

Clinical evidence indicates that 50% of all patients seen in hospital with an initial diagnosis of angina are indeed from a source other than cardiac. Pectoralis minor myofascial pain syndrome resembles that of an angina attack (1).
Introduction
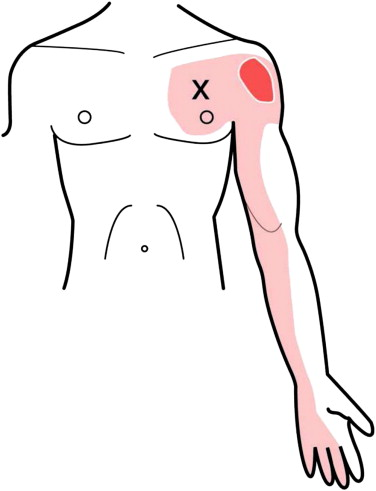
The pectoralis major, a powerful muscle located in the chest, is essential for many daily activities, from simple arm raises to more complex movements like shoulder rotation. However, despite its strength, the pectoralis major can be prone to painful trigger points, a condition that can cause symptoms sometimes confused with those of angina, giving rise to the term “pseudoangina.”
Painful trigger points are hyperirritable areas in the muscles, often felt as tight nodules or bands. In the case of the pectoralis major, these trigger points can cause local pain but also referred pain, which means that the pain is felt distant from the site of the injury. When these pains occur in the chest area, they can be misinterpreted as symptoms of angina.
Angina, also known as angina, is usually associated with insufficient blood supply to the heart muscle. Common symptoms include a feeling of tightness or pressure in the chest, sometimes accompanied by pain in the arms, neck, jaw, or back. These symptoms can be triggered by physical exertion or emotional stress.
In contrast, pseudoangina due to painful trigger points in the pectoralis major has similar characteristics, but is attributable to muscle tension rather than heart problems. Referred pain may radiate to the arm, neck, or even back, contributing to confusion with angina symptoms. It is essential to differentiate between these two conditions to ensure proper diagnosis and treatment.
The cause of trigger points in the pectoralis major can be varied, from muscle overuse to uncomfortable working positions. People who frequently perform repetitive arm movements or hold prolonged postures may be more prone to these trigger points. Additionally, factors such as stress, anxiety, and fatigue can also contribute to the formation of these tender points.
Treatment of pseudoangina related to pectoralis major trigger points often relies on approaches aimed at releasing muscle tension. Osteopathy, targeted stretching and massage can be effective in relieving pain and improving muscle mobility. In some cases, anti-inflammatory medications or muscle relaxants may be recommended.
In conclusion, although the pectoralis major is a strong muscle essential for many daily activities, it can be prone to painful trigger points that can lead to pseudoangina. Recognition of this condition is crucial to avoid confusion with angina and ensure appropriate symptom management. An accurate diagnosis, combined with appropriate therapeutic interventions, can help relieve pain and restore muscle functionality.
Define Pseudoangina
Pseudoangina, often called “false angina,” is a medical condition that has symptoms similar to angina, but is actually caused by muscular factors rather than heart problems. One of the most common examples of pseudoangina manifests through painful trigger points in the pectoralis major, a muscle located in the chest.
When painful trigger points form in the pectoralis major, they can cause local pain and referred pain, which is pain felt distant from the site of injury. This pain can often radiate to the arm, neck, or even back, creating a sensation of pain similar to that of angina. It is important to note that although the symptoms are similar, the underlying cause is different.
Painful trigger points often result from muscle overuse, awkward working positions, stress, or a combination of these factors. People who regularly perform repetitive arm movements, such as those involved in specific work or sporting activities, may be more prone to the formation of these tender points.
Symptoms of pseudoangina may include chest pain, tightness, or discomfort in the chest, similar to what one feels during an attack of angina. However, unlike angina, pseudoangina does not result from insufficient blood supply to the heart muscle, but rather from muscle tension in the pectoralis major.
Diagnosing pseudoangina often involves excluding other possible causes of chest pain, including heart problems. Tests such as electrocardiogram (ECG) may be performed to rule out the possibility of an underlying heart condition. When these tests rule out heart problems, attention turns to potential muscular causes.
Treatment of pseudoangina related to pectoralis major trigger points often relies on approaches aimed at releasing muscle tension. Osteopathy, which may include specific stretches, strengthening exercises and massage, is frequently recommended. Anti-inflammatory medications or muscle relaxants may also be prescribed to relieve pain and promote muscle relaxation.
In summary, pseudoangina is a condition that can mimic the symptoms of angina, but is caused by muscle problems rather than heart problems. In the particular case of pseudoangina related to pectoralis major trigger points, recognition of this condition is crucial for appropriate treatment. An accurate diagnosis, combined with tailored therapeutic interventions, can help relieve pain and restore muscle function, thereby improving the quality of life of those affected.
Dr. Janet Travell: Pioneer of Myofasciology
- Holistic Approach: Dr. Travell, in collaboration with Dr. David Simons, has developed a holistic approach to understanding muscular disorders, with particular emphasis on myofascial trigger points. They demonstrated that these points, when activated, can cause referred pain and muscle dysfunction.
- Identifying Trigger Points: Their work involved extensive identification of trigger points in muscles, including the pectoralis major. They emphasized the importance of recognizing these tender points to effectively treat muscle disorders.
Syndrome Myofascial du Grand Pectoral : Contribution de Travell
- Referred Pain in the Chest: The pectoralis major, being an important muscle of the chest, can develop trigger points responsible for referred pain. Travell’s work has contributed to the understanding of how these pains can sometimes mimic the symptoms of angina.
- Evidence-Based Treatments: Dr. Travell advocated evidence-based treatments for trigger points, including the application of manual pressure to deactivate these points and relieve associated pain.
- Relationship to Other Conditions: Travell’s work has also shed light on the relationship between pectoralis major myofascial syndrome and other conditions, such as rounded shoulders, highlighting the importance of treating underlying muscular imbalances.
- Multidisciplinary Treatment: She emphasized the importance of a multidisciplinary approach to treating myofascial disorders, encouraging collaboration between health professionals, including osteopaths, massage therapists and doctors.
Dr. Janet Travell’s legacy lies in her essential contributions to the understanding of muscular disorders, including pectoralis major myofascial syndrome. His work laid the foundation for effective treatment approaches and continues to influence clinical practices in the field of physical medicine and rehabilitation.
Causes
- Repetitive Movements: Frequently performing repetitive movements, especially in specific work or sports activities, can lead to excessive muscle contractions in the pectoralis major, contributing to the development of painful trigger points.
- Poor Posture: Maintaining improper posture, such as sitting or standing incorrectly for long periods of time, can create excessive tension in the pectoralis major. This can lead to the development of trigger points and contribute to myofascial syndrome.
- Emotional Stress: Emotional stress can cause widespread muscle tension throughout the body, including the pectoralis major. Chronic tension due to stress can encourage the development of trigger points and contribute to muscle irritation.
- Muscular Imbalances: An imbalance between the agonist and antagonist muscles, particularly between the pectoralis major and the back muscles, can lead to overload and excessive tension in the pectoralis major. This can create an environment conducive to the development of myofascial syndrome.
- Physical Trauma: Physical trauma, such as direct injuries or accidents, can trigger the formation of trigger points in the pectoralis major. Muscles may respond by contracting to protect the affected area, leading to persistent muscle tension.
- Unilateral Activities: Frequently participating in unilateral activities, where one side of the body is used more than the other, can lead to muscle imbalances. This can affect the pectoralis major, encouraging the development of trigger points.
- Genetic Factors: Some individuals may have a genetic predisposition to developing trigger points and myofascial conditions. However, the genetic contribution to myofascial syndrome is not yet completely understood.
Symptoms
- Local Pain: Pain in the pectoralis major region is one of the predominant symptoms. It may be felt as a stabbing, dull or burning pain and is usually concentrated in the chest.
- Referred Pain: Pectoralis major myofascial syndrome can cause referred pain, meaning the pain is felt in areas away from the muscle itself. This can include the shoulder area, upper back, and even the arm, sometimes mimicking the symptoms of angina.
- Feeling of Tightness: Some individuals may feel a feeling of tightness or constriction in the chest, often associated with muscle contraction in the pectoralis major.
- Muscle Stiffness: Muscle stiffness, particularly during arm or shoulder movements, may be present. This can affect normal shoulder mobility.
- Painful Trigger Points: The pectoralis major can develop trigger points, specific areas of the muscle that are hypersensitive to touch. Pressure on these points can trigger or worsen pain.
- Headaches: Muscle tension in the pectoralis major area can contribute to headaches, particularly in the temples and forehead.
- Difficulty Breathing: In some cases, people may experience difficulty breathing or chest tightness, although this is less common.
- Muscle Fatigue: Persistent muscle fatigue in the pectoralis major region may be present, affecting the ability to perform certain physical activities.
Pathophysiology
The pathophysiology of pectoralis major syndrome giving rise to pseudoangina involves complex mechanisms linked to painful trigger points and muscular tension in the muscle in question. Understanding these processes may help explain why angina-like symptoms can occur, despite a non-cardiac origin.
- Painful Trigger Points: Painful trigger points are specific areas in the muscles that are hyperirritable and sensitive to pressure. In the case of the pectoralis major, these points can form due to various factors such as muscular overuse, uncomfortable working positions, muscle trauma or chronic tension.
- Radiation of pain: When trigger points form in the pectoralis major, the pain is not necessarily limited to the affected area. It can radiate to other parts of the body, including the arm, neck and back. This radiation of pain is what creates a sensation of pain similar to that of angina, where pain can be felt in areas far from the original site.
- References to other parts of the body: Pain referred to in the case of the pectoralis major can sometimes be confused with symptoms of angina. The nerves that innervate the pectoralis major have connections to other parts of the body, contributing to the sensation of pain in areas that are commonly associated with angina.
- Trigger Point Activation: Activation of trigger points in the pectoralis major can be triggered by specific movements, prolonged positions or muscular stresses. These activations can cause local release of inflammatory chemicals and changes in local blood flow, thereby contributing to the sensation of pain.
- Interaction with nerves and the nervous system: Trigger points can influence the signals sent by nerves to the central nervous system. This can lead to an amplification of pain sensations and an inappropriate response to stimuli that would not normally cause pain.
- Differential diagnosis: Due to the similarity of symptoms between pseudoangina and angina, the differential diagnosis is crucial. Doctors can use tests such as an electrocardiogram (ECG) to rule out underlying heart problems and confirm that symptoms are related to muscle problems.
- Response to muscle treatments: Pseudoangina due to the pectoralis major often responds favorably to muscle treatments, such as osteopathy, targeted stretching, massage, and sometimes the use of anti-inflammatory medications or muscle relaxants. This positive response to muscular interventions reinforces the involvement of the muscles in the condition.
In summary, the pathophysiology of pectoralis major syndrome giving rise to pseudoangina is related to the formation of painful trigger points in the muscle, resulting in referred pain and a pain sensation similar to that of angina pectoris. Understanding these mechanisms is essential for an accurate diagnosis and to guide therapeutic approaches towards the management of muscle tension.
Factors causing pectoralis major myofascial syndrome
- Excessive muscle tension: Overuse or excessive tension of the pectoralis major muscle, often due to repetitive activities or unusual movements, can cause painful trigger points.
- Improper posture: Poor posture, especially posture that causes muscle imbalance, can put excessive pressure on the pectoral muscle, encouraging the development of painful trigger points.
- Physical trauma: Direct injuries, such as bruises or accidents, can damage the muscle fibers of the pectoralis major and contribute to the formation of painful trigger points.
- Emotional stress: Stress and anxiety can cause generalized muscle tension, including in the pectoralis major muscle, which can encourage the development of trigger points.
- Repetition of movements: Work or sports activities that involve repetitive movements of the arms and shoulders can contribute to the appearance of trigger points in the pectoral muscle.
- Poor Ergonomics: Frequent use of ill-fitting equipment or poor ergonomics at work or during exercise can lead to overuse of the pectoral muscle and contribute to myofascial syndrome.
- Sleep habits: Uncomfortable sleeping positions or inappropriate pillows can lead to muscle tension during the night, leading to the development of trigger points.

Exercise and stretching to relieve discomfort caused by pectoralis major myofasial syndrome
1. Pectoral Major Stretch:
- Stand near a corner of a wall or door.
- Place your forearm against the surface with your elbow bent at 90 degrees.
- Take a step forward to feel a stretch in the pectoralis major.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
2. Self-Massage with a Tennis Ball:
- Lie on the floor with a tennis ball under your pectoral major.
- Gently roll the ball over the tense area, looking for trigger points.
- Apply controlled pressure to sore spots for 15 to 30 seconds.
- Repeat as needed.
3. Shoulder Wedge Stretch:
- Stand in a corner with your arms on each wall, forming a 90-degree angle.
- Take a step forward to stretch your pectoral muscles and shoulders.
- Hold the position for 15 to 30 seconds.
- Repeat several times.
4. Back Muscle Strengthening Exercises:
- Perform exercises such as rows, lat pulldowns, and upper back extensions to strengthen the muscles opposite the pectoralis major.
- These exercises can help restore muscle balance.
5. Shoulder Stretch with a Strap or Towel:
- Hold a strap or towel behind your back with both hands.
- Slowly raise your arms while stretching the strap.
- Hold the position for 15 to 30 seconds.
- Repeat several times.
6. Stretching with a Door Frame:
- Stand in a doorway with your arms at shoulder height.
- Place your forearms and hands against the door frame.
- Take a slight step forward, leaning forward slightly to feel the stretch in the pectoralis major.
- Hold the position for 15 to 30 seconds.
- Repeat several times.
























{kind=link}