

Introduction to Patellofemoral Syndrome
Ah, patellofemoral syndrome, also known as “Runner’s Knee” or “Patellar Chondromalacia” – it’s like the knee decided to pursue an acting career and wanted its own stage name. “Runner’s knee,” seriously? Sounds like the title of a reality TV show for overactive knees.
Imagine, the kneecap which acts rebellious and decides to go off-piste in the trochlear groove. You know, the kind of journey that even GPS devices avoid. “Let’s take a little detour to the lateral side, just to spice up the life of the femur a little,” she seems to say. And then there’s the drama: friction, crepitus, and the cartilage softening like butter in the sun.
It’s almost as if the kneecap is a capricious star requiring a certain red-carpet quality to every flexion and extension movement. “I will not lower myself if the ground is not perfectly aligned with my high expectations,” she seems to proclaim, causing a crackling sound worthy of a concert of popcorn during a movie screening.
And let’s talk about this term “Chondromalacia”. Sounds more like a rare macaron disease than a knee condition, right? We almost imagine a medical diagnosis followed by a secret prescription to taste macaroons in the shadow of an old castle.
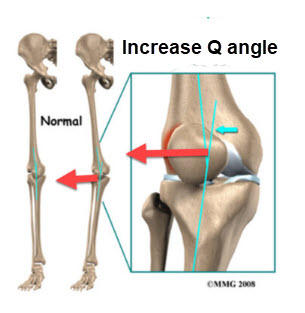
But back to our knees. This is a common phenomenon, especially among women. Ah, the famous female preference for the larger Q angle, as if women were experts in knee geometry. “Sure, Mr. Knee, I’ll show you how to make a Pythagorean Q angle. »
We can almost imagine female knees with a little sign “Warning: Q angle in action”. As if female knees are strutting proudly in a modern art exhibition, displaying their Q angle as the centerpiece of a glamorous collection of body parts.
So, what to do with this patellofemoral syndrome? Perhaps organize a talk show-style intervention where the patella can express itself freely about the pressures exerted by the trochlear groove. “It’s hard out there in the groove, Jerry! »
Ultimately, runner’s knee may not be a movie star, but it’s certainly a star in the medical world. And who knows, maybe with a little humor, this rebellious kneecap could find a way to get back on the right path, or at least, on the right trochlear groove.
Causes of Patellofemoral Syndrome
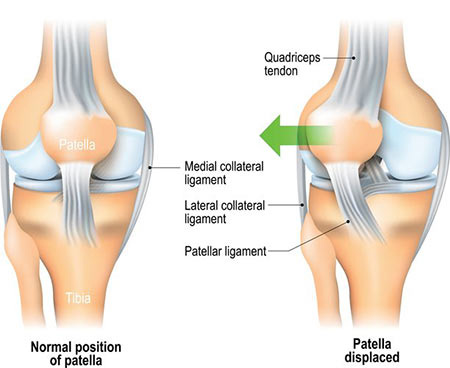
Patellofemoral Syndrome (PFS), commonly known as “Runner’s Knee,” is primarily caused by abnormal tracking of the patella (kneecap) within the femoral groove. This improper movement increases pressure on the patellofemoral joint, leading to irritation, inflammation, and pain. Several factors contribute to the development of PFS, with muscle imbalances, joint misalignment, and biomechanical issues playing a significant role.
1. Muscle Imbalances and Weaknesses
Muscle imbalances, particularly involving the quadriceps, are one of the leading causes of PFS. The quadriceps muscle group, located in the front of the thigh, is responsible for extending the knee and stabilizing the patella. Among the quadriceps muscles, the vastus medialis oblique (VMO) plays a crucial role in maintaining proper patellar tracking. If the VMO is weak compared to the vastus lateralis (on the outer side of the thigh), the patella may be pulled laterally (toward the outer knee), leading to abnormal alignment. This misalignment increases the friction between the patella and the femur, contributing to the pain and irritation characteristic of PFS.
2. Overuse and Repetitive Stress
PFS is often considered an overuse injury, especially among athletes and individuals who engage in repetitive activities like running, cycling, or squatting. These activities place constant pressure on the knee joint, particularly the patellofemoral area. Over time, this repetitive stress can cause irritation and inflammation in the cartilage beneath the patella, leading to the gradual development of PFS. Athletes and individuals with physically demanding jobs are particularly vulnerable to overuse injuries, making PFS a common condition in these populations.
3. Biomechanical Issues
Poor biomechanics, particularly in the lower extremities, can contribute significantly to PFS. One of the most common biomechanical contributors is overpronation (flat feet). Overpronation causes the foot to roll inward excessively when walking or running, which, in turn, affects the alignment of the knee. As the knee compensates for the misaligned foot, abnormal tracking of the patella occurs, increasing the risk of PFS. Other biomechanical issues include poor running form, improper posture, or weak hip muscles, which can affect the alignment of the entire leg and contribute to the condition.
4. Tight Muscles and Connective Tissue
Tightness in muscles and connective tissues, such as the hamstrings, iliotibial (IT) band, or calf muscles, can contribute to abnormal patellar tracking. Tight hamstrings can place additional stress on the knee joint, while a tight IT band can pull the patella laterally, increasing the likelihood of improper alignment. Similarly, inflexible calf muscles can alter gait mechanics, leading to compensatory movements that affect patellar tracking. Stretching and flexibility exercises are often recommended to relieve the tension in these muscle groups and improve knee function.
5. Patellar Malalignment
In some cases, anatomical factors can predispose individuals to PFS. A naturally high-riding patella (patella alta) or a shallow femoral groove can make it more difficult for the patella to stay properly aligned during movement. Additionally, structural differences such as a wider pelvis, which affects the Q-angle (the angle between the hip and knee), can place women at a higher risk of developing PFS. A greater Q-angle can lead to increased lateral pressure on the patella, contributing to its improper tracking.
6. Trauma or Previous Injury
A previous injury to the knee, such as a dislocation or fracture, can also increase the risk of PFS. Trauma to the patella or surrounding tissues can lead to scarring, weakened muscles, or damaged cartilage, all of which contribute to improper patellar movement. Even after the initial injury has healed, the resulting muscle weakness or joint instability can leave the patella more prone to misalignment and the development of PFS symptoms.
7. Improper Footwear or Activity Modification
Wearing improper footwear, particularly shoes that lack adequate support or cushioning, can exacerbate the strain on the patellofemoral joint. Unsupportive shoes can alter gait mechanics and increase the load on the knee, making it more difficult for the patella to track correctly. Additionally, improper modification of activities, such as suddenly increasing running mileage or intensity, can overload the knee joint and contribute to PFS.more
List of causes
- Abnormal Patellar Tracking: One of the primary causes is abnormal patellar tracking, where the kneecap fails to move smoothly within its groove during knee flexion and extension. This misalignment can exert excessive pressure on the cartilage, leading to irritation and eventual breakdown.
- Muscle Imbalances: Weakness or tightness in certain muscle groups around the knee can alter its biomechanics, contributing to patellar malalignment. Weak quadriceps muscles, for instance, may fail to stabilize the patella during movement, while tightness in the IT band or hamstrings can pull the patella off its normal path.
- Overuse or Repetitive Stress: Activities involving repetitive knee movements, such as running, jumping, or cycling, can exacerbate patellar malalignment and increase the risk of cartilage injury. Athletes engaged in sports like basketball or volleyball are especially susceptible due to the repetitive stress placed on their knees.
- Traumatic Injury: Acute trauma to the knee, such as a direct blow or sudden twisting motion, can damage the cartilage and surrounding structures, leading to inflammation and pain. Previous knee injuries, like patellar dislocation or ligament sprains, can also predispose individuals to chondromalacia patellae.
- Biomechanical Factors: Foot pronation (flat feet) or high-arched feet can contribute to abnormal patellar tracking by altering the alignment of the knee joint. Genetic predisposition may play a role in the development of structural abnormalities in the knee joint, increasing the risk of patellar malalignment and cartilage damage.
- Poor Biomechanics: Malalignment of the lower extremities, such as inward rotation of the femur or tibia, can contribute to abnormal patellar tracking and increase the risk of chondromalacia patellae.
- Joint Hypermobility: Individuals with hypermobile joints may experience excessive movement and instability in the knee joint, leading to increased stress on the patellar cartilage.
- Inadequate Warm-Up or Cool-Down: Failing to properly warm up before physical activity or neglecting to cool down afterward can leave the knee joint susceptible to injury and inflammation, predisposing individuals to chondromalacia patellae.
- Muscle Weakness in the Hip: Weakness in the hip abductor and external rotator muscles can alter pelvic alignment and hip stability, indirectly affecting patellar tracking and contributing to knee pain.
- Footwear: Wearing inappropriate footwear or shoes with inadequate support during physical activities can affect lower limb alignment and increase the risk of patellar malalignment and cartilage damage.
- Muscle Tightness in the Quadriceps: Tightness in the quadriceps muscles can pull the patella upwards, increasing pressure on the undersurface of the kneecap and contributing to chondromalacia patellae.
- Age and Degeneration: As individuals age, the cartilage in the knee joint may naturally wear down over time, increasing the likelihood of developing chondromalacia patellae, particularly in older adults.
- Genetic Factors: Certain genetic factors may predispose individuals to structural abnormalities in the knee joint, such as shallow femoral grooves or abnormal patellar shapes, which can increase the risk of patellar malalignment and cartilage damage.
- Overtraining: Engaging in excessive or high-intensity physical activity without adequate rest and recovery can lead to overuse injuries in the knee joint, including chondromalacia patellae.
- Improper Technique: Performing exercises or activities with improper form or technique can place undue stress on the knee joint and contribute to the development of chondromalacia patellae over time.
- Previous Knee Injuries: Individuals who have previously experienced knee injuries, such as ligament sprains or meniscus tears, may have altered joint mechanics and increased susceptibility to developing chondromalacia patellae.
- Excessive Weight: Being overweight or obese can place added stress on the knee joint during weight-bearing activities, leading to accelerated wear and tear on the patellar cartilage and an increased risk of chondromalacia patellae.
- Systemic Diseases: Certain systemic diseases, such as rheumatoid arthritis or juvenile idiopathic arthritis, can cause inflammation within the knee joint, leading to cartilage damage and contributing to the development of chondromalacia patellae.
- Nutritional Deficiencies: Inadequate intake of essential nutrients, such as vitamin D or calcium, necessary for maintaining healthy bone and cartilage integrity, may predispose individuals to cartilage degeneration and chondromalacia patellae.
- Hormonal Changes: Fluctuations in hormone levels, particularly in women during puberty, pregnancy, or menopause, can affect ligament laxity and joint stability, potentially increasing the risk of chondromalacia patellae.
- Sedentary Lifestyle: Prolonged periods of inactivity or sedentary behavior can lead to muscle weakness and stiffness, reducing joint support and increasing the likelihood of developing chondromalacia patellae upon resuming physical activity.
- Occupational Factors: Certain occupations or activities that involve repetitive kneeling, squatting, or heavy lifting may increase the risk of developing chondromalacia patellae due to increased stress on the knee joint over time.
- Environmental Factors: Environmental factors such as uneven surfaces or slippery conditions during physical activities can increase the risk of falls or sudden movements that may injure the knee joint and lead to chondromalacia patellae.
- Neuromuscular Conditions: Neuromuscular conditions, such as cerebral palsy or muscular dystrophy, that affect muscle control and coordination can alter normal joint mechanics and increase the risk of chondromalacia patellae development.
Symptoms of Patellofemoral Syndrome
atellofemoral Syndrome (PFS), often referred to as “Runner’s Knee,” involves pain around the front of the knee due to issues with how the kneecap (patella) moves along the femur. The pathophysiology of this condition is rooted in abnormal tracking of the patella within the femoral groove during movement, leading to increased pressure on the underlying cartilage. This improper alignment causes irritation, inflammation, and eventual softening of the cartilage (chondromalacia), which further exacerbates the symptoms and contributes to progressive pain and discomfort.
One key factor in the development of PFS is biomechanical stress. The patellofemoral joint is subjected to repetitive movements in activities such as running, jumping, or squatting, which increases the load on the joint. In a healthy knee, the patella glides smoothly along the femoral groove, but in PFS, it tends to deviate laterally or medially, leading to excessive friction between the patella and femur. This friction damages the cartilage and triggers pain during activities that require bending or straightening of the knee, such as walking up and down stairs, kneeling, or standing from a seated position.
Muscle imbalances and weaknesses are significant contributors to the abnormal patellar tracking seen in PFS. Weakness in the quadriceps, particularly the vastus medialis oblique (VMO), results in insufficient stabilization of the patella. This causes the patella to drift out of its proper alignment, leading to uneven wear on the cartilage. Tight hamstrings and iliotibial (IT) bands can also exacerbate this condition by pulling on the knee joint and altering its biomechanics. Additionally, poor flexibility in the calves and hips can affect the alignment of the knee joint, contributing to improper tracking of the patella.
Another factor that contributes to the pathophysiology of PFS is improper foot mechanics, such as flat feet (overpronation). Overpronation causes the foot to roll inward excessively during movement, which in turn affects the alignment of the knee and increases stress on the patellofemoral joint. Poor gait mechanics, whether from an abnormal foot structure or improper running form, place the knee under additional strain, further contributing to the misalignment and cartilage damage.
Inflammation is a key aspect of the pathophysiology of PFS. Repeated friction between the patella and femur leads to irritation and inflammation of the synovial tissue and cartilage. This inflammation can cause swelling around the knee joint, which further limits mobility and increases pain. In some cases, prolonged inflammation may result in chronic pain and contribute to the degradation of cartilage over time, making it harder for the joint to repair itself.
If left untreated, PFS can progress to more severe cartilage damage, including full-thickness cartilage loss and osteoarthritis of the patellofemoral joint. This is why early intervention is critical to prevent long-term damage. Treatment often focuses on correcting the underlying biomechanical issues and muscle imbalances that contribute to abnormal patellar tracking. Physical therapy, which includes exercises to strengthen the quadriceps, particularly the VMO, and stretch tight muscle groups, is one of the most effective ways to address the root cause of PFS.
Pathophysiology
atellofemoral Syndrome (PFS), often referred to as “Runner’s Knee,” involves pain around the front of the knee due to issues with how the kneecap (patella) moves along the femur. The pathophysiology of this condition is rooted in abnormal tracking of the patella within the femoral groove during movement, leading to increased pressure on the underlying cartilage. This improper alignment causes irritation, inflammation, and eventual softening of the cartilage (chondromalacia), which further exacerbates the symptoms and contributes to progressive pain and discomfort.
One key factor in the development of PFS is biomechanical stress. The patellofemoral joint is subjected to repetitive movements in activities such as running, jumping, or squatting, which increases the load on the joint. In a healthy knee, the patella glides smoothly along the femoral groove, but in PFS, it tends to deviate laterally or medially, leading to excessive friction between the patella and femur. This friction damages the cartilage and triggers pain during activities that require bending or straightening of the knee, such as walking up and down stairs, kneeling, or standing from a seated position.
Muscle imbalances and weaknesses are significant contributors to the abnormal patellar tracking seen in PFS. Weakness in the quadriceps, particularly the vastus medialis oblique (VMO), results in insufficient stabilization of the patella. This causes the patella to drift out of its proper alignment, leading to uneven wear on the cartilage. Tight hamstrings and iliotibial (IT) bands can also exacerbate this condition by pulling on the knee joint and altering its biomechanics. Additionally, poor flexibility in the calves and hips can affect the alignment of the knee joint, contributing to improper tracking of the patella.
Another factor that contributes to the pathophysiology of PFS is improper foot mechanics, such as flat feet (overpronation). Overpronation causes the foot to roll inward excessively during movement, which in turn affects the alignment of the knee and increases stress on the patellofemoral joint. Poor gait mechanics, whether from an abnormal foot structure or improper running form, place the knee under additional strain, further contributing to the misalignment and cartilage damage.
Inflammation is a key aspect of the pathophysiology of PFS. Repeated friction between the patella and femur leads to irritation and inflammation of the synovial tissue and cartilage. This inflammation can cause swelling around the knee joint, which further limits mobility and increases pain. In some cases, prolonged inflammation may result in chronic pain and contribute to the degradation of cartilage over time, making it harder for the joint to repair itself.
If left untreated, PFS can progress to more severe cartilage damage, including full-thickness cartilage loss and osteoarthritis of the patellofemoral joint. This is why early intervention is critical to prevent long-term damage. Treatment often focuses on correcting the underlying biomechanical issues and muscle imbalances that contribute to abnormal patellar tracking. Physical therapy, which includes exercises to strengthen the quadriceps, particularly the VMO, and stretch tight muscle groups, is one of the most effective ways to address the root cause of PFS.
It is important to note that pathophysiology may vary between individuals, and many of these factors may interact in complex ways.
Classification
- Grade 1 : softening of the knee cartilage, also known as mild chondromalacia
- Grade 2 : a moderate chondromalacia characterized by the presence of soft cartilage with abnormal surface features that suggest early tissue erosion
- Grade 3: thinning of cartilage and deterioration of active tissues
- Grade 4 : patella with severe chondromalacia characterized by significant deterioration of tissue and some exposed bone, increasing the risk of bones rubbing against each other

Pathway to Patellofemoral Syndrome Diagnosis
The following outlines a logical diagnostic pathway, from patient history and physical examination to diagnostic imaging, to ensure a comprehensive and accurate diagnosis.
1. Patient History
The diagnostic process begins with a thorough patient history. The healthcare provider will ask detailed questions regarding the nature of the pain, such as when it began, what activities exacerbate the symptoms, and if there was any associated trauma or injury. Common characteristics of PFS include:
- Anterior Knee Pain: This is typically described as a dull ache behind or around the kneecap.
- Worsening with Activity: Pain increases with activities like running, jumping, squatting, or climbing stairs.
- Pain during Prolonged Sitting: This is known as the “theater sign,” where knee pain increases after sitting for extended periods.
- No Specific Injury: Many patients do not recall any significant injury that triggered the pain; instead, the symptoms tend to develop gradually.
Identifying these symptoms helps distinguish PFS from other causes of knee pain, such as meniscal tears or ligament injuries.
2. Physical Examination
Following the patient history, a physical examination is conducted to further narrow down the diagnosis. During the examination, the healthcare provider will assess:
- Patellar Alignment and Tracking: The provider will observe the movement of the patella as the patient bends and straightens the knee. In PFS, the patella often moves laterally (outward) instead of staying centered within the femoral groove, especially during knee flexion.
- Quadriceps Strength: Muscle imbalances, particularly weakness in the vastus medialis oblique (VMO), can lead to lateral patellar tracking. The strength and function of the quadriceps will be assessed through resisted knee extension and other tests.
- Palpation: The provider will press on different areas around the patella to identify tender spots or areas of inflammation, which are typical in PFS. Pain is often localized around the edges of the kneecap or behind it.
- Patellar Grind Test: In this test, the provider applies downward pressure on the patella while the patient contracts the quadriceps muscle. Increased pain during this test may indicate patellofemoral joint issues, such as PFS.
- Observation of Gait and Biomechanics: The provider will analyze the patient’s walking or running gait to check for abnormal foot mechanics (e.g., overpronation or flat feet) that could contribute to knee malalignment. Hip and ankle mobility will also be assessed, as limited range of motion or improper alignment in these joints can lead to increased stress on the patella.
3. Diagnostic Tests
In most cases, PFS can be diagnosed through clinical evaluation without the need for advanced imaging. However, if the healthcare provider suspects other conditions or if the symptoms do not improve with initial treatment, imaging tests may be ordered to rule out other potential causes of knee pain, such as cartilage damage, arthritis, or bone deformities.
- X-rays: While X-rays are not typically required for PFS, they can be useful to rule out bone abnormalities, patellar malalignment (such as patella alta, where the kneecap sits higher than normal), or degenerative joint diseases.
- MRI (Magnetic Resonance Imaging): An MRI may be used in cases where more detailed imaging is needed to assess cartilage damage or rule out conditions like chondromalacia patellae (softening and breakdown of the cartilage under the kneecap). MRI can also detect subtle changes in the surrounding soft tissue structures.
- CT Scans or Bone Scans: These may be recommended in rare cases where a more detailed assessment of bone structure or metabolic activity is required, though they are not commonly used in the routine diagnosis of PFS.
4. Diagnosis of Exclusion
Patellofemoral Syndrome is often a diagnosis of exclusion, meaning that other potential causes of knee pain must first be ruled out. Conditions like patellar tendinitis, iliotibial band syndrome, meniscal tears, ligament injuries, or early-stage osteoarthritis can present with similar symptoms. After considering these possibilities and ruling them out through history, physical examination, and sometimes imaging, a diagnosis of PFS can be confidently made.
5. Final Diagnosis and Treatment Planning
Once Patellofemoral Syndrome is diagnosed, a treatment plan is created. This often includes physical therapy to strengthen the quadriceps and surrounding muscles, particularly the VMO, and to improve flexibility in tight muscle groups, such as the hamstrings and iliotibial band. Activity modification, footwear adjustments, and biomechanical corrections (such as using orthotics for flat feet) are also important aspects of managing PFS.
Risk factors
- Poor knee biomechanics: Faulty knee biomechanics, such as poor kneecap alignment or joint instability, can contribute to the development of patellofemoral syndrome.
- Muscle weakness: Weakening of the muscles around the knee, particularly the quadriceps and hip stabilizing muscles, can lead to muscle imbalance, increasing the risk of the condition.
- Overuse: Excessive physical activity, especially repetitive movements of the knee, can lead to overuse of the kneecap, contributing to the development of the syndrome.
- Anatomical problems: Some individuals may have anatomical characteristics that increase risk, such as abnormal patellar tilt or poor joint congruence.
- Patellar instability: Patellar instability, where the kneecap tends to move abnormally, is a significant risk factor for patellofemoral syndrome.
- Genetic factors: Some individuals may have a genetic predisposition to develop joint or muscle abnormalities that contribute to the syndrome.
- Age and sex: Patellofemoral syndrome is more common in adolescents and young adults. Additionally, women tend to be at higher risk than men.
- Specific sports activities: Certain sports activities, such as running, jumping, basketball or volleyball, which involve frequent flexion and extension movements of the knee, may increase the risk.
- Flat feet or excessive pronation: Biomechanical problems in the feet, such as flat feet or excessive pronation, can influence the development of the syndrome.
Osteopathy Treatment for Patellofemoral Syndrome (PFS)
Osteopathy is a holistic approach that emphasizes the body’s structural alignment and its relationship to function, making it a highly effective treatment for musculoskeletal disorders like Patellofemoral Syndrome (PFS). This condition involves improper tracking of the patella (kneecap), leading to pain and discomfort in the knee, particularly during activities such as running, walking upstairs, or sitting for extended periods. The goals of osteopathic treatment for PFS are to restore normal patellar tracking, reduce pain, and promote long-term joint health through manual therapies and exercises. Below is an overview of the osteopathic approach to treating Patellofemoral Syndrome:
1. Initial Assessment
Osteopathy starts with a comprehensive assessment to determine the underlying causes of the patient’s knee pain. The practitioner will take a detailed history, including the onset of symptoms, activity level, and any prior injuries. Physical examination will focus on:
- Posture and Gait Analysis: Identifying abnormalities in posture or walking patterns that may contribute to PFS, such as pronation of the foot or pelvic misalignment.
- Range of Motion Testing: Evaluating the mobility of the knee, hip, and ankle joints to identify restrictions that might contribute to patellar misalignment.
- Muscle Strength and Imbalance Testing: Assessing the strength of the quadriceps, hamstrings, hip flexors, and gluteal muscles. In PFS, muscle imbalances—particularly weakness in the vastus medialis oblique (VMO) and hip abductors—are common and contribute to improper patellar tracking.
- Palpation and Observation: Manual palpation of the knee joint to assess tenderness, inflammation, and abnormal tracking of the patella.
2. Manual Osteopathic Techniques
Once the assessment is complete, the osteopath will use a variety of manual techniques to address the specific issues contributing to PFS. These techniques are designed to reduce pain, improve joint mobility, and correct muscle imbalances.
a. Soft Tissue Manipulation
Soft tissue techniques involve gentle massage and stretching to release tension in the muscles and fascia surrounding the knee. Tight muscles, such as the quadriceps, hamstrings, and iliotibial (IT) band, can exacerbate PFS by pulling the patella out of alignment. Osteopathic soft tissue manipulation helps to:
- Relieve tension in the quadriceps and IT band, reducing lateral pull on the patella.
- Improve blood circulation to the knee joint, promoting healing and reducing inflammation.
- Restore normal muscle tone, ensuring balanced patellar movement.
b. Myofascial Release
Myofascial release is a specialized technique aimed at loosening restrictions in the connective tissue (fascia) that surrounds muscles and joints. In PFS, fascial restrictions around the knee can contribute to abnormal patellar tracking. By gently stretching and releasing these fascial tight spots, the osteopath can improve knee joint mobility and reduce pain.
c. Joint Mobilization
Joint mobilization techniques involve the controlled movement of the knee, hip, and ankle joints to improve their range of motion. For PFS, the osteopath may focus on:
- Mobilizing the knee joint to promote better patellar tracking within the femoral groove.
- Addressing hip joint restrictions, as limited hip mobility can lead to compensatory movements that affect the knee.
- Mobilizing the ankle joint, particularly in patients with flat feet or other biomechanical abnormalities, to improve alignment and reduce stress on the knee.
d. Muscle Energy Techniques (MET)
Muscle energy techniques are a form of active manual therapy in which the patient engages in gentle isometric contractions against the osteopath’s resistance. This helps to improve muscle strength and flexibility while reducing muscle imbalances. In PFS, MET can be particularly effective for:
- Strengthening the VMO, which plays a crucial role in stabilizing the patella.
- Releasing tight hip flexors and hamstrings that may be contributing to patellar misalignment.
- Improving flexibility and range of motion in the affected knee.
e. Lymphatic Drainage
Osteopaths may also use lymphatic drainage techniques to reduce inflammation and swelling around the knee. These gentle techniques stimulate the body’s natural lymphatic system, which helps remove excess fluid and waste products from the inflamed area, promoting faster recovery.
3. Rehabilitation and Strengthening Exercises
In addition to manual treatments, osteopathic treatment for PFS often includes a rehabilitation plan focused on strengthening weak muscles and stretching tight muscles. The goal is to correct muscle imbalances that contribute to abnormal patellar tracking.
a. Quadriceps Strengthening
One of the most important aspects of PFS rehabilitation is strengthening the quadriceps, especially the VMO. Exercises such as straight leg raises, squats, and lunges are prescribed to target this muscle group. A strong VMO helps to stabilize the patella and prevent it from shifting laterally.
b. Hip and Core Strengthening
Hip and core muscles play a significant role in maintaining proper alignment of the knee during movement. Weakness in the hip abductors and external rotators can cause the knee to collapse inward, increasing the risk of PFS. Osteopathic rehabilitation includes exercises such as clamshells, side-lying leg raises, and bridges to strengthen the hip and core muscles.
c. Flexibility Exercises
Stretching tight muscle groups is equally important in treating PFS. The osteopath will guide the patient through stretches for the quadriceps, hamstrings, calf muscles, and IT band. This helps to relieve tension on the knee joint and restore proper movement patterns.
4. Posture and Gait Correction
Many patients with PFS have biomechanical issues related to their posture or gait. Osteopathic treatment includes gait retraining and posture correction exercises to address these issues. This may involve:
- Footwear Recommendations: Patients with flat feet or other foot abnormalities may benefit from custom orthotics to improve their foot alignment and reduce stress on the knees.
- Gait Retraining: For runners, gait retraining techniques can help reduce excessive loading on the knees by promoting a more efficient running style.
5. Patient Education and Activity Modification
Osteopaths also focus on educating patients about their condition and how to prevent further injury. This includes advice on modifying activities that may aggravate PFS, such as running on hard surfaces or climbing stairs. The patient will learn proper warm-up and cool-down techniques to protect their knees during physical activity.
Role of Biomechanics in Patellofemoral Syndrome
Biomechanics plays a crucial role in patellofemoral syndrome, as it studies the mechanisms and movements of the body, especially those related to joint mechanics. In patellofemoral syndrome, biomechanics is often used to understand the forces acting on the kneecap and femur, as well as the movements that may contribute to the development and persistence of symptoms. Here are some aspects of biomechanics related to patellofemoral syndrome:
- Patella Tracking: Biomechanics helps evaluate how the patella follows the normal trajectory during knee movements. Improper tracking, where the kneecap moves out of its normal path, can cause excessive friction and stress, contributing to the syndrome.
- Quadriceps Angle: The angle formed by the quadriceps and patellar tendon is an important aspect. An abnormal angle can put increased pressure on the kneecap, contributing to irritation and pain.
- Forces on the Knee: Biomechanics evaluates the forces that pass through the knee during activities. Excessive or poorly distributed forces can contribute to stress on the kneecap, worsening symptoms.
- Knee Movements: Biomechanical analysis helps evaluate knee movements during walking, running or other activities. Certain movement patterns can increase the risk of chafing and discomfort.
- Muscle Deficits: Biomechanics can be used to identify specific muscle deficits, such as imbalances between the quadriceps muscles or gluteal muscles, which may contribute to the syndrome.
- Posture Assessment: A biomechanical analysis of overall posture can help identify imbalances that could influence knee mechanics.
- Loads during Physical Activity: For active people, biomechanics assesses how loads are distributed during specific activities, contributing to the planning of a suitable exercise program.
Preventative Measures for Patellofemoral Syndrome
Preventing Patellofemoral Syndrome (PFS) is essential for individuals prone to knee pain or those who engage in activities that place repetitive stress on the knees. By focusing on muscle strengthening, stretching, correcting biomechanical issues, and improving overall movement patterns, you can reduce the likelihood of PFS developing or recurring. Below are key preventative measures:
1. Strengthening and Stretching Exercises
A proper exercise regimen can significantly reduce the risk of developing PFS by correcting muscle imbalances and improving the flexibility of tight muscles. Key exercises include:
a. Quadriceps Strengthening
Strengthening the quadriceps, particularly the vastus medialis oblique (VMO), is vital for maintaining proper patellar tracking. Weakness in the quadriceps can cause the patella to move laterally, leading to increased friction in the joint. Exercises such as straight leg raises, wall squats, and step-ups help target the quadriceps. These exercises should be done with proper form to avoid further injury.
b. Glute and Hip Strengthening
The hips play a crucial role in stabilizing the knees. Weak hip muscles, particularly the hip abductors and external rotators, can cause the knee to collapse inward during activities like running or squatting. Strengthening the gluteus medius and hip stabilizers through exercises like side-lying leg raises, clamshells, and band walks can help improve knee alignment.
c. Hamstring and Calf Flexibility
Tight hamstrings and calf muscles can limit the range of motion in the knee, contributing to improper patellar tracking. Stretching these muscles regularly helps reduce tension around the knee joint. Hamstring stretches, calf stretches, and yoga poses that promote lower body flexibility, such as downward-facing dog, are effective ways to improve flexibility.
d. Iliotibial Band (IT Band) Stretching
The IT band runs along the outer thigh and can contribute to lateral patellar movement when tight. Foam rolling the IT band and performing specific IT band stretches can help relieve tension and improve knee mechanics. A common IT band stretch involves crossing one leg over the other while leaning sideways to stretch the outer hip and thigh.
By combining strengthening and stretching exercises, you can create a balanced approach that reduces the risk of overloading certain muscles, while ensuring that others are strong enough to support proper knee function.
2. Footwear and Orthotic Adjustments
Proper footwear is essential for preventing PFS, especially for individuals with abnormal foot mechanics, such as overpronation (flat feet) or high arches. Inappropriate footwear can alter the alignment of the knee, increasing stress on the patellofemoral joint.
a. Supportive Footwear
Wearing shoes with proper arch support and cushioning helps distribute forces more evenly through the lower extremities, reducing pressure on the knees. Individuals with flat feet or high arches should choose footwear that offers corrective support. Running or athletic shoes specifically designed for your foot type can help improve gait mechanics and reduce stress on the knees.
b. Orthotic Devices
In some cases, custom orthotics or over-the-counter shoe inserts may be recommended to correct foot abnormalities. Orthotics help to align the foot and ankle, which can, in turn, improve knee alignment and reduce patellar maltracking. For example, those with overpronation may benefit from arch support orthotics to prevent the inward collapse of the knee. Working with a podiatrist or orthopedic specialist to obtain properly fitted orthotics is essential for long-term relief.
c. Shock-Absorbing Insoles
For individuals who engage in high-impact activities like running, shock-absorbing insoles can help reduce the load on the knees. These insoles help to cushion the impact of repetitive foot strikes, which can reduce the risk of developing PFS, particularly in individuals who run or exercise on hard surfaces.
3. Gait Correction for Long-Term Relief
Gait refers to the pattern of how a person walks or runs, and abnormal gait mechanics can be a major contributor to PFS. Gait correction, often through physical therapy, can help prevent PFS by addressing movement patterns that place excessive strain on the knees.
a. Gait Analysis
A professional gait analysis, typically conducted by a physical therapist or sports medicine specialist, can identify biomechanical issues that contribute to PFS. This analysis involves observing your walking or running patterns, either visually or with the help of video analysis, to assess how your feet, ankles, knees, and hips move. Based on the results, the specialist can recommend corrective strategies.
b. Improving Running Form
For runners, poor form can exacerbate knee issues. Techniques such as shortening stride length, landing softly on the mid-foot rather than the heel, and maintaining proper posture can help reduce knee stress. A running coach or physical therapist can assist in retraining your running gait to minimize the risk of PFS.
c. Posture Correction
Poor posture, particularly in the hips or lower back, can affect the alignment of the lower body. A forward-tilted pelvis, for example, can increase stress on the knees during movement. Correcting these postural issues through targeted exercises and manual therapy can improve overall biomechanics, reducing the likelihood of PFS.
Radiographic Signs of Patellofemoral Syndrome (PFS)
While X-rays are often used as part of the diagnostic process for Patellofemoral Syndrome (PFS), they typically do not reveal early-stage soft tissue issues, as cartilage and tendons are not visible. However, in moderate to advanced stages of PFS or when there is structural damage, X-rays can provide important information. These imaging signs help clinicians assess the alignment and overall health of the patellofemoral joint, including factors that may contribute to improper patellar tracking.
Here are some key X-ray signs associated with Patellofemoral Syndrome:
1. Patellar Malalignment
One of the most common X-ray findings in PFS is patellar malalignment. This occurs when the patella does not sit correctly within the trochlear groove of the femur, causing pain and improper tracking during movement. In PFS, the patella may shift laterally (to the outside), a condition known as lateral patellar displacement. Lateral displacement can be identified through specific X-ray views, such as the Merchant view or sunrise view, where the knee is bent, allowing for a clearer assessment of the patella’s position within the femoral groove.
2. Patella Alta or Patella Baja
X-rays can also show whether the patella is abnormally positioned either too high or too low. These conditions are referred to as patella alta (high-riding patella) and patella baja (low-riding patella), respectively. Both conditions can disrupt normal patellar tracking. Patella alta places the kneecap at a mechanical disadvantage, leading to increased stress on the cartilage and greater susceptibility to PFS. Patella baja can also cause abnormal pressure within the joint, aggravating patellofemoral pain.
To assess patellar height, a lateral X-ray view is typically used, and the Insall-Salvati ratio (a ratio between the patella’s length and the patellar tendon) is measured. If the ratio is too high, it suggests patella alta, while a low ratio indicates patella baja.
3. Trochlear Dysplasia
Trochlear dysplasia refers to an abnormality in the shape or depth of the trochlear groove where the patella moves. Individuals with a shallow or flat trochlear groove are more likely to experience patellar instability, which contributes to the development of PFS. X-rays, particularly lateral and axial views, can help detect trochlear dysplasia. The groove may appear shallower than normal, increasing the likelihood of patellar dislocation or subluxation (partial dislocation).
4. Joint Space Narrowing
Joint space narrowing is a sign of cartilage degeneration, which can occur in cases of chronic PFS. As the cartilage under the patella wears down due to repeated stress or improper tracking, the space between the patella and femur may narrow. This narrowing indicates that the cushioning effect of the cartilage is reduced, leading to increased bone-on-bone contact, pain, and inflammation.
X-rays showing joint space narrowing can suggest more advanced patellofemoral cartilage damage, which may lead to conditions like chondromalacia patellae or patellofemoral osteoarthritis. These conditions are often associated with more severe or long-term PFS cases.
5. Osteophytes (Bone Spurs)
In advanced cases of PFS or when there is chronic stress on the patellofemoral joint, osteophytes (bone spurs) can develop along the edges of the patella or femoral groove. These bony outgrowths form as a result of the body’s attempt to repair the joint, often in response to cartilage damage or misalignment. Osteophytes can be visible on X-rays and are typically associated with longer-term joint degeneration.
Bone spurs can contribute to pain and further restrict the movement of the patella, aggravating the symptoms of PFS. When osteophytes are present, they indicate a more advanced stage of the syndrome, where conservative treatment options may be less effective.
6. Sclerosis or Subchondral Bone Changes
Sclerosis refers to the hardening or thickening of the subchondral bone (the layer of bone just beneath the cartilage). In PFS, chronic irritation of the cartilage can lead to increased stress on the subchondral bone, resulting in its thickening or hardening, which can be visible on X-rays.
Sclerosis is often seen in conjunction with cartilage damage and may indicate that the joint is trying to adapt to the loss of normal cartilage. This is a sign of more advanced joint degeneration and can also suggest the presence of chondromalacia patellae or early osteoarthritis in the patellofemoral joint.
7. Articular Cartilage Calcification
In some cases, X-rays may reveal calcification within the articular cartilage or the surrounding tissues. Calcification is a sign of chronic joint irritation or degenerative changes, and it can contribute to joint stiffness and pain in patients with PFS. While this is less commonly seen on X-rays, its presence often correlates with more advanced stages of cartilage damage.

FAQs on Patellofemoral Syndrome
Common Concerns and Questions
- What causes Patellofemoral Syndrome? Patellofemoral Syndrome is caused by improper tracking of the patella (kneecap) in the femoral groove, often due to muscle imbalances, overuse, biomechanical issues, or previous injuries.
- How is PFS diagnosed? Diagnosis is typically made through clinical examination, patient history, and sometimes imaging (X-rays or MRI) to rule out other knee conditions.
- What are the primary symptoms? The main symptom is pain around or behind the kneecap, especially during activities such as running, squatting, or climbing stairs.
- Can Patellofemoral Syndrome heal on its own? Mild cases can improve with rest, physical therapy, and strengthening exercises. However, chronic or severe cases may require more comprehensive treatment.
- Is PFS common in athletes? Yes, athletes who engage in repetitive activities like running or jumping are at a higher risk due to overuse of the knee joint.
- What are the best exercises for PFS? Strengthening the quadriceps, especially the vastus medialis oblique (VMO), along with hip and core strengthening exercises, are critical. Stretching the hamstrings, calves, and iliotibial (IT) band is also beneficial.
- Can I continue running with PFS? Continuing high-impact activities like running can exacerbate symptoms. Modifying activities and performing rehabilitative exercises are recommended until the condition improves.
- What role does footwear play? Proper footwear that offers support and shock absorption can help reduce the impact on the knees and prevent further irritation.
Long-Term Prognosis
The long-term prognosis for Patellofemoral Syndrome varies depending on the severity and the individual’s commitment to treatment. With proper management, including physical therapy, strength training, and activity modification, most individuals can expect to recover fully. However, neglecting treatment can lead to chronic pain or further cartilage damage, which may increase the risk of developing conditions like osteoarthritis. Preventative measures, such as maintaining muscle strength and flexibility, are essential for reducing the risk of recurrence. In severe or untreated cases, surgical intervention may be required, but this is typically reserved for cases that do not respond to conservative treatment.
Conclusion
Patellofemoral Syndrome, or “Runner’s Knee,” is a condition where pain occurs at the front of the knee, often due to improper patellar alignment or overuse. Early intervention, including rest, physical therapy, and corrective exercises, can prevent further deterioration of the cartilage beneath the kneecap. Strengthening the muscles around the knee and addressing biomechanical factors are crucial in both treatment and prevention. Long-term maintenance, including regular exercise and proper body mechanics, can significantly reduce the recurrence of symptoms and support joint health.
References
References
- Collins NJ, Barton CJ, van Middelkoop M, Callaghan MJ, Rathleff MS, Vicenzino BT et al. 2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain : recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017. Br J Sports Med 2018; 52(18): 1170-1178. [ PubMed ]
- Crossley KM, Stefanik JJ, Selfe J, Collins NJ, Davis IS, Powers CM et al. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester . Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med 2016; 50(14): 839-843. [ PMC free article ] [ PubMed ]
- Hart HF, Barton CJ, Khan KM, Riel H, Crossley KM. Is body mass index associated with patellofemoral pain and patellofemoral osteoarthritis? A systematic review and meta-regression and analysis . Br J Sports Med 2017; 51(10): 781-790. [ PubMed ]
- Nascimento LR, Teixeira-Salmela LF, Souza RB, Resende RA. Hip and Knee Strengthening Is More Effective Than Knee Strengthening Alone for Reducing Pain and Improving Activity in Individuals With Patellofemoral Pain: A Systematic Review With Meta-analysis . J Orthop Sports Phys Ther 2018; 48(1): 19-31. [ PubMed ]
- Neal BS, Lack SD, Lankhorst NE, Raye A, Morrissey D, van Middelkoop M. Risk factors for patellofemoral pain: a systematic review and meta-analysis . Br J Sports Med 2019; 53(5): 270-281. [ PubMed ]
- Robertson CJ, Hurley M, Jones F. People’s beliefs about the meaning of crepitus in patellofemoral pain and the impact of these beliefs on their behavior: A qualitative study . Musculoskelet Sci Pract 2017; 28:59-64. [ PubMed ]
- Rogan S, Haehni M, Luijckx E, Dealer J, Reuteler S, Taeymans J. Effects of Hip Abductor Muscles Exercises on Pain and Function in Patients With Patellofemoral Pain: A Systematic Review and Meta-Analysis . J Strength Cond Res 2018; 33(11): 3174-3187. [ PubMed ]
- Scali K, Roberts J, McFarland M, Marino K, Murray L. Is multi-joint or single joint strengthening more effective in reducing pain and improving function in women with patellofemoral pain syndrome? A systematic review and meta-analysis . Int J Sports Phys Ther 2018; 13(3): 321-334. [ PMC free article ] [ PubMed ]
- Smith BE, Moffatt F, Hendrick P, Bateman M, Rathleff MS, Selfe J et al. The experience of living with patellofemoral pain-loss, confusion and fear-avoidance: a UK qualitative study . BMJ Open 2018; 8(1): e018624. [ PMC free article ] [ PubMed ]
- Smith BE, Selfe J, Thacker D, Hendrick P, Bateman M, Moffatt F et al. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis . PLoS One 2018; 13(1): e0190892. [ PMC free article ] [ PubMed ]
- Van der Heijden RA, Lankhorst NE, van Linschoten R, Bierma‐Zeinstra SM, van Middelkoop M. Exercise for treating patellofemoral pain syndrome . Cochrane Database Syst Rev 2015; (1): CD010387. [ PubMed ]




 Weakness: Causes, Implications, and Solutions")













{kind=link}