

Meralgia paresthetica is dysesthesia on the anterior medial aspect of the thigh. This condition is caused by compression of the lateral femoral cutaneous nerve that runs along the anterior part of the hip and thigh.
Definition of dysesthesia : Dysesthesia occurs when the sensitivity of a part of the body is altered . Dysesthesias include tingling, tingling, burning and/or irritation, pain and numbness
Synonym : Femorocutaneous neuralgia, Femorocutaneous nerve syndrome, Bernhardt Roth syndrome, Lateral femoral cutaneous nerve syndrome, Lateral femoral cutaneous neuralgia.
Introduction
Meralgia paresthetica, a condition characterized by neuralgia, manifests through a spectrum of discomfort including pain, numbness, and dysesthesia specifically in the distribution of the lateral femoral cutaneous nerve. The predominant symptoms typically manifest as a burning pain along the lateral thigh, accompanied by heightened skin tenderness. Those afflicted with meralgia paresthetica often notice that certain activities, such as sitting, squatting, or wearing low-waisted clothing and wide belts, exacerbate their symptoms. The intricacies of this neuralgia point to the sensitivity and intricate interplay of the lateral femoral cutaneous nerve, causing distressing sensations that can significantly impact the quality of daily life.
The distinctive features of meralgia paresthetica stem from the compression or irritation of the lateral femoral cutaneous nerve, leading to the array of symptoms experienced by affected individuals. The burning pain along the lateral thigh is a hallmark of this condition and can range from mild discomfort to more severe and persistent sensations. This discomfort is often accompanied by numbness and dysesthesia, contributing to the complexity of the neuralgia.
Understanding the triggers and aggravating factors is pivotal for individuals dealing with meralgia paresthetica. The correlation between specific activities—such as sitting or wearing certain types of clothing—and the exacerbation of symptoms highlights the need for lifestyle modifications and targeted management strategies. The challenge lies in navigating daily routines to minimize the impact of these triggers, thus improving the overall well-being of individuals grappling with meralgia paresthetica.
Effective management of meralgia paresthetica involves a multifaceted approach. Medical interventions may include pain management strategies, such as medications or nerve blocks, aimed at alleviating the discomfort associated with the condition. Physical therapy and exercises that focus on the affected area can play a crucial role in enhancing flexibility and reducing nerve compression. Additionally, lifestyle adjustments, such as avoiding prolonged periods of sitting or wearing restrictive clothing, form an integral part of the overall management plan.
For those grappling with meralgia paresthetica, the impact extends beyond physical symptoms. The condition’s influence on daily activities and the challenges it poses can lead to a significant reduction in the quality of life. Exploring a comprehensive and personalized approach to managing meralgia paresthetica, which combines medical interventions, lifestyle modifications, and therapeutic exercises, is essential for minimizing the impact of this neuralgia. Ultimately, a nuanced understanding of the condition and a tailored management plan can empower individuals to navigate the complexities of meralgia paresthetica and regain control over their daily lives.
Compression often results from tight clothing, obesity, pregnancy, or prolonged standing or walking. Diagnosis involves recognizing the classic symptoms and may include physical examination or imaging if necessary. Treatment options range from lifestyle modifications, such as avoiding tight garments or weight management, to medications and, in severe cases, nerve decompression surgery. Understanding this anatomy is crucial for effective management and symptom relief.
Warning: For Informational Purposes Only: This article discusses Meralgia Paresthetica, a condition characterized by compression or irritation of the lateral femoral cutaneous nerve, leading to symptoms such as numbness, tingling, or burning pain in the outer thigh. While the information provided offers insights into the causes, symptoms, and potential treatments of this condition, it is not a substitute for professional medical advice, diagnosis, or treatment. Any osteopathic techniques or interventions mentioned herein are intended to inform readers about possible approaches to managing Meralgia Paresthetica. However, these techniques should only be performed by licensed osteopaths or qualified healthcare professionals trained in their safe and effective application. Attempting these techniques without proper guidance may result in harm or exacerbation of symptoms. If you suspect you have Meralgia Paresthetica or experience persistent discomfort in the affected areas, consult with a healthcare provider or osteopathic professional for a thorough evaluation and personalized treatment plan. Always seek professional guidance when dealing with nerve-related conditions to ensure appropriate care and avoid unnecessary complications.
Causes
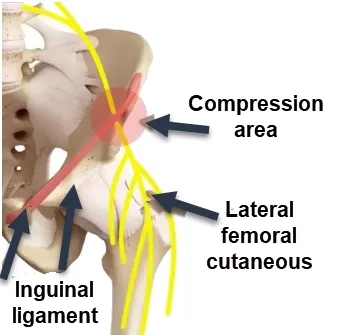
Meralgia paresthetica is a condition characterized by compression or irritation of the lateral femoral cutaneous nerve, leading to a spectrum of symptoms that can significantly impact an individual’s quality of life. The primary cause of meralgia paresthetica is compression of the nerve as it passes through the inguinal ligament, a band of tissue that runs across the front of the hip. This compression can result from various factors, and understanding these triggers is crucial in managing and preventing the condition.
One common cause of meralgia paresthetica is external pressure on the lateral femoral cutaneous nerve. Tight clothing, particularly belts or waistbands that cinch tightly around the waist, can compress the nerve and lead to the characteristic symptoms. Additionally, obesity can contribute to increased pressure on the nerve, making individuals with higher body mass indices more susceptible to developing meralgia paresthetica.
Pregnancy is another factor that can contribute to the development of meralgia paresthetica. The increased weight and pressure on the pelvic region during pregnancy may compress the lateral femoral cutaneous nerve, leading to symptoms. Hormonal changes during pregnancy could also play a role in the development of this condition.
In some cases, injury or trauma to the hip or pelvic region can lead to meralgia paresthetica. Accidents, falls, or surgical procedures in the area may cause compression or damage to the nerve, triggering the onset of symptoms. Individuals involved in activities that place repetitive stress on the hip, such as long-distance cycling or prolonged sitting, may also be at an increased risk.
Certain medical conditions, such as diabetes, can contribute to nerve damage and increase the likelihood of developing meralgia paresthetica. Diabetic neuropathy, characterized by damage to peripheral nerves, can affect the lateral femoral cutaneous nerve, leading to symptoms of pain, numbness, and tingling along the outer thigh.
The diagnosis of meralgia paresthetica involves a comprehensive evaluation of the individual’s medical history, symptoms, and often includes imaging studies to rule out other potential causes. Once diagnosed, management strategies focus on addressing the underlying cause and relieving symptoms. This may involve lifestyle modifications, such as avoiding tight clothing or losing weight, and incorporating physical therapy exercises to alleviate nerve compression.
- Nerve Compression: The most common cause of meralgia paresthetica is compression of the lateral cutaneous nerve of the thigh as it passes through the groin. This compression can result from various factors, including wearing tight clothing, obesity, an overtight abdominal belt, or direct trauma to the groin area.
- Metabolic diseases: Certain medical conditions, such as diabetes, may increase the risk of developing meralgia paresthetica. Metabolic disorders can influence nerve function and increase susceptibility to compression.
- Trauma or Surgical Procedures: Trauma or surgical procedures to the groin, thigh or pelvic region can cause compression of the lateral cutaneous nerve, leading to meralgia paresthetica.
- Pregnancy: In some pregnant women, increased pressure on the pelvic nerves from the growing uterus may contribute to the development of meralgia paresthetica.
- Tumors: Although rarer, tumors or lesions in the pelvic area can put pressure on the lateral cutaneous nerve, causing symptoms of meralgia paresthetica.
Symptoms
Meralgia paresthetica manifests through a distinctive set of symptoms, causing discomfort and altered sensations along the outer thigh. The hallmark symptom is often described as a burning or tingling pain that extends from the hip to the knee. This discomfort may vary in intensity, ranging from a mild annoyance to more severe, persistent pain. Individuals experiencing meralgia paresthetica may also report numbness in the affected area, adding a layer of sensory disruption to the condition. The lateral femoral cutaneous nerve, responsible for transmitting signals from the skin on the outer thigh to the brain, undergoes compression or irritation in this condition, leading to the altered sensations.
The symptoms of meralgia paresthetica are typically unilateral, affecting only one side of the body. The lateralization of symptoms provides a diagnostic clue for healthcare professionals evaluating individuals presenting with outer thigh discomfort. The pain or tingling sensation may be exacerbated by certain activities, such as prolonged standing, walking, or wearing tight clothing. Patients often report an increase in symptoms when engaging in movements that involve bending or stretching the hip joint.
Skin tenderness is another characteristic symptom of meralgia paresthetica. The affected area may become hypersensitive to touch, with even light pressure causing discomfort. This tenderness is often localized to the lateral thigh region corresponding to the distribution of the lateral femoral cutaneous nerve.
Individuals with meralgia paresthetica may notice that specific positions or activities worsen their symptoms. Prolonged periods of sitting, squatting, or wearing low-waisted clothing and tight belts can exacerbate the discomfort. The correlation between certain triggers and the aggravation of symptoms emphasizes the importance of lifestyle modifications in managing meralgia paresthetica.
The diagnosis of meralgia paresthetica involves a thorough clinical evaluation, considering the characteristic symptoms and potential contributing factors. Healthcare providers may conduct neurological examinations to assess sensory function and may order imaging studies to rule out other underlying conditions. Once diagnosed, the focus of management is on alleviating symptoms and addressing the underlying cause. Treatment strategies may include lifestyle modifications, such as avoiding activities that worsen symptoms, and incorporating physical therapy exercises to improve hip mobility and reduce nerve compression.
In summary, the symptoms of meralgia paresthetica, including burning or tingling pain, numbness, and skin tenderness along the outer thigh, are indicative of the compression or irritation of the lateral femoral cutaneous nerve. Recognizing these distinctive symptoms is crucial for accurate diagnosis and timely intervention to manage the discomfort and improve the overall quality of life for individuals affected by this nerve disorder.
- Tingling or tingling sensation: People with meralgia paresthetica may feel a tingling or tingling sensation on the surface of the thigh. This feeling may be intermittent or constant.
- Burning or pain: Some individuals may experience a burning sensation or pain in the affected area, usually on the outer side of the thigh. These sensations can vary in intensity.
- Numbness: Numbness, which can be mild or more pronounced, is another common symptom of meralgia paresthetica. This can make the skin feel numb or “sleepy.”
- Increased sensitivity: The affected area may become more sensitive to touch, and unpleasant sensations may be triggered by contact with clothing or other mild stimuli.
- Worse when standing or walking: Symptoms of meralgia paresthetica tend to get worse when standing or walking, as this can increase pressure on the lateral cutaneous nerve of the thigh.
- Sensitivity to temperature change: Some individuals with meralgia paresthetica may experience increased sensitivity to temperature change in the affected area. Exposure to hot or cold temperatures can trigger or worsen symptoms.
- Radiating pain: Pain or unpleasant sensations can sometimes radiate to other parts of the leg, knee, or hip, although the primarily affected area is usually the upper or anterior thigh.
- Worsened while sitting: Although standing and walking may worsen symptoms in some people, others may experience an increase in unpleasant sensations from sitting for long periods of time.
- Sensory Alterations: In addition to tingling and numbness, some people with meralgia paresthetica may experience sensory alterations such as an “electric shock” sensation or changes in skin perception.
- Responses to Direct Pressure: Applying direct pressure to the affected area may trigger or intensify symptoms in some people. For example, tightening a belt or wearing tight clothing can make unpleasant sensations worse.

The lateral femoral cutaneous nerve originates from the lumbar spine (L2-L3) and travels through the pelvis, passing under the inguinal ligament near the hip. It provides sensation to the skin of the lateral (outer) thigh. When this nerve is compressed, individuals often experience symptoms such as tingling, numbness, burning pain, or hypersensitivity in these highlighted areas. The red zone may indicate areas of higher intensity symptoms, while the yellow zone represents milder or broader involvement.
Compression can result from various factors, including tight clothing, obesity, pregnancy, prolonged standing, or repetitive hip flexion. Treatment involves identifying and addressing the underlying cause. Simple modifications such as loosening tight garments, weight management, and avoiding prolonged standing can often alleviate symptoms. In more severe cases, physical therapy, nerve blocks, or surgical intervention may be necessary.
Understanding this diagram helps clarify the affected areas and guides healthcare professionals in diagnosing and treating conditions associated with the lateral femoral cutaneous nerve. Early management is crucial for relieving discomfort and restoring quality of life.
Risk factors
Meralgia paresthetica is influenced by various risk factors that can increase an individual’s susceptibility to this nerve disorder. One significant risk factor is external pressure on the lateral femoral cutaneous nerve, often resulting from tight clothing, belts, or waistbands that constrict the waist area. Individuals who regularly wear such clothing may inadvertently subject the lateral femoral cutaneous nerve to chronic compression, contributing to the development of meralgia paresthetica. Moreover, obesity is a notable risk factor, as excess body weight places increased pressure on the pelvic region and the inguinal ligament, potentially compressing the nerve and triggering symptoms.
Certain occupational or lifestyle factors may also heighten the risk of developing meralgia paresthetica. Occupations that involve prolonged periods of standing, walking, or activities requiring repetitive hip movements, such as biking or weightlifting, can contribute to nerve compression and increase the likelihood of developing this condition. Similarly, individuals who engage in activities that involve direct trauma or injury to the hip and pelvic region may be at an elevated risk. Falls, accidents, or surgical procedures in this area can potentially lead to compression or damage to the lateral femoral cutaneous nerve.
Medical conditions, particularly those associated with nerve damage, serve as additional risk factors for meralgia paresthetica. Diabetes, for example, can cause peripheral neuropathy, affecting the function of nerves throughout the body, including the lateral femoral cutaneous nerve. Hormonal changes during pregnancy can also heighten the risk, as increased weight and pressure on the pelvic region may contribute to nerve compression. Additionally, underlying health conditions such as hypothyroidism or inflammatory disorders may influence nerve function and increase susceptibility to meralgia paresthetica.
Individual susceptibility to meralgia paresthetica may be further influenced by gender and age. Studies suggest that men may be more prone to developing this condition, possibly due to differences in body fat distribution and clothing styles. While meralgia paresthetica can occur at any age, it is more commonly reported in adults, with a higher prevalence in middle-aged individuals.
Recognition of these risk factors is crucial for both prevention and early intervention in individuals predisposed to meralgia paresthetica. Implementing lifestyle modifications, such as wearing loose-fitting clothing, maintaining a healthy weight, and incorporating regular exercise, can contribute to reducing the risk of developing this nerve disorder. Moreover, individuals with occupations involving prolonged standing or repetitive hip movements should be aware of potential risks and take preventive measures. By addressing these risk factors, individuals can proactively manage their health and minimize the likelihood of experiencing the discomfort associated with meralgia paresthetica.
- Obesity: Excess weight, particularly in the abdomen, can increase pressure on nerves in the pelvic region, including the lateral cutaneous nerve of the thigh, thereby promoting the development of meralgia paresthetica.
- Tight clothing: Wearing tight clothing around the waist, groin, or hips can put pressure on the lateral cutaneous nerve of the thigh, leading to symptoms of meralgia paresthetica.
- Pregnancy: Pregnant women are more likely to develop meralgia paresthetica due to the increased pressure placed on the pelvic nerves during pregnancy, as well as hormonal changes that can affect the nervous system.
- Diabetes: People with diabetes may be at increased risk of meralgia paresthetica due to the neurological complications associated with this metabolic disease.
- Surgery or trauma to the hip: Previous surgeries or trauma to the hip area can cause compression of the lateral cutaneous nerve, contributing to the symptoms of meralgia paresthetica.
- Activities that involve prolonged pressure on the pelvic region: Certain work or leisure activities that require prolonged pressure on the pelvic region, such as sitting for long periods of time, may increase the risk of meralgia paresthetica.
- Local inflammation or irritation: Local inflammatory conditions, such as bursitis, tendinitis, or irritation of surrounding tissues, can put pressure on the lateral cutaneous nerve and contribute to symptoms.
A Day in the Life of Someone Living with Meralgia Paresthetica
For someone living with Meralgia Paresthetica, each day begins with a lingering reminder of the condition as they get out of bed. The first steps of the day are often accompanied by a sharp, burning sensation along the outer thigh—a signal that the compressed lateral femoral cutaneous nerve is making its presence known. Despite the discomfort, they push through, knowing that this is just the start of what the day holds.
As they move through their morning routine, the act of bending down to put on socks or shoes can be challenging. The pain intensifies with movements that involve the hip, making something as simple as tying shoelaces feel like an ordeal. They might take a moment to gently massage the affected area, hoping to ease the numbness or tingling that often accompanies the pain, though relief is usually temporary.
Sitting down for breakfast can be another source of discomfort. Prolonged sitting exacerbates the symptoms, leading to a constant shifting in the chair, trying to find a position that offers some relief. If the day involves driving or sitting at a desk for long periods, the individual is likely to experience worsening pain and numbness, leading to a sense of frustration and exhaustion.
Walking offers some relief, but it’s a double-edged sword. While movement helps to reduce the nerve compression, too much walking or standing can trigger a flare-up, especially if the day involves activities that require prolonged standing, such as shopping or attending an event. The person might find themselves taking frequent breaks to rest, trying to strike a balance between staying active and not overdoing it.
In social situations, they may need to explain why they can’t sit for long or why they need to stand up frequently. This can lead to feelings of embarrassment or the need to avoid certain situations altogether. The chronic nature of Meralgia Paresthetica often means that the person must carefully plan their day, factoring in the need for breaks, comfortable seating, and strategies to manage the pain.
As the day winds down, the individual may look forward to lying down, hoping for some respite. However, even sleep can be elusive. The burning sensation might intensify when lying on the affected side, making it difficult to find a comfortable position. They might toss and turn, waking up frequently throughout the night, which only adds to the fatigue.
Despite the challenges, the person living with Meralgia Paresthetica learns to adapt. They become attuned to their body’s signals, knowing when to push through the pain and when to rest. They might explore different therapies, such as osteopathy, to manage their symptoms and improve their quality of life. Over time, they develop coping mechanisms, but each day remains a delicate balancing act, navigating the physical and emotional toll of the condition.
Differential diagnosis
- Crural neuralgia: Irritation or compression of the crural nerve can cause similar symptoms, such as pain and abnormal sensations in the thigh.
- Peripheral neuropathy: Conditions such as diabetes can lead to peripheral neuropathies, causing tingling, burning, and numbness in the lower extremities.
- Herniated lumbar disc: A herniated disc in the lumbar region can compress nerve roots and cause symptoms similar to meralgia paresthetica, such as thigh pain.
- Narrow lumbar canal syndrome: Narrowing of the lumbar spinal canal can lead to nerve compression, causing symptoms resembling those of meralgia paresthetica.
- Iliotibial Band Syndrome: Inflammation or irritation of the iliotibial band can cause pain and abnormal sensations along the thigh.
- Femoral Nerve Entrapment Syndrome: Compression of the femoral nerve can cause similar symptoms, such as pain and altered sensation in the thigh.
- Osteoarthritis of the hip: Osteoarthritis of the hip can cause pain in the pelvic region and thigh, which may be confused with the symptoms of meralgia paresthetica.
Recommendations
Management of meralgia paresthetica involves a range of recommendations aimed at alleviating symptoms, preventing exacerbations, and addressing underlying contributing factors. One primary recommendation is lifestyle modification, particularly in terms of clothing choices. Individuals affected by meralgia paresthetica are advised to wear loose-fitting clothing that minimizes pressure on the waist and hip areas. Opting for clothing styles that avoid tight belts or waistbands can significantly reduce compression on the lateral femoral cutaneous nerve, thereby mitigating symptoms.
Weight management is another crucial recommendation, as excess body weight places increased pressure on the pelvic region and exacerbates nerve compression. Adopting a healthy lifestyle that includes regular exercise and a balanced diet can contribute to weight maintenance and overall well-being. Physical activity should be tailored to avoid prolonged periods of standing or activities that involve repetitive hip movements, helping to minimize strain on the lateral femoral cutaneous nerve.
Individuals with meralgia paresthetica are encouraged to incorporate targeted exercises into their routine. Physical therapy focusing on hip mobility and strengthening exercises can be beneficial in relieving nerve compression. Stretching exercises that target the hip flexors and surrounding muscles can contribute to improved flexibility and reduced pressure on the lateral femoral cutaneous nerve.
Avoidance of specific postures or activities that worsen symptoms is a key recommendation. Prolonged periods of sitting, squatting, or engaging in activities that involve bending or stretching the hip joint should be minimized. Awareness of triggers and making conscious efforts to modify daily activities can contribute to symptom management and prevent exacerbations.
Medical interventions may be considered based on the severity of symptoms. Pain management strategies, including over-the-counter or prescribed medications, may be recommended to alleviate discomfort. In some cases, nerve blocks or injections may be administered to provide temporary relief. However, it’s essential to consult with a healthcare professional to determine the most appropriate medical interventions for individual cases.
In cases where meralgia paresthetica is associated with specific medical conditions, addressing the underlying health issue is paramount. For instance, individuals with diabetes should focus on managing their blood sugar levels to mitigate the impact on peripheral nerves. Hormonal changes during pregnancy may warrant closer monitoring and tailored interventions.
Regular follow-up with a healthcare provider is advised to track the progression of symptoms and adjust management strategies accordingly. In instances where conservative measures are insufficient, surgical options may be explored in consultation with a specialist.
- Consult a healthcare professional: If you think you have meralgia paresthetica, consult a doctor or neurologist for an accurate diagnosis. A healthcare professional will be able to assess your symptoms, determine the underlying cause and recommend a suitable treatment plan.
- Weight management: Maintaining a healthy weight can reduce pressure on nerves and ease symptoms. If you are overweight, gradual weight loss under the supervision of a healthcare professional may be beneficial.
- Wearing loose clothing: Avoid wearing tight clothing around the waist and hip, as this can put extra pressure on the affected nerve.
- Avoid awkward positions: Avoid standing or sitting in the same position for long periods of time. Change positions regularly to relieve pressure on the nerve.
- Use cushions or supports: A cushion or support can help relieve pressure on the nerve when you sit. Place it under the thigh to reduce pressure on the affected area.
- Physiotherapy: A physiotherapist can recommend specific exercises to strengthen the surrounding muscles and improve flexibility, helping to reduce pressure on the nerve.
- Medications: Your doctor may prescribe medications to relieve the pain and inflammation associated with meralgia paresthetica. These may include nonsteroidal anti-inflammatory drugs (NSAIDs), antidepressants or anticonvulsants.
- Avoid aggravating factors: Identify and avoid activities or positions that exacerbate your symptoms. For example, avoid crossing your legs for long periods of time.
- Heat and ice: Applying hot or cold compresses can help relieve pain and inflammation. Consult your healthcare professional to find out which option is best for your situation.
- Orthotics: In some cases, wearing orthotics or special belts can help reduce pressure on the nerve.
Frequently asked questions
- What is Meralgia Paresthetica (MP)?
- PD is a nerve condition characterized by abnormal sensations, such as tingling or burning, along the lateral cutaneous nerve of the thigh.
- What are the typical symptoms of PD?
- Symptoms include burning, tingling, numbness, or pain in the outer thigh.
- What are the common causes of Meralgia Paresthetica?
- Compression of the lateral cutaneous nerve of the thigh, often in the groin, is the primary cause of PD. This may result from tight clothing, weight gain, or other factors.
- How is Meralgia Paresthetica diagnosed?
- Diagnosis is based on medical history, physical examination, and sometimes neurological tests. Imaging tests may be done to rule out other causes.
- Is Meralgia Paresthetica a serious condition?
- Although generally not serious, PD can cause uncomfortable symptoms. Treatment is often aimed at relieving these symptoms.
- What are the treatment options for Meralgia Paresthetica?
- Treatments include self-care measures such as avoidance of triggers, medications to relieve pain, and sometimes corticosteroid injections. Weight loss may also be recommended.
- Can PD go away on its own?
- In some cases, PD may improve without treatment, especially if the underlying cause is identified and managed.
- What clothing or activities can make Meralgia Paresthetica worse?
- Tight clothing around the waist, especially belts, and activities that put pressure on the groin can make symptoms worse.
- Can specific exercises help relieve Meralgia Paresthetica?
- Stretching and muscle strengthening exercises can sometimes help relieve symptoms by reducing pressure on the nerve.
- When to consult a healthcare professional for Meralgia Paresthetica?
- Consult a healthcare professional if symptoms persist, worsen, or significantly affect your quality of life despite self-care measures.
Osteopathic treatments
Strain–Counterstrain
Psoas, TFL, Vastus lateralis and other muscles located in the region of the lateral femoral cutaneous nerve.
Diaphragm lift
The therapist stands sideways and faces the patient. The thumbs are placed just below the sternum, at the level of the costo-sternal junctions, while the rest of the fingers are distributed on the lateral edges of the ribs, towards the patient’s head. Asked the patient to exhale immediately after inhaling and not to hold their breath during this time, a cephalic and lateral lift is then performed by the therapist, lifting the diaphragm. Repeat this maneuver until all tension in the diaphragm is gone. When everything is finished, ask the patient to do the Valsalva maneuver (closing the throat and increasing intrathoracic pressure) and expanding the chest.

Muscle energy (Inflare, outflare)
Somatic dysfunction of the innominate
Iliac “inflare” . Somatic dysfunction of the iliac where we find a medial positioning of the EIAS; the iliac moves more easily in a medial direction and is more restricted in lateral movement
Iliac “outflare”. Somatic dysfunction of the iliac where we find a
lateral positioning of the EIAS; the iliac moves more freely in the
lateral direction and it is restricted in medial movement
Muscle energy (FRSR)
- The patient lies on his right side, knees and feet together, shoulders and pelvis perpendicular to the table.
- The therapist stands in front of the patient and, with his cephalad hand, touches the L2-L3 level.
- With his caudal hand, the therapist flexes the patient’s hips and knees until the movement is localized at the level of the L3 vertebral segment.
- The patient was instructed to straighten her lower leg and, with her caudad hand, the physician passively extended her to achieve movement at the L3 vertebral segment.
- The patient’s left upper leg was flexed and the foot placed in the popliteal space of the extended lower leg. The doctor then switched hands so that the caudal hand monitored the segment. The cephalad hand grasps the patient’s forearm and gently pulls it in an anterior and caudal direction until a rotational movement is felt at the L2-L3 level. The forearm is then moved backward and upward to induce flexion on the left side. The patient should now grasp the head of the table with the upper body while lying down. The patient was then instructed to take a deep breath, exhale completely and in doing so, reach to the lower part of the table by grasping the edge of the table with the upper arm and continue doing so for a few cycles respiratory. The physician then grasped the distal knee of the patient’s upper leg and raised it until the lumbar spine curved laterally toward the motion barrier, while monitoring the segment with the cephalad hand (Figure 4). The patient was asked to push her elevated foot toward the table for 3 to 5 seconds, while the physician provided isometric resistance. The patient was asked to relax for 3 to 5 seconds, after which the doctor elevated the foot further until movement was observed at the new barrier. The procedure was repeated at least three times, after which the somatic dysfunction improved. Finally, a passive stretch was performed after the last repetition.
Reference
- Kaiser R. Meralgia paresthetica. Rozhl Chir. 2018 Spring;97(6):286-290. [PubMed]
- Patijn J, Mekhail N, Hayek S, Lataster A, van Kleef M, Van Zundert J. Meralgia Paresthetica. Pain Practice. 2011 May-Jun;11(3):302-8. [ PubMed ]
- van Slobbe AM, Bohnen AM, Bernsen RM, Koes BW, Bierma-Zeinstra SM. Incidence rates and determinants in meralgia paresthetica in general practice. J Neurol. 2004 Mar;251(3):294-7. [ PubMed ]
- Grossman MG, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001 Sep-Oct;9(5):336-44. [PubMed]
- Berini SE, Spinner RJ, Jentoft ME, Engelstad JK, Staff NP, Suanprasert N, Dyck PJ, Klein CJ. Chronic meralgia paresthetica and neurectomy: a clinical pathologic study. Neurology. 2014 Apr 29;82(17):1551-5. [PMC free article] [PubMed]
- Harney D, Patijn J. Meralgia paresthetica: diagnosis and management strategies. Pain Med. 2007 Nov-Dec;8(8):669-77. [PubMed]
- Cheatham SW, Kolber MJ, Salamh PA. Meralgia paresthetica: a review of the literature. Int J Sports Phys Ther. 2013 Dec;8(6):883-93. [PMC free article] [PubMed]
- Credit in part, Ryan Coffey; Vikas Gupta.






")



















{kind=link}