
")
Introduction
The scapulohumeral rhythm is a key element in shoulder biomechanics. It describes the coordinated relationship between the shoulder blade (scapula) and the humerus, particularly during arm elevation. This phenomenon plays a critical role in maintaining shoulder stability, muscle strength, and range of motion. Simply put, for every two degrees of movement of the humerus in the glenohumeral joint, the scapula moves approximately one degree. This 2:1 ratio is crucial for proper shoulder function, particularly in movements such as abduction or flexion of the arm.
This concept was first studied by Inman, Saunders, and Abbott using radiography, and their research laid the foundation for today’s understanding of shoulder motion. These studies showed that the scapula plays an active role in the motion of the humerus, contrary to the initial belief that the scapula remained stationary during shoulder movements. Since then, this ratio has been widely accepted as a key indicator of normal shoulder function.
The scapulohumeral rhythm allows the glenoid fossa to remain properly positioned to accommodate the humeral head throughout the range of motion. By maintaining this stability, it also preserves the length-tension relationships of the glenohumeral muscles, allowing these muscles to produce force over a greater range of motion. Without this coordinated movement, the humeral head would dislodge from the glenoid fossa, leading to joint and muscle dysfunction.
Proper functioning of the scapulohumeral rhythm is essential to prevent injuries, especially in athletes who place a lot of strain on their shoulders. Repetitive movements, such as those seen in sports such as tennis, swimming or baseball, can cause imbalances in this rhythm, leading to pain and injury. This is why understanding and evaluating this mechanism is crucial for health professionals, especially in the field of osteopathy, where the goal is to restore harmony of movement and function.
With this in mind, it is essential to explore not only the normal functioning of the scapulohumeral rhythm, but also the potential causes of an imbalance, as well as the available assessment and treatment methods. This blog post will therefore delve into the different facets of this complex shoulder dynamic, providing insights into its movement phases, its functional importance, and the interventions required in case of dysfunction.
Mechanics of Scapulo-Humeral Rhythm
Coordinated movement between the humerus and scapula is fundamental to ensuring smooth and pain-free shoulder function. The mechanics of this movement, called scapulohumeral rhythm, are key to joint mobility and stability. Each joint and muscle group in the shoulder works in harmony to allow full range of motion of the arm. In particular, the glenohumeral joint and the scapulothoracic joint play a central role in this coordination.
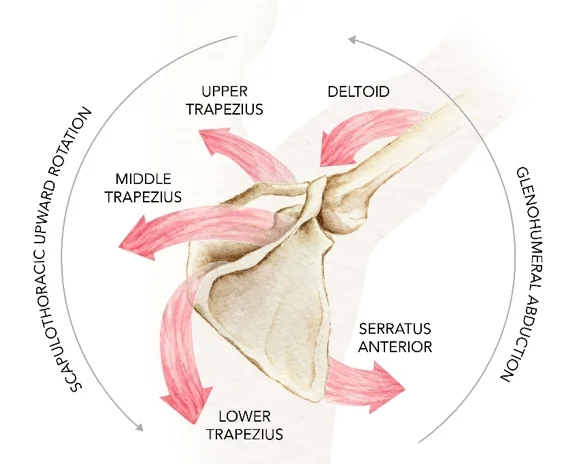
The movement of the humerus in the glenohumeral joint is a large part of arm elevation. However, as the arm continues to elevate, the scapula intervenes by rotating upward, a process called upward rotation of the scapula. This rotation is provided primarily by the upper and lower trapezius muscles as well as the serratus anterior muscle. Together, these muscles coordinate the movement to maintain the scapula in optimal position relative to the humerus, thus ensuring unrestricted motion.
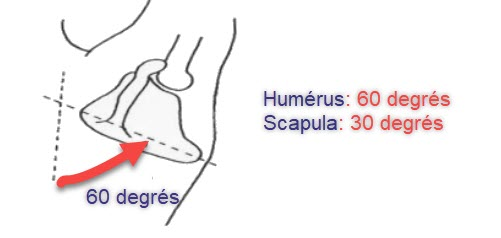
The 2:1 ratio of humerus to scapula movement means that the humerus moves twice as much as the scapula during arm elevation. Thus, of the 180° of full arm elevation, approximately 120° occurs in the glenohumeral joint, while the remaining 60° comes from scapula rotation. This ratio helps distribute the load across the different structures of the shoulder, reducing stress on the muscles, tendons, and ligaments surrounding the joint.
When the scapulohumeral rhythm is disrupted, it can lead to mobility issues or shoulder pain. For example, insufficient rotation of the scapula can cause the rotator cuff tendons to compress against the acromion, a problem commonly referred to as subacromial impingement. Additionally, overuse of the glenohumeral joint without adequate involvement of the scapula can cause premature wear of the joint structures, leading to osteoarthritis.
It is important to note that shoulder movement is not limited to simple arm elevation. Complex movements such as external and internal rotation, as well as combination movements, also require synchronization between the humerus and scapula. The ability of the scapula to adapt and move in relation to the humerus is essential to avoid muscle imbalances and injuries.
Thus, the mechanics of the scapulohumeral rhythm are not only about mobility, but also about joint stability. A good balance between mobility and stability allows athletes and active individuals to maintain optimal shoulder function, while preventing injuries related to excessive or incorrect use of the shoulder muscles. In osteopathy, the assessment of these mechanics is crucial to identify imbalances and plan appropriate management.
Muscle Coordination in Scapulothoracic and Glenohumeral Movement
The intricate coordination between the scapulothoracic and glenohumeral joints is essential for proper shoulder function. During arm elevation, key muscles work synergistically to ensure smooth and stable motion while maintaining the alignment of the humeral head within the glenoid fossa. This coordination minimizes stress on the shoulder structures and prevents injuries.
The upper trapezius, middle trapezius, and lower trapezius play distinct yet complementary roles in scapular movement. The upper trapezius initiates upward rotation of the scapula and helps elevate it during the early phases of arm elevation. The middle trapezius stabilizes the scapula against the thoracic wall, ensuring that it does not wing outward. The lower trapezius contributes to the final phases of upward rotation, particularly as the arm approaches full elevation.
The serratus anterior is another crucial muscle in scapular mechanics. It works to protract the scapula, moving it around the rib cage, while also assisting with upward rotation. This movement is vital to maintain the scapula’s optimal position relative to the humerus during elevation, reducing the risk of impingement or instability. Weakness in the serratus anterior often results in conditions such as scapular winging, which disrupts the balance of scapulothoracic motion.
The deltoid is the primary mover of the humerus during arm elevation. As it lifts the arm, it generates significant force. However, without the stabilizing actions of the scapular muscles, the deltoid’s force could push the humeral head upward against the acromion, leading to subacromial impingement. The coordinated activity of the trapezius and serratus anterior ensures the scapula rotates upward and outward, creating sufficient space for the humerus to move freely.
The combined efforts of these muscles adhere to the classic 2:1 scapulohumeral rhythm. For every 2 degrees of motion at the glenohumeral joint, there is approximately 1 degree of motion at the scapulothoracic joint. This distribution of movement helps to spread mechanical loads across the shoulder complex, reducing stress on individual structures and enhancing the efficiency of motion.
Disruptions in this muscle coordination can lead to significant shoulder dysfunctions. Insufficient activation of the trapezius or serratus anterior can result in incomplete scapular rotation, while overactivation of the upper trapezius may cause excessive elevation and muscle imbalances. These issues often manifest as shoulder pain, reduced range of motion, and pathologies such as rotator cuff injuries.
Effective rehabilitation involves targeting these key muscles with strengthening and stabilization exercises. Ensuring proper coordination between the deltoid, trapezius, and serratus anterior is critical for restoring optimal scapulothoracic and glenohumeral motion, preserving shoulder health, and preventing future injuries.
Phases of Movement
The complete elevation of the arm in abduction or flexion is broken down into three distinct phases, each characterized by a specific coordination between the humerus and the scapula. These phases are crucial to understanding the functioning of the scapulohumeral rhythm and the possible disturbances that can occur.
Phase 1: Initial elevation (0°-30°)
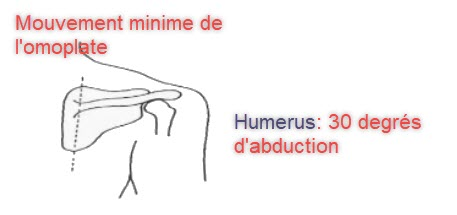
In this phase, which covers the first 30° of elevation, the scapula remains relatively stable. This is often referred to as the “setup” phase because the scapula can either rotate slightly inward, outward, or not move at all. During this phase, the 2:1 motion ratio is not yet in place. This motion is primarily due to the glenohumeral joint, where the humerus begins to elevate while the scapula is “lying down.” This phase allows movement to be initiated while providing initial stabilization of the scapulothoracic joint.
The stability of this phase is based on the coordinated action of the deltoid and the supraspinatus muscle.
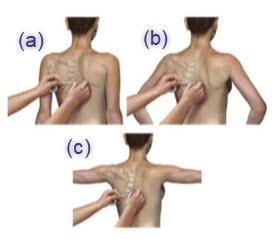
The image shows the relationship between the scapula and humerus during the first 30 degrees of lateral arm elevation. Arrows indicate the deltoid muscle (lower arrow) and trapezius muscle (upper arrow), which work together to initiate arm abduction, while the scapula remains relatively stable in this initial phase.
These muscles work together to initiate abduction of the arm while maintaining the head of the humerus in position within the glenoid fossa. Without proper muscle coordination, problems such as subluxations or dyskinesias of the scapula can occur, leading to pain and reduced mobility.
Phase 2: Intermediate elevation (30°-90°)

The second phase covers elevation between 30° and 90°. This is when the scapulohumeral rhythm really comes into play. The scapula begins to rotate upward, a movement that is primarily controlled by the upper and lower fibers of the trapezius as well as the serratus anterior muscle.

This upward rotation of the scapula helps keep the head of the humerus centered in the glenoid fossa, thus avoiding impingement and injury.
The 2:1 ratio is established during this phase, with approximately 40° of motion at the glenohumeral joint and 20° of upward rotation of the scapula.
This coordination is essential to prevent shoulder pathologies such as rotator cuff tendinopathies or subacromial bursitis. Dysfunction in this phase can lead to overload of the shoulder muscles, particularly the deltoid and rotator cuff muscles, which can ultimately lead to injuries.
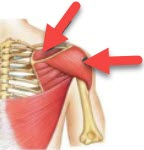
Phase 3: Full elevation (90°-180°)
The third phase involves the last 90° of the elevation movement. During this phase, the scapula continues to rotate upward, but also begins to rise along the rib cage. This elevation helps maintain the relationship between the humerus and the scapula while avoiding any compression of the subacromial structures.
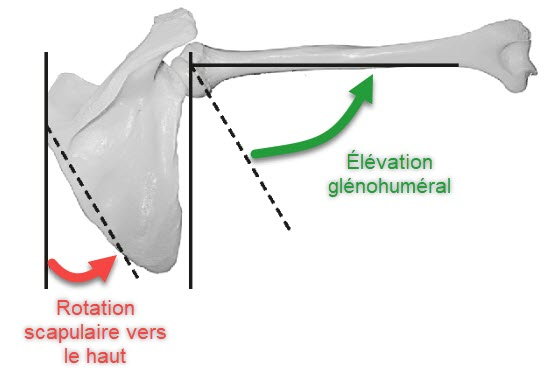
The image shows the relationship between glenohumeral elevation (green arrow) and upward scapular rotation (red arrow). During this phase, the humerus continues to elevate while the scapula rotates upward to maintain optimal coordination of the scapulohumeral rhythm. This helps preserve stability and efficiency of movement in the shoulder joint.
During this phase, the 2:1 ratio of scapulohumeral motion continues. The motion is also characterized by an increase in the angle between the scapular spine and the clavicle, which increases by an additional 10°. This adaptation allows the shoulder to achieve full elevation while minimizing stress on the surrounding tendons and ligaments.
Functional Importance of the Scapulo-Humeral Rhythm
The scapulohumeral rhythm is more than just joint mechanics; it represents a key function to ensure optimal mobility and stability of the shoulder. Its role is essential for the proper functioning of the glenohumeral joint and to prevent injuries related to excessive or incorrect use of the shoulder.
The main function of the scapulohumeral rhythm is to allow the glenoid fossa to maintain an optimal position to receive the head of the humerus throughout the movements of the arm. This synchronization ensures that the head of the humerus remains centered in the glenoid fossa, thus reducing the risks of subluxation or dislocation.
Another important function is the preservation of the length-tension relationships of the glenohumeral muscles. These muscles, particularly the rotator cuff muscles, are responsible for stabilizing the humerus in the glenoid fossa during movement. As the scapula rotates upward, it prevents these muscles from shortening excessively, allowing them to maintain their force production over a greater range of motion. This is crucial for activities that involve repeated arm elevation, such as throwing or swimming.
Another key role of the scapulohumeral rhythm is to distribute loads and forces between the glenohumeral joint and the scapulothoracic joint. By distributing motion between these two joints, the shoulder can perform complex movements while minimizing stress on individual structures. This distribution of forces is essential to prevent overuse injuries, such as tendinopathy or rotator cuff tears.
In addition to its mechanical role, the scapulohumeral rhythm has a protective function. By maintaining coordination between the humerus and scapula, it helps reduce compression of soft structures, such as the rotator cuff tendons and the subacromial bursa, beneath the acromion. Without this coordination, painful conditions such as subacromial impingement can occur, limiting shoulder function and causing chronic pain.
Finally, the scapulohumeral rhythm is a key indicator of overall shoulder health. An imbalance in this rhythm can be a sign of various pathologies, ranging from muscle dysfunction to more serious joint problems, such as osteoarthritis or adhesive capsulitis. For this reason, an accurate assessment of the scapulohumeral rhythm is essential to detect and treat underlying problems.
Causes of Abnormal Scapulo-Humeral Rhythm
An abnormal scapulohumeral rhythm can result from various pathologies or injuries affecting the shoulder, clavicle or surrounding muscles. These abnormalities can lead to imbalances in movement, reducing mobility and increasing the risk of injury.
Clavicle fractures, for example, can disrupt the natural motion of the scapula. The clavicle plays a critical role in stabilizing the scapula and rotating it upward. If the clavicle is fractured, the ability of the scapula to rotate is compromised, which can lead to dysfunction of the scapulohumeral rhythm. This results in reduced mobility and increased pain during arm elevation movements.
Paralysis of the spinal accessory nerve, which innervates the trapezius muscle, is another common cause of dysfunction. Without the trapezius to control upward rotation of the scapula, the 2:1 ratio is disrupted, leading to an imbalance between the humerus and scapula. This dysfunction often results in limited arm elevation and rapid muscle fatigue.
Weakness of the serratus anterior muscle can also cause an alteration in the scapulohumeral rhythm. The serratus anterior is responsible for the protraction and upward rotation of the scapula. When this muscle is weakened, as in the case of a long thoracic nerve injury, the scapula can “detach” from the rib cage, a phenomenon called scapula alata. This condition causes abnormal movement of the shoulder, limiting function and causing pain during elevation movements.
Joint pathologies such as osteoarthritis of the acromioclavicular joint and degeneration of the glenohumeral joint can also affect the scapulohumeral rhythm. Osteoarthritis causes wear and tear on the articular cartilage, limiting movement and causing pain. The resulting stiffness can lead to reduced upward rotation of the scapula, disrupting the 2:1 ratio.
Adhesive capsulitis, also known as frozen shoulder, is a condition where the joint capsule of the shoulder becomes inflamed and rigid, leading to severe limitation of movement. This condition completely disrupts the scapulohumeral rhythm, making raising the arm extremely painful and difficult.
Properly diagnosing these underlying causes is essential to restoring normal shoulder motion. Assessing the scapulohumeral rhythm can help identify abnormalities and guide appropriate therapeutic interventions, such as strengthening exercises, manual therapy, or surgery in more severe cases.
Assessment Tests
Assessment of scapulohumeral rhythm requires a thorough clinical analysis to detect abnormalities and dysfunctions. Two specific tests, the lateral scapular glide test (LSST) and the scapular dyskinesia test, are commonly used to assess coordination between the humerus and scapula.
Lateral scapular glide test
The lateral scapular glide test (LSST) is a simple but effective test to measure scapular position in different phases of arm movement. This test involves measuring the distance between the inferomedial angle of the scapula and the nearest spinous process at three different arm positions: at rest (0° of elevation), at 45° of abduction, and at 90° of abduction.
An asymmetry of 1.5 cm or more between the two sides is generally considered pathological and may indicate a dysfunction of the scapulohumeral rhythm. The LSST allows the detection of deviations in the position of the scapula, which is essential for diagnosing problems such as scapular dyskinesia or muscle weakness of the serratus anterior or trapezius.
Scapular Dyskinesia Test
Another important visual test is the scapular dyskinesia test . It assesses the quality of scapular movement during weighted shoulder flexion and abduction movements. This test relies on visual observation of the scapula as the patient performs these movements. Scapular dyskinesia is suspected when the scapula exhibits irregular movements, such as abnormal rotation, premature elevation, or excessive tilting.

Patients with scapular dyskinesia often have muscle imbalances between the stabilizing muscles of the scapula, such as the serratus anterior, rotator cuff muscles, and upper and lower trapezius muscles. Scapular dyskinesia is particularly common in patients with chronic shoulder pain, a history of shoulder injuries, or repetitive activities that place high demands on the shoulder, such as in athletes.
The classification of scapular dyskinesia is divided into three main types:
- Type 1: Excessive downward rotation of the scapula, often accompanied by anterior tilt. This dysfunction is usually caused by weakness of the serratus anterior or tightness of the posterior capsule.
- Type 2: Internal tilt of the scapula with excessive displacement of the medial angle of the scapula. This presentation is often related to weakness of the lower trapezius and rhomboid.
- Type 3: Excessive elevation of the scapula with insufficient upward rotation. This dysfunction is frequently seen in acute or post-traumatic injuries, such as clavicle fracture or spinal accessory nerve palsy.
The use of these two tests is crucial to identify imbalances and dysfunctions in the scapulohumeral rhythm, allowing an appropriate treatment plan to be put in place to restore normal movement. Treatment may include specific strengthening exercises, manual therapy to correct muscle imbalances, or, in some cases, surgery to repair structural damage.
Global functional assessment of the shoulder is also essential, as dysfunctions of the scapulohumeral rhythm can lead to cascading effects on other parts of the body, including neck or thoracic pain due to postural compensation. Health professionals, such as osteopaths, play a key role in this assessment by using a holistic approach to identify the underlying causes of dysfunctions and treat them.
Care and Rehabilitation
Once a scapulohumeral rhythm imbalance has been identified, a multimodal treatment approach is necessary to restore shoulder function and mobility. Treatment typically combines manual techniques, strengthening and stretching exercises, and rehabilitation strategies targeting the muscles involved in scapula and humerus movement.
The first goal of rehabilitation is to restore muscular balance . Muscles such as the serratus anterior, lower trapezius, and deltoid must be strengthened to ensure harmonious movement between the humerus and scapula. Specific exercises, such as resistance-banded shoulder raises or resisted external rotation movements, are used to target these muscles. These exercises improve dynamic shoulder stability and minimize the risk of long-term injury.
The use of manual techniques is also crucial in management. Osteopaths and other manual health professionals can use gentle mobilization techniques to release joint restrictions at the thoracic spine, acromioclavicular joint, or glenohumeral joint. These techniques help improve mobility and restore proper synchronization of scapulohumeral motion. Gentle manipulations of the scapula, in particular, can correct postural deviations and improve scapular glide on the rib cage.
Another essential aspect of treatment is stretching tight muscles . The pectoralis major, latissimus dorsi, and levator scapulae are often tight in patients with scapulohumeral rhythm dysfunction. Specific stretching exercises, such as the pectoralis major wall stretch or the latissimus dorsi side-bending stretch, can help release these tensions and improve shoulder range of motion.
Rehabilitation is not limited to physical exercises. Patient education is equally important. It is essential that patients understand the importance of maintaining good posture, adopting correct lifting techniques, and strengthening their shoulder girdle muscles. Ergonomic adjustments, such as changing the height of the workstation or using protective equipment during sports activities, can also help prevent recurrence of injuries.
The final phase of rehabilitation includes functional rehabilitation , which aims to restore the functional abilities of the shoulder for specific activities, especially for athletes or people with physically demanding jobs. Proprioception and dynamic stabilization exercises, such as the use of exercise balls or balance boards, are essential to improve coordination between the shoulder and trunk muscles.
In more severe cases, where conservative methods fail, surgery may be necessary. Surgery is usually reserved for cases of significant rotator cuff tears, severe joint injuries, or fractures. After surgery, rehabilitation becomes even more crucial to ensure a full recovery and avoid future complications.
Post-surgical rehabilitation follows a specific protocol, with gradual steps to restore mobility, then strength. The first few weeks focus on pain and inflammation management, followed by passive and then active range of motion exercises. Eventually, strengthening and stability exercises are reintroduced to allow the patient to regain full function.
Conclusion
The scapulohumeral rhythm is a complex and essential mechanism for the health and functionality of the shoulder. Understanding and assessing this rhythm is crucial to prevent and treat shoulder injuries, especially in athletes or people performing repetitive movements. An imbalance in this rhythm can lead to pain, reduced mobility, and long-term joint pathologies.
Through a multidisciplinary approach, including manual techniques, targeted exercises and adequate education, it is possible to restore a harmonious scapulohumeral rhythm. Early management not only prevents future complications, but also optimizes the performance and quality of life of patients.
In osteopathy, the role of the healthcare professional is to assess and treat these dysfunctions while supporting the patient in a process of overall healing. Care must always be individualized to meet the specific needs of each patient, taking into account their medical history and level of activity.
Thus, the key to a healthy shoulder lies in the harmony of movement between the humerus and the scapula, a balance that helps preserve both mobility and joint stability.
References
- Kibler, W. B. (1998). The role of the scapula in athletic shoulder function. The American Journal of Sports Medicine, 26(2), 325–337. https://doi.org/10.1177/03635465980260022801
- Ludewig, P. M., & Reynolds, J. F. (2009). The association of scapular kinematics and glenohumeral joint pathologies. Journal of Orthopaedic & Sports Physical Therapy, 39(2), 90–104. https://doi.org/10.2519/jospt.2009.2808
- McQuade, K. J., & Smidt, G. L. (1998). Dynamic scapulohumeral rhythm: The effects of external resistance during elevation of the arm in the scapular plane. Journal of Orthopaedic & Sports Physical Therapy, 27(2), 125–133. https://doi.org/10.2519/jospt.1998.27.2.125
- Inman, V. T., Saunders, J. B. de C. M., & Abbott, L. C. (1944). Observations on the function of the shoulder joint. The Journal of Bone and Joint Surgery, 26(1), 1–30.
- Ludewig, P. M., Hoff, M. S., Osowski, E. E., Meschke, S. A., & Rundquist, P. J. (2004). Relative balance of serratus anterior and upper trapezius muscle activity during push-up variations. Journal of Orthopaedic & Sports Physical Therapy, 34(5), 242–248. https://doi.org/10.2519/jospt.2004.34.5.242
- Roche, S. J., & Funk, L. (2011). Scapular dyskinesis in shoulder injury: A review. International Journal of Shoulder Surgery, 5(2), 46–51. https://doi.org/10.4103/0973-6042.83189
- Lukasiewicz, A. C., McClure, P., Michener, L., Pratt, N., & Sennett, B. (1999). Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. Journal of Orthopaedic & Sports Physical Therapy, 29(10), 574–586. https://doi.org/10.2519/jospt.1999.29.10.574
- Myers, J. B., Laudner, K. G., Pasquale, M. R., Bradley, J. P., & Lephart, S. M. (2005). Scapular position and orientation in throwing athletes. The American Journal of Sports Medicine, 33(2), 263–271. https://doi.org/10.1177/0363546504268138
- Kibler, W. B., & McMullen, J. (2003). Scapular dyskinesis and its relation to shoulder pain. Journal of the American Academy of Orthopaedic Surgeons, 11(2), 142–151. https://doi.org/10.5435/00124635-200303000-00008
- Phadke, V., Camargo, P., & Ludewig, P. M. (2009). Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Brazilian Journal of Physical Therapy, 13(1), 1–9. https://doi.org/10.1590/s1413-35552009005000013

























{kind=link}