

Introduction
Overview of Rotator Cuff Tendinitis in Baseball Pitchers
Rotator cuff tendinitis is a common overuse injury among baseball pitchers, characterized by inflammation and microtears in the tendons of the rotator cuff muscles. These muscles play a crucial role in stabilizing the shoulder joint during the repetitive and high-intensity motions required for pitching. The nature of the sport, which demands maximum external and internal rotation of the arm, places significant stress on the shoulder. Over time, this can lead to pain, decreased range of motion, and impaired performance.
The condition often develops due to the repetitive overhead throwing motions inherent in baseball, which involve extreme angular velocities and forces. Without proper technique and conditioning, these movements can cause microtrauma to the rotator cuff tendons, eventually leading to chronic inflammation, tears, and reduced functional stability of the shoulder.
Importance of Proper Mechanics and Injury Prevention
Proper throwing mechanics are essential to minimize the risk of rotator cuff tendinitis. The throwing motion is a complex sequence that relies on the coordinated action of the lower body, core, and shoulder—often referred to as the “kinetic chain.” Any disruption in this chain can increase stress on the shoulder, leading to compensatory movements that heighten the risk of injury.
Prevention strategies focus on enhancing strength, flexibility, and neuromuscular control throughout the kinetic chain. Strengthening the surrounding musculature, such as the scapular stabilizers and core muscles, helps maintain dynamic stability. Additionally, maintaining proper posture and throwing mechanics can reduce undue stress on the rotator cuff.
Early identification of symptoms and addressing muscular imbalances or mechanical flaws are critical to avoiding long-term complications. For baseball pitchers, a proactive approach that includes regular assessments, conditioning programs, and education on proper techniques can significantly reduce the likelihood of rotator cuff tendinitis and enhance overall athletic performance.

.
Ball throwing movement phase
The lower limbs and trunk play a fundamental role as force generators, ensuring optimal energy production and transfer to propel the ball upon release. The harmonious coordination of this “kinetic chain” proves crucial to minimize the need for strong stress on the shoulder.
The throwing motion contributes to the smooth synchronization of this kinetic chain. The scapula occupies a key position in influencing the positioning of the glenoid, thus allowing extreme movements without impact. If the kinetic chain is broken at any level, it places increased stress on the shoulder, necessary to maintain normal throwing speed, control and performance.
A thorough understanding of the components of the kinetic chain and the mechanics of normal throwing is essential. The glenohumeral joint offers a variety of extreme movements. The action of throwing a baseball requires the rotator cuff to support repetitions of contractions and relaxations without dysfunction. The precise role of the cuff is to position and center the humeral head with great precision in the shallow glenoid fossa during the throw. This delicate balance is commonly referred to as the “ pitcher’s paradox .”
Throwing Mechanics
External and Internal Rotations in Throwing
The throwing motion in baseball places extraordinary demands on the shoulder, particularly during external and internal rotations. External rotation occurs as the pitcher winds up, bringing the arm backward to generate the energy required for the throw. This phase stretches the muscles and tendons of the rotator cuff to their maximum capacity, creating a “cocking” position. The shoulder joint undergoes extreme stress in this position, with the humeral head positioned within the shallow glenoid fossa, stabilized by the surrounding musculature and connective tissues.
Internal rotation follows as the arm propels forward during the acceleration phase. This movement requires a rapid and forceful contraction of the internal rotators, such as the subscapularis muscle, while the external rotators decelerate the motion to maintain joint stability. The transition from external to internal rotation must occur seamlessly, as improper timing or muscle imbalance can lead to excessive wear and tear on the rotator cuff tendons and ligaments. This repetitive stress, common in baseball pitchers, is a primary contributor to overuse injuries like rotator cuff tendinitis.
Role of the Kinetic Chain in Energy Transfer
The kinetic chain plays a pivotal role in generating and transferring energy during the throwing motion. This biomechanical concept describes how different body segments work together in a coordinated sequence to produce efficient and powerful movement. For pitchers, the kinetic chain starts in the lower body, with the legs and hips generating force through ground reaction. This energy is then transferred to the torso and upper body, culminating in the throwing arm.
Proper coordination of the kinetic chain ensures that the energy flows efficiently from the ground up, reducing the stress placed on the shoulder. The legs and core provide the foundation for force production, while the scapula acts as a stable base for the shoulder joint. The scapulothoracic rhythm, or the synchronized movement between the scapula and the thorax, is critical in positioning the glenoid optimally for the humeral head. Any breakdown in the kinetic chain—such as weak hip rotation, limited trunk mobility, or scapular dyskinesis—can force the shoulder to compensate, leading to excessive strain and potential injury.
Efficient energy transfer also depends on proper timing. A delayed or poorly sequenced movement in one part of the kinetic chain can disrupt the entire motion, requiring the shoulder to work harder to compensate. This is why strength and conditioning programs for pitchers emphasize the entire kinetic chain rather than isolating the shoulder muscles alone.
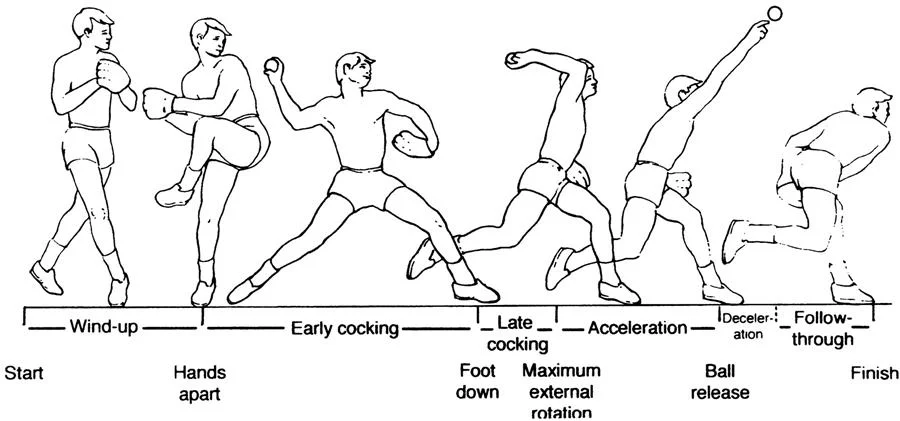
Key Phases of the Throwing Motion
The throwing motion is divided into distinct phases, each with unique biomechanical demands on the shoulder:
Follow-Through Phase
The final phase involves the body absorbing the residual forces from the throw. The shoulder, scapula, and lower body must work together to dissipate energy effectively. Failure to execute this phase properly can lead to residual strain on the shoulder and elbow.
Wind-Up Phase
This initial phase involves the pitcher’s preparation to throw. The body shifts weight to the back leg while the hands come together, creating potential energy. This phase is relatively low in stress but sets the foundation for the rest of the motion.
Stride Phase
As the pitcher strides forward, the kinetic chain is activated. The lower body generates rotational torque through the hips and trunk, which is essential for building momentum. During this phase, the throwing arm begins to move into external rotation.
Cocking Phase
The cocking phase marks the transition from stride to acceleration. The arm reaches maximum external rotation as the pitcher prepares to release the ball. This is the most vulnerable phase for the shoulder, as the rotator cuff must stabilize the humeral head in the glenoid while resisting extreme forces. Weakness or instability in this phase can lead to injuries such as labral tears or rotator cuff damage.
Acceleration Phase
During acceleration, the arm rapidly moves from external to internal rotation. The pectoralis major, latissimus dorsi, and subscapularis muscles generate the force needed to propel the ball forward. The rotator cuff works eccentrically to maintain joint stability. This is the most explosive phase, with high angular velocities and significant stress on the shoulder structures.
Release Phase
At the moment the ball leaves the hand, the arm is at maximum speed. The shoulder and elbow experience peak forces, and the wrist helps guide the ball for accuracy. Proper mechanics during this phase are essential to prevent overloading the shoulder.
Deceleration Phase
After the ball is released, the arm slows down rapidly, with the posterior shoulder muscles, including the infraspinatus and teres minor, working eccentrically to decelerate the motion. This phase is critical for protecting the shoulder from injury, as improper deceleration can lead to rotator cuff overuse or posterior shoulder pain.
The Pitcher’s Paradox
Definition and Biomechanics
The “Pitcher’s Paradox” describes the intricate balance between achieving optimal throwing performance and maintaining the long-term health of the shoulder joint. This paradox emerges because the very mechanics that enable a pitcher to throw with exceptional velocity and precision also expose the shoulder to significant biomechanical stress and potential injury.
Throwing involves a complex interplay of movements, particularly external and internal rotation of the shoulder. During the pitching motion, the arm must reach extreme levels of external rotation in the cocking phase, followed by rapid internal rotation during the acceleration phase. This sequence generates tremendous angular velocity, often exceeding 7,000 degrees per second. The shoulder’s ability to handle such extreme movements depends on the precise coordination of the rotator cuff muscles, scapular stabilizers, and the kinetic chain.
The paradox lies in the need for both mobility and stability in the shoulder joint:
- Mobility: To achieve the range of motion required for high-velocity throws, the shoulder must allow excessive external rotation. This often leads to adaptations, such as increased joint laxity or posterior capsule tightness.
- Stability: Despite this mobility, the shoulder must remain stable to prevent injuries like subluxations, labral tears, or rotator cuff damage. Stability relies on the dynamic support provided by the rotator cuff muscles and surrounding soft tissues.
Biomechanically, the glenohumeral joint is uniquely suited for this dual role. Its ball-and-socket structure permits a wide range of motion but inherently lacks bony stability. As a result, the shoulder depends heavily on soft tissue structures—such as the rotator cuff, labrum, and scapular stabilizers—to maintain alignment and function during the intense forces of throwing. Any disruption in this balance increases the risk of injury and highlights the core challenge of the Pitcher’s Paradox.
Challenges in Balancing Performance and Joint Health
Balancing high performance with joint health in pitchers is a significant challenge, as the demands of the sport push the shoulder to its limits. Below are key challenges pitchers face and strategies used to mitigate these risks:
- Repetitive Stress and Overuse
Pitchers repeatedly subject their shoulders to high levels of stress, particularly during competitive seasons. Over time, repetitive microtrauma can lead to rotator cuff tendinitis, labral tears, or degenerative changes in the shoulder joint. The volume and intensity of pitching must be carefully managed to avoid overuse injuries.- Prevention Tip: Implement strict pitch count limits and ensure adequate rest between games. Younger athletes, in particular, benefit from guidelines designed to reduce overuse injuries.
- Asymmetrical Shoulder Adaptations
The repetitive motion of throwing often leads to structural changes in the shoulder, such as increased external rotation (external rotation gain) and decreased internal rotation (glenohumeral internal rotation deficit, or GIRD). While these adaptations can enhance throwing velocity, they also predispose pitchers to injuries like internal impingement or labral tears.- Prevention Tip: Regular assessment of range of motion and targeted stretching exercises can help address imbalances and reduce the risk of injury.
- Weakness in the Kinetic Chain
Pitching relies on efficient energy transfer from the lower body through the core to the shoulder and arm. Weakness or dysfunction in any part of this kinetic chain places increased stress on the shoulder, as it compensates for the loss of power or stability elsewhere.- Prevention Tip: Incorporate whole-body conditioning programs that strengthen the legs, hips, core, and scapular stabilizers. This holistic approach ensures efficient energy transfer and reduces strain on the shoulder.
- Deceleration and Eccentric Control
The deceleration phase of throwing places significant demands on the posterior shoulder muscles, particularly the infraspinatus and teres minor. These muscles must work eccentrically to slow down the arm after ball release. Insufficient eccentric strength or endurance can lead to posterior shoulder pain and fatigue.- Prevention Tip: Include eccentric strengthening exercises, such as resisted shoulder rotations and reverse flys, to improve posterior shoulder endurance.
- Fatigue and Poor Mechanics
Fatigue is a major risk factor for injury. As pitchers tire, their mechanics often deteriorate, leading to compensatory movements that increase stress on the shoulder. This is particularly evident in younger or less conditioned athletes.- Prevention Tip: Monitor signs of fatigue, such as decreased velocity or control, and emphasize recovery. Educating athletes on proper mechanics can also reduce compensatory movements and their associated risks.
- Balancing Velocity and Longevity
The modern emphasis on high-velocity pitching has increased injury rates among athletes. While velocity is a critical component of performance, it often comes at the expense of long-term joint health.- Prevention Tip: Encourage athletes to focus on both velocity and command. Balanced training programs that incorporate rest, mobility, and stability work are essential for sustaining a long career.
- Inadequate Recovery and Rehabilitation
Recovery is as important as performance, yet many athletes and teams overlook its role in preventing injuries. Insufficient recovery time between games or inadequate rehabilitation after minor injuries can lead to chronic shoulder problems.- Prevention Tip: Establish comprehensive recovery protocols, including rest, soft tissue mobilization, and therapeutic exercises. Addressing minor issues early can prevent them from developing into major injuries.
Common Shoulder Injuries in Pitchers
Baseball pitchers are particularly susceptible to shoulder injuries due to the repetitive and high-intensity nature of the throwing motion. These injuries often result from the extreme demands placed on the shoulder joint, which must balance mobility and stability under immense stress. Below are the most common shoulder injuries in pitchers, along with their causes, symptoms, and management strategies.
Rotator Cuff Tears
The rotator cuff is a group of four muscles and their tendons—supraspinatus, infraspinatus, teres minor, and subscapularis—that stabilize the shoulder joint and allow for a wide range of motion. In pitchers, rotator cuff tears often result from overuse, repetitive microtrauma, or acute injury.
- Causes:
- Excessive external rotation during the cocking phase.
- High eccentric forces during deceleration.
- Fatigue or muscular imbalances in the rotator cuff.
- Symptoms:
- Persistent shoulder pain, particularly during or after throwing.
- Weakness in overhead movements.
- Difficulty lifting the arm or performing daily activities.
- Management:
- Rest and activity modification to reduce stress on the shoulder.
- Physical therapy focused on strengthening the rotator cuff and scapular stabilizers.
- Severe or full-thickness tears may require surgical intervention, such as arthroscopic repair.
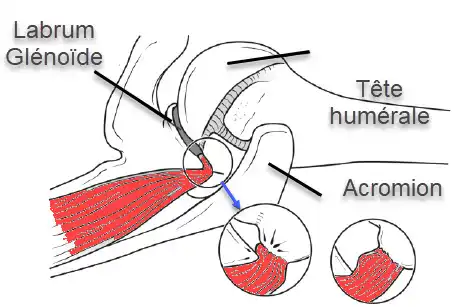
Labrum Injuries
The labrum is a ring of cartilage that surrounds the glenoid cavity, enhancing the stability of the shoulder joint by deepening the socket. In pitchers, labral injuries—particularly SLAP (Superior Labrum Anterior and Posterior) tears—are common due to the repetitive overhead motion of throwing.
- Causes:
- Shearing forces during the cocking and acceleration phases.
- Excessive strain on the biceps tendon, which attaches to the labrum.
- Instability or improper mechanics that increase joint stress.
- Symptoms:
- Deep, dull pain in the shoulder, especially during throwing.
- Clicking, catching, or locking sensations in the joint.
- Reduced throwing velocity or control.
- Management:
- Rest and anti-inflammatory treatments to reduce pain and swelling.
- Rehabilitation exercises targeting scapular mechanics and rotator cuff strength.
- For significant tears, arthroscopic surgery may be needed to repair or remove damaged tissue.
Tendinopathies
Tendinopathy refers to the inflammation, degeneration, or microtearing of tendons, often due to overuse. In pitchers, rotator cuff tendinopathy and biceps tendinopathy are the most common forms.
- Causes:
- Repetitive overhead throwing leading to cumulative stress on tendons.
- Poor biomechanics or muscle imbalances in the shoulder and scapula.
- Insufficient recovery time between games or training sessions.
- Symptoms:
- Aching pain in the shoulder or along the front of the arm.
- Pain that worsens with throwing or lifting activities.
- Stiffness and reduced range of motion, especially after periods of rest.
- Management:
- Rest and icing to reduce inflammation.
- Eccentric strengthening exercises to promote tendon healing.
- Corticosteroid injections or platelet-rich plasma (PRP) therapy in severe cases.
Shoulder Instability
Shoulder instability occurs when the humeral head fails to remain centered in the glenoid socket during movement. This is often seen in pitchers due to the repetitive forces exerted on the joint, which can stretch or damage stabilizing structures like the capsule, labrum, or ligaments.
- Causes:
- Increased joint laxity from repetitive external rotation.
- Weakness or fatigue of the rotator cuff and scapular muscles.
- Poor posture or altered throwing mechanics.
- Symptoms:
- Sensation of the shoulder “slipping” or “giving out.”
- Pain or discomfort during specific phases of throwing.
- Reduced throwing velocity or accuracy.
- Management:
- Strengthening exercises focused on dynamic stabilizers, such as the rotator cuff and scapular muscles.
- Avoidance of activities that exacerbate symptoms.
- Severe cases may require surgical stabilization, such as capsular tightening or labral repair.
Preventing Shoulder Injuries
While these injuries are common in pitchers, they can often be prevented with proper care and training:
- Biomechanical Analysis: Assess throwing mechanics regularly to identify and correct inefficiencies.
- Conditioning Programs: Focus on strengthening the entire kinetic chain, including the legs, core, scapula, and rotator cuff.
- Rest and Recovery: Adhere to pitch count limits and incorporate sufficient rest days to prevent overuse injuries.
- Prehabilitation: Perform preventative exercises, such as scapular stabilization drills and rotator cuff strengthening.
By addressing these factors, pitchers can significantly reduce their risk of developing shoulder injuries while improving their performance on the mound.
Symptoms and Stages of Shoulder Injuries in Pitchers
Understanding the progression of shoulder injuries in pitchers is crucial for early detection and effective management. These injuries typically evolve through identifiable stages, each with distinct symptoms and warning signs. Below is an overview of the two main stages and associated symptoms commonly observed in pitchers experiencing shoulder issues.
Stage I: Painful Shoulder Syndrome
In the initial stage, referred to as Painful Shoulder Syndrome, symptoms are often mild and occur intermittently. These early warning signs may be overlooked or dismissed as typical post-game soreness, but recognizing them is critical to prevent progression to more severe stages.
- Symptoms:
- Deep, dull pain localized in the anterior or posterior shoulder during or after throwing.
- Discomfort when performing specific pitches, such as sliders or curveballs.
- Reduced throwing velocity or accuracy.
- Mild stiffness or tightness, especially after extended periods of rest.
- Key Characteristics:
- Pain typically subsides with rest and may not initially interfere with daily activities.
- Athletes can often continue throwing but may notice a decrease in performance.
- Swelling oraround the shoulder joint may be present.
- Warning Signs:
- Persistent discomfort after games or training sessions.
- Difficulty recovering between games, even with rest and icing.
- Subtle changes in throwing mechanics as the body compensates for pain.
Stage II: Deep Pathological Pain
If untreated, Painful Shoulder Syndrome can progress to Deep Pathological Pain, characterized by more significant structural damage and chronic symptoms. At this stage, the injury often begins to interfere with both athletic performance and daily life.
- Symptoms:
- Difficulty sleeping on the affected side due to nighttime pain.
- Pain that no
- Key Characteristics:
- The shoulder feels weak and unstable, often described as “giving out” during motion.
- Throwing becomes increasingly difficult or impossible, with a noticeable decline in step speed and accuracy.
- Pain may radiate to surrounding areas, such as the upper arm or scapular region.
- Warning Signs:
- Athletes may require stronger pain management, such as prescription medications or corticosteroid injections.
- Persistent swelling and a sensation of grinding or catching in the shoulder joint.
- Altered mechanics or compensatory movements leading to additional stress on other joints, such as the elbow.
Associated Symptoms and Warning Signs
In both stages, additional symptoms and warning signs may indicate a worsening condition or the presence of secondary complications:
- Loss of Shoulder Function:
- Difficulty lifting the arm overhead or behind the back.
- Weakness when performing simple tasks, such as carrying objects or pushing open doors.
- Postural Changes:
- Poor posture, including rounded shoulders or scapular winging, due to muscular imbalances.
- Visible asymmetry in shoulder height or scapular positioning.
- Compensatory Pain:
- Pain or discomfort in adjacent areas, such as the neck, upper back, or opposite shoulder.
- Increased stress on the elbow or wrist due to altered throwing mechanics.
- Behavioral Changes:
- Hesitancy or fear of throwing at full velocity.
- Avoidance of certain pitches or changes in playing habits to reduce discomfort.
- Fatigue and Inflammation:
- Generalized shoulder fatigue, especially during late innings or after prolonged games.
- Persistent swelling or localized tenderness around the glenohumeral joint.
Importance of Early Intervention
Recognizing and addressing symptoms in the early stages can prevent further damage and shorten recovery time. Key steps include:
- Stage I: Rest, icing, and targeted physical therapy to reduce inflammation and restore strength.
- Stage II: Advanced diagnostic imaging, such as MRI or ultrasound, may be needed to assess structural damage, followed by a comprehensive rehabilitation program. Surgery may be required for severe cases.
By understanding these stages and associated symptoms, athletes, coaches, and healthcare professionals can take proactive steps to manage shoulder injuries, ensuring a safer and more effective return to sport.
Symptoms and Stages of Shoulder Injuries in Pitchers
Understanding the progression of shoulder injuries in pitchers is crucial for early detection and effective management. These injuries typically evolve through identifiable stages, each with distinct symptoms and warning signs. Below is an overview of the two main stages and associated symptom
Stage II: Deep Pathological Pain
If untreated, Painful Shoulder Syndrome can progress to Deep Pathological Pain, characterized by more significant structural damage and chronic symptoms. At this stage, the injury often begins to interfere with both athletic performance and daily life.
- Symptoms:
- Persistent, deep pain in the posterior shoulder that worsens with activity.
- Limited range of motion, particularly in abduction and external rotation.
- Difficulty sleeping on the affected side due to nighttime pain.
- Pain that no longer responds effectively to rest or over-the-counter pain relief.
- Key Characteristics:
- The shoulder feels weak and unstable, often described as “giving out” during motion.
- Throwing becomes increasingly difficult or impossible, with a noticeable decline in step speed and accuracy.
- Pain may radiate to surrounding areas, such as the upper arm or scapular region.
- Warning Signs:
- Athletes may require stronger pain management, such as prescription medications or corticosteroid injections.
- Persistent swelling and a sensation of grinding or catching in the shoulder joint.
- Altered mechanics or compensatory movements leading to additional stress on other joints, such as the elbow.
Associated Symptoms and Warning Signs
In both stages, additional symptoms and warning signs may indicate a worsening condition or the presence of secondary complications:
- Loss of Shoulder Function:
- Difficulty lifting the arm overhead or behind the back.
- Weakness when performing simple tasks, such as carrying objects or pushing open doors.
- Postural Changes:
- Poor posture, including rounded shoulders or scapular winging, due to muscular imbalances.
- Visible asymmetry in shoulder height or scapular positioning.
- Compensatory Pain:
- Pain or discomfort in adjacent areas, such as the neck, upper back, or opposite shoulder.
- Increased stress on the elbow or wrist due to altered throwing mechanics.
- Behavioral Changes:
- Hesitancy or fear of throwing at full velocity.
- Avoidance of certain pitches or changes in playing habits to reduce discomfort.
- Fatigue and Inflammation:
- Generalized shoulder fatigue, especially during late innings or after prolonged games.
- Persistent swelling or localized tenderness around the glenohumeral joint.
Importance of Early Intervention
Recognizing and addressing symptoms in the early stages can prevent further damage and shorten recovery time. Key steps include:
- Stage I: Rest, icing, and targeted physical therapy to reduce inflammation and restore strength.
- Stage II: Advanced diagnostic imaging, such as MRI or ultrasound, may be needed to assess structural damage, followed by a comprehensive rehabilitation program. Surgery may be required for severe cases.
By understanding these stages and associated symptoms, athletes, coaches, and healthcare professionals can take proactive steps to manage shoulder injuries, ensuring a safer and more effective return to sport.
Diagnosis and Differential Diagnosis
Identifying and differentiating rotator cuff tendinitis from other conditions with overlapping symptoms is essential for accurate treatment. Below is an outline of diagnostic criteria for rotator cuff tendinitis and the conditions with similar presentations, including their key features.
Diagnostic Criteria for Rotator Cuff Tendinitis
Rotator cuff tendinitis is primarily diagnosed based on clinical evaluation, including a detailed history and physical examination. Imaging studies are used when necessary to confirm the diagnosis or rule out other conditions.
- Key Diagnostic Features:
- Patient History:
- Complaints of pain localized to the shoulder, particularly around the anterior or lateral aspects.
- Symptoms worsen with overhead activities or repetitive motions.
- Pain may radiate down the upper arm but rarely past the elbow.
- Physical Examination:
- Painful Arc Test: Pain during shoulder abduction, typically between 60–120 degrees.
- Hawkins-Kennedy Test: Pain induced by passive internal rotation of the shoulder.
- Neer Test: Pain when the shoulder is passively flexed while internally rotated.
- Weakness or pain during resisted external rotation (indicative of supraspinatus or infraspinatus involvement).
- Imaging Studies:
- X-rays: May reveal calcific tendinitis or acromial impingement.
- Ultrasound: Effective for identifying tendon thickening, tears, or fluid accumulation.
- MRI: Used for detailed visualization of the rotator cuff, particularly in chronic or severe cases.
- Patient History:
- Red Flags:
Symptoms that do not improve with rest or conservative management may indicate a more severe condition, such as a tear or nerve involvement.
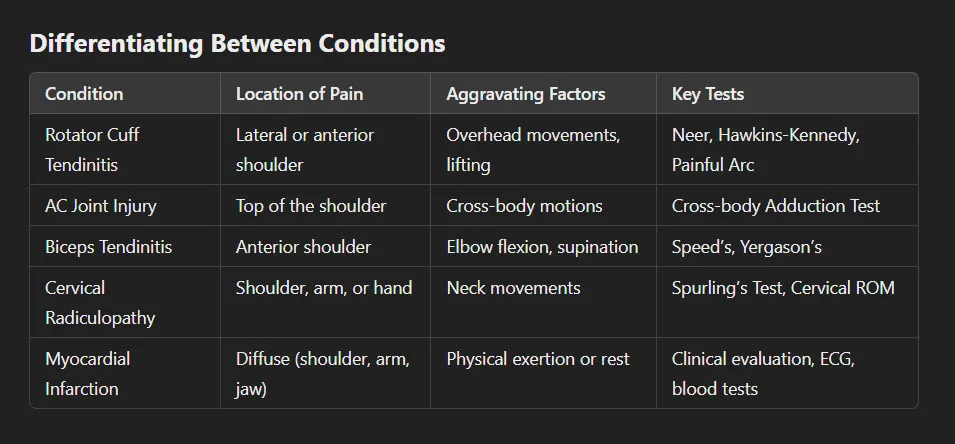
Conditions with Similar Symptoms
Several conditions can mimic the symptoms of rotator cuff tendinitis, requiring careful differential diagnosis.
1. Acromioclavicular (AC) Joint Injury
- Overview: Injuries to the AC joint, such as sprains or separations, occur from direct trauma or repetitive strain.
- Symptoms:
- Localized pain and tenderness over the AC joint.
- Pain exacerbated by cross-body movements (e.g., horizontal adduction).
- Visible deformity or swelling in more severe cases.
- Key Differentiator: Pain is localized to the top of the shoulder, distinct from the lateral or anterior shoulder pain typical of rotator cuff tendinitis.
2. Biceps Tendinitis
- Overview: Inflammation of the long head of the biceps tendon, often coexisting with rotator cuff pathology.
- Symptoms:
- Anterior shoulder pain, especially along the bicipital groove.
- Pain worsens with resisted elbow flexion or forearm supination.
- Clicking or popping sensation during shoulder movements.
- Key Differentiator: Positive results on Speed’s Test (pain during resisted shoulder flexion) and Yergason’s Test (pain with resisted supination of the forearm).
3. Cervical Radiculopathy
- Overview: Nerve root compression in the cervical spine can cause referred pain to the shoulder and arm.
- Symptoms:
- Radiating pain from the neck into the shoulder, arm, or hand.
- Numbness, tingling, or weakness in the affected arm.
- Symptoms worsen with neck movements, such as extension or lateral rotation.
- Key Differentiator: Positive Spurling’s Test (pain radiating to the arm with cervical spine compression) and absence of pain during shoulder-specific maneuvers.
4. Myocardial Infarction (Heart Attack)
- Overview: While uncommon, shoulder pain can occasionally be a presenting symptom of a myocardial infarction, particularly in women or older adults.
- Symptoms:
- Diffuse, poorly localized shoulder pain that may extend to the jaw, back, or arm.
- Associated symptoms such as chest pain, shortness of breath, nausea, o
- r sweating.
- Key Differentiator: Presence of systemic symptoms and risk factors (e.g., age, smoking, diabetes). Immediate medical attention is required for suspected cases.
Osteopathic Approach to Treatment
- The osteopathic approach to treating shoulder injuries, such as rotator cuff tendinitis, emphasizes holistic care to restore function, relieve pain, and promote healing. Treatment is designed to address the root cause of the issue, often focusing on biomechanical imbalances, muscular dysfunction, and tissue inflammation. Below, we explore four key components of osteopathic treatment: rest and inflammation management, myofascial release techniques, glenohumeral joint mobilization, and strengthening and rehabilitation exercises.
1. Rest and Inflammation Management
The initial phase of treatment aims to reduce pain and inflammation in the affected shoulder while minimizing further stress on the injured tissues.
Rest:
Relative rest is recommended to prevent aggravating the injury while maintaining gentle movement to avoid stiffness or muscle atrophy. Complete immobilization is generally avoided unless the pain is severe.
Activities involving repetitive overhead motions or heavy lifting should be temporarily halted.
Inflammation Control:
Cold Therapy: Applying cold compresses to the shoulder for 15–20 minutes several times daily can reduce acute inflammation and alleviate pain.
Anti-inflammatory Measures: Natural anti-inflammatory strategies, such as omega-3-rich diets, and prescribed NSAIDs may also be considered.
Postural Support:
Poor posture can exacerbate shoulder pain. Osteopaths often recommend ergonomic adjustments, such as proper desk and seating positions, to support recovery.
2. Myofascial Release Techniques
Myofascial release focuses on alleviating restrictions in the connective tissue that may contribute to pain and dysfunction in the shoulder.
Targeted Muscles:
Techniques focus on releasing tension in the supraspinatus, infraspinatus, subscapularis, and teres minor, as well as surrounding structures such as the trapezius and levator scapulae.
These muscles are often tense or knotted due to overuse or compensatory strain.
Techniques Used:
Direct Myofascial Release: The osteopath applies sustained pressure to areas of restriction, gradually lengthening the fascia to improve tissue mobility.
Indirect Myofascial Release: Gentle pressure is applied in the direction of least resistance, allowing the tissue to naturally release tension.
Instrument-Assisted Myofascial Release: Tools, such as Graston instruments, may be used to enhance release techniques, especially for chronic cases.
Benefits:
Reduces muscular tension that exacerbates inflammation and restricts movement.
Enhances blood flow and lymphatic drainage to promote healing.
3. Glenohumeral Joint Mobilization
Joint mobilization is a cornerstone of osteopathic treatment, aiming to restore proper alignment and movement to the shoulder joint. The glenohumeral joint’s complex biomechanics make it particularly vulnerable to dysfunction, and mobilization helps address these issues.
Techniques:
Grade I and II Mobilizations: Gentle oscillatory movements are applied to reduce pain and improve joint lubrication, often used in the acute phase.
Grade III and IV Mobilizations: Larger, more sustained movements are used to increase the range of motion and address joint stiffness.
Traction: Gentle pulling of the humeral head creates space in the joint, relieving pressure on inflamed structures like the rotator cuff tendons and bursa.
Goals:
Improve the mechanics of the glenohumeral joint, reducing impingement on the rotator cuff.
Restore a functional scapulohumeral rhythm, essential for coordinated shoulder movement.
Complementary Techniques: Mobilization is often combined with stretching to address tight posterior capsules, which can contribute to internal impingement and limited internal rotation.
4. Strengthening and Rehabilitation Exercises
Strengthening and rehabilitation exercises play a critical role in restoring shoulder function, preventing recurrence, and enhancing overall stability.
Early Phase Exercises:
Focus on isometric contractions of the rotator cuff muscles to build strength without exacerbating pain.
Gentle range-of-motion exercises, such as pendulum swings or wall crawls, help maintain flexibility.
Progressive Strengthening:
Rotator Cuff: Resistance bands or light weights are used to strengthen key muscles, including the supraspinatus, infraspinatus, subscapularis, and teres minor.
Scapular Stabilizers: Exercises such as scapular retractions, serratus punches, and prone YTWs focus on muscles like the rhomboids, trapezius, and serratus anterior.
Core and Lower Body: Addressing the kinetic chain by strengthening the core and legs ensures proper energy transfer during throwing or lifting activities.
Functional Training:
Exercises mimic real-life movements to prepare the shoulder for daily activities or sports. For pitchers, this may include controlled throwing drills to restore proper mechanics gradually.
Plyometric exercises, such as medicine ball throws, can help improve dynamic stability in advanced stages of rehabilitation.
Stretching:
Stretching the posterior shoulder capsule, pectoralis minor, and latissimus dorsi is essential to maintain flexibility and prevent compensatory tightness.
Prevention Strategies for Shoulder Injuries in Pitchers
Preventing shoulder injuries in pitchers requires a proactive, holistic approach that emphasizes proper mechanics, conditioning, and regular monitoring. Below, we explore three critical prevention strategies: optimizing throwing mechanics, strengthening the kinetic chain, and implementing regular assessment and conditioning.
1. Optimizing Throwing Mechanics
Proper throwing mechanics are essential to minimize unnecessary stress on the shoulder and reduce the risk of injury. Poor technique or compensatory movements can lead to overloading specific structures, such as the rotator cuff and labrum.
- Key Components of Proper Mechanics:
- Balanced Stance and Stride: A stable stance and controlled stride ensure that the kinetic chain operates efficiently, preventing undue strain on the shoulder.
- Smooth Arm Path: The arm should follow a consistent, efficient path, avoiding excessive “high elbows” or sidearm motions that increase stress on the shoulder.
- Hip-Shoulder Separation: Proper timing between the rotation of the hips and shoulders generates maximum force with minimal effort, reducing shoulder strain.
- Training Recommendations:
- Video Analysis: Using slow-motion video to analyze throwing mechanics helps identify inefficiencies or compensatory movements.
- Throwing Progressions: Gradually increase throwing intensity, focusing on form before power. Start with shorter distances and progress to longer throws.
- Coaching and Feedback: Work with experienced coaches or sports medicine professionals to ensure optimal technique and correct improper habits early.
2. Strengthening the Kinetic Chain
The throwing motion relies on the entire kinetic chain, from the legs to the core to the shoulder. Weakness or dysfunction in any part of the chain can increase stress on the shoulder as it compensates for inefficiencies.
- Lower Body Strength:
- The legs and hips generate the majority of the force in the throwing motion. Strong quadriceps, hamstrings, glutes, and hip rotators are essential for stability and power.
- Recommended Exercises: Squats, lunges, step-ups, and resisted hip rotations.
- Core Stability:
- A stable core ensures efficient energy transfer from the lower body to the upper body. Weakness in the core can lead to overcompensation in the shoulder.
- Recommended Exercises: Planks, Russian twists, medicine ball throws, and anti-rotation presses.
- Scapular Stabilization:
- The scapula provides a stable base for the shoulder. Dysfunctional scapular mechanics (e.g., winging or tilting) increase the risk of rotator cuff strain.
- Recommended Exercises: Scapular retractions, serratus punches, wall slides, and prone YTWs.
- Rotator Cuff Strengthening:
- Strengthening the rotator cuff muscles ensures they can stabilize the humeral head during extreme movements.
- Recommended Exercises: Resistance band external and internal rotations, side-lying external rotations, and prone horizontal abduction.
3. Regular Assessment and Conditioning
Consistent monitoring and conditioning are crucial for identifying potential issues early and maintaining optimal performance.
- Pre-Season Screening:
- Conduct a thorough musculoskeletal assessment before the season begins. Look for areas of tightness, weakness, or asymmetry that could predispose the athlete to injury.
- Assess range of motion, particularly external and internal rotation, and check for signs of glenohumeral internal rotation deficit (GIRD).
- Pitch Count Monitoring:
- Adhere to recommended pitch counts and ensure adequate rest between outings. Overuse is a significant contributor to shoulder injuries, especially in younger athletes.
- In-Season Conditioning:
- Maintain a regular strength and conditioning routine throughout the season. Focus on recovery exercises, such as light stretching and foam rolling, after games.
- Gradually adjust intensity levels to avoid early-season fatigue or late-season burnout.
- Postural Assessments:
- Poor posture, such as rounded shoulders or forward head positioning, can alter throwing mechanics and increase injury risk. Regularly assess posture and address imbalances with targeted exercises.
- Recovery Protocols:
- Include adequate rest, sleep, and nutrition in the athlete’s routine. Recovery is essential for repairing tissue microtrauma caused by repetitive throwing.
- Utilize active recovery techniques, such as swimming or low-impact cardio, to maintain mobility and endurance.
- Strength Maintenance:
- Prevent strength imbalances by focusing on bilateral and unilateral exercises for both the dominant and non-dominant sides.
Conclusion
Summary of Key Points
Shoulder injuries in pitchers, such as rotator cuff tendinitis, labral tears, and shoulder instability, are common due to the repetitive and high-stress nature of the throwing motion. Proper diagnosis and management require a thorough understanding of the mechanics of throwing and the interconnected structures of the shoulder.
- Key Prevention Strategies: Optimizing throwing mechanics, strengthening the kinetic chain, and regular assessments are crucial for reducing the risk of injury and ensuring long-term shoulder health.
- Effective Treatment Approaches: Rest, inflammation management, myofascial release, joint mobilization, and progressive strengthening exercises play a pivotal role in recovery. Addressing both acute symptoms and underlying biomechanical dysfunctions ensures a holistic approach to care.
- Understanding Injury Stages: Recognizing the early symptoms of shoulder pain (Stage I: Painful Shoulder Syndrome) allows for timely interventions to prevent progression to more severe conditions (Stage II: Deep Pathological Pain).
Importance of Early Intervention and Holistic Care
Early intervention is critical to minimizing the impact of shoulder injuries and ensuring optimal recovery. Ignoring early symptoms or delaying treatment can lead to chronic pain, long-term dysfunction, and even career-ending conditions. A proactive approach includes:
- Identifying subtle changes in performance, pain, or range of motion.
- Implementing tailored rehabilitation programs to restore strength, mobility, and joint stability.
- Addressing the entire kinetic chain to optimize energy transfer and reduce compensatory strain on the shoulder.
The holistic nature of osteopathic care integrates physical, functional, and lifestyle factors to achieve sustainable outcomes. By focusing on prevention, early diagnosis, and comprehensive treatment, pitchers can maintain peak performance, extend their careers, and protect their long-term health.
Reference
- Wilk et al. Shoulder Injuries in the Overhead Athlet




















{kind=link}