

During the osteopathic examination, it is important to recognize the somatovisceral and viscerosomatic reflexes in order to reach a differential diagnosis. The trigger points of the pectoralis major provide an example of each phenomenon. A myofascial syndrome of the pectoralis major will cause a faster heartbeat by somatovisceral reflex. A more accelerated heartbeat will cause by viscerosomatic reflex a myofascial syndrome in the pectoralis major.
This vicious cycle between the muscle fibers of the pectoralis major and the heart is nourished in patients who have a slumped posture and rounded shoulders. This posture causes greater myofascial tension in the pectoralis major, but can also lead to heart rhythm dysfunction, a demonstrable somatovisceral reflex.
The viscero-somatic reflexes are the somatic reflection of a visceral pathology. How to distinguish, with the help of palpation, a tissue that has reacted to a viscerosomatic reflex or that is in somatic dysfunction. Beal, suggests that the more the area of dysfunction extends, the more the viscera becomes responsible for the dysfunction. Localized textural changes in the skin and subcutaneous tissues also provide indications of the severity and acuity or chronicity of the underlying visceral pathology
Osteopathy
The osteopathic profession has always recognized the truth of certain basic principles, namely that altered or deficient function manifests itself effectively at the level of the somatic system, that these somatic factors can manifest as presymptomatic signs of disease and that they can take the form of local or distant manifestations of a dysfunction such as somatovisceral or viscero-somatic reflexes.
Although these notions are accepted as basic principles of osteopathic philosophy, there is little scientific data other than clinical experience to support them.
define the viscero-somatic reflex
A viscerosomatic reflex is the resonance of the consequence of afferent stimuli resulting from a visceral disorder on somatic tissues. The reflex is triggered by afferent signals from visceral receptors; they are transmitted to the dorsal column of the spinal cord, where they synapse with interconnected neurons. These in turn carry the stimulus to sympathetic and peripheral motor outputs, resulting in sensory and motor changes in the somatic tissues of skeletal muscles, viscera, blood vessels, and skin.
Supraventricular tachyarrhythmias
Supraventricular tachyarrhythmias have been documented to originate from the trigger point located in the right pectoralis major (at the level of the fifth intercostal space), midway between the sternal margin and the nipple line (2).
- Treatment of the somatovisceral reflex will be
- Release the trigger point
- Correct the underlying postural problem if present.
- Correction of this somatic dysfunction results in an immediate return of normal heart function (19).
Clinical symptoms attributed to the autonomic sequelae of myofascial dysfunction include (1, 2,8, 19):
- Diarrhea and dysmenorrhea
- Decreased gastric motility
- Headache
- Proprioceptive disorders and dizziness
- Excessive maxillary sinus secretion
- Cardiac arrhythmias
- Ptosis, excessive tearing, conjunctival redness
Heart disease (2) will have the viscosomatic reflex to trigger trigger points in the pectoral.
- They occur as a result of coronary artery disease.
- This example of a viscerosomatic reflex has a significant prevalence as demonstrated in a study of 72 patients.
- Dorsal muscle trigger points have been reported in 61% of patients with heart disease (2).
- The treatment of these points is an important factor in the reduction of the coronary reflex (19), but also the reduction of back pain.
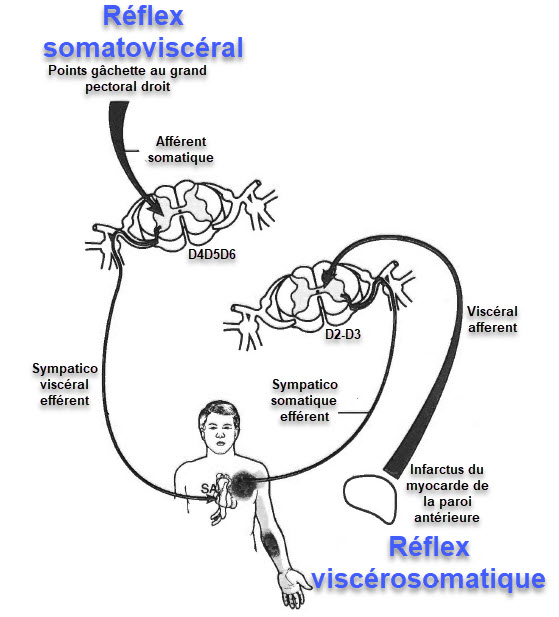
Pectoral trigger points and associated reflexes. HER, sinoatrial node of the heart.
Posture and heart condition
- A posture or activity that activates a TrP, if it is not corrected or if it is continued, can also perpetuate it.
- TrPs of the pectoralis major are activated and perpetuated by a round shoulder posture because it produces a sustained shortening of the pectoral muscles.
- This activation is likely to occur during prolonged sitting and when reading and writing.
- Conversely, the shortening of the TrP in this muscle can induce such a posture.
- The major TrPs of Pectoralis can be triggered or reactivated in several ways:
- by heavy lifting (especially when overuse of the adduction of the arms (use of manual hedge trimmers),
- by lifting supported in a fixed position (use of an electric saw),
- by immobilizing the arm in the adduct position (sling or cast arm),
- by sustained high levels of anxiety, or by exposure
- Muscles tired in cold air (sitting in the shade in a wetsuit after swimming, or when exposed to the draft of an air conditioner).
- Acute myocardial infarction returns pain from the heart to the midline of the major and minor pecs.
Injury to the heart muscle triggers a viscosomatic process that activates trigger points in the pectoral muscles.
After an acute infarction, these self-sustaining trigger points tend to persist in the chest wall unless they are released.
Reference
- Simons DG, Travell JG, Simons LS . Travell and Simons’ Myofascia! Pain and Dysfimction: The Trigger Point Manual. Volume 1: Upper HalfofBody, 2nd ed. Baltimore MD: Williams & Wilkins; 1999.
- Travell JG, Simons DC. Myofoscial Pain and DysfUnction: The Trigger Point Manual. Volume I. The Upper Extremities. Baltimore, MD: Williams & Wilkins; 1983.













{kind=link}