

Understanding Osgood-Schlatter: When Growth Strains the Knee
Osgood-Schlatter disease is a painful condition that usually affects growing adolescents. This condition manifests itself as localized inflammation at the junction of the patellar tendon with the upper part of the tibia, just below the knee. It frequently occurs in young people participating in sporting activities requiring repeated jumps and frequent changes of direction, such as football, basketball or gymnastics. Osgood-Schlatter disease is the result of excessive strain on the patellar tendon during growth, leading to irritation and inflammation at its insertion point.
During adolescent growth, bones and muscles develop rapidly. It is at this stage that the risk of developing Osgood-Schlatter disease is highest. Sports activities that involve sudden movements, frequent jumping, and excessive strain on the knee increase stress on the patellar tendon, contributing to the development of this painful condition.
Symptoms of Osgood-Schlatter disease typically include pain and tenderness at the anterior tibial tubercle, the area where the patellar tendon attaches to the shinbone. The pain may worsen with physical activities, especially when climbing stairs, running, or bending the knee. Often, localized swelling can accompany the pain, and in some cases, a bony bump may form at that location.
Diagnosis of Osgood-Schlatter disease is usually based on clinical examination, medical history, and patient-reported symptoms. Imaging tests such as x-rays may be done to rule out other possible causes of knee pain and confirm the diagnosis.
Treatment for Osgood-Schlatter disease aims to relieve pain, reduce inflammation and allow a gradual return to physical activities. Conservative measures often include rest, application of ice, elevation of the affected knee, and taking nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce discomfort. Stretching and muscle strengthening exercises may be recommended to stabilize the knee and prevent excessive strain on the patellar tendon.
In most cases, Osgood-Schlatter disease improves over time as the adolescent completes the growth phase. However, appropriate symptom management is essential to avoid worsening and ensure optimal recovery.
It is crucial to educate adolescents, their parents and coaches about the prevention of Osgood-Schlatter disease. This may include advice on warming up before physical activity, using appropriate equipment, adopting correct landing techniques when jumping, and limiting the intensity and frequency of workouts.
Synonym : Anterior tibial apophysitis, Anterior tibial growth apophysitis, Osgood’s disease
What Causes Osgood-Schlatter? Growth, Stress, and Biomechanics
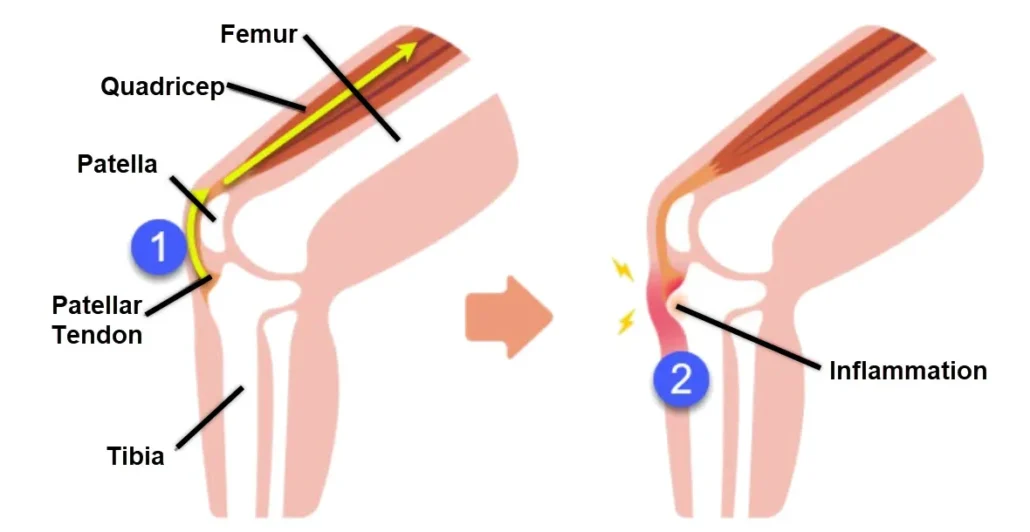
Osgood-Schlatter disease (OSD) is a common condition in adolescents, particularly those who are active in sports. It is characterized by inflammation and pain at the point where the patellar tendon attaches to the tibia (shinbone), just below the kneecap. While the exact cause of OSD is not fully understood, several factors are believed to contribute to its development.
One of the primary causes of OSD is repetitive stress and overuse of the quadriceps muscle and patellar tendon, which occurs during activities that involve running, jumping, or quick changes in direction. These repetitive movements can strain the patellar tendon, leading to inflammation and pain at the site of attachment on the tibia. OSD typically occurs during periods of rapid growth, such as puberty, when bones, muscles, and tendons are undergoing significant changes. During growth spurts, the bones may grow faster than the surrounding muscles and tendons, leading to tension and pulling on the patellar tendon.
This increased tension can contribute to the development of OSD. Imbalances in muscle strength and flexibility, particularly between the quadriceps and hamstrings, can also play a role in the development of OSD. Weakness or tightness in the quadriceps muscles relative to the hamstrings can lead to increased stress on the patellar tendon during physical activity, increasing the risk of injury and inflammation. Certain biomechanical factors, such as abnormal knee alignment or foot mechanics, may predispose individuals to OSD. For example, excessive inward rotation of the knees (known as knee valgus) or flat feet (pronation) can alter the distribution of forces across the knee joint, placing increased stress on the patellar tendon and contributing to OSD. Participation in certain sports that involve repetitive running, jumping, or squatting movements, such as basketball, soccer, volleyball, and gymnastics, is strongly associated with an increased risk of OSD. These activities place greater strain on the patellar tendon and may exacerbate underlying biomechanical issues. While less well-established, there may be a genetic predisposition to OSD, as it tends to run in families.
Certain individuals may inherit structural variations in the bones, muscles, or tendons around the knee joint that increase their susceptibility to developing OSD when exposed to repetitive stress and physical activity. Inadequate warm-up routines or lack of proper stretching before physical activity can also contribute to the development of OSD. Insufficient warm-up may lead to increased stiffness and reduced flexibility in the muscles and tendons, making them more susceptible to injury during exercise. In some cases, OSD may develop following a direct blow to the knee or a previous injury to the patellar tendon. Trauma or microtrauma to the tendon can disrupt its normal structure and function, predisposing it to inflammation and pain with subsequent activity. In summary, Osgood-Schlatter disease is a multifactorial condition caused by a combination of overuse, growth-related changes, muscle imbalances, biomechanical factors, genetic predisposition, sports participation, and inadequate warm-up or stretching practices. Understanding these contributing factors is important for preventing and managing OSD in adolescents who are at risk for this condition.
The main causes and risk factors include:
- Rapid growth: During the period of rapid growth in adolescence, bones can sometimes grow faster than tendons and muscles, leading to increased stress on the tendon insertion areas.
- Sports activities: Adolescents involved in sports such as football, basketball, volleyball, gymnasium, and other high-impact activities may be more likely to develop Osgood-Schlatter disease due to repeated stress on the knee.
- Individual anatomy: Some people may have an anatomy that predisposes them to developing this condition, such as a particular position of the foot, knee, or pelvis.
- Genetic factors: There is a genetic component, and the disease can sometimes occur in members of the same family.
- Gender: Boys are more likely than girls to develop Osgood-Schlatter disease.
Although Osgood-Schlatter disease can cause discomfort and pain, it is usually self-limiting and improves over time, particularly after adolescent growth ends.
Recognizing the Signs: How Osgood-Schlatter Pain Presents
Symptoms of Osgood-Schlatter disease can manifest in various ways, often causing discomfort and limitations in physical activities. This condition primarily affects adolescents, particularly those engaged in sports or activities that involve repetitive stress on the knees. Understanding the symptoms is crucial for timely diagnosis and management.
First and foremost, individuals with Osgood-Schlatter disease commonly experience pain and tenderness below the kneecap. This discomfort typically worsens during activities such as running, jumping, or climbing stairs. The pain may also intensify with direct pressure on the affected area, such as kneeling.
Additionally, swelling and inflammation are hallmark symptoms of Osgood-Schlatter disease. The area around the tibial tuberosity, where the patellar tendon inserts into the shinbone, may appear swollen and feel warm to the touch. This swelling can contribute to the overall discomfort experienced by the individual.
Another prevalent symptom is the presence of a bony bump or prominence at the top of the shinbone, just below the kneecap. This bump, known as the tibial tuberosity, may become more prominent and tender over time as the condition progresses. It is often visible and palpable, serving as a diagnostic indicator for healthcare professionals.
Moreover, individuals with Osgood-Schlatter disease may notice stiffness and limited range of motion in the affected knee. This stiffness can make it challenging to perform certain movements and activities, further impeding physical function and participation in sports or recreational pursuits.
In some cases, the symptoms of Osgood-Schlatter disease may extend beyond the knee region. Patients may experience referred pain, meaning discomfort radiates to adjacent areas such as the thighs or shins. This referred pain can exacerbate the overall discomfort and affect daily activities.
Furthermore, adolescents with Osgood-Schlatter disease may observe changes in their gait or movement patterns. They may alter their posture or adopt compensatory strategies to alleviate discomfort, which can potentially lead to biomechanical imbalances and further exacerbate symptoms over time.
It is important to note that the severity of symptoms can vary among individuals with Osgood-Schlatter disease. While some may experience mild discomfort that resolves with rest and conservative measures, others may endure persistent pain and functional limitations that require medical intervention.
In addition to the physical symptoms, Osgood-Schlatter disease can also have psychological implications for affected individuals, particularly young athletes. Chronic pain and limitations in participation may impact their self-esteem, mood, and overall quality of life, highlighting the importance of holistic management approaches.
Overall, recognizing the symptoms of Osgood-Schlatter disease is essential for accurate diagnosis and appropriate management. Early intervention and targeted treatment strategies can help alleviate discomfort, promote healing, and facilitate a safe return to physical activity for adolescents affected by this condition.
- Knee pain: Pain is usually felt just below the kneecap, where the tendon attaches to the shinbone. The pain can be mild to severe and often gets worse during physical activity.
- Swelling: Slight swelling may be seen around the anterior tibial tuberosity, the sensitive area of the tendon attachment.
- Local redness and warmth: Due to inflammation, the skin around the affected area may become red and hot.
- Tenderness to touch: The anterior tibial tuberosity may be tender to touch, and pressure on this area may cause pain.
- Worsening during activity: Pain tends to get worse during or after physical activities such as running, jumping, or any movement that uses the quadriceps muscles.
- Stiffness: Some individuals may experience stiffness in the knee, especially after a period of inactivity.
- Eventually, a bulge: In more advanced cases, a bony bulge may form at the anterior tibial tuberosity.
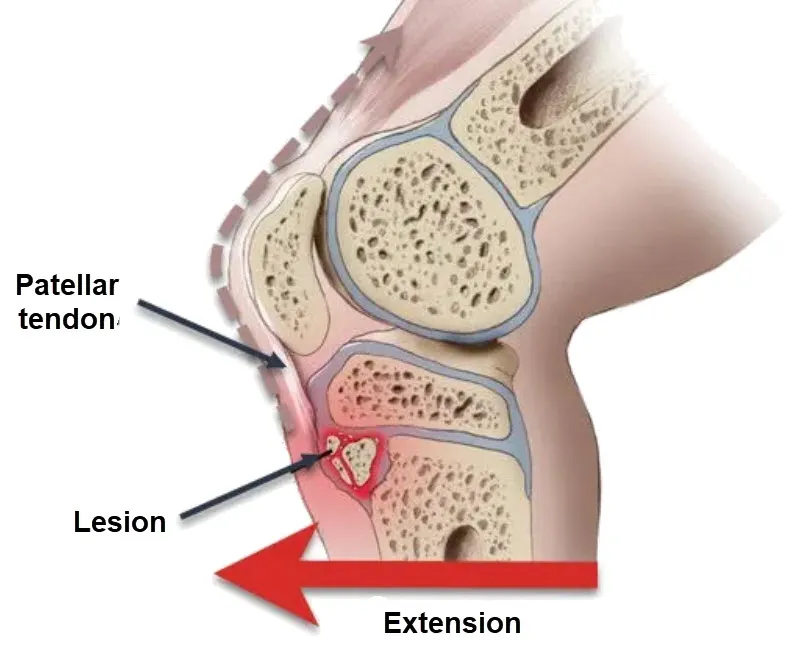
Inside the Knee: The Pathophysiology of Osgood-Schlatter Disease
Understanding the pathophysiology of Osgood-Schlatter disease provides insights into the mechanisms underlying its development and progression. This condition primarily affects the growth plate at the proximal end of the tibia, known as the tibial tuberosity, where the patellar tendon inserts. Several factors contribute to the pathogenesis of Osgood-Schlatter disease, including repetitive stress, growth spurts, and biomechanical factors.
Repetitive stress plays a central role in the pathophysiology of Osgood-Schlatter disease. Adolescents engaged in sports or activities that involve frequent running, jumping, or squatting place repetitive strain on the patellar tendon and its insertion at the tibial tuberosity. This repetitive stress can lead to microtrauma and inflammation at the tendon-bone interface, initiating the pathological cascade characteristic of Osgood-Schlatter disease.
During periods of rapid growth, such as puberty, the bones and soft tissues undergo significant changes to accommodate increased height and muscle mass. Growth spurts can exacerbate the susceptibility of the tibial tuberosity to injury and inflammation, as the growing bones place additional strain on the patellar tendon insertion. This heightened vulnerability to stress during periods of rapid growth contributes to the onset and exacerbation of Osgood-Schlatter disease.
Biomechanical factors also influence the pathophysiology of Osgood-Schlatter disease. Abnormalities in lower limb alignment, muscle imbalances, and poor technique during physical activities can alter the distribution of forces across the knee joint, placing excessive stress on the patellar tendon and tibial tuberosity. These biomechanical abnormalities may predispose individuals to develop Osgood-Schlatter disease or exacerbate existing symptoms.
Microscopic examination of affected tissues in Osgood-Schlatter disease reveals characteristic histopathological changes. Histologically, there is evidence of chronic inflammation, with infiltration of inflammatory cells such as macrophages and lymphocytes into the tendon-bone interface. Additionally, fibrocartilaginous changes may occur, with fibroblasts producing collagen fibers in an attempt to repair the damaged tissue. These histopathological findings reflect the chronic nature of Osgood-Schlatter disease and its inflammatory component.
Furthermore, imaging studies, such as X-rays and magnetic resonance imaging (MRI), can provide valuable insights into the structural changes associated with Osgood-Schlatter disease. X-rays may reveal fragmentation and irregularity of the tibial tuberosity, along with soft tissue swelling and calcifications at the tendon insertion site. MRI can detect edema and inflammation in the patellar tendon and adjacent soft tissues, aiding in the diagnosis and assessment of disease severity.
Ultimately, the pathophysiology of Osgood-Schlatter disease involves a complex interplay of repetitive stress, growth-related changes, and biomechanical factors. Understanding these underlying mechanisms is essential for guiding treatment strategies aimed at alleviating symptoms, promoting healing, and preventing long-term complications. By addressing the root causes of Osgood-Schlatter disease and implementing targeted interventions, healthcare professionals can optimize outcomes for adolescents affected by this condition.
The pathophysiology of Osgood-Schlatter disease primarily involves mechanisms of repeated mechanical stress on the anterior tibial tuberosity in adolescents during periods of rapid growth. Here are the key stages in the pathophysiology of this condition:
- Rapid Growth: Osgood-Schlatter disease usually manifests itself during rapid adolescent growth. During this time, bones, muscles, and tendons may grow at different rates.
- Excessive Patella Tendon Pull: Active adolescents, especially those playing high-impact sports or performing activities requiring repeated jumping and bending movements, may place excessive pull on the patellar tendon.
- Anterior Tibial Tuberosity Irritation: Due to repeated traction, the anterior tibial tuberosity, where the patellar tendon attaches to the tibia, can be subject to constant irritation. This area becomes prone to inflammation and pain.
- Inflammatory Response: Continued irritation causes a local inflammatory response. Immune cells and inflammatory mediators can be recruited to the affected area.
- Reactive Ossification: In response to chronic inflammation, there may be reactive ossification of the anterior tibial tuberosity. This results in an accumulation of additional bone tissue, contributing to the enlargement of the tuberosity.
- Bone Fragmentation: In some cases, traction and increased ossification can lead to the formation of bone fragments around the anterior tibial tuberosity.
- Pain and Symptoms: The combination of inflammation, reactive ossification, and tendon traction can lead to pain, tenderness, and symptoms characteristic of Osgood-Schlatter disease.
Dr. Robert Osgood: The Mind Behind a Landmark Diagnosis
After completing his internship, his first hospital assignment led him to occupy the position of radiologist at the Boston Children’s Hospital in 1902 and 1903. It was during this period that he undertook in-depth observations on the anomalies of growth and trauma related to the tibial tuberosity in adolescents, which were recorded in an article published on January 29, 1903. These alterations have since been referred to as Osgood-Schlatter disease, Dr. Schlatter having also contributed to description of this condition at a later date.
His research findings laid the foundation for the medical understanding of Osgood-Schlatter disease, shedding light on the mechanisms underlying this painful condition that affects the tibial tuberosity in growing adolescents. His work has contributed significantly to the advancement of knowledge in the field of pediatric radiology and orthopedics, providing important perspectives for the diagnosis and management of this specific condition.
It is worth emphasizing that collaboration between physicians, such as that between Dr. Osgood and Dr. Schlatter, has often been crucial to the recognition and in-depth understanding of new medical entities. The joint naming of the disease reflects this collaboration and the lasting impact of their respective contributions on the medical community.
Who’s at Risk? Athletes, Growth Spurts, and Other Triggers
Several risk factors contribute to the development of Osgood-Schlatter disease, a condition primarily affecting adolescents engaged in physical activities. Understanding these risk factors is crucial for identifying individuals who may be more susceptible to this condition and implementing preventive measures accordingly.
One significant risk factor for Osgood-Schlatter disease is participation in sports or activities that involve repetitive stress on the knees. Sports such as soccer, basketball, volleyball, and gymnastics often require running, jumping, and quick changes in direction, placing significant strain on the patellar tendon and its insertion at the tibial tuberosity. The repetitive nature of these movements increases the likelihood of microtrauma and inflammation at the tendon-bone interface, predisposing individuals to Osgood-Schlatter disease.
Adolescents experiencing growth spurts are also at heightened risk of developing Osgood-Schlatter disease. During periods of rapid growth, such as puberty, the bones and soft tissues undergo significant changes to accommodate increased height and muscle mass. This rapid skeletal growth can outpace the development of the surrounding musculature and skeletal structures, leading to biomechanical imbalances and increased stress on the patellar tendon insertion. As a result, adolescents undergoing growth spurts are more susceptible to developing Osgood-Schlatter disease.
Furthermore, certain biomechanical factors can increase the risk of Osgood-Schlatter disease in susceptible individuals. Lower limb alignment abnormalities, such as genu valgum (knock-knees) or excessive foot pronation, can alter the distribution of forces across the knee joint, placing additional strain on the patellar tendon and tibial tuberosity. Muscle imbalances, particularly weakness or tightness in the quadriceps and hamstring muscles, can also contribute to abnormal loading of the knee joint and predispose individuals to Osgood-Schlatter disease.
In addition to biomechanical factors, lifestyle factors may influence the risk of developing Osgood-Schlatter disease. Obesity and excessive body weight can increase the mechanical stress on the knees, exacerbating the strain placed on the patellar tendon insertion. Sedentary behavior and inadequate physical activity levels may also contribute to muscular weakness and imbalance, further predisposing individuals to Osgood-Schlatter disease when they engage in more strenuous activities.
Lastly, genetic predisposition may play a role in the development of Osgood-Schlatter disease. While the precise genetic factors involved remain unclear, studies suggest that certain individuals may have a genetic susceptibility to developing musculoskeletal conditions such as Osgood-Schlatter disease. Family history of the condition or other musculoskeletal disorders may increase an individual’s risk of experiencing similar problems.
Overall, a combination of factors, including participation in high-impact sports, growth-related changes, biomechanical abnormalities, lifestyle factors, and genetic predisposition, contribute to the risk of developing Osgood-Schlatter disease. Identifying and addressing these risk factors through targeted interventions and preventive measures can help reduce the incidence and severity of this condition in adolescents.
- Age and Growth Period: Osgood-Schlatter disease most often occurs in adolescents during their period of rapid growth, usually between ages 10 and 15 in boys and between ages 8 and 13 in girls.
- Gender: Boys are more likely to develop Osgood-Schlatter disease than girls, although this disparity may fade as girls become more active in sports.
- Intensive Physical Activities: Participation in sports that involve frequent jumping, sprinting, and other repetitive movements may increase risk. Sports such as football, basketball, volleyball, and track and field are often associated with Osgood-Schlatter disease.
- Muscle Tension: Activities that cause excessive strain on the patellar tendon, such as repeated jumping, can contribute to the development of this condition.
- Genetic Factors: There are indications that genetic predisposition may play a role in susceptibility to Osgood-Schlatter disease.
- Anatomical Factors: Certain individual anatomical aspects, such as the length of the lower limbs or the conformation of the patella, can also influence the risk.
Preventing Osgood-Schlatter: Tips for Growing Active Teens
Here are some tips that can help reduce the risk of developing Osgood-Schlatter disease:
- Proper warm-up: Before participating in sports activities, make sure you do a proper warm-up. This may include stretching exercises and light exercises to prepare the muscles and tendons for physical activity.
- Muscle strengthening: Strengthen the muscles surrounding the knee, with emphasis on the quadriceps, hamstrings and thigh muscles. A well-balanced training program can help stabilize the knee and reduce pressure on the patellar tendon.
- Managing training intensity: Avoid a sudden or excessive increase in training intensity. It is essential to allow the body to gradually adapt to higher activity levels.
- Reducing high-impact activities: If Osgood-Schlatter disease develops or you are at risk, it may help to temporarily reduce high-impact activities, such as repetitive jumping.
- Using support: Using knee braces or other support devices can help stabilize the knee and reduce strain on the tendon.
- Medical follow-up: If symptoms appear, consult a healthcare professional. A medical evaluation can help establish an appropriate treatment plan, which may include specific recommendations for exercises and activity modifications.
It is important to note that Osgood-Schlatter disease may go away on its own as the adolescent gets older and the bones stop growing. However, proper symptom management and prevention can help minimize discomfort and promote faster recovery.
Not Just Growing Pains: Conditions That Mimic Osgood-Schlatter
- Patellar Tendinitis: Inflammation of the patellar tendon can cause similar symptoms, with pain and tenderness in the kneecap.
- Iliotibial Band Syndrome: This condition results from friction of the fascia lata on the outer condyle of the femur, causing pain on the outside of the knee.
- Osteochondritis Dissecans of the Knee: A condition in which a piece of cartilage and bone breaks away from the knee joint, causing pain and limited mobility.
- Anterior Tibial Tuber Fracture: A fracture of the anterior tibial tubercle can also cause pain in the patella and anterior part of the knee.
- Juvenile Idiopathic Arthritis: A form of arthritis that can affect children and adolescents, causing joint pain and inflammation.
- Bone Tumors: Although rare, bone tumors can cause knee pain in adolescents.
- Patellofemoral Pain Syndrome: A condition characterized by pain around the kneecap, often related to physical activities.
- Prepatellar Bursitis: Inflammation of the prepatellar bursa can cause pain in the front of the knee.
Treating Osgood-Schlatter: From Rest to Rehabilitation
- Rest: It is essential to allow the knee to rest, avoiding physical activities that exacerbate the pain. This may include temporary breaks from high-impact sporting activities.
- Application of Ice: Applying ice to the painful area can help reduce inflammation. It is recommended to apply ice for 15 to 20 minutes, several times a day.
- Compression: Using a compression bandage can help reduce swelling around the anterior tibial tuberosity.
- Elevation: Elevating the leg can also help reduce swelling and promote lymphatic drainage.
- Painkillers and Anti-inflammatories: Over-the-counter medications, such as ibuprofen or acetaminophen, may be taken under the supervision of a healthcare professional to relieve pain and inflammation.
- Stretching and Muscle Strengthening: Targeted stretching and strengthening exercises may be recommended to improve flexibility and muscle strength around the knee.
Exercises That Help: Safe Moves for the Adolescent Knee
- Wall Hamstring Stretch:
- Find a free space near a wall.
- Lie on your back and position yourself near the wall.
- Stretch one leg against the wall while keeping the other leg bent on the floor.
- Feel the stretch in the back of the extended leg.
- Hold for 15 to 30 seconds, then switch legs.
- Standing Calf Stretch:
- Face a wall and place your hands on it.
- Step one foot back, keeping it straight, and bend your front knee.
- Keep your back heel on the ground and feel the stretch in your calf.
- Hold for 15 to 30 seconds, then switch legs.
- Straight leg raise:
- Lie on your back with one leg bent and the other straight.
- Contract your thigh muscles and raise your straight leg toward the ceiling.
- Hold for a few seconds, then lower it.
- Do 10 to 15 repetitions of each leg.
- Quadriceps stretch:
- Stand on one leg and bring the heel of the other toward your butt.
- Hold your foot with your hand, feeling the stretch in the front of the thigh.
- Hold for 15 to 30 seconds, then switch legs.
- Hip extension in prone position:
- Lie on your stomach with your legs straight.
- Raise one leg off the ground by contracting your glutes.
- Hold for a few seconds, then lower it.
- Do 10 to 15 repetitions of each leg.
These stretches can help improve muscle flexibility around the knee. Be sure to perform them gently and gradually, avoiding any sudden movements that could aggravate Osgood-Schlatter disease. If you experience significant pain while stretching, stop immediately and consult a healthcare professional.
What X-rays Reveal: Imaging Clues in Osgood-Schlatter Disease
On an x-ray, signs of Osgood-Schlatter disease may include:
- Enlargement of the Anterior Tibial Tuberosity: The anterior tibial tuberosity, where the patellar tendon attaches to the tibia, may appear enlarged on x-rays. This is due to excessive traction of the tendon, causing irritation and increased ossification of the tuberosity.
- Bone Fragmentation: In some cases, bone fragments may be visible around the anterior tibial tuberosity, resulting from irritation and repeated stress on this area.
- Calcifications: Calcification deposits may be seen near the patellar tendon insertion site on the anterior tibial tuberosity.
- Possibly, An Elevation of the Tuberosity: In more advanced cases, a significant elevation of the anterior tibial tuberosity may be visible on x-rays.
However, it is essential to note that the diagnosis of Osgood-Schlatter disease is not based on radiographic findings alone. The clinical picture, including symptoms and physical examination, is also crucial in making an accurate diagnosis.

This X-ray shows a classic presentation of Osgood-Schlatter disease in the right knee. The red arrow points to a bony prominence on the tibial tuberosity, where the patellar tendon attaches. This enlargement is caused by repetitive stress, leading to inflammation and pain in adolescents, especially those involved in physical activities like running and jumping. The condition is self-limiting, but rest and physical therapy can alleviate symptoms.
Test Your Knowledge: Osgood-Schlatter Quick Quiz
Questionnaire 1
1. What is the main anatomical feature of Osgood-Schlatter disease mentioned in the text?
a) Enlargement of the foot
b) Swelling of the knee
c) Anterior tibial tuberosity
d) Muscle atrophy
e) Fracture of the femur
2. Which sporting activity is particularly associated with the development of Osgood-Schlatter disease according to the text?
a) Swimming
b) Tennis
c) Gymnastics
d) Cycling
e) Running
3. What are the typical symptoms of Osgood-Schlatter disease discussed in the text?
a) Pain in the elbow
b) Tenderness in the ankle
c) Pain when bending the knee
d) Redness and warmth in the back
e) Stiffness in the neck
4. What is the least mentioned risk factor in the development of Osgood-Schlatter disease?
a) Rapid growth
b) Intensive physical activities
c) Genetic factors
d) Advanced age
e) Individual anatomy
5. Who is generally responsible for diagnosing Osgood-Schlatter disease according to the text?
a) Dermatologist
b) Ophthalmologist
c) Dental surgeon
d) General practitioner
e) Radiologist
6. What is the main recommendation for pain relief in the treatment of Osgood-Schlatter disease?
a) Application of heat
b) Rest
c) Massage
d) Intensive exercise
e) Diet rich in sugar
7. What is Dr. Robert Bayley Osgood’s main contribution to the understanding of Osgood-Schlatter disease?
a) Discovery of the responsible virus
b) Development of a revolutionary treatment
c) In-depth observations on growth abnormalities
d) Creation of a vaccine
e) No notable medical contribution
8. What is the most common growing period for the development of Osgood-Schlatter disease?
a) 5-10 years
b) 20-25 years
c) 10-15 years
d) 30-35 years
e) 15-20 years
9. What is the main recommendation for the prevention of Osgood-Schlatter disease according to the text?
a) Avoid all physical activity
b) Use anti-inflammatory medications
c) Avoid warming up before sporting activity
d) Reduce water consumption
e) Strengthen the muscles surrounding the knee
10. What is the role of stretching and muscle strengthening exercises in the treatment of Osgood-Schlatter disease?
a) Worsen symptoms
b) No effect
c) Relieve pain
d) Cause inflammation
e) Replace rest
Answers:
- c) Anterior tibial tuberosity
- c) Gymnastics
- c) Pain during knee flexion
- d) Advanced age
- d) General practitioner
- b) Repos
- c) In-depth observations on growth anomalies
- c) 10-15 years
- e) Strengthen the muscles surrounding the knee
- c) Relieve pain
Questionnaire 2
1. What is Osgood-Schlatter disease also called according to the text? a) Scoliosis b) Arthritis c) Anterior tibial apophysitis d) Osteoporosis e) Herniated disc
2. What is the main symptom of Osgood-Schlatter disease mentioned in the text? a) Migraine b) Pain in the anterior tibial tubercle c) Blurred vision d) Abdominal pain e) Shoulder pain
3. How is Osgood-Schlatter disease usually diagnosed? a) Blood test b) Abdominal ultrasound c) Clinical examination, medical history and x-rays d) Brain scan e) Allergy test
4. What is the growing period during which the risk of developing Osgood-Schlatter disease is highest according to the text? a) Early childhood b) Adolescence c) Adulthood d) Old age e) Preadolescence
5. What advice is given for the prevention of Osgood-Schlatter disease in the text? a) Avoid all physical exercise b) Use crutches at all times c) Consume energy drinks d) Follow a diet high in sugar e) Adopt correct landing techniques when jumping
6. What is the role of stretching and muscle strengthening exercises in the treatment of Osgood-Schlatter disease? a) Worsen symptoms b) No effect c) Relieve pain d) Cause inflammation e) Replace rest
7. What is the main recommendation for pain relief in the treatment of Osgood-Schlatter disease? a) Application of heat b) Rest c) Massage d) Intensive exercise e) Diet rich in sugar
8. What is the least mentioned risk factor in the development of Osgood-Schlatter disease? a) Rapid growth b) Intensive physical activities c) Genetic factors d) Advanced age e) Individual anatomy
9. The main goal of treatment for Osgood-Schlatter disease is to increase pain. (Right wrong)
10. The diagnosis of Osgood-Schlatter disease is usually made by a Dermatologist. (Right wrong)
Answers:
- c) Anterior tibial apophysitis
- b) Pain in the anterior tibial tubercle
- c) Clinical examination, medical history and x-rays
- b) L’adolescence
- e) Adopt correct landing techniques when jumping
- c) Relieve pain
- b) Repos
- d) Advanced age
- Faux
- Faux
Questionnaire 3
- What is the main sporting activity associated with the development of Osgood-Schlatter disease according to the text? a) Swimming b) Tennis c) Basketball d) Golf e) Climbing
- What are the main symptoms of Osgood-Schlatter disease mentioned in the text? a) Headache and nausea b) Anterior tibial tubercle pain, swelling and bony bump c) Shoulder pain and fatigue d) Abdominal pain and fever e) Blurred vision and tenderness to touch
- What mechanism is involved in the development of Osgood-Schlatter disease according to the pathophysiology described in the text? a) Lack of exercise b) Emotional stress c) Rapid growth and excessive strain on the patellar tendon d) Excessive sugar consumption e) Lack of sleep
- What risk factors are mentioned in the text in relation to Osgood-Schlatter disease? a) Eating fruits and vegetables b) Being left-handed c) Rapid growth, intensive sports activities, individual anatomy, genetic factors and male gender d) Wearing glasses e) Practicing meditation
- What is the main recommendation for the prevention of Osgood-Schlatter disease according to the text? a) Drinking lots of coffee b) Doing jumps without warming up c) Using inappropriate shoes d) Adopting correct landing techniques when jumping and limiting the intensity of workouts e) Ignoring signs of pain
Answers:
- c) Basketball
- b) Pain in the anterior tibial tubercle, swelling and bony bump
- c) Rapid growth and excessive tension on the patellar tendon
- c) Rapid growth, intensive sports activities, individual anatomy, genetic factors and male sex
- d) Adopt correct landing techniques when jumping and limit the intensity of training
Scientific References and Further Reading
- Rathleff MS, Straszek CL, Blønd L, Thomsen JL. [Knee pain in children and adolescents]. Weekly Laeger. 2019 Mar 25;181(13) [ PubMed ]2.
- Murphy CE, Kenny CM. Not just for boys: a rare case of symptomatic Osgood-Schlatter disease in a skeletally mature woman. BMJ Case Rep. 2019 Mar 26;12(3) [PMC free article] [PubMed]3.
- Seyfettinoglu F, Köse Ö, Oğur HU, Tuhanioğlu Ü, Çiçek H, Acar B. Is There a Relationship between Patellofemoral Alignment and Osgood-Schlatter Disease? A Case-Control Study. J Knee Surg. 2020 Jan;33(1):67-72. [ PubMed ]4.
- Siddiq MAB. Osgood-Schlatter Disease Unveiled Under High-frequency Ultrasonogram. Cureus. 2018 Oct 04;10(10):e3411. [PMC free article] [PubMed]5.
- Hart E, Meehan WP, Bae DS, d’Hemecourt P, Stracciolini A. The Young Injured Gymnast: A Literature Review and Discussion. Curr Sports Med Rep. 2018 Nov;17(11):366-375. [PubMed]6.
- Midtiby SL, Wedderkopp N, Larsen RT, Carlsen AF, Mavridis D, Shrier I. Effectiveness of interventions for treating apophysitis in children and adolescents: protocol for a systematic review and network meta-analysis. Chiropr Man Therap. 2018;26:41. [PMC free article] [PubMed]7.
- Watanabe H, Fujii M, Yoshimoto M, Abe H, Toda N, Higashiyama R, Takahira N. Pathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer Players: A Prospective Cohort Study. Orthop J Sports Med. 2018 Aug;6(8):2325967118792192. [PMC free article] [PubMed]8.
- Indiran V, Jagannathan D. Osgood-Schlatter Disease. N Engl J Med. 2018 Mar 15;378(11):e15. [PubMed]9.
- Nkaoui M, El Alouani EM. Osgood-schlatter disease: risk of a disease deemed banal. Pan Afr Med J. 2017;28:56. [PMC free article] [PubMed]10.
- Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007 Feb;19(1):44-50. [ PubMed ]11.
- Itoh G, Ishii H, Kato H, Nagano Y, Hayashi H, Funasaki H. Risk assessment of the onset of Osgood-Schlatter disease using kinetic analysis of various motions in sports. PLoS One. 2018;13(1):e0190503. [PMC free article] [PubMed]12.
- Patel DR, Villalobos A. Evaluation and management of knee pain in young athletes: overuse injuries of the knee. Transl Pediatr. 2017 Jul;6(3):190-198. [PMC free article] [PubMed]



 Weakness: Causes, Implications, and Solutions")














{kind=link}