standing, or performing daily tasks due to neurogenic claudication or spinal instability.
- Cauda Equina Syndrome: This rare but serious condition involves compression of the cauda equina nerves, leading to bowel or bladder dysfunction and requiring emergency surgery.
- Surgical Procedures
- Laminectomy: The most common surgery for lumbar stenosis, laminectomy involves removing part of the vertebra (the lamina) to relieve pressure on the spinal cord and nerves.
- Foraminotomy: This procedure enlarges the foramina, the openings where nerve roots exit the spinal canal, to alleviate nerve compression.
- Spinal Fusion: In cases of instability or spondylolisthesis, spinal fusion stabilizes the affected vertebrae by fusing them together using bone grafts or implants.
- Minimally Invasive Surgery (MIS): MIS techniques involve smaller incisions, less tissue damage, and shorter recovery times compared to traditional open surgeries.
- Post-Surgical Recovery
- Recovery times vary depending on the procedure and individual factors. Most patients begin physical therapy soon after surgery to regain strength and mobility.
- Follow-up care is crucial to monitor healing, manage any complications, and prevent recurrence.
Preventing Lumbar Stenosis Worsening
While lumbar stenosis often results from age-related degeneration, proactive measures can help slow its progression and alleviate symptoms. Maintaining spinal health through lifestyle adjustments and preventive strategies is crucial for long-term management.
Keeping Your Spine Healthy
Healthy spinal habits are foundational for preventing the worsening of lumbar stenosis. Regular care and awareness can reduce stress on the lumbar spine and maintain mobility.
- Stay Active:
- Engage in low-impact activities such as walking, swimming, or cycling to promote circulation, flexibility, and strength.
- Avoid prolonged periods of inactivity, which can lead to stiffness and muscular imbalances.
- Good Posture:
- Maintain a neutral spine position during daily activities to minimize unnecessary stress.
- Practice proper lifting techniques by bending at the knees and keeping heavy objects close to the body.
- Hydration and Nutrition:
- Drink plenty of water to support disc hydration and joint lubrication.
- Consume a balanced diet rich in anti-inflammatory foods, including fruits, vegetables, and omega-3 fatty acids, to combat inflammation and support tissue repair.
Ergonomics, Exercises, and Weight Management
Adopting ergonomic practices, targeted exercises, and weight management can significantly impact the progression of lumbar stenosis.
- Ergonomics:
- Optimize your workspace:
- Use a chair with lumbar support to maintain the natural curve of the spine.
- Position computer screens at eye level to avoid neck strain.
- Take frequent breaks to stretch and move during long periods of sitting or standing.
- Use supportive footwear to reduce impact on the spine during walking or standing.
- Optimize your workspace:
- Exercises:
- Incorporate specific exercises to strengthen the core, improve flexibility, and reduce spinal load:
- Core Strengthening:
- Planks and bridges stabilize the lumbar spine and reduce pressure on the vertebrae.
- Stretching:
- Hamstring and hip flexor stretches improve lower body flexibility, relieving tension on the lumbar region.
- Pelvic Tilts:
- Gentle pelvic tilts promote mobility and reduce stiffness in the lower back.
- Flexion Exercises:
- Forward bending movements create more space in the spinal canal, reducing nerve compression.
- Core Strengthening:
- Incorporate specific exercises to strengthen the core, improve flexibility, and reduce spinal load:
- Weight Management:
- Maintain a healthy weight to decrease the mechanical load on the lumbar spine.
- Combine regular physical activity with a nutritious diet to achieve and sustain an optimal weight.
Osteopathic Support in Prevention
Osteopathy can play a pivotal role in preventing the worsening of lumbar stenosis by addressing biomechanical and systemic factors:
- Regular Assessments:
- Osteopaths can identify and correct postural or movement dysfunctions that contribute to spinal stress.
- Manual Therapy:
- Techniques like soft tissue massage and gentle mobilizations improve circulation and restore balance to the musculoskeletal system.
- Patient Education:
- Guidance on ergonomic setups, home exercises, and lifestyle adjustments empowers patients to take an active role in their spinal health.
Radiographic signs of lumbar stenosis
Radiographic imaging plays a crucial role in diagnosing lumbar spinal stenosis, providing valuable insights into the structural changes within the spine that contribute to narrowing of the spinal canal. Several radiographic signs are indicative of lumbar stenosis, including changes in intervertebral disc height, facet joint hypertrophy, ligamentum flavum thickening, and evidence of neural compression.
One of the hallmark radiographic signs of lumbar stenosis is a reduction in intervertebral disc height. Degenerative changes in the spine, such as disc desiccation and herniation, can lead to decreased disc height, contributing to the collapse of the disc space and narrowing of the spinal canal. This reduction in disc height is often accompanied by osteophyte formation along the vertebral bodies, further encroaching upon the space available for the nerves.
Facet joint hypertrophy is another common radiographic finding associated with lumbar stenosis. As the facet joints degenerate due to osteoarthritis, they may undergo hypertrophy or enlargement, resulting in the formation of bone spurs and narrowing of the neural foramina. This narrowing can impinge upon the exiting nerve roots, leading to symptoms of radiculopathy such as pain, numbness, and weakness in the lower back and legs.
Thickening of the ligamentum flavum is also observed in patients with lumbar stenosis and can be visualized on radiographic imaging. The ligamentum flavum is a strong, elastic ligament that runs along the posterior aspect of the spinal canal, helping to maintain its integrity. In response to degenerative changes and increased mechanical stress, the ligamentum flavum may hypertrophy and thicken, further encroaching upon the already narrowed spinal canal and compressing the neural elements within it.
Radiographic signs of neural compression are crucial for confirming the diagnosis of lumbar stenosis and assessing its severity. Compression of the nerve roots within the spinal canal can result in foraminal narrowing, where the passageways through which the nerves exit the spinal canal become constricted. This can be visualized on imaging studies such as MRI or CT scans, which can also reveal evidence of nerve root impingement, such as nerve root displacement or flattening
- Narrowing of the spinal canal: X-rays may show narrowing of the spinal canal in the lumbar region, which is characteristic of lumbar stenosis.
- Osteophyte Formation: Osteophytes, or bony growths, can develop along the edges of the vertebrae, contributing to the narrowing of the spinal canal.
- Facet joint hypertrophy: The facet joints, which connect the vertebrae, can become hypertrophied in response to increased stress on the spine, also contributing to narrowing of the canal.
- Displaced intervertebral discs: A herniated disc or displacement of the intervertebral discs can put pressure on surrounding structures, contributing to the symptoms of stenosis.
- Spinal Instability: X-ray can also reveal signs of spinal instability, although this can be more accurately assessed with other imaging tests such as MRI.
It is important to note that the diagnosis of lumbar stenosis does not rely solely on x-rays, and other imaging tests such as MRI (magnetic resonance imaging) may also be necessary to obtain a complete assessment of the structures. of the spine and surrounding soft tissues.


Conclusion
In conclusion, lumbar spinal stenosis is a degenerative condition of the spine that results from the narrowing of the spinal canal in the lumbar region. This process may be related to the body’s natural aging and various anatomical changes that occur over time.
The forward flexion test, or stoop test, is emerging as an important diagnostic tool in the evaluation of spinal stenosis. By asking the patient to lean forward, this test seeks to reproduce the symptoms associated with the condition, thereby contributing to the clinical confirmation of the diagnosis.
Symptoms of lumbar spinal stenosis, such as lower back pain, leg radiation, numbness, and muscle weakness, may be exacerbated by certain movements and positions. The forward bend test aims to induce these symptoms by increasing the narrowing of the spinal canal during flexion.
Management of lumbar spinal stenosis depends on the severity of symptoms and may involve non-surgical approaches such as physical therapy, anti-inflammatory medications, and lifestyle adjustments. For cases that are more severe or resistant to conservative treatment, surgical options, such as decompressive laminectomy, may be considered to relieve spinal nerve compression.
It is essential to emphasize that lumbar spinal stenosis requires a personalized approach from healthcare professionals, taking into account the complexity of symptoms and variability from person to person. Combining the forward bend test with other clinical assessment and imaging elements contributes to a better understanding of the condition, allowing the development of treatment plans tailored to individual patient needs. By continuing to explore and understand the underlying mechanisms of lumbar spinal stenosis, healthcare professionals can improve their ability to relieve symptoms and improve the quality of life of those affected by this condition.
References
- Tang C, Moser FG, Reveille J, Bruckel J, Weisman MH. Cauda Equina Syndrome in Ankylosing Spondylitis: Challenges in Diagnosis, Management, and Pathogenesis. J Rheumatol. 2019 Dec;46(12):1582-1588. [ PubMed ]
- Glassman DM, Magnusson E, Agel J, Bellabarba C, Bransford RJ. The impact of stenosis and translation on spinal cord injuries in traumatic cervical facet dislocations. Spine J. 2019 Apr;19(4):687-694. [ PubMed ]
- Bindal S, Bindal SK, Bindal M, Bindal AK. Noninstrumented Lumbar Fusion with Bone Morphogenetic Proteins for SpinalStenosis with Spondylolisthesis in the Elderly. World Neurosurg. 2019 Jun;126:e1427-e1435. [ PubMed ]
- Messiah S, Tharian AR, Candido KD, Knezevic NN. Neurogenic Claudication: a Review of Current Understanding and Treatment Options. Curr Pain Headache Rep. 2019 Mar 19;23(5):32. [ PubMed ]
- Urits I, Burshtein A, Sharma M, Testa L, Gold PA, Orhurhu V, Viswanath O, Jones MR, Sidransky MA, Spektor B, Kaye AD. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Curr Pain Headache Rep. 2019 Mar 11;23(3):23. [ PubMed ]
- Bagley C, MacAllister M, Dosselman L, Moreno J, Aoun SG, El Ahmadieh TY. Current concepts and recent advances in understanding and managing lumbar spine stenosis . F1000Res. 2019;8 [ PMC free article ] [ PubMed ]
- Melancia JL, Francisco AF, Antunes JL. Spinalstenosis . Handb Clin Neurol. 2014;119:541-9. [ PubMed ]
- Akar E, Somay H. Comparative morphometric analysis of congenital and acquired lumbar spinal stenosis . J Clin Neurosci. 2019 Oct;68:256-261. [ PubMed ]
- Schroeder GD, Kurd MF, Vaccaro AR. Lumbar SpinalStenosis : How Is It Classified? J Am Acad Orthop Surg. 2016 Dec;24(12):843-852. [ PubMed ]
- Shim DM, Kim TG, Koo JS, Kwon YH, Kim CS. Is It Radiculopathy or Referred Pain? Buttock Pain in SpinalStenosis Patients. Clin Orthop Surg. 2019 Mar;11(1):89-94. [ PMC free article ] [ PubMed ]
- Stienen MN, Ho AL, Staartjes VE, Maldaner N, Veeravagu A, Desai A, Gautschi OP, Bellut D, Regli L, Ratliff JK, Park J. Objective measures of functional impairment for degenerative diseases of the lumbar spine: a systematic review of the literature. Spine J. 2019 Jul;19(7):1276-1293. [ PubMed ]
- Kaye AD, Manchikanti L, Novitch MB, Mungrue IN, Anwar M, Jones MR, Helander EM, Cornett EM, Eng MR, Grider JS, Harned ME, Benyamin RM, Swicegood JR, Simopoulos TT, Abdi S, Urman RD, Deer TR , Bakhit C, Sanapati M, Atluri S, Pasupuleti R, Soin A, Diwan S, Vallejo R, Candido KD, Knezevic NN, Beall D, Albers SL, Latchaw RE, Prabhakar H, Hirsch JA. Responsible, Safe, and Effective Use of Antithrombotics and Anticoagulants in Patients Undergoing Interventional Techniques: American Society of Interventional Pain Physicians (ASIPP) Guidelines. Pain Physician. 2019 Jan;22(1S):S75-S128. [ PubMed ]
- Credit in part: Lite Wu; Ricardo Cruz.
- Credit in part René Cailliet, Low back pain edition 3


















{kind=link}