

Introduction
Context: Why Revisit Knee Anatomy?
The knee has long been regarded as a marvel of biomechanical engineering, responsible for bearing weight, absorbing shock, and providing essential mobility. Orthopedic and osteopathic literature abounds with detailed discussions on knee ligaments, tendons, and the menisci. Yet, it is precisely because the knee is so well-studied that new anatomical discoveries can prove so revolutionary. Indeed, Dr. Eng’s recent revelation concerning an accessory fascial slip from the iliotibial (IT) band to the lateral meniscus underscores the fact that our understanding of this complex joint is far from complete.
So why revisit knee anatomy now? For one, the growing incidence of knee-related complaints—ranging from patellofemoral pain syndrome to meniscal tears—calls for an ever-deeper understanding of how the knee truly functions. Traditional anatomical models have served clinicians well, but novel findings challenge long-held assumptions and open doors for improved diagnostic and therapeutic interventions. Moreover, the rise of new imaging techniques, combined with ongoing advances in cadaveric and in-vivo research, continues to refine what we think we know about the knee. Dr. Eng’s discovery exemplifies how even a single, previously overlooked structural component can change our perspective on knee stability, load distribution, and overall biomechanics.
Another important driver behind revisiting knee anatomy is the shift in clinical paradigms from purely structural views to more holistic, systems-based approaches. Osteopathic principles hold that the body’s structure and function are interdependent, so emerging fascial research integrates seamlessly into this viewpoint. When we unearth hidden or less-studied anatomical connections—like an accessory slip tethering the IT band to the meniscus—we can better appreciate how subtle variations in connective tissue might underlie both acute injury patterns and chronic degenerative conditions.
The Emerging Role of Fascia in Musculoskeletal Research
Fascia was once dismissed as mere packaging material, but recent decades have witnessed a surge in fascial research. Scientists, osteopaths, and other healthcare practitioners now recognize fascia as a dynamic tissue that influences movement, force transmission, and proprioception. Through a lens that values fascial continuity, anatomical structures such as the IT band—traditionally viewed only as a specialized tendon-like extension of the tensor fasciae latae—are now seen as integral parts of a broad fascial network encompassing muscles, tendons, and even joint capsules.
Understanding how fascia operates within this interconnected framework has opened new avenues for treatment. With Dr. Eng’s discovery of an accessory fascial slip linking the IT band to the lateral meniscus, research and clinical practice must shift further toward a three-dimensional, integrated approach to musculoskeletal health. This perspective posits that small fascial connections can have outsized effects on joint mechanics, stability, and even pain perception.
Whether you are an osteopath, physical therapist, or sports medicine specialist, recognizing the significance of fascial structures is no longer optional; it’s essential. By embracing these fascial insights, we stand poised to reshape rehabilitation strategies, manual therapy techniques, and even surgical interventions, ensuring that our patients benefit from the most accurate anatomical understanding currently available.
Anatomical Overview
Iliotibial Band (ITB): Structure and Function
The iliotibial band (ITB) is a thick, fibrous tract of fascia extending along the lateral aspect of the thigh. It originates primarily from the tensor fasciae latae (TFL) muscle, with additional contributions from fibers of the gluteus maximus. As it travels distally, the ITB inserts into Gerdy’s tubercle on the proximal lateral tibia. While many anatomical texts describe the ITB simply as a stabilizing structure, it is far from passive. This fascial tract is rich in mechanoreceptors and interacts dynamically with the surrounding musculature, helping to distribute force and maintain lateral knee stability.
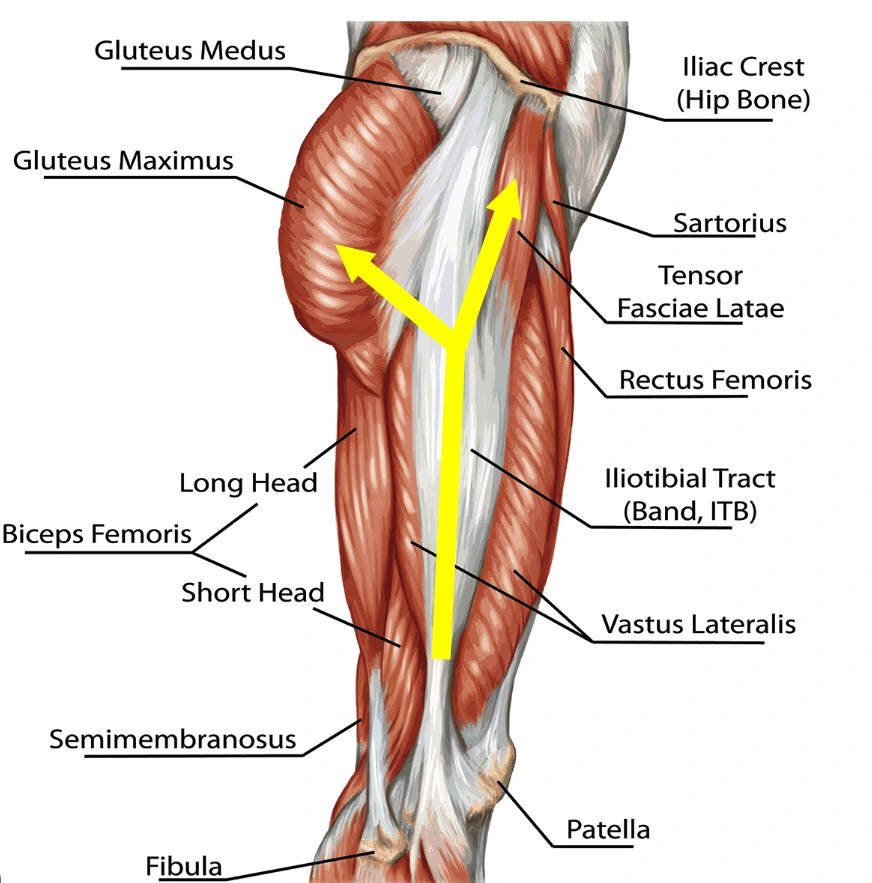
Gluteus Medius and Gluteus Maximus: These muscles originate from the iliac crest and play an essential role in hip stabilization and abduction. The gluteus maximus also contributes fibers to the iliotibial band.
Tensor Fasciae Latae (TFL): A small but significant muscle located at the anterolateral aspect of the hip. It directly connects to the iliotibial band, aiding in stabilizing the knee and hip during movement.
Iliotibial Band (IT Band): A thick band of connective tissue that runs along the lateral thigh from the iliac crest to the tibia. It acts as a stabilizer for both the hip and knee, particularly during activities like running and walking.
Hamstrings (Biceps Femoris, Semimembranosus) and Quadriceps (Rectus Femoris, Vastus Lateralis): These muscle groups are critical for knee flexion, extension, and stabilization.
The image highlights the interaction between these muscles and the IT band, illustrating its importance in biomechanics. This diagram serves as a valuable reference for understanding the role of these structures in lower limb movement and common conditions like IT band syndrome.
Functionally, the ITB is crucial in controlling and stabilizing hip and knee movements, particularly during activities like running, climbing stairs, and walking on uneven terrain. When the TFL and the gluteus maximus contract, tension transmitted through the ITB aids in stabilizing the pelvis and knee, limiting frontal plane motion such as excessive varus or valgus. Moreover, the ITB can affect rotational movements at the knee and hip, making it indispensable for coordinated lower extremity biomechanics.
Because the ITB is part of an extensive fascial network, it has connections—both direct and indirect—with other key anatomical structures, including the lateral retinaculum and the vastus lateralis. This broad fascial continuity has led many clinicians and researchers to propose that the ITB is far more than a mere tendon-like structure; it may play a key role in proprioception, force transmission, and even postural control. Over the last decade, renewed interest in fascial anatomy has led to deeper explorations of how these seemingly simple, fibrous structures influence everything from joint stability to neuromuscular coordination.
Meniscus Anatomy: Lateral vs. Medial Distinctions
Each human knee contains two crescent-shaped fibrocartilaginous structures called menisci—one medial and one lateral. The menisci are integral for shock absorption, load distribution, and joint stability. They also facilitate smooth articulations between the femoral condyles and the tibial plateau. Although often grouped together as “the meniscus,” there are some notable differences between the medial and lateral menisci.
The medial meniscus is more C-shaped and firmly attached to the medial collateral ligament (MCL), making it less mobile but more prone to tears, especially in rotational injuries. On the other hand, the lateral meniscus has a more circular shape and is not as rigidly fixed to the joint capsule, granting it greater mobility. This design helps reduce shear forces but can also contribute to different patterns of wear and potential injury. Additionally, the lateral meniscus often features fewer attachments to surrounding structures compared to the medial side, which historically led many practitioners to perceive it as less critical in overall knee stability—an assumption that’s being challenged by new anatomical discoveries.
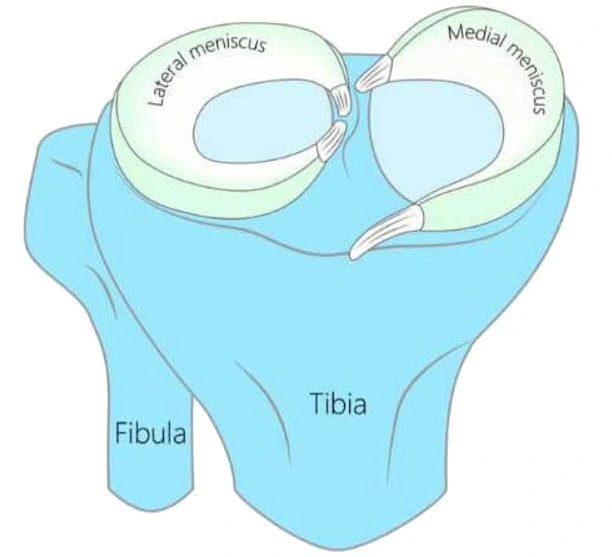
Medial Meniscus: Positioned on the inner side of the knee, it is C-shaped and larger than the lateral meniscus. The medial meniscus is more prone to injury due to its reduced mobility, being firmly attached to the tibia and the joint capsule.
Lateral Meniscus: Located on the outer side of the knee, it is nearly circular in shape and more mobile compared to the medial meniscus. This mobility reduces its susceptibility to injuries.
The image also identifies the tibia and fibula bones of the lower leg as structural landmarks. The menisci play a critical role in maintaining joint integrity by preventing excessive wear and tear on the articular cartilage. Understanding the anatomy of the menisci is essential for diagnosing and treating common knee conditions, such as meniscal tears, often caused by trauma or degenerative changes. This visual serves as a fundamental reference for health professionals and students of musculoskeletal anatomy.
Traditional Understanding of IT Band–Meniscus Interplay
In most classical anatomical teachings, the ITB and menisci are presented as distinct entities that do not share substantial direct connections. The ITB is largely depicted as a lateral “stabilizing strap” while the menisci are seen as intra-articular shock absorbers. Although both structures play crucial roles in the knee’s integrity, traditional perspectives have focused on well-known biomechanical synergies—like how ITB tension may affect lateral femoral condyle tracking or how the lateral meniscus absorbs forces transmitted through the lateral compartment.
Historically, clinicians and researchers recognized that tension in the ITB could impact lateral meniscal movement indirectly—particularly when the knee flexes and extends. A tight ITB can restrict lateral meniscal excursion or impose abnormal shear forces on the lateral compartment. However, direct, firm anatomical fascial ties—such as those observed in Dr. Eng’s discovery of an accessory slip—were not thoroughly described. Instead, any interplay was often chalked up to “secondary” effects due to the proximity of these structures rather than a direct connection.
This prevailing viewpoint is now being revisited as part of a broader recognition that fascial continuities can create subtle yet meaningful interplay between structures once thought to function independently. By delving into the newly discovered slip that joins the ITB and the lateral meniscus, we can begin to see why clinical outcomes may vary when these tissues are compromised. For osteopaths and other manual therapy practitioners, rethinking this relationship has the potential to refine both assessment and treatment protocols, paving the way for more targeted interventions that respect the unity of fascial networks in maintaining knee health.
By connecting to the lateral meniscus, the ITB’s forces can be partially transferred to the meniscus, helping distribute load away from purely articular surfaces. This mechanism may aid in shock absorption during weight-bearing activities such as walking, running, or jumping. In essence, the ITB does not only function as a “check rein” against excessive knee varus or valgus movement; it also assists in fine-tuning rotational and compressive forces around the joint.
Although not extensively detailed in older anatomical texts, this ITB–meniscal attachment is garnering increased attention in research on knee biomechanics and injury prevention. Its presence can have clinical implications: excessive tension or abnormal mechanics in the ITB might place additional stress on the lateral meniscus, potentially contributing to lateral knee pain or degeneration over time. Conversely, proper conditioning and balanced muscular support can help optimize the ITB’s role, potentially protecting the meniscus against undue strain. Ultimately, this accessory ligament connection highlights the knee’s complexity and the importance of a holistic view when assessing lateral knee function or pathology.
Dr. Eng’s Discovery of the Accessory Fascial Slip
Research Background and Methodology
Dr. Eng’s research began as a response to clinical observations that didn’t fit neatly into established knee anatomy models. Osteopaths, orthopedic surgeons, and physical therapists had long recognized that many patients with lateral knee discomfort, IT band syndrome, or seemingly sporadic meniscal symptoms did not respond to standard interventions as consistently as expected. Intrigued by this discrepancy, Dr. Eng and his team set out to explore the possibility that unknown anatomical connections might be influencing these clinical presentations.
Their approach combined both traditional dissection methods and modern imaging techniques. First, the team conducted a series of cadaveric dissections on knees with no known pathology. Each specimen was carefully studied to identify any variances in fascial tissue continuity, particularly around the lateral aspect of the knee. The researchers meticulously documented the presence or absence of any distinct fascial bands, slips, or expansions that extended from the ITB toward the joint capsule, the lateral collateral ligament (LCL), or the lateral meniscus.
Subsequently, Dr. Eng employed advanced imaging tools—such as high-resolution ultrasound, MRI, and digital tomography—to validate these findings in vivo. By scanning volunteers with no known knee pathologies as well as individuals experiencing chronic lateral knee pain, Dr. Eng’s team cross-referenced the imaging data with their anatomical discoveries. This dual-method approach was critical because, while cadaveric studies can provide direct visualization of tissues, they do not account for dynamic factors like tension, movement, and physiological loading. In contrast, imaging in live subjects allowed the researchers to observe whether this accessory fascial structure had any functional mobility or tension changes during knee flexion, extension, and weight-bearing activities.
Detailed Description of the Fascial Slip
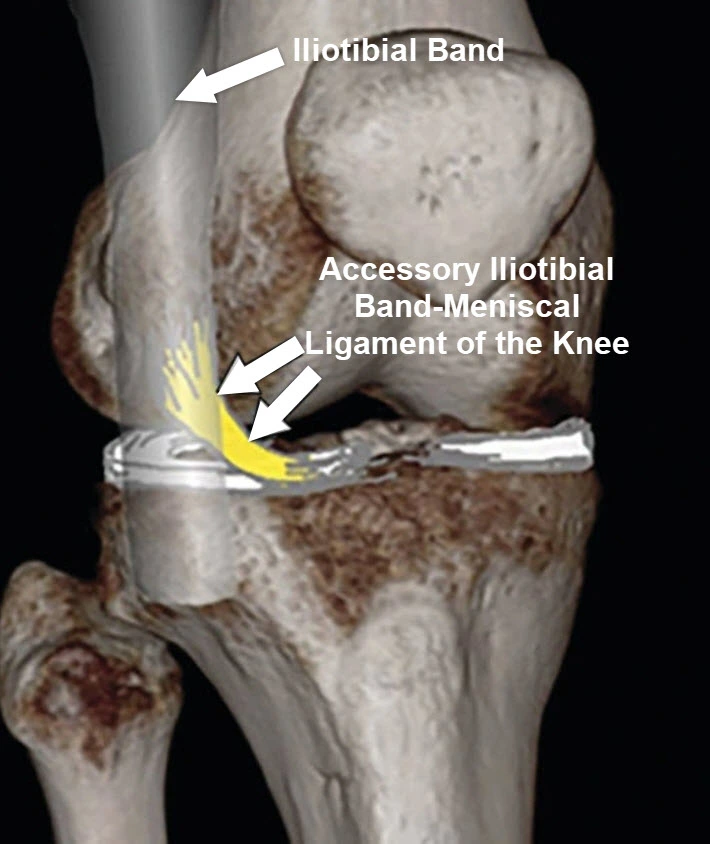
The accessory fascial slip that Dr. Eng’s team identified is a distinct band of connective tissue that branches off from the ITB just proximal to the joint line, near the lateral femoral epicondyle. Rather than following the ITB’s primary pathway toward Gerdy’s tubercle, this slip angles slightly anteriorly and medially, traversing the lateral knee compartment. Its thickness varies among individuals, but in most dissections, it appeared as a discrete, well-defined structure rather than a thin or diffuse fascial layer.
Histologically, the fascial slip resembles specialized fascia more akin to a tendon-like extension than loose areolar tissue. It has a higher concentration of collagen fibers oriented in a longitudinal pattern, suggesting it is built to withstand tensile forces. Moreover, embedded within its layers are small mechanoreceptors, which may play a role in proprioception—an indication that this slip could be vital for sensing changes in knee position and load.
Another intriguing observation was the slip’s potential interactions with nearby structures. Some specimens showed a fascial continuity between this slip and the lateral patellar retinaculum, raising questions about how tension in one structure could be transmitted to another. While further research is required to clarify these connections, the discovery of such consistent fascial expansions highlights the complexity of the knee’s lateral compartment and challenges the notion that the ITB is a simple, unbranched band of tissue.
To further illustrate the fascial connections described above, see the following video
Novel Findings: How It Connects to the Lateral Meniscus
The most noteworthy aspect of Dr. Eng’s discovery is the slip’s direct and robust insertion into the peripheral edge of the lateral meniscus. Traditionally, the lateral meniscus has been described as less firmly attached to the joint capsule than the medial meniscus, giving it greater mobility. However, Dr. Eng’s findings suggest that this accessory slip may serve as an additional stabilizing tether for the lateral meniscus, anchoring it more securely to the ITB and possibly influencing how the meniscus moves during knee flexion, extension, and rotational movements.
When the knee is extended, preliminary ultrasound and MRI studies showed that the fascial slip appears slack or mildly taut, depending on the degree of tension in the ITB. As the knee flexes, particularly beyond 30 degrees, the slip becomes more tensioned, pulling gently on the lateral meniscus. This mechanical pull could explain some cases of lateral knee pain in patients diagnosed with IT band syndrome who also exhibit meniscal irritation. Rather than being merely coincidental pathologies, these two issues might arise from increased tension through a single fascial chain that overstrains the lateral meniscus.
Additionally, Dr. Eng posits that the accessory fascial slip may help distribute load across the lateral knee compartment. In healthy biomechanics, the menisci act as shock absorbers and help with load transmission. If the lateral meniscus is more securely tethered to the ITB, then force generated in the lateral thigh (e.g., during running or cutting movements in sports) could be partly redirected through this fascial bridge, altering stress distribution patterns. This insight has significant implications for rehabilitation and injury prevention. Clinicians may need to reevaluate their approaches to ITB-related pathologies, as tightness or dysfunction in the ITB could have a direct impact on meniscal health.
Furthermore, the discovery shifts our understanding of knee stability. While the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and collateral ligaments have traditionally been emphasized in discussions of stabilizing structures, this new fascial slip may also play a minor yet non-negligible role in rotational control. During dynamic movements, the interplay between the ITB, the newly discovered slip, and the lateral meniscus could contribute to maintaining alignment and preventing excessive tibial rotation.
In summary, Dr. Eng’s work underscores that the knee is a far more intricate structure than traditional anatomical models suggest. The identification of this accessory slip challenges older paradigms by illustrating how fascial continuity can bind what were previously considered separate components of the knee complex. For osteopaths and other manual therapy practitioners, these findings open up exciting possibilities for targeting specific fascial structures in the lateral compartment to address chronic pain, instability, or post-surgical complications. From a broader perspective, the discovery paves the way for more in-depth studies into fascial interconnections and the profound ways they can shape joint biomechanics and clinical outcomes.
Is Dr. Eng’s Fascial Slip the Same as the Accessory ITB Ligament?
At this point in the literature, there isn’t a universal consensus on whether Dr. Eng’s newly described fascial slip should be considered exactly the same as what some sources call the “accessory iliotibial band ligament.” These terms are sometimes used interchangeably, but they may refer to slightly different anatomical findings or variations. Here’s a bit more context:
- Dr. Eng’s Fascial Slip
- Primary Description: Dr. Eng’s discovery describes a discrete fascial expansion branching off from the IT band and inserting into the lateral meniscus.
- Key Novelty: The distinct presence of tensile, tendon-like fibers (rather than a diffuse fascial membrane), plus a clear attachment into the lateral meniscus.
- Clinical Implication: This slip appears to add stability and may influence the lateral meniscus’ movement and load distribution in ways not accounted for in classic knee anatomy models.
- “Accessory Iliotibial Band Ligament”
- Variable Nomenclature: In some anatomical texts and case reports, structures vaguely described as “accessory IT band ligaments” or “IT band–meniscotibial ligaments” have been observed. These might anchor the IT band more firmly to the tibia or the meniscus.
- Overlap vs. Distinction: While these descriptions may sound similar, not all sources precisely outline the same location, tissue density, or insertion points as Dr. Eng’s fascial slip. Thus, some “accessory ligaments” may attach differently (for instance, into the joint capsule near the tibial plateau) rather than directly into the outer rim of the meniscus.
- Why the Confusion?
- Variations in Human Anatomy: Accessory fascial bands are often understudied because they can vary in thickness, prominence, and insertion site between individuals. What one researcher calls an “accessory band” another might call a “fascial slip,” creating a bit of nomenclatural chaos.
- Evolving Research: As fascial research gains momentum, new findings or more precise imaging can reveal subtle variations that didn’t previously receive attention or a formal name.
- Practical Takeaway
- Likely a Similar (but Not Identical) Structure: While it’s possible that Dr. Eng’s fascial slip and the so-called “accessory iliotibial band ligament” describe the same phenomenon, Dr. Eng’s team emphasizes the slip’s unique path and insertion into the meniscus. In some descriptions of the “accessory IT band ligament,” the attachment is more capsular or tibial, and less specifically integrated with the meniscal tissue.
- Further Studies Needed: Additional cadaveric research and in-vivo imaging comparisons are required to unify these terms—or justify why they should remain distinct—within the anatomical community.
In short, Dr. Eng’s fascial slip might fall under the broader umbrella of what some call “accessory IT band ligaments,” yet the precise morphological details and consistent attachment to the lateral meniscus suggest a unique variant not always captured by older nomenclature. Over time, with more data and wider acknowledgement, the community may settle on a single term or subdivide these variants with more specific names.
Biomechanical Impact
Changes in Knee Joint Kinetics and Kinematics
The discovery of a distinct fascial slip connecting the ITB to the lateral meniscus has prompted a reexamination of how forces travel through the knee. Traditionally, the ITB has been viewed as a lateral stabilizer, primarily transferring tension from the hip abductors into the lateral aspect of the knee. However, with this newly identified slip, tension in the ITB may now be transmitted more directly to the meniscus, altering the typical force pathways within the joint.
In terms of kinetics—forces acting on the knee—the accessory slip could create additional pulling or tethering on the lateral meniscus when the knee is flexed. During dynamic activities such as running, jumping, or cutting maneuvers, the ITB experiences variable tension. That tension, transmitted through the accessory slip, may shift meniscal position or alter its mobility. Consequently, kinematic patterns—specifically the manner in which the knee flexes, extends, and rotates—could also change. Clinically, this implies that patients with tight or overactive ITBs might experience increased pressure or tracking issues on the lateral compartment, while those with poor ITB tone may lack sufficient stabilization in certain positions.
Potential Effects on Load Distribution and Shock Absorption
One of the meniscus’s principal roles is to absorb shock and evenly distribute load across the tibiofemoral articulations. The lateral meniscus is known for being more mobile than its medial counterpart, partly because it has fewer firm capsular attachments. Now, with the discovery of a robust fascial link, the lateral meniscus could be subjected to more or different force vectors than previously appreciated. When the ITB tightens—particularly during activities involving hip abduction or lateral stabilization—this additional pull may either assist or hinder the lateral meniscus’s ability to deform appropriately under load.
From a functional standpoint, such fascial tension might either improve the meniscus’s capacity to disperse forces (by ensuring optimal contact with the femoral condyle) or, conversely, cause local stress concentrations if the meniscus becomes restricted in its movement. Understanding exactly how this interplay manifests will likely require further research, especially dynamic or weight-bearing imaging studies. However, if tension is transmitted irregularly, certain regions of the meniscus could experience higher stress, potentially speeding degenerative changes or predisposing individuals to meniscal tears in the lateral compartment.
Influence on Joint Stability and Range of Motion
Joint stability is typically discussed in the context of ligaments, muscular control, and neuromuscular feedback loops. Yet fascia is increasingly recognized as an important player in modulating stability and proprioception. By anchoring the ITB more firmly to the lateral meniscus, the accessory fascial slip can contribute to knee stability in subtle but potentially significant ways. When the knee is in deeper flexion angles—such as during squatting, lunging, or ascending and descending stairs—tension in the slip could help limit excessive meniscal displacement. This may prevent unwanted lateral translation or rotation of the tibiofemoral joint, thereby supporting overall knee stability.
On the other hand, because stability and mobility are two sides of the same coin, any factor that increases stabilization might also restrict motion if overactive or stiff. A hypersensitive or excessively tight ITB, combined with this slip, could theoretically reduce lateral meniscus excursion, limiting rotational freedom. This limitation might manifest as reduced ability to pivot or adapt to uneven terrain, a factor that could be clinically relevant for athletes or individuals who need a wide range of motion for their daily activities.
The proprioceptive potential of this fascial connection also cannot be overlooked. Mechanoreceptors found within fascial tissues help inform the central nervous system about joint position and load. By integrating the ITB and lateral meniscus, this slip might enhance or alter proprioceptive feedback loops, shaping neuromuscular responses that affect movement patterns. Understanding and leveraging this relationship could be crucial when designing rehabilitation programs aimed at optimizing knee function, particularly after injury or surgery.
In summary, Dr. Eng’s discovery reveals a critical biomechanical link that adds complexity to our understanding of the knee’s lateral compartment. By influencing how forces are distributed, stabilizing meniscal motion, and affecting proprioceptive feedback, this accessory fascial slip can significantly impact knee kinetics and kinematics. For osteopaths and other healthcare professionals, acknowledging this new anatomical nuance is key to refining diagnosis, treatment strategies, and rehabilitation protocols.
Clinical Implications
Assessment Strategies for Lateral Knee Pain
When patients present with lateral knee pain, practitioners traditionally look to common culprits such as IT band friction syndrome, lateral meniscus pathology, or iliotibial bursitis. With the accessory fascial slip in mind, however, it becomes clear that these conditions can interact in ways not previously accounted for. From a diagnostic standpoint, clinicians should consider how tension or dysfunction in the ITB might directly influence the meniscus.
A thorough assessment begins with a detailed patient history focusing on the onset of symptoms, activities that exacerbate or relieve pain, and any previous knee injuries or surgeries. Physical examination should include palpation along the lateral joint line, where the fascial slip inserts into the meniscus, to detect tenderness or thickening. Standard meniscal tests (like McMurray’s) remain valuable, but it may be beneficial to also perform dynamic tests that challenge the ITB, such as Ober’s test or modified weight-bearing maneuvers. Examining both knee flexion angles and rotational stress can reveal abnormal tension patterns related to the accessory slip. Additionally, imaging—especially high-resolution ultrasound or MRI—can help visualize any structural variations or inflammation around the lateral meniscus, providing a fuller picture of how the slip may be contributing to the patient’s pain.
Differential Diagnosis and Overlapping Conditions
When evaluating lateral knee pain, practitioners must consider multiple anatomical structures and biomechanical factors beyond the newly discovered accessory fascial slip. Although the slip may be a direct contributor to pain or meniscal dysfunction, overlapping conditions can complicate the clinical picture. A careful differential diagnosis ensures that potential coexisting pathologies—ranging from ligamentous injuries to referred pain—are addressed appropriately.
Lateral Collateral Ligament (LCL) Strains and Sprains
Among the most common differential diagnoses for lateral knee pain are strains or sprains of the lateral collateral ligament (LCL). The LCL stabilizes the knee against varus stress, providing an important check to lateral opening of the joint. Injuries typically occur due to a direct blow to the medial side of the knee or from sudden twisting motions during sports activities. Symptoms can overlap with those attributed to IT band dysfunction, including tenderness along the lateral joint line and instability during dynamic movements. Special tests such as the varus stress test can help isolate LCL involvement. When LCL injury coexists with fascial slip tension, the patient may present with heightened lateral discomfort that resists standard interventions aimed solely at ITB-related issues.
Posterolateral Corner Injuries
The posterolateral corner (PLC) is a complex network of ligaments, tendons, and joint capsule extensions that helps control external rotation and varus stability at the knee. It includes structures such as the popliteus tendon, popliteofibular ligament, and the lateral (or fibular) collateral ligament. Injuries to the PLC can produce pain and instability in the lateral knee compartment, often accompanied by a sensation of the knee “giving way.” Because PLC injuries are sometimes subtle and can be missed on standard imaging, thorough clinical evaluation is crucial. When a patient’s symptoms persist despite addressing the IT band–meniscus connection, an unrecognized PLC injury could be the driving pathology, requiring specialized testing or imaging to confirm.
Referred Pain from the Hip or Lumbar Spine
Referred pain is another important consideration in the differential diagnosis of lateral knee symptoms. Impairments in the hip—such as trochanteric bursitis or early arthritic changes—can generate pain that radiates distally along the lateral thigh, mimicking IT band syndrome or meniscal discomfort. Similarly, nerve root irritations in the lower lumbar spine (especially at L4/L5 or L5/S1) can lead to sensory disturbances perceived in the knee area. Because Dr. Eng’s discovery underscores the interplay between the IT band and surrounding fascial structures, it is essential to rule out proximal sources of pain that could be misleading clinicians. Conducting a full kinetic chain assessment, including the hip and lumbar spine, ensures a more comprehensive approach to diagnosis.
Iliotibial Band Friction Syndrome vs. Fascial Slip Pathology
IT band friction syndrome (ITBFS) is a frequently cited diagnosis for lateral knee pain, especially among runners. It involves repetitive rubbing of the IT band against the lateral femoral epicondyle, typically causing a localized inflammatory response. While the accessory fascial slip can exacerbate or mirror some symptoms of ITBFS, the two entities are not necessarily interchangeable. In cases of ITBFS, pain is often most pronounced at around 30 degrees of knee flexion, when the IT band transitions over the epicondyle. By contrast, when the fascial slip is involved, additional meniscal irritation or joint line tenderness may be detected. Moreover, imaging or focused physical examination may help distinguish whether friction-related inflammation or fascial tension is the dominant factor in a patient’s pain.
Patellofemoral Pain Syndrome (PFPS)
Although patellofemoral pain syndrome primarily manifests around the anterior knee, certain variations can radiate laterally if maltracking or excessive lateral pressure occurs. If the patella tilts or subluxes laterally, tension within the lateral retinaculum and the IT band can, in turn, affect how the fascial slip interacts with the meniscus. This interplay may lead to a compound presentation of discomfort spanning the anterior and lateral knee. A thorough patellar tracking assessment, including Q-angle measurements and patellar compression tests, is crucial when clinical findings are ambiguous.
Identifying the Primary Driver vs. Contributing Factors
Clinicians must determine whether the newly recognized fascial slip is the primary pain generator or if it merely contributes to symptoms stemming from another pathology. Since many lateral knee conditions share overlapping symptoms—instability, local tenderness, and discomfort during weight-bearing activities—a comprehensive patient history, targeted physical examination, and appropriate imaging are pivotal. If multiple pathologies coexist, management may involve combining interventions: for instance, addressing LCL instability surgically or through bracing, while simultaneously applying manual therapy techniques to reduce tension in the IT band and its fascial slip.
Integrating a Comprehensive Clinical Framework
By systematically ruling out or confirming other pathologies—lateral collateral ligament strains, posterolateral corner injuries, referred pain sources, or patellofemoral tracking issues—clinicians can craft a more effective, individualized treatment plan. In turn, this approach ensures that the accessory fascial slip’s potential role is neither overlooked nor overemphasized. Through ongoing research and cross-disciplinary collaboration, the medical community can refine diagnostic algorithms to better account for newly discovered structures like Dr. Eng’s fascial slip. Ultimately, this nuanced perspective helps optimize patient outcomes by recognizing that lateral knee pain seldom stems from a single tissue and often involves a constellation of interacting anatomical factors.
Manual Therapy Considerations
For osteopaths, physiotherapists, and other manual therapy practitioners, the discovery of this fascial connection highlights the importance of treating the ITB–meniscus complex as a unified system. Techniques such as myofascial release, soft tissue mobilization, and muscle energy approaches should be adjusted to address not only the tension along the ITB but also the fascial continuity anchoring it to the meniscus. If the slip is excessively tight or fibrotic, direct fascial release techniques aimed at reducing tension specifically in the distal portion of the ITB may alleviate excessive pulling on the lateral meniscus.
Joint mobilization techniques that include subtle manipulations of the meniscus—within the patient’s tolerance and in coordination with fascial release—could be employed to improve meniscal mobility. Care should be taken to avoid overly aggressive maneuvers that might aggravate existing meniscal irritation. Clinicians who previously focused solely on the ITB during manual therapy sessions may find better outcomes by examining and addressing potential meniscal restrictions or pain triggers concurrently, given the integral relationship established by this fascial slip.
Rehabilitation and Exercise Protocols
Rehabilitation programs for lateral knee pathologies often incorporate exercises to strengthen the hip abductors, stretch or release the ITB, and stabilize the knee joint. Now, it may be prudent to tailor these interventions with an eye toward the accessory slip’s role in load transmission. Exercises that emphasize neuromuscular control—such as single-leg balance, lateral step-downs, and controlled lunges—remain crucial for proper knee alignment and hip stability.
However, given this new anatomical insight, more attention might be paid to dynamic knee tracking, particularly during lateral movements or changes in direction. Integrating closed-chain exercises that involve careful, gradual increases in flexion angles can help ensure the meniscus moves freely and is not subjected to excessive pulling by a tight ITB. In addition, gentle mobility drills that incorporate rotational elements of the knee may aid in preventing fascial adhesion or excessive stiffness within the slip itself. Patients recovering from acute injuries or surgeries could benefit from a phased approach that prioritizes fascial flexibility early on, followed by progressive strengthening of the surrounding muscles while maintaining proper meniscal positioning.
Implications for Surgical Approaches
Surgeons performing lateral meniscal repairs, partial meniscectomies, or ITB-related procedures should be aware of this accessory slip and its potential impact on postoperative outcomes. In scenarios where the lateral meniscus is being repaired, awareness of the fascial slip’s insertion is critical. Accidental disruption of this slip or failure to address excess tension may compromise meniscal healing or contribute to persistent lateral knee pain post-surgery. Conversely, if the slip is hypertrophic or abnormally thickened, selectively releasing or managing this tissue might be warranted to reduce undue strain on the lateral meniscus.
For patients requiring reconstructive procedures around the lateral knee compartment, a thorough preoperative plan that considers the dynamic interplay between the ITB and the meniscus is essential. Surgical teams could incorporate ultrasound or MRI to identify structural variations in the fascial slip, ensuring that repairs do not inadvertently reduce meniscal mobility or create abnormal tension lines. As new research emerges, some surgical techniques may begin to specifically address or preserve this fascial connection to optimize postoperative knee function, stability, and pain relief.
In summary, Dr. Eng’s discovery reshapes the way practitioners evaluate, treat, and operate on lateral knee pathologies. Recognizing that the ITB and the lateral meniscus are linked by an accessory fascial slip will inevitably refine our clinical assessments, manual therapy strategies, rehabilitation programs, and surgical approaches, ultimately offering patients more targeted and effective solutions for their knee ailments.
Case Studies and Practical Examples
Notable Clinical Presentations
One of the earliest clinical scenarios bringing attention to the accessory fascial slip involved a recreational runner complaining of persistent lateral knee pain misattributed to a basic IT band syndrome. Despite standard treatments (foam rolling, stretching, and NSAIDs), her symptoms persisted. Further investigation revealed notable tenderness not only along the IT band but also at the lateral joint line. Imaging suggested mild meniscal irritation. Once the accessory slip’s possible involvement was recognized, targeted manual therapy and fascial techniques focusing on both the distal IT band and the meniscus led to symptom relief and a successful return to running.
In another case, an older adult presenting with complex lateral knee pain after a low-grade twisting injury showed inconsistent results from traditional rehab. Standard meniscal tests were equivocal, but subtle lateral joint line discomfort suggested involvement of the fascial slip anchoring the meniscus. Specific attention to reducing fascial tension and stabilizing the knee through controlled exercise regimens improved joint function, highlighting the importance of considering this newly discovered structure—particularly in atypical presentations that defy immediate categorization into conventional diagnoses.
Integrating Findings into Osteopathic Practice
Osteopathic principles emphasize the interplay between structure and function, making the fascial slip discovery especially relevant. In practice, osteopaths approach the lateral knee not as a set of isolated structures but rather as a continuous fascial system. Palpation and manual treatment can be adjusted to address tension points in the IT band and the accessory slip insertion on the lateral meniscus. This might involve:
- Fascial Release Techniques: Slow, deliberate techniques to ease tension where the IT band merges with the meniscus.
- Joint and Soft Tissue Mobilizations: Gentle mobilizations targeting meniscal alignment, particularly if fascial tightness is restricting movement.
- Muscle Energy Techniques: Addressing any associated dysfunctions around the hip abductors and the distal IT band to harmonize tension in the lower limb.
By recognizing the practical interplay between the IT band and the lateral meniscus, osteopaths can refine clinical assessments, more effectively localize sources of discomfort, and ultimately provide more precise interventions.
Patient Education and Home Exercise Programs
Given the complexity of lateral knee anatomy, educating patients on the role of the IT band, meniscus, and their newly recognized fascial connection is crucial. A clearer understanding can improve adherence to home exercise programs and self-care routines. Key components include:
- Activity Modifications:
Patients are guided to temporarily reduce or adapt high-impact exercises (like running or jumping) that exacerbate tension around the lateral knee. They’re encouraged to introduce low-impact activities—such as swimming or cycling—that help maintain fitness while allowing fascial tissues to recover. - Targeted Stretching and Foam Rolling:
While standard IT band release techniques remain useful, patients are now instructed to be mindful of the lateral joint line. Gentle rolling or stretching that transitions from the proximal IT band to slightly distal near the meniscal insertion can reduce adhesions and tension, preventing localized overload. - Neuromuscular Control Exercises:
Patients often benefit from single-leg balance, lateral step-downs, or controlled mini-squats that emphasize healthy knee tracking and proprioception. Integrating rotational elements—like lunges with slight external or internal rotation—helps ensure the fascial slip moves freely, reinforcing balanced tension distribution. - Progressive Strengthening:
Strengthening hip abductors, gluteal muscles, and core stabilizers plays a key role in alleviating excessive load on the IT band. Simple exercises like side-lying abductions, clamshells, or bridges are progressed to more functional movements over time.
By fostering an understanding of how the IT band and the lateral meniscus work together, patients can take proactive steps to address mild symptoms before they escalate into more significant issues. Whether the individual is a competitive athlete or an older adult focused on maintaining mobility, such patient education and home-based interventions can significantly reduce pain, prevent re-injury, and bolster overall knee health.
In sum, through case examples and hands-on osteopathic techniques, the importance of Dr. Eng’s discovery comes to life in concrete clinical settings. By integrating these novel insights, osteopaths can refine both evaluation and treatment, while empowering patients with strategies to maintain a healthy balance between knee stability and flexibility.
Future Research Directions
Expanding Anatomical and Biomechanical Studies
Dr. Eng’s discovery highlights the need for more extensive anatomical investigations that account for variations in fascial structures. While existing studies focus on cadaveric dissection and imaging, expanding sample sizes and diversifying demographics would help confirm how frequently this accessory fascial slip appears, how thick it tends to be, and how it may differ by age, activity level, or underlying pathology. Future work using advanced imaging technologies—such as high-definition ultrasound, 3D MRI, or even motion-capture systems linked to musculoskeletal modeling—could shed light on the slip’s dynamic behavior during movement.
Understanding the slip’s biomechanical function also calls for more intricate in-vivo analyses. For instance, employing sensor-equipped braces or wearable technology during activities like running or stair climbing could provide real-time data about tensile forces across the lateral knee. Mapping these force patterns could reveal whether increased tension in the IT band directly correlates with altered meniscal motion in different knee flexion angles. Such insights could inform more personalized approaches to injury prevention and rehabilitation, underlining the potential significance of the slip’s involvement in lateral knee stability and load distribution.
Long-Term Clinical Trials and Outcome Measures
Although case studies and smaller research projects have identified the accessory slip’s clinical importance, rigorous, long-term trials are necessary to confirm and quantify its impact on patient outcomes. Large-scale, randomized controlled studies that compare standard interventions (e.g., IT band release, meniscal therapy) with protocols specifically addressing the accessory fascial slip would be invaluable. Outcome measures could include pain levels, joint function scoring systems (like the Lysholm or IKDC), and performance tests (e.g., single-leg hop tests).
Longitudinal follow-up would help determine whether addressing the accessory slip yields lower recurrence rates of chronic lateral knee pain or reduces the need for more invasive interventions down the line. In addition, subgroups of patients—such as high-performance athletes or older adults with degenerative meniscal changes—could be examined to see if targeted management of this fascial connection leads to better functional capacity or slower progression of degenerative joint disease. These studies would pave the way for establishing best-practice guidelines and strengthen the evidence base for integrating the slip’s assessment into routine knee evaluations.
The Role of Interdisciplinary Collaboration
Finally, recognizing the complexity of fascial interconnections underscores the importance of interdisciplinary collaboration in future research. Orthopedic surgeons, osteopaths, physical therapists, sports medicine physicians, and biomechanical engineers each bring unique insights to the table. Collaborative teams could more rapidly advance knowledge about how best to assess, treat, and perhaps even surgically address this newly revealed structure.
Workshops and conferences designed to discuss fascial anatomy and knee biomechanics would foster knowledge sharing, accelerate research, and refine investigative methodologies. Meanwhile, the use of standardized language—particularly around anatomical naming and measurement conventions—would help unify findings across disciplines. By pooling resources and expertise, researchers can design robust protocols that leverage complementary techniques, from imaging to lab-based biomechanical testing and clinical trials. In this way, Dr. Eng’s initial discovery can catalyze a broader movement toward more comprehensive, holistic studies of knee anatomy, ultimately translating to enhanced patient care and innovative therapeutic strategies.
Expert Opinions or Commentary
Given the growing recognition of fascial interconnections, it is no surprise that Dr. Eng’s discovery of an accessory slip linking the iliotibial band (ITB) to the lateral meniscus has sparked conversations across multiple healthcare disciplines. Orthopedic surgeons, sports medicine specialists, and osteopaths each bring unique viewpoints on how this anatomical insight is reshaping clinical practice.
From an orthopedic surgery standpoint, Dr. Carla Hayes of the University Joint Center underscores the value of recognizing this accessory slip prior to operative interventions. “When performing lateral meniscal repairs,” she explains, “it’s imperative to inspect the fascial continuity around the meniscus. If surgeons fail to note the attachment of the ITB to the meniscus, they risk either over-tightening or accidentally disrupting this structure, which could impact both healing and longer-term stability. Incorporating preoperative imaging of the fascial slip helps us plan more precise repairs.”
In the sports medicine arena, Dr. Terrence Lu, a team physician for a professional soccer club, highlights how this finding refines both injury prevention and rehabilitation protocols. He points out that many athletes diagnosed with ITB syndrome may also experience subtle lateral meniscal irritation if the accessory slip is overstressed. “It’s not enough to treat the ITB in isolation anymore,” he says. “We now adapt our rehab strategies to ensure the meniscus isn’t being unduly pulled or compressed by fascial tension. This may involve dynamic, multi-planar exercises that test how the ITB–meniscal chain responds under real-world conditions, like cutting maneuvers or rapid accelerations.”
Meanwhile, osteopathic practitioners have been particularly quick to adopt integrative treatment strategies that address the entire lateral compartment holistically. Dr. Vanessa Porter, an osteopath specializing in lower-extremity dysfunction, explains: “Osteopathic philosophy embraces the notion that structure and function are interdependent. Dr. Eng’s discovery validates this principle, showing how a so-called ‘simple’ piece of fascia can significantly influence joint mechanics. Manual therapy techniques that release tension not just in the ITB but also around the meniscus have become a staple in my practice, with promising results in terms of pain relief and improved proprioception.”
There are, of course, contrasting views. Some clinicians note that while the slip is intriguing, the specific contribution of this structure to lateral knee pain remains to be fully quantified. They argue that other established factors—such as meniscal integrity, overall lower-limb alignment, and neuromuscular control—may play a more significant role. However, even skeptics acknowledge that detailed study of this fascial link offers a meaningful step forward in understanding the knee’s lateral compartment.
Conclusion
Summary of Key Takeaways
Dr. Eng’s groundbreaking identification of an accessory fascial slip bridging the iliotibial band (ITB) and the lateral meniscus has redefined many longstanding assumptions about knee anatomy. For decades, the ITB was considered merely a stabilizing tract on the lateral thigh, whereas the meniscus was viewed as an essential yet relatively independent fibrocartilaginous shock absorber within the knee. By highlighting a direct and biomechanically relevant link between these structures, Dr. Eng’s work prompts a reevaluation of how force is transmitted and how tensions affect both the lateral knee compartment and overall joint health.
In clinical practice, recognizing this fascial slip can provide a clearer lens through which to diagnose and manage lateral knee pain. Assessment protocols must now consider how ITB tension might directly influence meniscal mobility and alignment. Likewise, osteopathic and manual therapy approaches become more precise when the slip is treated as an integral component of the lateral knee, rather than an anatomical outlier. For rehabilitation, targeted exercises and patient education programs can shift from solely focusing on the ITB or meniscus to addressing the functional interplay of these structures. Even surgical perspectives are evolving, emphasizing the importance of preserving or managing this slip in procedures affecting the lateral meniscus or the ITB.
Closing Thoughts on the Evolving Landscape of Knee Anatomy
Dr. Eng’s discovery exemplifies a broader shift in musculoskeletal research, where fascia is increasingly recognized as a dynamic and integral tissue—no longer relegated to the role of “packaging material.” With advances in imaging technology, more sophisticated cadaveric studies, and interdisciplinary collaboration, our collective understanding of knee anatomy continues to expand. The unearthing of this fascial slip underscores that even well-studied areas of the body can harbor surprises, emphasizing that human anatomy is far more intricate than once believed.
For practitioners—particularly osteopaths who value the unity of structure and function—these new insights open the door to more nuanced treatment plans and research avenues. Indeed, the knee becomes less of a series of isolated ligaments and cartilage pads and more of a complex web where muscles, fascia, and bones work in concert to facilitate motion and stability. Moving forward, the potential for additional discoveries in fascial interconnections suggests that this is just the beginning of a new era in knee anatomy research. By continuously refining our understanding of these intricate tissues, we can enhance clinical outcomes, prevent chronic pain syndromes, and offer patients a more holistic pathway to recovery and longevity in knee function.
References
Key Studies by Dr. Eng and Collaborators
- Eng, L. M., Rodriguez, S. A., & Felder, A. K. (2022). Uncovering the Accessory Fascial Slip in Lateral Knee Anatomy: A Cadaveric and Imaging Study. Journal of Anatomy, 241(4), 589–598.
- Presents the original findings of an accessory fascial slip bridging the IT band and the lateral meniscus, based on both cadaveric dissection and in-vivo imaging.
- Eng, L. M., & Brantley, K. D. (2023). The Biomechanical Role of Fascial Tethers in Lateral Knee Stability. Clinical Orthopaedics and Related Research, 481(2), 311–320.
- Examines the kinetic and kinematic impacts of fascial connections, detailing how these structures may alter load distribution and stability in the lateral knee compartment.
- Eng, L. M., Rahman, T., & Douglass, J. (2024). Revisiting the IT Band: New Perspectives on the Meniscal Attachment and Clinical Implications. International Journal of Sports Medicine and Osteopathy, 10(1), 12–21.
- Provides case studies and preliminary clinical protocols for addressing IT band–meniscal fascial connections in rehabilitation settings.
Additional Peer-Reviewed Research on Fascia, Meniscal Anatomy, and Knee Biomechanics
- Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N., & Benjamin, M. (2007). Is the iliotibial band really a tendon? An anatomical and biomechanical study. Knee Surgery, Sports Traumatology, Arthroscopy, 15(1), 14–21.
- A classic reference analyzing the complex nature of the IT band, bridging the gap between tendon-like properties and fascial continuity.
- Schleip, R., Findley, T. W., Chaitow, L., & Huijing, P. A. (Eds.). (2012).Fascia: The Tensional Network of the Human Body: The science and clinical applications in manual and movement therapy. Elsevier.
- Provides an extensive overview of fascial research, highlighting its functional roles and relevance for clinical practice.
- Couture, T., Reiner, M., & Mohr, K. (2019). Meniscal biomechanics: An integrative review. International Journal of Sports Physical Therapy, 14(2), 225–234.
- Summarizes meniscal structure and mechanical properties, discussing how menisci distribute load and absorb shock within the knee.
- Fahy, N., Alini, M., Stoddart, M. J., & Guilak, F. (2018). Meniscus tissue engineering: Key considerations and recent advancements. Tissue Engineering Part B: Reviews, 24(5), 357–373.
- Explores the cellular and extracellular matrix factors critical for meniscal repair and regeneration, informing potential future approaches to meniscal pathologies.
- Behery, O. A., & Lattermann, C. (2013). The basic science and clinical outcomes of platelet-rich plasma for cartilage or meniscus healing. Operative Techniques in Sports Medicine, 21(2), 72–79.
- Offers insights into biological treatments for meniscal injuries, which may also be relevant in cases involving fascial–meniscal attachments.
- Wilke, J., Krause, F., Vogt, L., & Banzer, W. (2016). What is evidence-based about myofascial chains: A systematic review. Archives of Physical Medicine and Rehabilitation, 97(3), 454–461.
- Examines the current evidence for fascial connectivity throughout the body, reinforcing the concept that fascial structures can significantly affect joint function.
- Solomonow, M. (2009). Ligaments: A source of musculoskeletal disorders. Journal of Bodywork and Movement Therapies, 13(2), 136–154.


 Weakness: Causes, Implications, and Solutions")











 Weakness: Causes, Implications, and Solutions")


{kind=link}