



Introduction
Biceps tendon rupture is a relatively common injury that occurs when the tendon that attaches the biceps muscle to the bone is torn or ruptured. This injury may occur suddenly during strenuous activity or weight lifting, or it may result from gradual wear and tear from repetitive movements or age-related degeneration.
Symptoms of a biceps tendon rupture can vary depending on the severity of the injury. In severe cases, where the tendon is completely ruptured, people may feel severe pain in the shoulder or elbow at the time of injury, followed by sudden weakening or inability to flex or lift the arm . In less severe cases, persistent shoulder or elbow pain, muscle weakness, and an abnormal bump or protrusion near the joint may be seen.
Treatment for a biceps tendon rupture depends on several factors, including the severity of the injury, the person’s age and activity level, and their recovery goals. In some cases, especially in older people or those whose activities do not require maximum muscle strength, conservative treatment may be recommended. This may include measures such as rest, ice application, use of anti-inflammatories, and gradual rehabilitation to restore strength and mobility.
However, in cases where tendon rupture results in significant loss of function or the person is active and requires optimal muscle strength, surgery may be recommended. Surgery usually aims to reattach the tendon to the original site or attach it to another location on the bone to restore muscle function. After surgery, a period of intensive rehabilitation is often necessary to strengthen the surrounding muscles, improve mobility and promote full recovery.
It is important to note that even with proper treatment, recovery from a ruptured biceps tendon can take time and require a commitment to the rehabilitation process. Complications such as joint stiffness, persistent weakness, or recurrence of the injury are possible, especially without proper rehabilitation.
Prevention of biceps tendon ruptures may be possible by adopting proper lifting techniques, avoiding sudden and excessive movements, strengthening the shoulder and arm muscles through regular exercise, and consulting a healthcare professional to treat any persistent pain or weakness. Good physical preparation and adequate warm-up before exercise or physical activity can also help reduce the risk of injury.
Symptoms of Biceps Tendon Rupture
Biceps tendon rupture manifests itself by several distinctive symptoms which may vary depending on the severity of the injury and the anatomical particularities of each individual. One of the most common symptoms is severe pain in the arm, which can occur suddenly during the activity that caused the injury or gradually over time if the tendon degenerates. This pain may be located near the shoulder or elbow, depending on where the rupture occurs.
In addition to pain, a tearing or popping sensation in the arm may be felt at the time of injury. Immediately afterwards, it is common to observe swelling and hematoma in the affected area, resulting from the accumulation of blood and lymphatic fluid in the damaged tissues. This swelling may be associated with increased sensitivity to touch and local warmth.
Another common symptom of biceps tendon rupture is significant weakness in the affected arm. Patients may have difficulty performing simple movements such as bending the elbow or rotating the forearm, and may experience a feeling of looseness or heaviness in the arm. This weakness can make daily activities difficult and limit the ability to use the arm normally.
In addition to physical symptoms, biceps tendon rupture can also have a psychological impact on patients. Pain, loss of strength and limitation of activities can lead to feelings of frustration, depression and anxiety, especially in people who are very active or dependent on the use of their arms in their work or hobbies.
It is important to note that the symptoms of biceps tendon rupture can vary from person to person, and some patients may not experience all of the symptoms described. Additionally, symptom management may differ depending on the severity of the injury and the individual needs of the patient. In all cases, it is recommended to consult a healthcare professional for an accurate diagnosis and appropriate treatment plan.
Bicipital tendon rupture can present with several symptoms, which can vary depending on the severity of the rupture. Here are some common symptoms associated with a bicipital tendon rupture:
- Sudden pain: Bicipital tendon rupture is often associated with sharp, sudden pain in the front of the arm. The pain can be severe, and it may occur at the time of the injury.
- An audible “pop”: Some patients report hearing a tearing sound or “pop” as the tendon ruptures.
- Swelling: Swelling may develop in the front of the arm, near the shoulder or elbow, due to inflammation associated with the rupture.
- Muscle weakness: Rupture of the bicipital tendon can lead to decreased muscle strength in the arm, especially when flexing the elbow. The person may have difficulty lifting objects or performing movements that strain the biceps muscle.
- Arm deformity: In some cases of complete tendon rupture, there may be a visible deformity or abnormal protrusion of the biceps muscle. This may be noticeable when the arm is flexed.
- Difficulty performing certain movements: Arm movements, particularly elbow flexion, can be painful and difficult to perform.
- Bruising: Bruising may appear around the affected area due to the traumatic impact or inflammation associated with the rupture.
Anatomy of the Biceps Tendon
- The biceps tendon is a vital component of the musculoskeletal system, connecting the biceps brachii muscle to bones in the shoulder and elbow. It plays a crucial role in upper limb movement, including flexion and supination of the forearm, as well as stabilizing the shoulder joint. Understanding the anatomy and function of the biceps tendon provides essential insights into its vulnerability to injuries like ruptures.
- Structure and Function
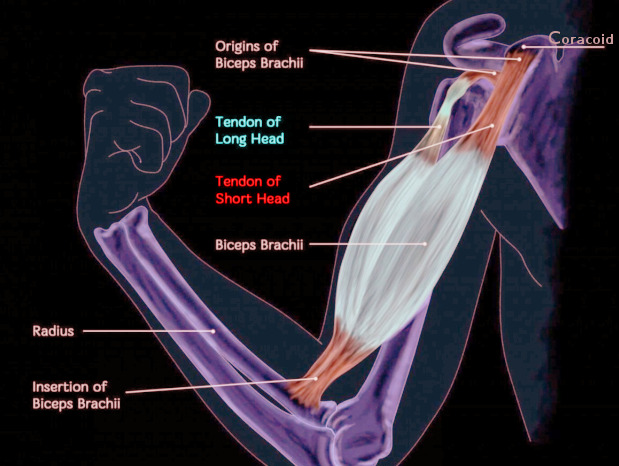
- The biceps tendon is divided into two distinct sections corresponding to the two heads of the biceps brachii muscle:
- Long Head of the Biceps (LHB): This tendon originates from the supraglenoid tubercle of the scapula and passes through the bicipital groove in the humerus. The long head is more prone to wear and tear due to its course through the shoulder joint, where it endures significant mechanical stress.
- Short Head of the Biceps (SHB): This tendon arises from the coracoid process of the scapula. Unlike the long head, the short head is less commonly injured due to its anatomical location and reduced exposure to tensile forces.
- The biceps tendon attaches distally at the radial tuberosity of the radius, facilitating forearm supination (rotating the palm upward) and elbow flexion. Additionally, the biceps muscle plays a minor role in stabilizing the shoulder joint by preventing dislocation during arm movements.
- Role in Shoulder and Elbow Stability
- Beyond its primary functions, the biceps tendon contributes to the overall stability of the shoulder and elbow:
- Shoulder Stability: The long head of the biceps acts as a dynamic stabilizer of the glenohumeral joint. It prevents excessive forward or downward displacement of the humeral head during arm movements, especially overhead activities.
- Elbow Stability: The biceps tendon works synergistically with other muscles and ligaments to maintain the integrity of the elbow joint during dynamic actions such as lifting or pushing.
- The biceps tendon’s role in stabilization makes it susceptible to injuries from repetitive motions or sudden traumatic forces, particularly in active individuals and athletes.
- Common Sites of Rupture (Proximal vs. Distal)
- The biceps tendon is most vulnerable to rupture at two key sites: proximal and distal.
- Proximal Ruptures:
- Most ruptures occur at the long head of the biceps tendon.
- Commonly associated with degenerative changes, repetitive strain, or chronic tendinitis.
- Proximal tears often cause a characteristic “Popeye” deformity, where the muscle belly retracts downward.
- Distal Ruptures:
- Less common, accounting for approximately 3-5 cases per 100,000 annually.
- Typically caused by acute trauma, such as lifting a heavy object with an extended arm.
- Distal ruptures lead to a loss of supination strength and elbow flexion power.
- In both cases, the severity of the rupture and its impact on function depend on the extent of tendon damage and associated conditions, such as rotator cuff tears or tendinopathy.
- Understanding the anatomy and function of the biceps tendon underscores its importance in upper limb mechanics and highlights the need for proper care to prevent and manage injuries effectively.
Types of Bicipital Tendon Tears
icipital tendon tears can occur due to acute trauma, overuse, or degenerative changes. These injuries are classified into three primary types: proximal tears, distal tears, and chronic issues like tendinitis and micro tears. Understanding these variations helps in diagnosing the condition and tailoring appropriate treatment.
Proximal Tears: Characteristics and Effects
Proximal tears affect the tendon that connects the long head of the biceps (LHB) to the shoulder. These are the most common type of bicipital tendon tears, often caused by repetitive overhead motions, degenerative changes, or sudden trauma.
- Characteristics:
- Proximal tears usually begin with fraying of the tendon, progressing to partial or complete rupture.
- Partial tears can cause persistent pain, tenderness, and weakness, particularly during overhead activities or shoulder rotations.
- A complete tear often results in a visible “Popeye” deformity, where the biceps muscle retracts downward toward the elbow.
- Effects:
- Proximal tears typically lead to reduced arm strength and discomfort but may not significantly affect daily activities in less active individuals.
- In athletes or physically active individuals, the loss of tendon function can hinder performance and stability, often necessitating surgical repair.
Distal Tears: Rarity and Symptoms
Distal tears occur at the tendon connecting the biceps to the radial tuberosity in the forearm. These injuries are less common, accounting for only 3-5 cases per 100,000 annually, and are more frequently seen in men aged 30-50.
- Characteristics:
- Typically result from sudden, forceful stress, such as lifting heavy weights or catching a falling object.
- The tendon may tear partially or completely, with complete tears often causing a “pop” sensation and visible deformity.
- Symptoms:
- Loss of strength in elbow flexion and forearm supination (turning the palm upward).
- Swelling, bruising, and difficulty performing tasks requiring strong arm movements.
- If untreated, compensatory use of other arm muscles can lead to improper biomechanics and further issues.
Tendinitis and Micro Tears: Chronic Issues
Tendinitis and micro tears develop gradually due to overuse, repetitive strain, or degenerative changes in the biceps tendon. These are common in individuals with repetitive arm motions, such as athletes or manual laborers.
- Characteristics:
- Inflammation of the tendon, particularly in the long head, leading to pain and stiffness.
- Chronic wear can result in tiny micro tears, increasing the risk of complete rupture.
- Symptoms:
- Persistent pain, especially with movement.
- Swelling and tenderness in the shoulder.
- Decreased range of motion and functional limitations.

Causes of Biceps Tendon Rupture
Biceps tendon rupture is a traumatic injury that typically occurs during strenuous activity involving a sudden movement of the arm, such as when lifting a heavy object or during a sudden forceful movement. This type of injury is often associated with sports such as weightlifting, tennis, or baseball, where the biceps tendon is put under extreme stress. Biceps tendon rupture can also result from progressive degeneration due to natural wear and tear of the tissues, especially in older people.
When a biceps tendon rupture occurs, it is often accompanied by immediate severe pain in the arm, followed by swelling and hematoma in the affected area. Patients may also experience significant weakness in the affected arm, as well as loss of the ability to perform certain movements, such as bending the elbow or rotating the forearm.
Treatment for biceps tendon rupture depends on several factors, including the severity of the injury, the patient’s age and activity level, and their recovery goals. In some cases, a conservative approach, such as rest, ice, anti-inflammatories, and rehabilitation, may be recommended to relieve pain and restore muscle function. However, in more severe cases or in younger, active patients, surgery to repair the tendon may be necessary.
Rehabilitation after a ruptured biceps tendon is a crucial step in the recovery process, aimed at restoring strength, flexibility and mobility to the affected arm. Progressive strengthening exercises, under the supervision of a physical therapist, are often recommended to help rebuild weakened muscles and prevent long-term complications, such as joint stiffness or loss of muscle strength.
Bicipital tendon rupture can be caused by a variety of factors, whether related to acute trauma, age-related wear and tear, or overuse of the biceps muscle. Here are some of the main causes of bicipital tendon rupture:
- Acute trauma: A sudden injury, such as a fall onto the extended arm or direct impact to the arm, can cause a rupture of the bicipital tendon. This can occur during sports accidents, falls or other traumatic incidents.
- Age-related wear and tear: With aging, tendons tend to gradually wear out due to degenerative processes. Reduced flexibility and strength of tendons increases the risk of rupture. Older people may be more likely to experience a bicipital tendon rupture due to these age-related changes.
- Overuse: Repetitive activities involving the arm, especially repeated elbow flexion, can contribute to wear and tear of the bicipital tendon. This may be seen in athletes participating in certain sports or in individuals performing physically demanding work or household tasks.
- Pre-existing conditions: Certain medical conditions, such as tendinopathy (inflammation of the tendon), arthritis, or other connective tissue disorders, can weaken tendons and increase the risk of rupture.
- Medications and injections: Certain medications, especially corticosteroids, can weaken tendons and increase the risk of rupture. Additionally, repeated injections of corticosteroids into the tendon area can also contribute to tendon weakening.
It is important to note that bicipital tendon rupture is often the result of a combination of these factors rather than a single isolated cause. People who experience persistent pain, weakness, or other symptoms in the arm should consult a healthcare professional for an accurate diagnosis and appropriate treatment recommendations.
Predisposing Factors
Several factors can predispose a person to a bicipital tendon rupture. These factors can increase the vulnerability of the tendon and increase the risk of injury. Here are some of the predisposing factors for bicipital tendon rupture:
- Age: The risk of bicipital tendon rupture increases with age. Tendons tend to lose their elasticity and strength over the years, making older people more likely to experience tendon ruptures.
- Gender: Men generally have a higher risk of bicipital tendon rupture than women. This may be due to anatomical and hormonal differences.
- Intensive physical activities: Participating in intensive physical activities, especially those that frequently strain the biceps muscle, can increase the risk of tendon rupture. This includes throwing sports, intense strength training, and other activities requiring frequent use of the arm.
- Pre-existing tendinopathies: Tendinopathies, such as chronic inflammation of the tendon (tendinitis), can weaken the bicipital tendon and increase the risk of rupture. Untreated tendinopathy can progress to tendon rupture.
- Medical Conditions: Certain medical conditions, such as arthritis, diabetes, and other metabolic disorders, can weaken tendons and increase the risk of rupture.
- Use of corticosteroids: Regularly taking corticosteroid medications can weaken tendons and increase the risk of rupture. This may be due to suppression of the normal healing process of the tendons.
- Individual anatomy: Some individuals may have an anatomy that makes them more predisposed to tendon ruptures. This may include variations in tendon structure or genetic factors.
- Improper training techniques: Using improper training techniques, including excessive loads or poor weight lifting technique, can increase the risk of bicipital tendon injury.
Diagnosis of Bicipital Tendon Injuries
Accurate diagnosis of bicipital tendon injuries is essential to ensure effective treatment and recovery. Diagnosis typically involves a combination of clinical examination and imaging techniques, which help identify the severity and location of the injury.
Clinical Examination
A thorough clinical examination is the first step in diagnosing bicipital tendon injuries. During the assessment, the healthcare provider will review the patient’s medical history, focusing on symptoms, recent activities, and any incidents that may have caused the injury. Key elements of the clinical examination include:
- Physical Inspection:
- Visible signs of injury, such as swelling, bruising, or deformities like the “Popeye” sign (a bulge in the lower arm from a retracted biceps muscle) in cases of complete rupture.
- Observation of muscle atrophy or abnormal movement patterns.
- Palpation:
- Gentle pressure along the tendon to locate tenderness or detect gaps in the tendon, which may indicate a tear.
- Assessment of pain or swelling near the shoulder or elbow.
- Range of Motion and Strength Testing:
- Evaluation of arm and shoulder movement to detect pain, stiffness, or limitations.
- Testing biceps strength by having the patient flex the elbow or supinate the forearm against resistance. Weakness or pain during these tests suggests tendon damage.
- Specialized Tests:
- Speed’s Test: Pain in the bicipital groove when the arm is lifted against resistance indicates long head tendon issues.
- Yergason’s Test: Pain or discomfort during resisted supination points to biceps tendon pathology.
- Hook Test: Inability to hook the biceps tendon with a finger near the elbow suggests a distal tendon rupture.
Imaging Techniques (MRI, Ultrasound)
While clinical examination provides critical clues, imaging is often used to confirm the diagnosis, assess the extent of the injury, and rule out other conditions.
- MRI (Magnetic Resonance Imaging):
- Provides detailed images of soft tissues, including the biceps tendon.
- Effective for detecting partial tears, complete ruptures, and degenerative changes.
- Helps identify associated injuries, such as rotator cuff tears or labral damage.
- Ultrasound:
- A dynamic, cost-effective tool for visualizing tendon injuries in real time.
- Useful for detecting partial tears, inflammation, or fluid accumulation around the tendon.
- Can assess tendon movement during specific arm motions, aiding in diagnosis.
Prevention Tips for Bicipital Tendon Injuries
Preventing bicipital tendon injuries involves maintaining proper biomechanics, strengthening the muscles and tendons, and addressing potential risk factors. By incorporating preventive strategies into daily routines or exercise programs, individuals can reduce their risk of injury and maintain healthy tendon function.
Proper Lifting Techniques
One of the most common causes of biceps tendon injuries is improper lifting, especially during strenuous activities or weight training. To prevent unnecessary stress on the tendons:
- Use Correct Form: Keep the back straight, engage the core muscles, and use the legs to lift heavy objects instead of relying solely on the arms or shoulders.
- Avoid Jerky Movements: Lift weights or objects in a controlled manner, minimizing sudden or excessive forces on the tendons.
- Distribute the Load: When lifting, ensure the weight is balanced and not disproportionately stressing one arm or shoulder.
- Know Your Limits: Avoid attempting to lift weights or objects beyond your capacity, as overloading can increase the risk of tendon tears.
Strengthening Exercises for Shoulders and Arms
Building strength in the shoulder, arm, and surrounding muscles helps stabilize the joints and reduce strain on the biceps tendons. Incorporate the following exercises into your routine:
- Rotator Cuff Strengthening: Exercises like external rotations with resistance bands can enhance shoulder stability and reduce biceps tendon overcompensation.
- Eccentric Biceps Curls: Slowly lowering the weight during a biceps curl strengthens the tendons and increases their resilience.
- Scapular Stability Exercises: Work on shoulder blade stability with movements like rows or wall slides to optimize shoulder mechanics.
- Progressive Overload: Gradually increase resistance or weight over time to allow the tendons to adapt safely.
Warm-Up and Stretching Before Activities
Preparing the muscles and tendons before physical activity is crucial for injury prevention:
- Dynamic Warm-Up: Engage in activities like arm circles, light jogging, or jumping jacks to increase blood flow and muscle temperature.
- Stretching: Perform gentle stretches targeting the biceps, shoulders, and forearms to improve flexibility and reduce stiffness.
- Gradual Intensity Increase: Ease into intense activities to allow tendons to acclimate to the demands.
Managing Chronic Pain and Tendinitis
Chronic pain or tendinitis in the biceps tendon can predispose it to further injury. Proactive management includes:
- Rest and Recovery: Allow adequate rest between workouts or activities to prevent overuse.
- Ice Therapy: Apply ice to reduce inflammation after repetitive arm movements.
- Anti-Inflammatory Measures: Use over-the-counter medications or topical treatments as directed by a healthcare professional.
- Physical Therapy: Seek guidance for customized exercises to address chronic issues and strengthen weak areas.
Conclusion
In conclusion, biceps tendon rupture is a traumatic injury that can have a significant impact on a person’s daily life. Characteristic symptoms such as severe pain, swelling, hematoma and weakness in the affected arm can make simple activities difficult, affecting the ability to work, engage in physical activities and perform normal daily tasks.
Management of biceps tendon rupture requires a thorough medical evaluation to determine the severity of the injury and develop an appropriate treatment plan. In some cases, a conservative approach including rest, ice, anti-inflammatories, and rehabilitation may be sufficient to promote healing and restore muscle function. However, in more severe cases or in younger, active patients, surgery to repair the tendon may be necessary.
Regardless of the treatment chosen, rehabilitation supervised by a healthcare professional is essential to optimize results and minimize the risk of long-term complications, such as joint stiffness or loss of muscle strength. By carefully following medical recommendations and engaging in an appropriate rehabilitation program, patients can expect a full recovery and regain optimal functionality of the affected arm.
Ultimately, effective management of biceps tendon rupture requires a multidisciplinary approach, combining medical, surgical, and rehabilitation interventions to meet each patient’s individual needs and promote successful recovery.
References
- van der Vis J, Janssen SJ, Haverlag R, van den Bekerom MPJ. Functional outcome in patients who underwent distal biceps tendon repair. Arch Orthop Trauma Surg. 2018 Nov;138(11):1541-1548. [ PubMed ]2.
- Witkowski J, Królikowska A, Czamara A, Reichert P. Retrospective Evaluation of Surgical Anatomical Repair of Distal Biceps Brachii Tendon Rupture Using Suture Anchor Fixation. Med Sci Monit. 2017 Oct 17;23:4961-4972. [ PMC free article ] [ PubMed ]3.
- Castricini R, Familiari F, De Gori M, Riccelli DA, De Benedetto M, Orlando N, Galasso O, Gasparini G. Tenodesis is not superior to tenotomy in the treatment of the long head of biceps tendon lesions. Knee Surg Sports Traumatol Arthrosc. 2018 Jan;26(1):169-175. [ PubMed ]4.
- Vestermark GL, Van Doren BA, Connor PM, Fleischli JE, Piasecki DP, Hamid N. The prevalence of rotator cuff pathology in the setting of acute proximal biceps tendon rupture. J Shoulder Elbow Surg. 2018 Jul;27(7):1258-1262. [ PubMed ]5.
- Kelly MP, Perkinson SG, Ablove RH, Tueting JL. Distal Biceps Tendon Ruptures: An Epidemiological Analysis Using a Large Population Database. Am J Sports Med. 2015 Aug;43(8):2012-7. [ PubMed ]6.
- Thomas JR, Lawton JN. Biceps and Triceps Ruptures in Athletes. Hand Clin. 2017 Feb;33(1):35-46. [ PubMed ]7.
- Quach T, Jazayeri R, Sherman OH, Rosen JE. Distal biceps tendon injuries–current treatment options. Bull NYU Hosp Jt Dis. 2010;68(2):103-11. [ PubMed ]8.
- O’Driscoll SW, Goncalves LB, Dietz P. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007 Nov;35(11):1865-9. [ PubMed ]9.
- Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. [ PubMed ]10.
- Aflatooni JO, Meeks BD, Froehle AW, Bonner KF. Biceps tenotomy versus tenodesis: patient-reported outcomes and satisfaction. J Orthop Surg Res. 2020 Feb 18;15(1):56. [ PMC free article ] [ PubMed ]11.
- Yao C, Weng W, Zhou X, Poonit K, Yang J, Lin D, Sun C, Yan H. Individual Treatment of Delayed Distal Biceps Tendon Rupture: Case Report and Literature Review. Ann Plast Surg. 2019 Mar;82(3):277-283. [ PubMed ]12.
- Ribeiro LM, Almeida Neto JI, Belangero PS, Pochini AC, Andreoli CV, Ejnisman B. Reconstruction of the distal biceps tendon using semitendinosus grafting: Description of the technique. Rev Bras Ortop. 2018 Sep-Oct;53(5):651-655. [ PMC free article ] [ PubMed ]13.
- Lang NW, Bukaty A, Sturz GD, Platzer P, Joestl J. Treatment of primary total distal biceps tendon rupture using cortical button, transosseus fixation and suture anchor: A single center experience. Orthop Traumatol Surg Res. 2018 Oct;104(6):859-863. [ PubMed ]14.
- Cerciello S, Visonà E, Corona K, Ribeiro Filho PR, Carbone S. The Treatment of Distal Biceps Ruptures: An Overview. Seals. 2018 Dec;6(4):228-231. [ PMC free article ] [ PubMed ]15.
- Amin NH, Volpi A, Lynch TS, Patel RM, Cerynik DL, Schickendantz MS, Jones MH. Complications of Distal Biceps Tendon Repair: A Meta-analysis of Single-Incision Versus Double-Incision Surgical Technique. Orthop J Sports Med. 2016 Oct;4(10):2325967116668137. [ PMC free article ] [ PubMed ]16.
- Pereira DS, Kvitne RS, Liang M, Giacobetti FB, Ebramzadeh E. Surgical repair of distal biceps tendon ruptures: a biomechanical comparison of two techniques. Am J Sports Med. 2002 May-Jun;30(3):432-6. [ PubMed ]17.
- Lintner S, Fischer T. Repair of the distal biceps tendon using suture anchors and an anterior approach. Clin Orthop Relat Res. 1996 Jan;(322):116-9. [ PubMed ]18.
- Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. [ PubMed ]19.
- Heinzelmann AD, Savoie FH, Ramsey JR, Field LD, Mazzocca AD. A combined technique for distal biceps repair using a soft tissue button and biotenodesis interference screw. Am J Sports Med. 2009 May;37(5):989-94. [ PubMed ]20.
- Sanchez-Sotelo J, Morrey BF, Adams RA, O’Driscoll SW. Reconstruction of chronic ruptures of the distal biceps tendon with use of an achilles tendon allograft. J Bone Joint Surg Am. 2002 Jun;84(6):999-1005. [ PubMed ]21.
- Hamer MJ, Caputo AE. Operative treatment of chronic distal biceps tendon ruptures. Sports Med Arthrosc Rev. 2008 Sep;16(3):143-7. [ PubMed ]22.
- Tarallo L, Lombardi M, Zambianchi F, Giorgini A, Catani F. Distal biceps tendon rupture: advantages and drawbacks of the anatomical reinsertion with a modified double incision approach. BMC Musculoskelet Disord. 2018 Oct 10;19(1):364. [ PMC free article ] [ PubMed ]23.
- Geaney LE, Mazzocca AD. Biceps brachii tendon ruptures: a review of diagnosis and treatment of proximal and distal biceps tendon ruptures. Phys Sportsmed. 2010 Jun;38(2):117-25. [ PubMed ]24.
- Logan CA, Shahien A, Haber D, Foster Z, Farrington A, Provencher MT. REHABILITATION FOLLOWING DISTAL BICEPS REPAIR. Int J Sports Phys Ther. 2019 Apr;14(2):308-317. [ PMC free article ] [ PubMed ]25.
- Frank RM, Cotter EJ, Strauss EJ, Jazrawi LM, Romeo AA. Management of Biceps Tendon Pathology: From the Glenoid to the Radial Tuberosity. J Am Acad Orthop Surg. 2018 Feb 15;26(4):e77-e89. [ PubMed ]
























{kind=link}