

Introduction
Acute whiplash is a constellation of symptoms including nonradicular neck pain that spreads nondermatomally into the shoulders and interscapular region; Often, headaches accompany these symptoms. The trapezius is commonly affected, causing muscle spasms and limited range of motion of the cervical spine. Typically, whiplash results from trauma to the cervical spine and associated soft tissues, but it can also occur without an obvious precipitating event.
Given that more than 93% of the world’s population uses a smartphone, it is not surprising to see an increasing incidence of neck sprains due to poor posture while looking at the smartphone screen. The relationship between cervical spine angle and device screen can be quantified using a cumulative average of neck tilt angles over time. If the observed tilt angle is excessive, significant stress is placed on the cervical spine and soft tissues. The pathological lesions responsible for these symptoms can be evaluated by considering the sternocleidomastoid muscle.
Symptoms of acute whiplash, such as pain, muscle spasms, and limitation of movement, may be exacerbated by sudden neck movements or prolonged poor posture. People who spend long hours staring at their smartphone in a downward tilted position may experience increased tension in the cervical region, which contributes to the development of this condition.
Modern technology, particularly the widespread use of smartphones, has introduced new challenges to neck health. The increasing incidence of posture-related whiplash highlights the importance of raising awareness for conscious use of electronic devices. Ergonomic advice and behavioral changes can help mitigate the risk of developing whiplash from prolonged smartphone use.
To assess the potential impact on the cervical spine, it is essential to understand the relationship between neck angle and the smartphone screen. Users should be aware of the risks associated with prolonged posture and adopt habits that reduce strain on the cervical spine. Regular breaks, neck stretching exercises, and ergonomic adjustments can play a crucial role in preventing whiplash related to smartphone use.
Causes of acute whiplash
Acute whiplash strains, often associated with accidents such as automobile collisions, falls, or sports injuries, are injuries that affect the ligaments of the neck. Understanding the causes of these acute whiplash injuries is crucial for accurate assessment and appropriate management.
The first and most common cause of an acute whiplash is a sudden movement of the neck, usually in a direction of rapid flexion and extension. This commonly occurs in car accidents where the head is suddenly propelled forward and then backward, creating excessive strain on the cervical ligaments. Sports trauma, particularly in activities like football or rugby, can also cause rapid movements of the neck leading to sprains.
Falls, whether they occur head-on on the ground or during a slip, can also be a significant cause of acute whiplash. The impact of the fall can force the neck into an unnatural position, leading to ligament damage. Falls on ice, uneven sidewalks or stairs are common scenarios where such injuries can occur.
Another major contributing factor is playing high-risk sports without adequate protective equipment. Extreme sports, such as motocross or bungee jumping, can expose the neck to significant forces, increasing the risk of acute whiplash injuries.
Diving accidents, especially when the head hits the water at high speed, can cause sudden neck movements that can cause whiplash. Reckless diving into unfamiliar areas can also lead to acute neck injuries due to the presence of rocks or obstacles below the water surface.
Environmental factors such as extreme weather conditions can also contribute to acute whiplash. For example, reckless driving on icy or snowy roads can lead to collisions, increasing the risk of neck injuries.
Aside from trauma, daily activities can also play a role in acute whiplash. Prolonged poor posture, especially when using electronic devices, can place excessive pressure on the neck, increasing the vulnerability of the cervical ligaments.
It is essential to note that susceptibility to whiplash may vary from person to person depending on various factors such as neck muscle strength, flexibility, and general physical condition. People with previous whiplash injuries may be more likely to develop this injury in the future.
- Physical Trauma: Direct trauma, such as a car accident, fall, or sudden impact, can lead to an acute whiplash injury. During these events, the head may experience sudden movements of flexion, extension or rotation, putting excessive strain on the muscles, tendons and ligaments of the neck.
- Poor Posture: Improper posture, especially during prolonged activities such as using a smartphone with the head tilted downward, can contribute to the development of an acute whiplash injury. This prolonged position can cause excessive strain on the neck structures, causing pain and discomfort.
- Repetitive Activities: Repetitive neck movements, such as those performed in certain occupations or during daily activities, can contribute to excessive wear and tear on cervical structures, increasing the risk of sprains.
- Muscle Stress: Excessive muscle stress due to strenuous physical activities, sudden movements or awkward postures can also be a cause of acute whiplash.
- Lifestyle Factors: Lifestyle habits such as a sedentary lifestyle, lack of exercise, being overweight and smoking can contribute to fragile neck structures, increasing susceptibility to whiplash.
- Genetic Predisposition: Some people may have a genetic predisposition to musculoskeletal conditions, which may influence the likelihood of developing a whiplash in response to triggering factors.
- Occupational Factors: Certain occupations may result in increased exposure to the risk of whiplash. Workers performing repetitive tasks, those who carry heavy loads inappropriately, or those who are exposed to constant vibration may be more likely to develop neck strain.
- Pre-Existing Conditions: Pre-existing medical conditions, such as cervical arthritis, can weaken neck structures, increasing vulnerability to sprains.
- Sports Accidents: Sports activities, especially those that involve sudden movements, impacts or falls, can increase the risk of acute whiplash.
- Anatomical Defects: Congenital or acquired anatomical abnormalities of the cervical spine can contribute to instability or excessive strain, increasing the risk of sprains.
- Age: Natural aging can lead to degeneration of intervertebral discs and joints, making cervical structures more susceptible to injury.
- Environmental Conditions: Environmental conditions such as stressful work conditions, lack of workplace ergonomics, or physically restrictive environments can contribute to excessive neck strain.
- Mechanical Conditions: Mechanical disorders of the cervical spine, such as joint instability, may predispose to acute whiplash.
Symptoms of acute whiplash
This injury generally occurs following a sudden movement of the neck, often during an accident, and it can cause various clinical manifestations. It is important to note that symptoms may appear immediately after the traumatic incident or appear gradually over time.
Neck pain is one of the most characteristic symptoms of an acute whiplash. This pain may be localized at the base of the neck or extend up to the shoulders. It can range from mild to intense, and some people describe it as a feeling of stiffness or muscle tension.
Neck stiffness is commonly observed in individuals suffering from an acute whiplash injury. This stiffness can make neck mobility difficult, limiting the ability to turn the head or perform tilting movements. The neck muscles may also have increased sensitivity, worsening the stiffness you feel.
Inflammation of the tissues around injured ligaments is another common symptom. This inflammation may manifest as visible swelling in the neck, creating a feeling of warmth and sensitivity to the touch. Swelling can contribute to the general discomfort associated with whiplash.
Headaches are often reported by people suffering from an acute whiplash injury. These headaches are usually felt at the base of the skull and can be described as persistent, shooting pain. Headaches can be exacerbated by neck movements or prolonged standing in a certain position.
Feelings of dizziness or dizziness may also accompany an acute whiplash injury. This may be related to the disruption of the body’s natural balance due to the neck injury. Affected people may feel unsteady or light-headed.
In some cases, neurological symptoms may occur. This includes numbness or tingling that radiates to the arms, shoulders, or even the face. These symptoms may indicate irritation of the cervical nerves and require immediate medical attention.
It is crucial to emphasize that while these symptoms can be seen in cases of acute whiplash, each person may have variations in how these symptoms manifest. Additionally, some individuals may only experience mild symptoms, while others may experience severe pain and significant discomfort.
- Neck Pain: Neck pain is the most common symptom. It may be localized or spread to other areas, such as the shoulders, base of the skull or upper back.
- Muscle Stiffness: Neck muscles may experience stiffness, limiting range of motion. This stiffness can make it difficult to turn or tilt the head sideways.
- Headaches: Headaches, often felt in the back of the head, can accompany neck pain. These headaches are usually described as pressure or tension.
- Muscle Spasms: Muscle spasms in the cervical region may occur in response to inflammation and muscle tension, contributing to stiffness.
- Numbness or Tingling: Some individuals may experience numbness or tingling sensations in the neck, shoulders, or even arms. This can result from irritation of the nerves.
- Fatigue: Constant pain and muscle tension can lead to general fatigue, affecting overall well-being.
- Sensitivity to Touch: The affected area may become tender to touch, and palpation may intensify the pain.
- Difficulty Sleeping: Neck pain can make it difficult to find a comfortable position to sleep, leading to sleep disturbances.
Pathophysiology
The pathophysiology of acute whiplash provides complex insight into the mechanisms underlying these traumatic neck injuries. These sprains usually occur as a result of a sudden force that causes excessive movement of the neck, stretching or tearing the cervical ligaments. The pathophysiology of these injuries can be broken down into several key stages, highlighting the anatomical and functional changes that occur in cervical structures.
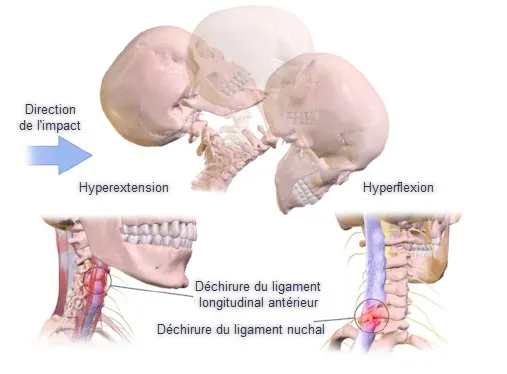
The initial event in the pathophysiology of an acute whiplash is usually trauma, such as a car accident, a fall, or sports trauma. This trauma causes the neck to suddenly move in a particular direction, often hyperflexion or hyperextension.
At the anatomical level, the cervical ligaments, which are responsible for the stability of the cervical spine, experience excessive tension during sudden movement. Ligaments can be stretched beyond their elastic limit, resulting in microtears or, in more severe cases, a complete tear.
The neck muscles, which also play a crucial role in maintaining cervical stability, can be overused during an acute whiplash injury. This muscle overuse can lead to muscle spasms, adding to the pain and stiffness associated with this injury.
The joints between the cervical vertebrae can also be impacted. The forces generated during an acute whiplash can cause joint subluxations or dislocations, leading to an alteration of the normal alignment of the cervical vertebrae.
In response to these injuries, inflammation develops in the affected area. Inflammation is a natural reaction of the body to an injury, intended to protect the affected area and initiate the healing process. However, in the case of an acute whiplash, excessive inflammation can contribute to pain, swelling, and stiffness.
Cervical nerves can also be affected during an acute whiplash injury, leading to neurological symptoms such as numbness, tingling, or muscle weakness in the arms, shoulders, or even face. These symptoms often result from irritation of the cervical nerve roots due to deformation of the surrounding anatomical structures.
The pathophysiology of acute whiplash may also have long-term implications. Structural changes in ligaments, muscles and joints can contribute to the development of chronic problems such as cervical spondylosis, a degenerative joint condition.
- Initial Trauma: Acute whiplash usually occurs as a result of direct trauma, such as a car accident, a fall, or an impact that causes a sudden force to the cervical area. This trauma can lead to sudden movements of the head, putting strain on the structures of the neck.
- Soft Tissue Injury: The initial trauma can cause damage to the soft tissues of the neck, including muscles, tendons and ligaments. Excessive tension and compression forces can cause micro-tears in these structures.
- Inflammatory Response: In response to injury, the body triggers an inflammatory response. This inflammatory response is characterized by the release of chemical mediators, such as prostaglandins, which promote vasodilation, increased vascular permeability, and attraction of immune cells.
- Edema Formation: Inflammation causes edema, or swelling, to form in the affected area. Edema can compress surrounding structures, increasing pressure and contributing to pain and stiffness.
- Muscle Spasms: Damage and inflammation can trigger muscle spasms in the cervical region. These spasms are a protective response of the body to limit mobility and stabilize the injured area.
- Nerve Irritation: In cases of severe injury, the cervical nerves may become irritated, leading to symptoms such as numbness, tingling, or electrical sensations in the neck and shoulder area.
- Postural Adaptations: In response to pain and stiffness, individuals may involuntarily adopt postural adaptations, such as limiting neck movement, which can lead to increased muscle tension and worsen the condition.
- Healing and Repair: Over time, the process of healing and repair begins. Collagen fibers are laid down to repair injured tissue, but the quality of this healing can vary and sometimes lead to a loss of normal function.
The pathophysiology of acute whiplash reflects a complex sequence of biological and structural responses aimed at repairing damaged tissues. The severity of lesions can vary from mild to severe, thereby influencing the clinical presentation and prognosis of the condition. Appropriate management, including initial care, rehabilitation and appropriate therapeutic approaches, aims to promote optimal recovery while minimizing potential complications.
Prevention
Prevention of acute whiplash involves a proactive approach focused on changing behaviors, adopting good ergonomic practices, and taking steps to reduce potential risks. Here are some prevention strategies:
- Physical Trauma: Direct trauma, such as a car accident, fall, or sudden impact, can lead to an acute whiplash injury. During these events, the head may experience sudden movements of flexion, extension or rotation, putting excessive strain on the muscles, tendons and ligaments of the neck.
- Poor Posture: Improper posture, especially during prolonged activities such as using a smartphone with the head tilted downward, can contribute to the development of an acute whiplash injury. This prolonged position can cause excessive strain on the neck structures, causing pain and discomfort.
- Repetitive Activities: Repetitive neck movements, such as those performed in certain occupations or during daily activities, can contribute to excessive wear and tear on cervical structures, increasing the risk of sprains.
- Muscle Stress: Excessive muscle stress due to strenuous physical activities, sudden movements or awkward postures can also be a cause of acute whiplash.
- Lifestyle Factors: Lifestyle habits such as a sedentary lifestyle, lack of exercise, being overweight and smoking can contribute to fragile neck structures, increasing susceptibility to whiplash.
- Genetic Predisposition: Some people may have a genetic predisposition to musculoskeletal conditions, which may influence the likelihood of developing a whiplash in response to triggering factors.
- Occupational Factors: Certain occupations may result in increased exposure to the risk of whiplash. Workers performing repetitive tasks, those who carry heavy loads inappropriately, or those who are exposed to constant vibration may be more likely to develop neck strain.
- Pre-Existing Conditions: Pre-existing medical conditions, such as cervical arthritis, can weaken neck structures, increasing vulnerability to sprains.
- Sports Accidents: Sports activities, especially those that involve sudden movements, impacts or falls, can increase the risk of acute whiplash.
- Anatomical Defects: Congenital or acquired anatomical abnormalities of the cervical spine can contribute to instability or excessive strain, increasing the risk of sprains.
- Age: Natural aging can lead to degeneration of intervertebral discs and joints, making cervical structures more susceptible to injury.
- Environmental Conditions: Environmental conditions such as stressful work conditions, lack of workplace ergonomics, or physically restrictive environments can contribute to excessive neck strain.
- Mechanical Conditions: Mechanical disorders of the cervical spine, such as joint instability, may predispose to acute whiplash.
- Physical Trauma: Direct trauma, such as a car accident, fall, or sudden impact, can lead to an acute whiplash injury. During these events, the head may experience sudden movements of flexion, extension or rotation, putting excessive strain on the muscles, tendons and ligaments of the neck.
- Poor Posture: Improper posture, especially during prolonged activities such as using a smartphone with the head tilted downward, can contribute to the development of an acute whiplash injury. This prolonged position can cause excessive strain on the neck structures, causing pain and discomfort.
- Repetitive Activities: Repetitive neck movements, such as those performed in certain occupations or during daily activities, can contribute to excessive wear and tear on cervical structures, increasing the risk of sprains.
- Muscle Stress: Excessive muscle stress due to strenuous physical activities, sudden movements or awkward postures can also be a cause of acute whiplash.
- Lifestyle Factors: Lifestyle habits such as a sedentary lifestyle, lack of exercise, being overweight and smoking can contribute to fragile neck structures, increasing susceptibility to whiplash.
- Genetic Predisposition: Some people may have a genetic predisposition to musculoskeletal conditions, which may influence the likelihood of developing a whiplash in response to triggering factors.
- Occupational Factors: Certain occupations may result in increased exposure to the risk of whiplash. Workers performing repetitive tasks, those who carry heavy loads inappropriately, or those who are exposed to constant vibration may be more likely to develop neck strain.
- Pre-Existing Conditions: Pre-existing medical conditions, such as cervical arthritis, can weaken neck structures, increasing vulnerability to sprains.
- Sports Accidents: Sports activities, especially those that involve sudden movements, impacts or falls, can increase the risk of acute whiplash.
- Anatomical Defects: Congenital or acquired anatomical abnormalities of the cervical spine can contribute to instability or excessive strain, increasing the risk of sprains.
- Age: Natural aging can lead to degeneration of intervertebral discs and joints, making cervical structures more susceptible to injury.
- Environmental Conditions: Environmental conditions such as stressful work conditions, lack of workplace ergonomics, or physically restrictive environments can contribute to excessive neck strain.
- Mechanical Conditions: Mechanical disorders of the cervical spine, such as joint instability, may predispose to acute whiplash.
Collier Cervical
The cervical collar, also known as a cervical collar or support collar, is a medical device used to provide support and immobilization to the neck. It is often prescribed as part of the initial treatment of acute whiplash and other medical conditions requiring neck stabilization. Here are some important aspects regarding the cervical collar:
Objectives of the Cervical Collar
- Immobilization: The primary purpose of the cervical collar is to partially or completely immobilize the cervical region, thereby limiting neck movement. This helps reduce stress on damaged structures and promotes healing.
- Structural Support: By providing structural support, the cervical collar helps maintain the neutral position of the neck, reducing the risk of inappropriate movements that could aggravate the injury.
- Pain Reduction: By limiting neck mobility, the cervical collar can help reduce pain associated with movement and muscle tension.
Types of Cervical Collars
- Soft Collars: These collars are soft and lightweight, providing moderate support. They are often used in cases of mild neck sprains or for increased comfort.
- Semi-Rigid Collars: These collars offer an intermediate level of support and stability. They are prescribed for cervical sprains of moderate severity.
- Rigid Collars: Rigid cervical collars provide maximum immobilization. They are usually prescribed for more serious injuries, such as cervical fractures.

Use and Precautions
- Medical Prescription: The prescription for a cervical collar must be made by a healthcare professional based on the assessment of the injury and the specific needs of the patient.
- Duration of Use: The duration of use of a cervical collar depends on the severity of the injury and the recommendations of the healthcare professional. Prolonged use without medical advice may lead to muscle weakness.
- Correct Fit: It is essential that the cervical collar fits correctly to provide optimal support without restricting breathing or blood circulation.
- Limiting Activities: While wearing the cervical collar, the patient is often encouraged to limit activities, particularly neck movements, to promote healing.
- Regular Assessment: Regular assessment by a health professional is necessary to adjust treatment according to the evolution of the injury.
Diagnosis and Treatment
Diagnostic
- Clinical Assessment: A healthcare professional will perform a thorough clinical assessment by asking the patient about the circumstances of the injury, examining symptoms, and assessing neck mobility and tenderness.
- Imaging: Imaging tests such as X-rays, MRIs or CT scans may be recommended to assess the severity of injuries, identify possible fractures or check the integrity of cervical structures.
- Neurological Evaluation: In more serious cases, a neurological evaluation may be carried out to detect possible nerve damage.
Treatment
- Rest and Pain Management:
- Initial rest to allow healing.
- Using nonsteroidal anti-inflammatory drugs (NSAIDs) can help reduce inflammation and pain.
- Application of Ice or Heat:
- Applying ice in the first 24 to 48 hours can help reduce inflammation. Subsequently, the use of heat can relieve muscle tension.
- Collier Cervical :
- In some cases, a cervical collar may be prescribed to support the neck and limit movement during the initial recovery phase.
- Gentle Mobility Exercises:
- Gentle mobility exercises may be recommended once the acute phase of the injury has passed. These exercises aim to gradually restore neck mobility.
- Osteopathy:
- Osteopathy can include stretching sessions, muscle strengthening, and relaxation techniques to promote recovery.
- Stress Management and Postural Advice:
- Educating the patient on stress management and adopting good postural practices can help prevent recurrences.
- Medical monitoring :
- Regular medical follow-up is essential to monitor healing progress, adjust the treatment plan if necessary, and ensure there are no complications.
More Serious Cases
- Collaboration Multidisciplinaire :
- In cases of serious injuries or persistent symptoms, collaboration between different healthcare professionals, such as specialists in orthopedics, neurology, or physical medicine, may be necessary.
- Surgery :
- In rare cases requiring surgical intervention, this could be considered, particularly in the event of fractures or severe injuries.
Stretching and exercise
Specific stretches and exercises can play an important role in recovery and prevention of acute whiplash. However, it is crucial to undertake them carefully and under the supervision of a healthcare professional, especially in the initial stages of the injury. Here are some stretches and exercises that may be beneficial, but they should be tailored to each individual based on the severity of the injury and the advice of a healthcare professional:
- Neck Stretches:
- Side Tilt: Sit or stand, slowly tilt your head to one side with your ear toward your shoulder. Hold the position for 15 to 30 seconds.
- Neck Rotation: Slowly turn your head to one side, toward the shoulder, holding the position for a few seconds. Repeat on the other side.
- Flexion-Extension: Slowly tilt your head forward (flexion) and backward (extension), holding each position for a few seconds.
- Muscle Strengthening Exercises:
- Lateral Bends Against Resistance: Place one hand on the side of the head and apply light resistance by tilting the head sideways. Repeat on each side.
- Forward Bends Against Resistance: Place your hands on the back of your head and apply resistance while tilting your head forward.
- Controlled Rotation: Sit or stand with your spine straight, slowly turn your head from one side to the other, controlling the movement.
- General Relaxation Exercises:
- Shoulder Exercises: Exercises aimed at relaxing and strengthening the shoulder muscles can also help relieve tension in the cervical region.
- Yoga or Pilates: These disciplines can include movements that promote flexibility and stability of the spine.
- Trapezius Stretching Exercises:
- Upper Trapezius Stretch: Gently lower one shoulder while tilting your head toward the opposite side to stretch the upper trapezius. Repeat on the other side.
- Gentle Aerobic:
- Low-impact aerobic activities, such as light walking or swimming, can help maintain blood circulation and promote healing without causing excess strain on the neck.
Conclusion
In conclusion, acute whiplash, often caused by trauma such as a car accident, fall, or impact, can lead to painful damage to neck structures. This disorder, although often considered benign, requires thorough evaluation and appropriate management to ensure optimal recovery.
The diagnosis of whiplash is based on a detailed clinical assessment, possibly supplemented by imaging examinations to assess the severity of the lesions. Symptoms can vary in severity, from temporary neck pain to more serious symptoms, such as headaches, numbness, or muscle spasms.
Initial treatment aims to control pain, reduce inflammation and promote healing. Measures such as rest, application of ice or heat, and use of medications may be prescribed. Cervical collars and osteopathy can also play an important role in managing the injury.
The pathophysiology of whiplash involves an inflammatory response of the body, edema formation, muscle spasms, and healing processes. Understanding these biological mechanisms is essential to guide treatment appropriately.
Mobility and strengthening exercises, under the supervision of a healthcare professional, are often integrated into the recovery phase. Preventing whiplash involves adopting good postural practices, stress management, and ergonomic measures at work and at home.
In the event of persistent symptoms or complications, multidisciplinary collaboration and regular medical monitoring are recommended. Most people recover completely with time and proper treatment. It is essential that patients follow the advice of their healthcare professionals to minimize the risk of complications and ensure a full recovery of their cervical well-being.
References
- Evans RW. Persistent post-traumatic headache, postconcussion syndrome, and whiplash injuries: the evidence for a non-traumatic basis with an historical review. Headache. 2010 Apr;50(4):716-24. [PubMed]2.
- Pearce JM. Whiplash injury: a reappraisal. J Neurol Neurosurg Psychiatry. 1989 Dec;52(12):1329-31. [PMC free article] [PubMed]3.
- Toney-Butler TJ, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 28, 2023. Motor Vehicle Collisions. [PubMed]4.
- Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chin J Traumatol. 2009 Oct;12(5):305-14. [PubMed]5.
- Bandong AN, Leaver A, Mackey M, Ingram R, Shearman S, Chan C, Cameron ID, Moloney N, Mitchell R, Doyle E, Leyten E, Rebbeck T. Adoption and use of guidelines for whiplash: an audit of insurer and health professional practice in New South Wales, Australia. BMC Health Serv Res. 2018 Aug 08;18(1):622. [PMC free article] [PubMed]6.
- de Jonge MC, Kramer J. Spine and sport. Semin Musculoskelet Radiol. 2014 Jul;18(3):246-64. [PubMed]7.
- Parikh P, Santaguida P, Macdermid J, Gross A, Eshtiaghi A. Comparison of CPG’s for the diagnosis, prognosis and management of non-specific neck pain: a systematic review. BMC Musculoskelet Disord. 2019 Feb 14;20(1):81. [PMC free article] [PubMed]8.
- Anderson C, Yeung E, Toong T, Tong T, Reed N. A narrative review on cervical interventions in adults with chronic whiplash-associated disorder. BMJ Open Sport Exerc Med. 2018;4(1):e000299. [PMC free article] [PubMed]9.
- Cassidy JD, Carroll LJ, Côté P, Lemstra M, Berglund A, Nygren A. Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. N Engl J Med. 2000 Apr 20;342(16):1179-86. [PubMed]10.
- Ivancic PC, Sha D. Comparison of the whiplash injury criteria. Accid Anal Prev. 2010 Jan;42(1):56-63. [PubMed]11.
- Binder A. The diagnosis and treatment of nonspecific neck pain and whiplash. Eura Medicophys. 2007 Mar;43(1):79-89. [PubMed]12.
- Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining « whiplash » and its management. Spine (Phila Pa 1976). 1995 Apr 15;20(8 Suppl):1S-73S. [PubMed]13.
- Yadla S, Ratliff JK, Harrop JS. Whiplash: diagnosis, treatment, and associated injuries. Curr Rev Musculoskelet Med. 2008 Mar;1(1):65-8. [PMC free article] [PubMed]14.
- Van Geothem JW, Biltjes IG, van den Hauwe L, Parizel PM, De Schepper AM. Whiplash injuries: is there a role for imaging? Eur J Radiol. 1996 Mar;22(1):30-7. [ PubMed ]15.
- Ngatchou W, Beirnaert J, Lemogoum D, Bouland C, Youatou P, Ramadan AS, Sontou R, Alima MB, Plumaker A, Guimfacq V, Bika C, Mols P. Application of the Canadian C-Spine rule and nexus low criteria and results of cervical spine radiography in emergency condition. Pan Afr Med J. 2018;30:157. [PMC free article] [PubMed]16.
- Churilov IuK, Bagaudinov KG, Orel AM, Lapteva NV, Imenovskiĭ IE. [Clinical-neurological and radiological diagnostics of whiplash trauma and it’s consequences in flight crew]. Voen Med Zh. 2008 Jun;329(6):22-6. [PubMed]17.
- Michaleff ZA, Maher CG, Verhagen AP, Rebbeck T, Lin CW. Accuracy of the Canadian C-spine rule and NEXUS to screen for clinically important cervical spine injury in patients following blunt trauma: a systematic review. CMAJ. 2012 Nov 06;184(16):E867-76. [PMC free article] [PubMed]18.
- Panjabi MM, Cholewicki J, Nibu K, Grauer JN, Babat LB, Dvorak J. Mechanism of whiplash injury. Clin Biomech (Bristol, Avon). 1998 Jun;13(4-5):239-249. [PubMed]19.
- Hernández-Sousa MG, Sánchez-Avendaño ME, Solís-Rodríguez A, Yáñez-Estrada M. [Disability by cervical sprain I and II and the use of neck collar]. Rev Med Inst Mex Seguro Soc. 2013 Mar-Apr;51(2):182-7. [ PubMed ]20.
- Ruiz-Molinero C, Jimenez-Rejano JJ, Chillon-Martinez R, Suarez-Serrano C, Rebollo-Roldan J, Perez-Cabezas V. Efficacy of therapeutic ultrasound in pain and joint mobility in whiplash traumatic acute and subacute phases. Ultrasound Med Biol. 2014 Sep;40(9):2089-95. [PubMed]






")











{kind=link}