

Spondylolisthesis comes from the Greek derivatives “spondylos”, meaning vertebra, and “olisthanein”, meaning to slip. Essentially, it is defined as the slipping of one vertebra over another.
Introduction
Stress fractures are caused by repetitive loading on the back of the lumbar vertebrae, especially when the spine is in extension. In the spine, the vertebral body is designed to receive loads and the intervertebral disc is designed to shock absorber. The posterior unit of the vertebra is not designed to receive excessive loads, but to protect the spine. During extension, the center of gravity is shifted posteriorly. The facet joints then have to bear a load for which they are not designed.
The lumbar spine is lordotic and the facet joints are constantly receiving excessive weight due to the posterior shift of the center of gravity. Any situation that causes overload in extension will eventually lead to deterioration of the cartilaginous surfaces and ultimately premature wear of the cartilaginous surfaces. Overloading of the facet joint, especially with repetitive or high-intensity loads, can lead to the development of stress fractures. Stress fractures of the interarticular isthmus themselves produce pain, but they also create problems when they develop into spondylolisthesis.
- In 25% of patients with spondylolysis, spondylolisthesis develops. Gymnasts have a four-fold increased risk of developing spondylolisthesis due to repetitive hyperflexion-hyperextension maneuvers such as inverting, jumping, dismounting, and dorsiflexion exercises.
- Approximately 90% of spondylolysis occurs at L5, and the risk of slippage is at L5 – S1.
- The hamstrings are usually contracted: The body reacts strongly to the forward vertebral slide by tilting the pelvis backwards, with the help of the hamstring.


A bit of history
Although it was Kilian who coined the word “spondylolisthesis” in 1854, it was actually Georges Herbiniaux, a Belgian obstetrician, who first described it in 1782 when he reported the complete dislocation of the L5 vertebral body on the sacrum, causing narrowing of the birth canal and difficulty during childbirth.
In fact, many cases of spondylolisthesis reported before 1900 were documented by obstetricians. In 1888, Franz Ludwig von Neugebauer was one of the first to recognize that the most common form of spondylolisthesis, isthmic, was associated with separation of the posterior neural arch from the vertebral body.
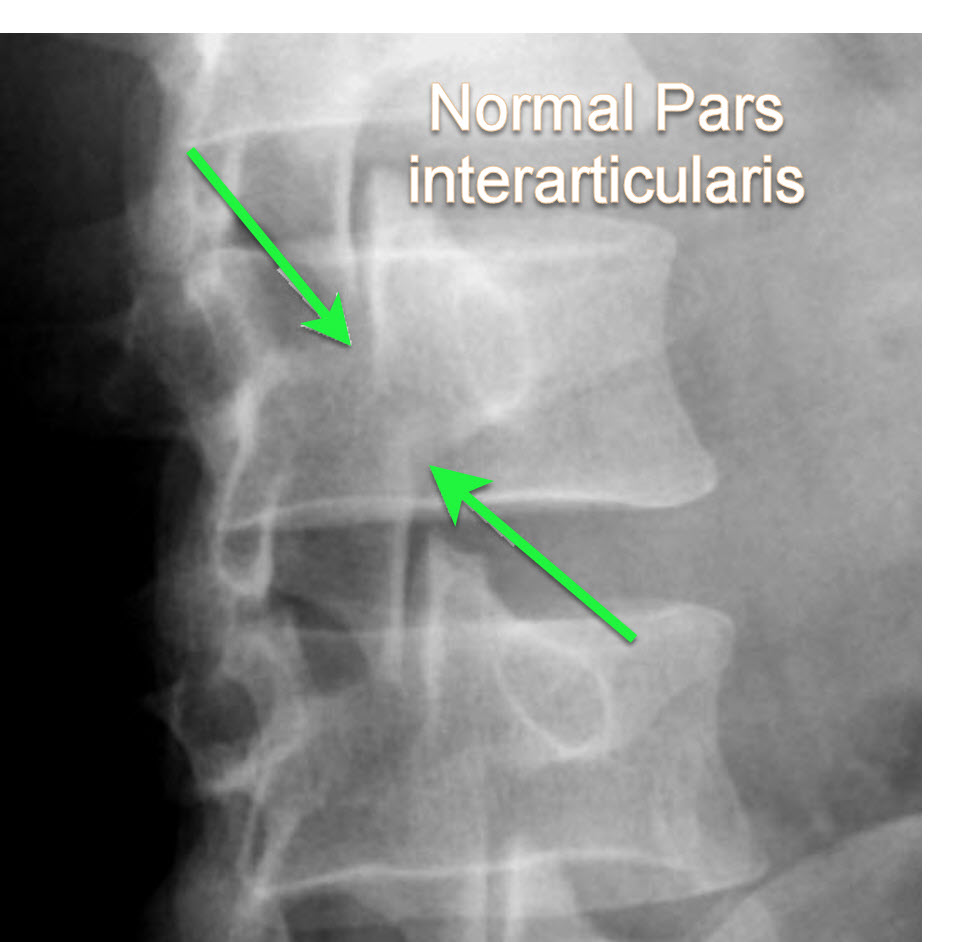
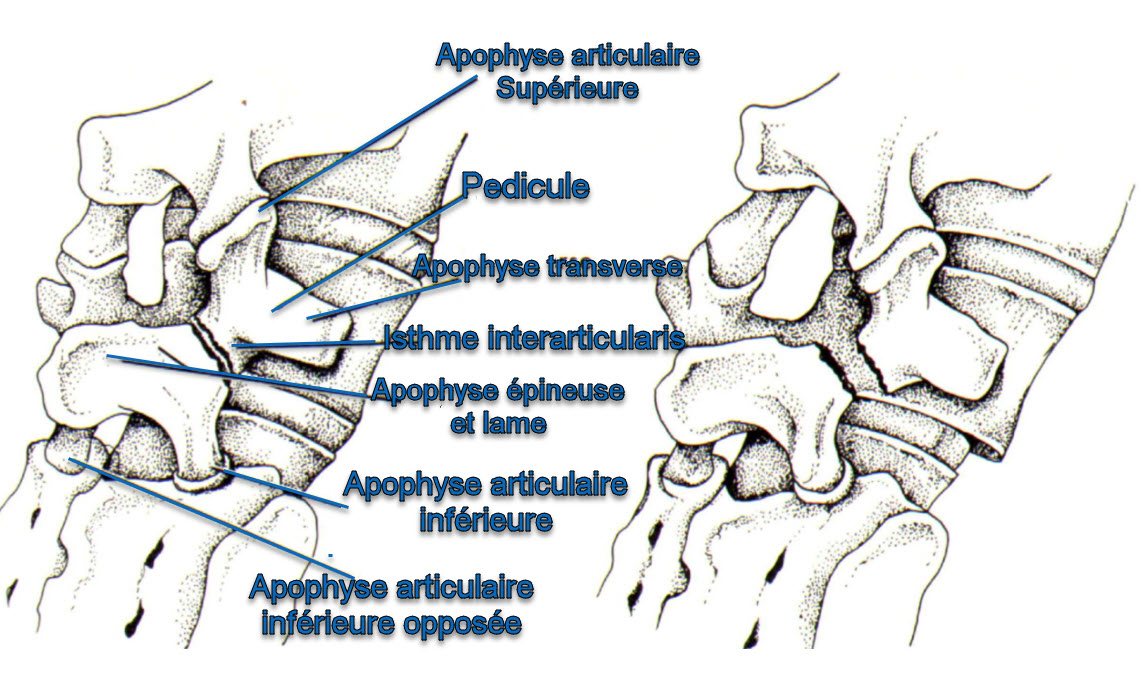
He noted that a bony defect was frequently encountered at the junction of the inferior and superior articular processes, or pars interarticularis, allowing anterior displacement of the vertebral body while the spinous process and inferior articular surfaces remained aligned with the posterior sacrum. This bony defect at the pars interarticularis was subsequently termed “spondylolysis.” The purpose of this chapter is to describe the evolving understanding of the etiology, diagnosis, and treatment of spondylolisthesis, particularly of the isthmic type.
In the late 19th and early 20th centuries, studies attempted to identify the cause of spondylolysis, which was thought to be a major factor in spondylolisthesis. In 1888, Neugebauer proposed the theory of abnormal ossification, but it was refuted in the early 1900s. In 1931, Willis examined 1,520 human skeletons, finding no evidence of abnormal ossification. Congdon and Meyerding also contributed to the understanding of spondylolysis and its association with spondylolisthesis, noting that the condition was more common in men.
Furthermore, he suggested that trauma appeared to play a significant role in the etiology of spondylolysis, with approximately 38% of patients in the series attributing the cause to trauma. However, Meyerding maintained that congenital defects and apparent instability of the lumbosacral joint could also contribute to spondylolysis.
In 1932, Norman Capener attempted to explain the pathogenesis of spondylolysis and the demographic characteristics of spondylolisthesis through the study of 34 cases of affected patients. Like Meyerding, he noted a predominance in men (53-47%). Capener described the detrimental effect of the sacrum on the fifth vertebra, acting as a wedge that divides the pars interarticularis and causes vertebral slippage. He also discussed reasons limiting the slippage, noting that the iliolumbar ligaments restrain excessive anterior displacement of the vertebral body, and bony proliferation on the sacrum can stop the progression of the L5 vertebra slippage.
From 1939 to 1951, additional studies were conducted to understand the incidence and etiology of spondylolysis. Martin Batts (1939) found no cases of double ossification center in 200 fetal vertebral columns, and Maurice Roche and George Rowe (1951) found no consistent association between accessory ossification center and spondylolysis after examining 53 fetuses and 20 human embryos.
Types of lumbar spondylolisthesis
- Dysplastic : This type of spondylolisthesis is due to congenital anomalies of the superior facets of the sacrum or the inferior facets of the fifth lumbar vertebra, which allow L5 to slide on S1. No defects of the interarticular isthmus are observed. The sacrum is not strong enough to support the weight and the effort. The isthmus and the inferior facets of L5 therefore become deformed. If the isthmus lengthens, it is impossible to distinguish this type from isthmic type II b) on radiographs. If the isthmus separates, it becomes impossible to distinguish this type from isthmic type II a) on radiographs. This type is also associated with defects of the sacrum and the vertebral arch. A familial tendency is observed.
- Spondylolytic (isthmic): This type is due to a defect in the interarticular isthmus that allows L5 to slide forward relative to S1. There are three subtypes of isthmic spondylolisthesis:
- A fatigue (stress) fracture of the interarticular isthmus – lytic. Attenuation of the pars
- An elongated but intact interarticular isthmus
- Acute fracture of the interarticular isthmus
- Degenerative : The lesion results from long-standing intersegmental instability, followed by remodeling of the articular processes at the affected level. Multiple small compression fractures on the inferior articular process of the vertebra that is slipping forward have also been suggested as a possible cause. The articular processes change direction, assuming a more horizontal position as the slippage increases. This lesion is four times more common in women than in men, and six times more likely to occur at the L4-5 level than at adjacent levels. This lesion is not usually seen in persons under 40 years of age.
- Traumatic : This type of spondylolisthesis follows fractures in the region of the bony hook, other than fractures of the interarticular isthmus, in particular of the pedicle, the lamina or a facet.
- Pathological : This type of spondylolisthesis results from localized or generalized osteopathy and fragility or weakness of the bone structure such as osteogenesis imperfecta.


Causes
- Abnormal Development: In some cases, lumbar spondylolisthesis may result from abnormal development of the facet joints, the small joints between the vertebrae.
- Facet Dysplasia: Facet dysplasia is a condition where the facet joints do not develop normally, which can cause one vertebra to slip past another.
- Congenital Defect: Some people are born with a genetic predisposition to develop spondylolisthesis due to congenital abnormalities of the facet joints.
- Trauma: Trauma, such as fractures or facet joint injuries, can contribute to spondylolisthesis, especially in individuals exposed to sports activities or repetitive motions.
- Repetitive Stress: Repetitive movements of the spine, such as excessive extension or flexion, can contribute to fatigue of the facet joints, increasing the risk of spondylolisthesis.
- Hyperlordosis: Excessive inward curvature of the lumbar spine, known as hyperlordosis, can increase pressure on the facet joints and promote slippage of the vertebrae.
- Spondylolysis: Spondylolysis is a fracture of the posterior arch of the vertebra, often at the level of the fifth lumbar vertebra (L5). If spondylolysis is left untreated, it can progress to spondylolisthesis.
- Aging: Natural aging of the spine, associated with degeneration of the intervertebral discs and wear of the facet joints, may increase the risk of spondylolisthesis in older adults.
- Vertebral Instability: Vertebral instability, often associated with weakness of the ligaments that hold the vertebrae in place, can lead to slippage of the vertebrae.
Symptoms
- Lower Back Pain: Pain in the lower back is one of the most common symptoms. The pain can be felt in the lower back and can be aggravated by movement, physical exertion, or prolonged standing.
- Lumbar Stiffness: Some individuals may experience stiffness in the lumbar region, which can limit spinal mobility.
- Radiating Pain: If the spinal slip compresses the nerve roots, it can cause radiating pain along the sciatic nerve, usually into the buttocks and legs. This is often called sciatica.
- Muscle Weakness: Compression of nerve roots can cause muscle weakness in the legs. This may manifest as difficulty walking, climbing stairs, or lifting objects.
- Numbness and Tingling: Nerve compression can also cause feelings of numbness, tingling, or pins and needles in the legs or feet.
- Decreased Bladder or Bowel Control: In severe cases of lumbar spondylolisthesis, nerve compression can cause loss of bladder or bowel control. This requires immediate medical attention.
- Difficulty Standing Upright: Some individuals may have difficulty maintaining a straight standing position due to pain and stiffness.
- Decreased Step Size: Muscle weakness and pain can cause a decrease in step size while walking.
One factor that makes the cause of pain in spondylolysis and spondylolisthesis more confusing is that the severity of symptoms does not necessarily correlate with the degree of slippage. Indeed, one person may have a significant forward slippage with minimal pain, while another person may have only a minor slippage but experience more significant S1 pain.
Pathophysiology
- Posterior arch fracture
- Posterior arch fracture can result from a variety of causes, including repeated stresses on the spine, trauma, or congenital abnormalities. This fracture can weaken the stability of the affected vertebra.
- Slippage of the vertebra
- Due to the posterior arch fracture, the vertebra may begin to slide forward relative to the underlying vertebra. This slippage may be gradual and occur over a period of time.
- Spinal instability
- The progressive slippage leads to spinal instability in the lumbar spine. This instability can cause misalignment of the vertebrae and lead to changes in the normal position of the spine.
- Compression of neighboring structures
- Spondylolisthesis can cause compression of nearby structures, including intervertebral discs, nerves, and facet joints. This can cause symptoms such as pain, stiffness, and neurological problems.
- Inflammatory response
- Compression of structures can trigger an inflammatory response in the affected area. Inflammation can contribute to the pain and discomfort associated with spondylolisthesis.
- Compensatory reaction
- The body may respond by developing compensatory mechanisms to maintain overall balance and stability of the spine. This may include changes in the curvature of the spine (lordosis or kyphosis) to compensate for the slippage.
- Clinical symptoms
- Clinical symptoms of lumbar spondylolisthesis may include lower back pain, stiffness, difficulty standing or walking, and in some cases, neurological symptoms such as numbness or weakness.
Classifications
Classification of lumbar spondylolisthesis is often based on the degree of slippage of the vertebrae and the underlying cause of the spondylolisthesis. Two commonly used classification systems are the Meyerding classification and the Wiltse classification.
- Meyerding classification:
- Grade I: Less than 25% anterior slippage of the upper vertebra relative to the lower vertebra.
- Grade II: 25-50% slip.
- Grade III: 50-75% slip.
- Grade IV: 75-100% slippage.
- Grade V: Complete slippage, the upper vertebra is completely in front of the lower vertebra.
- Wiltse classification:
- Dysplastic: Associated with congenital facet dysplasia.
- Isthmic: Associated with spondylolysis, a fracture of the posterior arch of the vertebra.
- Degenerative: Resulting from degeneration of the intervertebral discs and facet joints.
- Traumatic: Resulting from a fracture or traumatic injury.
- Pathological: Associated with an underlying disease, such as a tumor or infection.
- Marchetti and Bartolozzi classification:
- Type I: Degenerative spondylolisthesis with severe disc disease.
- Type II: Degenerative spondylolisthesis with moderate disc disease.
- Type III: Dysplastic spondylolisthesis with spondylolysis.
- Type IV: Dysplastic spondylolisthesis without spondylolysis.

Spondylolysis may contribute to decreased intervertebral space.
Spondylolysis can lead to spinal instability and, over time, contribute to degenerative changes in the spine, including decreased intervertebral space.
Here’s how it can happen:
- Posterior arch fracture: Spondylolysis often involves a fracture of the posterior arch of the vertebra.
- Spinal Instability: This fracture can lead to spinal instability, where the affected vertebra may begin to slip relative to the underlying vertebra.
- Degenerative changes: Instability and progressive slippage can lead to degenerative changes in the intervertebral discs and facet joints, contributing to decreased intervertebral space.
These changes can be seen on medical images such as X-rays or MRIs of the spine. It is essential to note that the severity of spinal cord space narrowing can vary from individual to individual depending on the severity of spondylolysis and other factors such as age, physical activity, and genetics. A healthcare professional can provide an accurate diagnosis and recommend an appropriate treatment plan based on the specific situation.
Differential diagnosis of lumbar spondylolisthesis
- Herniated Disc: A herniated disc occurs when the gelatinous core inside an intervertebral disc extends beyond its normal position, putting pressure on surrounding structures and causing symptoms similar to spondylolisthesis.
- Spinal Stenosis: Spinal stenosis is the narrowing of the spinal canal, which can compress the spinal cord or nerve roots, causing lower back pain, leg pain, and weakness.
- Facet Arthritis: Arthritis of the facet joints can cause lower back pain similar to spondylolisthesis, especially with spinal movements.
- Vertebral Fracture: A fracture of the vertebra can cause lower back pain and, in some cases, spinal instability that can be confused with spondylolisthesis.
- Pyramidalis Muscle Syndrome: This syndrome can cause pain in the buttocks and legs due to compression of the sciatic nerve, thus simulating the symptoms of spondylolisthesis.
- Spinal Tumors: Tumors in the spine can cause pain and neurological symptoms, sometimes similar to those of spondylolisthesis.
- Spinal Infections: Infections, such as osteomyelitis, can affect the vertebrae and cause symptoms similar to spondylolisthesis.
- Sacroiliitis: Inflammation of the sacroiliac joints can cause pain in the lower back and buttocks, resembling some symptoms of spondylolisthesis.
- Lumbar Spinal Cord Syndrome: A condition where the lumbar spinal cord is narrowed, which can cause symptoms of pain, weakness and numbness in the legs, similar to spondylolisthesis.
- Facet Syndrome: Irritation or inflammation of the facet joints can cause lower back pain and stiffness, mimicking the symptoms of spondylolisthesis.
Prevention of Spondylolisthesis
- Maintain a healthy weight: Maintaining an appropriate body weight is essential to reduce pressure on the spine, especially in the lumbar region. Excess weight can increase stress on the intervertebral discs and promote slippage of the vertebrae.
- Adopt good posture: Proper posture is crucial for spinal health. Make sure to maintain an upright posture when sitting or standing. Use chairs with good lumbar support, and avoid sitting or standing in the same position for long periods of time.
- Strengthen your core muscles: Strengthening exercises, especially those that target your core and back muscles, can help stabilize your spine. Exercises like sit-ups, back extensions, and planks can strengthen the muscles that surround your spine.
- Do stretching exercises: Regular stretching exercises can improve the flexibility of the spine and surrounding muscles. Be sure to focus your stretches on the lower back to maintain adequate range of motion.
- Avoid sudden movements: Avoid sudden movements or excessive twisting of the spine, especially when lifting heavy objects. Use proper lifting techniques to reduce stress on the spine.
- Engage in low-impact physical activities: Opt for low-impact physical activities, such as swimming, walking or cycling, which are less stressful on the spine than high-impact activities like running.
- See a healthcare professional regularly: Regular visits to a healthcare professional, such as a chiropractor or osteopath, can help you maintain the health of your spine and identify any potential problems before they become serious.
- Avoid a sedentary lifestyle: An active lifestyle is beneficial for spinal health. Avoid a sedentary lifestyle by incorporating physical activities into your daily routine.
Muscles most involved in spondylolisthesis
The muscles most involved often depend on the type of spondylolisthesis and the specific region of the spine affected. However, generally speaking, certain muscle groups may be involved in the context of spondylolisthesis:
- Paraspinal muscles: The muscles along the spine, including the erector spinae muscles, are important for maintaining stability and posture. In spondylolisthesis, these muscles may be used to compensate for vertebral slippage.
- Abdominal Muscles: The abdominal muscles, especially deep muscles such as the transverse abdominis, are essential for supporting the lower back and contributing to spinal stability.
- Gluteal muscles: The gluteal muscles, such as the gluteus maximus, may be strained due to changes in pelvic position associated with spondylolisthesis.
- Hamstrings: These muscles in the back of the thigh may be involved because of their connection to the pelvis and spine.
- Pelvic floor muscles: These muscles support the pelvic region and may be affected due to pelvic adjustments related to spondylolisthesis.
Frequently Asked Questions
Q: What is spondylolytic spondylolysis and what does it involve?
Spondylolytic spondylolysis is defined as a defect or fracture of the interarticular isthmus (pars interarticularis) of the vertebral arch. It most commonly occurs in the lower lumbar vertebrae, primarily at the L5 vertebra. Spondylolisthesis is defined as the progressive anterior slippage of a vertebra caused by spondylolysis.
Q: What are the types of lumbar spondylolisthesis?
There are different types of lumbar spondylolisthesis, including dysplastic, isthmic, degenerative, traumatic, and pathological. Each type is associated with specific causes, such as congenital anomalies, fractures, degeneration of the intervertebral discs, trauma, or pathological conditions.
Q: What are the clinical symptoms of lumbar spondylolisthesis?
Clinical symptoms of lumbar spondylolisthesis may include lower back pain, stiffness, difficulty standing or walking, and neurological symptoms such as numbness, tingling, and muscle weakness. In severe cases, there may be loss of bladder or bowel control.
Q: What causes lumbar spondylolisthesis?
Causes of lumbar spondylolisthesis may include abnormal development of the facet joints, facet dysplasia, congenital defects, trauma, repetitive stress, hyperlordosis, spondylolysis, and natural aging of the spine.
Q: How is lumbar spondylolisthesis diagnosed?
Diagnosis of lumbar spondylolisthesis can be made using radiographs. Some specific radiographic signs include slippage of the vertebrae, Meyerding’s line to measure the degree of slippage, the presence of osteophytes, widening of the facet joints, spondylolysis, deformation of the intervertebral discs, and other signs of instability.
Q: What are the differential diagnoses of lumbar spondylolisthesis?
Differential diagnoses of lumbar spondylolisthesis include herniated disc, spinal stenosis, facet arthritis, vertebral fracture, piriformis syndrome, spinal tumors, spinal infections, sacroiliitis, lumbar spinal canal stenosis, and facet syndrome.
Q: How is lumbar spondylolisthesis classified?
Two commonly used classification systems are the Meyerding classification, which measures the degree of slippage, and the Wiltse classification, which categorizes spondylolisthesis based on the underlying cause (dysplastic, isthmic, degenerative, traumatic, pathologic). Another classification by Marchetti and Bartolozzi also takes into account the degree of disc disease.
Q: How does the pathophysiology of lumbar spondylolisthesis occur?
The pathophysiology of lumbar spondylolisthesis often involves posterior arch fracture, progressive slippage of the vertebra, spinal instability, compression of neighboring structures, an inflammatory response, and a compensatory reaction of the body to maintain balance and stability of the spine. This can result in symptoms such as pain, stiffness, and neurological problems.
Q: What are the treatment methods for lumbar spondylolisthesis?
Treatment for lumbar spondylolisthesis may include conservative approaches such as osteopathy, analgesic medications, and activity modification. In severe or symptomatic cases, surgery may be considered to stabilize the spine and reduce slippage. The choice of treatment depends on a variety of factors, including the severity of symptoms and the underlying cause of the spondylolisthesis.
Radiographic Signs
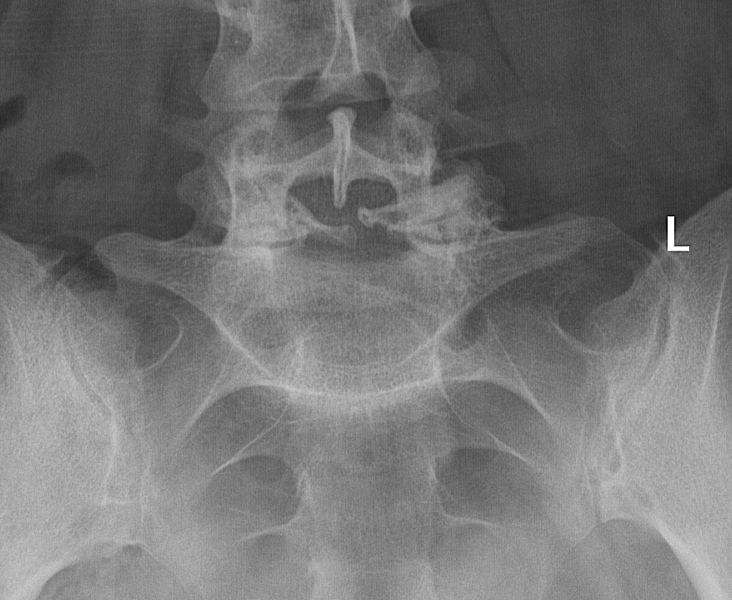
X-rays are one of the most commonly used imaging methods to diagnose lumbar spondylolisthesis. There are some specific radiographic signs that may indicate the presence of this condition. Here are some of the signs that radiologists and healthcare professionals look for when interpreting spinal X-rays for lumbar spondylolisthesis:
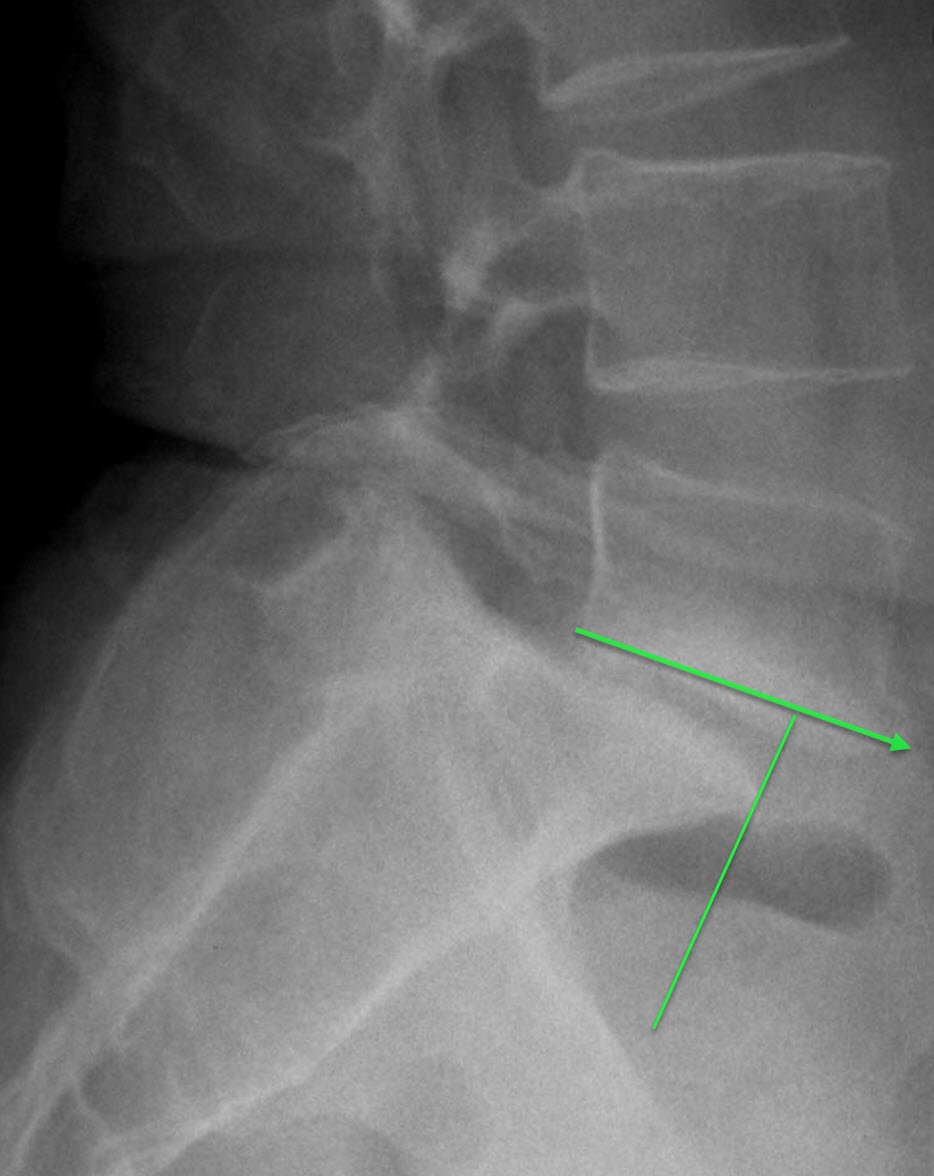
- Vertebral Slippage: The most obvious sign is the anterior slippage of one vertebra relative to the vertebra below it. This can be seen on the lateral (side) x-ray. The degree of slippage is usually measured as a percentage of the width of the vertebral body.
- Meyerding Line: This line is used to measure the degree of slippage. It is drawn along the posterior part of the upper vertebra and measures the distance from the lower vertebra. The measurement is expressed as a percentage of the width of the lower vertebra.
- Osteophytes: Bone spurs (osteophytes) may form around the slipped vertebra in response to instability and degeneration.
- Facet Joint Widening: Widening or irregularity of the facet joints may indicate instability in these joints.
- Spondylolysis: The presence of spondylolysis, a fracture of the posterior arch of the vertebra, may be a preliminary sign of spondylolisthesis.
- Intervertebral Disc Deformation: Changes in the shape of the intervertebral discs, such as flattening or decreased height, may also be observed.
- Intervertebral Space Narrowing: The space between the vertebrae can be reduced due to slippage and degeneration of the discs.
- Signs of Instability: Signs of instability, such as changes in the relative position of the vertebrae during flexion and extension, may be assessed.
- Oblique radiographs of the lumbosacral spine may show a rupture of the pars interarticularis which represents the rupture in the neck of the ” Scottish Terrier (or Scottish Terrier with collar)”
The Scottie Dog Radiographic
The term “Scottie dog” has become common in the field of medical imaging to describe a specific radiographic configuration that is evident during imaging of the lumbar spine, particularly in the context of lateral (lateral) radiographs. This particular appearance is reminiscent of the silhouette of a Scottish terrier dog, hence the term itself. The radiographic signs of the “Scottie dog” are closely related to the anatomy of the lumbar vertebrae and can be clearly observed during radiographic evaluation of the spine.
To better understand this distinctive radiographic configuration, let’s look at the main components of the “Scottie dog” on a lumbar radiograph.
The Scottie dog’s ear is represented by the spinous process of the vertebra. This bony structure projects backward from the upper part of the vertebra, creating the first characteristic of the canine silhouette. The Scottie dog’s head is formed by the superior articular process of the vertebra. This process extends horizontally from the vertebral body, adding a distinctive dimension to the radiographic image.
The neck of the Scottie dog corresponds to the pedicle of the vertebra. This short portion of the vertebra connects the vertebral body to the head, forming an important structural link in the canine silhouette. The body of the Scottie dog is represented by the vertebral body itself, the central portion of the vertebra that contributes to the overall appearance of the figure.
The forelimb of the Scottie dog is formed by the transverse process of the vertebra. This process extends laterally from the vertebral body, creating an extension similar to a dog’s forelimb. Finally, the hindleg of the Scottie dog is formed by the inferior articular process, which extends downward from the vertebral body, completing the caniniform representation of the lumbar spine on the radiograph.
This particular configuration is of great use to radiologists and healthcare professionals when assessing the anatomy and integrity of the lumbar vertebrae. The visualization of the “Scottie dog” allows a deeper understanding of the spinal structures, facilitating the diagnosis and monitoring of spinal conditions.
Although the term “Scottie dog” is informal, it has become widely recognized and accepted in the medical field due to its ability to simplify the description of this distinctive radiographic configuration. Thus, when a medical professional uses this term, it instantly conjures up a clear image of the canine silhouette present on the lumbar radiograph, thus facilitating communication within the medical community.



Quizz
Quizz 1
- What anatomical feature is primarily responsible for the excessive weight on the facet joints in the lumbar spine?
- A) Anterior shift of the center of gravity
- B) Posterior shift of the center of gravity
- C) Lateral shift of the center of gravity
- D) None of the above
- What percentage of patients with spondylolysis develop spondylolisthesis?
- A) 10%
- B) 25%
- C) 50%
- D) 75%
- Which type of athletes have a four-fold increased risk of developing spondylolisthesis due to repetitive maneuvers?
- A) Swimmers
- B) Runners
- C) Gymnasts
- D) Cyclists
- At which vertebral level does approximately 90% of spondylolysis occur?
- A) L3
- B) L4
- C) L5
- D) S1
- Who first described the condition known as spondylolisthesis in 1782?
- A) Kilian
- B) Georges Herbiniaux
- C) Franz Ludwig von Neugebauer
- D) Norman Capener
- Which classification system categorizes spondylolisthesis based on the degree of slippage?
- A) Wiltse Classification
- B) Meyerding Classification
- C) Marchetti and Bartolozzi Classification
- D) None of the above
- What type of spondylolisthesis is due to congenital anomalies of the facet joints?
- A) Dysplastic
- B) Isthmic
- C) Degenerative
- D) Traumatic
- Which muscle group is typically contracted to counteract the forward vertebral slide in spondylolisthesis?
- A) Quadriceps
- B) Hamstrings
- C) Biceps
- D) Pectorals
- In the context of spondylolisthesis, what does a spondylolytic defect involve?
- A) Anterior arch of the vertebra
- B) Interarticular isthmus (pars interarticularis)
- C) Lateral process of the vertebra
- D) Transverse process of the vertebra
- Which type of spondylolisthesis results from localized or generalized osteopathy and fragility of the bone structure?
- A) Dysplastic
- B) Isthmic
- C) Degenerative
- D) Pathological
Answers:
- B) Posterior shift of the center of gravity
- B) 25%
- C) Gymnasts
- C) L5
- B) Georges Herbiniaux
- B) Meyerding Classification
- A) Dysplastic
- B) Hamstrings
- B) Interarticular isthmus (pars interarticularis)
- D) Pathological
Quizz 2
- What is the primary mechanical issue leading to the deterioration of the cartilaginous surfaces in the lumbar spine?
- A) Excessive flexion
- B) Posterior shift of the center of gravity
- C) Excessive lateral bending
- D) Anterior shift of the center of gravity
- Which type of spondylolisthesis is associated with congenital anomalies of the superior facets of the sacrum or the inferior facets of the fifth lumbar vertebra?
- A) Isthmic
- B) Dysplastic
- C) Degenerative
- D) Traumatic
- According to the text, which muscle group helps to counteract the forward vertebral slide in spondylolisthesis?
- A) Quadriceps
- B) Hamstrings
- C) Pectorals
- D) Deltoids
- Who was the first to describe spondylolisthesis, and in which year?
- A) Franz Ludwig von Neugebauer, 1888
- B) Georges Herbiniaux, 1782
- C) Norman Capener, 1932
- D) Kilian, 1854
- In the Meyerding classification system, what grade represents 50-75% slippage of the vertebra?
- A) Grade I
- B) Grade II
- C) Grade III
- D) Grade IV
- What does the Wiltse classification system focus on in categorizing spondylolisthesis?
- A) Degree of slippage
- B) Presence of neurological symptoms
- C) Underlying cause of the condition
- D) Severity of pain
- Which type of spondylolisthesis is characterized by a defect in the interarticular isthmus allowing forward slippage of L5 relative to S1?
- A) Degenerative
- B) Pathological
- C) Dysplastic
- D) Isthmic
- What does the presence of a bony defect at the pars interarticularis typically indicate?
- A) Traumatic spondylolisthesis
- B) Pathological spondylolisthesis
- C) Spondylolysis
- D) Degenerative spondylolisthesis
- Which muscle groups are identified as being involved in compensating for spondylolisthesis?
- A) Pectoral and biceps muscles
- B) Hamstrings and abdominal muscles
- C) Triceps and latissimus dorsi
- D) Gastrocnemius and soleus
- What is a common symptom of lumbar spondylolisthesis that does not necessarily correlate with the degree of vertebral slippage?
- A) Numbness in the feet
- B) Severe back pain
- C) Decreased intervertebral space
- D) Difficulty standing upright
Answers
- B) Posterior shift of the center of gravity
- B) Dysplastic
- B) Hamstrings
- B) Georges Herbiniaux, 1782
- B) Grade II
- C) Underlying cause of the condition
- D) Isthmic
- C) Spondylolysis
- B) Hamstrings and abdominal muscles
- B) Severe back pain
Quizz3
- Which diagnostic imaging modality is considered the gold standard for assessing the degree of slippage and structural changes in spondylolisthesis?
- A) X-ray
- B) MRI
- C) CT scan
- D) Ultrasound
- In the context of spondylolisthesis, what does the term “functional instability” refer to?
- A) Pain caused by muscle spasms
- B) Increased vertebral slippage with movement
- C) Decreased range of motion
- D) Static positioning of the vertebrae
- What is the primary surgical intervention recommended for severe spondylolisthesis with neurological deficits?
- A) Anterior discectomy
- B) Posterior decompression and fusion
- C) Percutaneous screw fixation
- D) Laminectomy
- Which grade of Meyerding classification corresponds to a vertebral slippage of 75-100%?
- A) Grade III
- B) Grade IV
- C) Grade V
- D) Grade II
- Which non-surgical treatment modality is often used to manage symptoms in spondylolisthesis?
- A) Spinal fusion
- B) Physical therapy
- C) Epidural steroid injections
- D) Vertebroplasty
- Which biomechanical factor is most commonly associated with the development of isthmic spondylolisthesis in athletes?
- A) Excessive rotation of the lumbar spine
- B) Repetitive forward flexion and extension
- C) Heavy lifting
- D) Prolonged sitting
- In spondylolisthesis, which anatomical structure’s degeneration is most closely associated with the development of degenerative spondylolisthesis?
- A) Intervertebral discs
- B) Facet joints
- C) Lamina
- D) Spinous processes
- What is the primary goal of conservative management for spondylolisthesis?
- A) Eliminate vertebral slippage
- B) Improve functional mobility and reduce pain
- C) Correct spinal curvature
- D) Prevent further slippage
- Which demographic is most commonly affected by degenerative spondylolisthesis?
- A) Young athletes
- B) Elderly women
- C) Middle-aged men
- D) Adolescents
- What is a common physical examination finding in patients with spondylolisthesis?
- A) Positive straight leg raise test
- B) Decreased reflexes in the lower extremities
- C) Tenderness over the spinous processes
- D) Reduced lumbar lordosis
Answers
- C) CT scan
- B) Increased vertebral slippage with movement
- B) Posterior decompression and fusion
- B) Grade IV
- B) Physical therapy
- B) Repetitive forward flexion and extension
- B) Facet joints
- B) Improve functional mobility and reduce pain
- B) Elderly women
- C) Tenderness over the spinous processes
References
- Randall RM, Silverstein M, Goodwin R. Review of Pediatric Spondylolysis and Spondylolisthesis. Sports Med Arthrosc Rev. 2016 Dec;24(4):184-187. [ PubMed ]2.
- Kreiner DS, Baisden J, Mazanec DJ, Patel RD, Bess RS, Burton D, Chutkan NB, Cohen BA, Crawford CH, Ghiselli G, Hanna AS, Hwang SW, Kilincer C, Myers ME, Park P, Rosolowski KA, Sharma AK , Taleghani CK, Trammell TR, Vo AN, Williams KD. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of adult isthmic spondylolisthesis. Spine J. 2016 Dec;16(12):1478-1485. [ PubMed ]3.
- Alqarni AM, Schneiders AG, Cook CE, Hendrick PA. Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review. Phys Ther Sport. 2015 Aug;16(3):268-75. [ PubMed ]4.
- Bouras T, Korovessis P. Management of spondylolysis and low-grade spondylolisthesis in fine athletes. A comprehensive review. Eur J Orthop Surg Traumatol. 2015 Jul;25 Suppl 1:S167-75. [ PubMed ]5.
- Baker JF, Errico TJ, Kim Y, Razi A. Degenerative spondylolisthesis: contemporary review of the role of interbody fusion. Eur J Orthop Surg Traumatol. 2017 Feb;27(2):169-180. [ PubMed ]6.
- Matz PG, Meagher RJ, Lamer T, Tontz WL, Annaswamy TM, Cassidy RC, Cho CH, Dougherty P, Easa JE, Enix DE, Gunnoe BA, Jallo J, Julien TD, Maserati MB, Nucci RC, O’Toole JE, Rosolowski K, Sembrano JN, Villavicencio AT, Witt JP. Guideline summary review: An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2016 Mar;16(3):439-48. [ PubMed ]7.
- Schöller K, Alimi M, Cong GT, Christos P, Härtl R. Lumbar Spinal Stenosis Associated With Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta-analysis of Secondary Fusion Rates Following Open vs Minimally Invasive Decompression. Neurosurgery. 2017 Mar 01;80(3):355-367. [ PubMed ]8.
- Koreckij TD, Fischgrund JS. Degenerative Spondylolisthesis. J Spinal Disord Tech. 2015 Aug;28(7):236-41. [ PubMed ]9.
- Schulte TL, Ringel F, Quante M, Eicker SO, Muche-Borowski C, Kothe R. Surgery for adult spondylolisthesis: a systematic review of the evidence. Eur Spine J. 2016 Aug;25(8):2359-67. [ PubMed ]10.
- Alfieri A, Gazzeri R, Prell J, Röllinghoff M. The current management of lumbar spondylolisthesis. J Neurosurg Sci. 2013 Jun;57(2):103-13. [ PubMed ]


















{kind=link}
{kind=link}