

Adductor tendinopathy includes various conditions that occur in and around the tendon due to excessive and prolonged stress.
Introduction
Adductor tendinopathy is a set of conditions resulting from excessive and chronic use of the tendon, generating molecular alterations and collagen degradation. This process frequently leads to thickening of the tendon, a loss of its biomechanical characteristics and the emergence of pain.
The involvement of inflammation in adductor tendinopathy remains subject to debate. Studies have revealed a general absence of inflammatory cells around the lesion, calling into question the use of the term “tendinitis“. This highlights the complexity of the tissue response, suggesting that alternative mechanisms, such as structural alterations, could play a significant role.
On a molecular level, adductor tendinopathy involves separation and degeneration of collagen. These changes alter the biomechanical function of the tendon, contributing to its thickening. However, the direct correlation between these molecular changes and the manifestation of pain requires in-depth understanding.
It is crucial to recognize that this condition presents macroscopic manifestations such as tendon thickening, but also more subtle aspects related to molecular alterations. Understanding the multifactorial nature of adductor tendinopathy is of crucial importance for the development of effective therapeutic approaches.
The Complexity of Adductor Tendinopathy
Adductor tendinopathy poses a complex challenge, characterized by profound molecular alterations within the tendon. These changes, such as collagen degeneration, have a significant impact on tendon structure and function. Besides observable thickening, loss of biomechanical characteristics compounds the complexity of treatment and recovery.
At the molecular level, adductor tendinopathy causes major structural changes, particularly collagen degeneration. This molecular alteration compromises the resilience of the tendon, contributing to its thickening and deterioration of its biomechanical function. The macroscopic manifestation of tendon thickening is accompanied by more subtle challenges related to the loss of its biomechanical characteristics, making the condition complex to treat.
The difficulty in treating adductor tendinopathy lies in the need to restore not only the macroscopic structure of the tendon but also its biomechanical properties. The observed thickening is only one facet of the problem, and restoring tendon functionality requires a holistic approach taking into account molecular and structural aspects.
The focus on collagen degeneration highlights the importance of exploring innovative treatment strategies focused on collagen regeneration and preservation. Understanding the molecular mechanisms underlying adductor tendinopathy is essential for designing targeted interventions to restore tendon health comprehensively.
Evolution of Terminology
The evolution of medical language reflects the constant progression of our understanding of pathologies. In the context of conditions affecting tendons, a striking example of this evolution is the transition from the term “tendinitis” to “tendinopathy”. Initially, the former was widely used to describe these conditions, suggesting a predominant inflammatory component.
However, extensive research has revealed a complex reality. It was observed that, contrary to the inflammatory involvement suggested by the term “tendinitis”, there was frequently an absence of inflammatory components in tendon lesions. This observation led to a revision of medical vocabulary to better reflect the diverse nature of the changes observed at the structural and functional level of tendons.
The transition to the term “tendinopathy” marked a significant shift in our understanding of tendon conditions. This broader terminology more precisely encompasses the variety of alterations that tendons can undergo, going beyond simple inflammation. It recognizes that tendon disorders can involve molecular changes, structural alterations, and biomechanical modifications without necessarily including an active inflammatory process.
Thus, the change in medical language from “tendinitis” to “tendinopathy” demonstrates the ongoing effort to align terminology with emerging scientific knowledge. This development allows a more precise description of tendon conditions, encouraging a more nuanced diagnostic and therapeutic approach. It also highlights the importance of remaining adaptable in medical nomenclature to accurately reflect the complexity of disease processes, thereby promoting more effective and personalized healthcare.
Debate on Inflammation
The ongoing debate over the role of inflammation in adductor tendinopathy highlights the need for continued research to elucidate the mechanisms underlying this condition. Despite the frequent observation of the absence of inflammatory cells, calling into question the purely inflammatory aspect, it is crucial to recognize that other mechanisms could contribute to the pain and alterations observed in this pathology.
The absence of inflammatory cells around tendon lesions has raised questions about the use of the term “tendinitis” to describe adductor tendinopathy. This finding does not necessarily mean the complete absence of inflammation, but rather that other processes, perhaps degenerative or molecular in nature, may play a central role in the development of pain and tissue changes.
It is imperative to recognize the complexity of adductor tendinopathy and explore mechanisms beyond the traditional inflammatory paradigm. The observed alterations in the molecular structure of the tendon may be linked to degenerative processes, highlighting the need for an in-depth understanding of these mechanisms to guide treatment approaches.
Precise understanding of the mechanisms underlying adductor tendinopathy is crucial for the development of effective therapeutic approaches. Future research should focus on identifying molecular factors, structural changes, and degenerative processes that contribute to pain and progression of this condition. A holistic approach integrating these various elements could make it possible to develop targeted interventions aimed at treating not only the symptoms, but also the underlying mechanisms.
Treatment Approaches and Future Outlook
Faced with the complexity of adductor tendinopathy, it becomes imperative to adopt holistic treatment approaches, encompassing various aspects such as rehabilitation, load management, and targeted methods. Understanding the multifactorial nature of this condition requires a comprehensive approach that goes beyond simply alleviating symptoms.
Rehabilitation plays a crucial role in the management of adductor tendinopathy. Adapted programs aimed at strengthening the tendon, improving biomechanics and promoting tissue repair can contribute to recovery. Load management, adjusting activities to avoid overuse, is also essential to prevent recurrence and promote lasting recovery.
The future of adductor tendinopathy management could also benefit from advances in the field of tissue regeneration. Innovative therapies, such as cell therapy or growth factors, could offer promising prospects to stimulate healing and restore tendon function more effectively. The introduction of more personalized methods, based on individual patient characteristics, could also revolutionize the way we approach the treatment of this condition.
As a practitioner of osteopathy, these advances in the understanding and treatment of adductor tendinopathy are of paramount importance. We seek to provide useful and up-to-date information through our blog, Osteomag, to support those facing this condition. By encouraging an integrated approach that combines different treatment modalities, we aim to support the effective management of adductor tendinopathy, while remaining attentive to constant developments in research and healthcare. Our commitment to integrating this emerging knowledge into daily practice aims to improve the quality of care we provide to our patients.
Why adductor muscle overuse prefer to react in a non inflammatory manner (tedinopathy) instead with a inflammatory (tendinitis) one
The preference of adductor tendons (and tendons in general) to react in a non-inflammatory manner is related to their unique structure and function. Unlike some other tissues in the body, tendons have a relatively poor blood supply. This limited blood flow makes it challenging for the body to mount a robust inflammatory response in these areas.
When tendons experience stress or overuse, they tend to undergo a degenerative process rather than a classic inflammatory one. This is often characterized by changes in the tendon’s structure, such as microtears, collagen disorganization, and an increase in non-inflammatory cells like fibroblasts. This process is what is referred to as tendinopathy.
The limited blood supply to tendons means that the healing response is not as quick or pronounced as in more vascularized tissues. Instead of a rapid inflammatory reaction, the body’s response in tendons is more focused on repairing and remodeling the tissue over time. This is why a tendinopathic response, involving degenerative changes, is more common in tendons, including those in the adductor region.
Understanding these mechanisms is crucial for effective diagnosis and management of adductor tendinopathy, often involving targeted rehabilitation, modification of activities, and sometimes interventions to promote tissue healing. If you have specific cases or aspects you’d like to delve into, feel free to share more details, André.
Anatomy of the Adductors
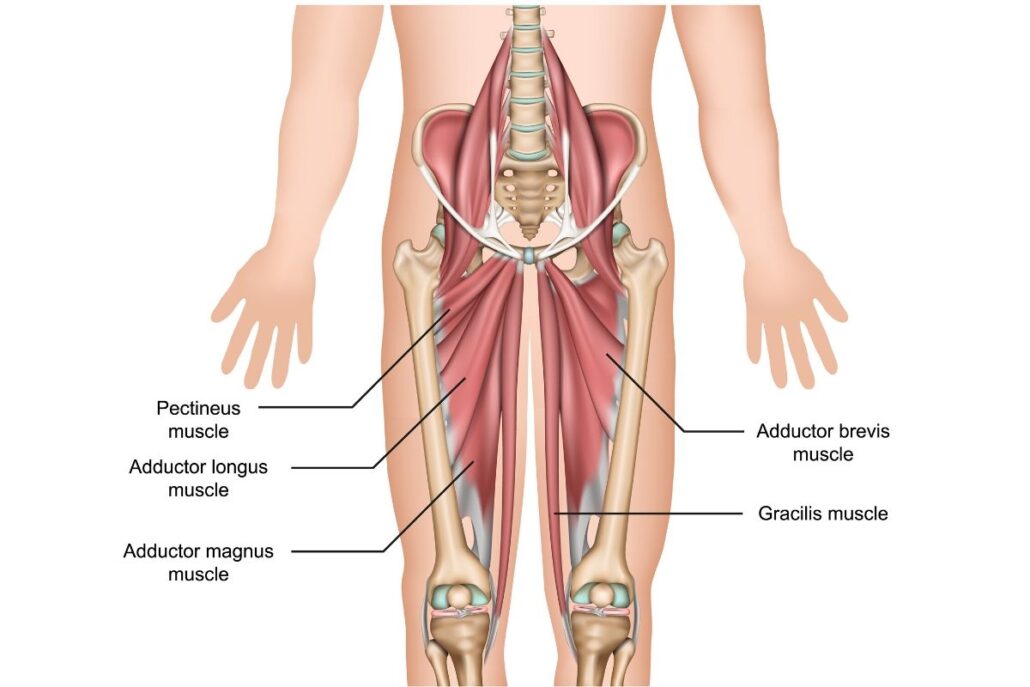
The adductors are a group of muscles located on the inner thigh, playing a vital role in the stability and movement of the pelvis. Made up of several muscles, the main ones being the adductor longus, the adductor brevis, and the adductor medius, these muscles work together to bring the leg closer to the middle of the body.
- Location of the Adductors: The adductors extend along the inner side of the thigh, attached to the pubic bone and inserting on the femur. Their fan-shaped arrangement allows for fluid and coordinated movement during contraction.
- Main Functions: The adductors are responsible for adduction of the thigh, that is to say the movement of the leg towards the midline of the body. This action is crucial for movements as simple as walking, as well as more complex activities like running, jumping, or playing sports such as soccer and tennis.
- Importance in Pelvic Stability: In addition to their role in movement, the adductors contribute to pelvic stability. Working in tandem with the abductor muscles, they maintain the necessary balance between the two sides of the pelvis.
- Injury Prevention: Due to their involvement in a variety of physical activities, the adductors can be prone to injury, especially when overused. A proper warm-up and specific stretches can help prevent injuries and keep these muscles flexible.
Causes of adductor tendinopathy
The causes of adductor tendinopathy are multiple and often linked to factors of overuse, excessive stress, and degenerative mechanisms in the tendon. One of the main causes lies in excessive and repetitive strain on the adductors, the muscles responsible for bringing the lower limbs together. This overuse may result from specific sporting activities, particularly those involving rotational movements, frequent changes of direction, or heavy loading, as is often the case in ball sports or activities requiring lateral movements.
Anatomical factors also play a role in the development of adductor tendinopathy. A particular pelvic morphology, excessive rotation of the femur, or muscular imbalances can create additional stress on the adductor tendons, thus contributing to their vulnerability. These anatomical factors may be inherent to the person or result from poorly compensated muscular imbalances.
Furthermore, errors in training technique or abrupt changes in the intensity or type of physical activity can also be triggers for adductor tendinopathy. Poor technique when performing movements, insufficient warm-up, or periods of inactivity followed by resumptions of intense activity can increase the risk of developing this condition.
Direct trauma, although less common, can also contribute to adductor tendinopathy. Impacts, shocks, or acute injuries can damage the tendon, thus triggering inflammatory and degenerative processes.
Finally, certain lifestyle factors can influence the occurrence of adductor tendinopathy. A lack of adequate rest, insufficient sleep, an unbalanced diet, or stressful lifestyle habits can weaken the musculoskeletal system, making tendons more susceptible to injury.
- Overuse or Intense Physical Activity: Excessive use of the adductor muscles, often due to intense sporting activity, repetitive training or sudden movements, can lead to microtrauma to the tendons, thus contributing to the development of tendinopathy.
- Lack of Warm-up or Stretching: Inadequate warm-up before physical activity or lack of proper stretching can increase the risk of adductor injuries. Poorly prepared muscles are more likely to experience excessive stress.
- Improper Training Technique: Using improper technique when performing exercises, especially those involving the adductor muscles, can put excessive strain on the tendons, eventually leading to tendinopathy.
- Muscular Imbalances: An imbalance between the adductor and abductor muscles can disrupt the alignment of the pelvis, leading to overload of the adductor tendons. This can result from muscle weakness, poor posture, or neglecting certain muscle groups in training.
- Anatomical Factors: Some individuals may be predisposed to adductor tendinopathy due to their anatomy, such as the shape of the pelvis or variations in muscle structure.
- Underlying Medical Conditions: Certain medical conditions, such as arthritis, may increase the risk of adductor tendinopathy. Likewise, poor blood circulation or inflammatory conditions can contribute to this condition.
- Overtraining: Excessive training volume without adequate recovery periods can lead to muscle fatigue and increase the risk of injury, including adductor tendinopathy.
Symptoms of adductor tendinopathy
The symptoms of adductor tendinopathy are varied and can significantly affect the quality of life of affected individuals. One of the most common signs is localized pain on the inner thigh, near the junction with the pubis. This pain may be felt during physical activity, but it may also persist at rest, interfering with daily activities.
Increased sensitivity to touch in the adductor region is also a common symptom. People with adductor tendinopathy may feel pain when palpating the affected area, indicating an inflammatory reaction or structural alterations in the tendon.
Joint mobility may be reduced due to pain and stiffness associated with adductor tendinopathy. Movements such as hip extension, abduction, or internal rotation can trigger discomfort, thereby limiting the hip’s range of motion.
The symptom of tendon thickening is also seen in adductor tendinopathy. An ultrasound or magnetic resonance imaging (MRI) may reveal enlargement of the tendon, a sign of underlying structural changes.
In some cases, adductor tendinopathy can cause lameness or impair the affected person’s normal gait. This is often a protective response by the body to avoid putting further strain on the damaged tendon, but it can also lead to muscle and joint imbalances.
It is important to note that adductor tendinopathy can manifest variably from one individual to another, and the severity of symptoms can also vary. Some may experience mild pain and moderate discomfort, while others may experience severe pain and significant limitation of function.
- Pain: Pain is the most common symptom of adductor tendinopathy. It is usually felt on the inside of the thigh, along the adductor line. The pain can be acute or chronic and may increase with physical activity.
- Sensitivity to Touch: The affected area may be sensitive to touch. Light pressure on the adductor tendons can trigger or intensify the pain.
- Muscle Stiffness: The adductor muscles can become stiff, which can lead to decreased flexibility and mobility in the thigh region.
- Swelling: In some cases, slight swelling may occur around the affected area, indicating an inflammatory reaction.
- Pain During Activity: Pain may worsen during or after physical activities, especially those involving rotational movements of the thigh or changes in direction.
- Nighttime Pain: Some individuals may experience worsening pain during the night, disrupting sleep.
- Muscle Weakness: Adductor tendinopathy can lead to muscle weakness in the affected thigh, which can result in decreased strength during physical activity.
- Crepitations: In some cases, crepitations or grinding sounds may be felt during thigh movements, which may indicate abnormalities in the tendons.
Pathophysiology of adductor tendinopathy
The pathophysiology of adductor tendinopathy is complex, involving molecular and structural processes within the tendon. This condition often results from chronic overuse, exposing the adductors to excessive stress. At the molecular level, significant alterations occur, including degeneration of collagen, an essential component of tendon structure.
Prolonged overuse leads to repeated microtrauma to the adductor tendon. These microtraumas induce a complex tissue response. Collagen degeneration, characterized by separation and degradation of this key structural protein, compromises tendon strength and flexibility. These molecular changes contribute to tendon thickening, a macroscopic feature often seen in adductor tendinopathy.
Another facet of pathophysiology lies in the ongoing debate over the role of inflammation. Despite the frequent absence of inflammatory cells around tendon injuries, some experts suggest that subclinical inflammatory processes may be present. This duality highlights the complexity of the tissue responses involved in adductor tendinopathy, requiring in-depth exploration of potential inflammatory mechanisms.
Impaired vascularization is also a key aspect of the pathophysiology. Tendons have limited vascularity, which can hinder the ability of the adductor tendon to regenerate effectively. Inadequate blood flow compromises the supply of essential nutrients and repair cells, contributing to the progression of tendinopathy.
The pathophysiology of adductor tendinopathy highlights the importance of understanding the underlying mechanisms to guide treatment approaches. Therapeutic interventions should aim to attenuate molecular alterations, promote tissue regeneration and restore tendon biomechanical function. Rehabilitation strategies, load management and potential advances in regenerative therapies could play a vital role in the management of this complex condition.
- Repetitive Strain Injuries: Adductor tendinopathy is often associated with repetitive strain injuries resulting from excessive strain or overuse of the adductor muscles. These microtraumas can occur during sporting activities, repetitive movements or excessive load on the tendons.
- Inflammation: Microtrauma causes an inflammatory response in the adductor tendons. Inflammation is characterized by the release of pro-inflammatory chemical mediators, leading to increased blood flow and infiltration of immune cells into the affected area.
- Collagen Degradation: Overuse and chronic inflammation can lead to the breakdown of collagen, the main structural protein of tendons. This breakdown of connective tissue weakens tendons and compromises their ability to withstand mechanical loads.
- Cellular Alterations: Tendon cells (tenocytes) can undergo alterations in their function and structure in response to microtrauma and inflammation. This contributes to tendon dysfunction and progression of tendinopathy.
- New Vessel Formation: In some cases, new blood vessels (new blood vessels) may form in the tendon area, which is a sign of response to ongoing inflammation.
- Fibroblast Response: Fibroblasts, responsible for collagen synthesis, can be activated in order to repair tissue damage. However, unbalanced regulation of this response can lead to the formation of abnormal scar tissue.
- Alterations in the Extracellular Matrix (ECM): The extracellular matrix, composed primarily of collagen and other proteins, undergoes alterations that affect the structure and function of the tendon. These changes compromise the normal strength and elasticity of the tendon.
Adductor tendinopathy is often multifactorial, involving both mechanical factors, such as overload and repetitive strain, and biological factors, such as inflammation and tissue breakdown. A thorough understanding of pathophysiology is crucial to guide treatment approaches, which may include load management, muscle rehabilitation, physical therapy, and in some cases, specific medical interventions.
Differential diagnoses of adductor tendinopathy
- Inguinal Hernia: An inguinal hernia can cause pain in the groin area and can sometimes be confused with adductor tendinopathy.
- Hip Pathologies: Hip joint problems, such as hip arthritis or coxarthrosis, can manifest as groin pain and can be confused with an adductor condition.
- Pubalgia: Pubalgia, also known as adductor syndrome, can cause pain in the groin area and can be confused with adductor tendinopathy. However, pubalgia often involves inflammation of the pubic structures rather than the adductor tendons specifically.
- Hip Bursitis: Inflammation of the bursae around the hip can lead to symptoms similar to adductor tendinopathy.
- Ilioinguinal Nerve Pathologies: Irritation or compression of the ilioinguinal nerve can cause pain in the inguinal region and can be considered as a differential diagnosis.
- Gynecological or Urological Conditions: In women, gynecological conditions such as endometriosis or urological problems can sometimes manifest as pain in the pelvic region and be confused with adductor problems.
- Hip or Pelvic Fractures: Hip or pelvic fractures can cause acute pain in the groin area and require evaluation to rule out these emergency situations.
It is important to consult a healthcare professional for an accurate diagnosis, as management may vary depending on the underlying condition. Medical tests, such as medical imaging (MRI, x-rays) and clinical examinations, are often used to confirm the diagnosis and develop an appropriate treatment plan.
Therapeutic approach
- Rest and Avoidance of Irritating Activities: Reducing activities that exacerbate pain is crucial. Relative rest allows tissues to heal and recover. Avoiding movements or activities that excessively strain the adductors is often recommended.
- Ice and Compression: Applying ice can help reduce inflammation and pain. The use of cold compresses may be beneficial, especially in the early stages of the injury.
- Elevation and Rest: Elevating the affected leg can help reduce swelling and promote blood circulation.
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): NSAIDs, such as ibuprofen, may be prescribed to reduce pain and inflammation. However, their prolonged use should be supervised by a healthcare professional due to possible side effects.
- Physical Therapy: Strengthening and stretching exercises, prescribed by an osteopath, can help restore adductor strength and flexibility. Rehabilitation techniques can also be used to improve pelvic stability and biomechanics.
- Shock Wave Therapy: This technique involves applying acoustic waves to the affected area to stimulate tissue healing.
- Infiltrations Corticosteroids: In some cases, corticosteroid injections may be used to reduce local inflammation.
- Surgical Intervention: If conservative measures are not effective, surgery may be considered, although this is generally reserved for severe and treatment-resistant cases.















{kind=link}