

Cauda equina syndrome is a rare and serious medical condition that results from compression of the nerve roots at the base of the spine, forming what is called the nerve “cauda equina.” This condition is a medical emergency requiring immediate intervention.
When your back sounds the alarm: discovering cauda equina syndrome
There are lower back pains that go beyond simple lumbago. Sometimes, the body sends signals of unexpected severity, as if sounding the alarm to warn of imminent danger. Cauda equina syndrome is one of these absolute medical emergencies where every minute counts. This rare but formidable condition manifests as compression of a bundle of nerve roots located at the lower end of the spinal cord—a region doctors call the cauda equina, literally “horse’s tail,” because of its appearance on imaging.

Beneath this poetic name lies a serious clinical reality. These nerve roots, originating in the lumbar and sacral levels (L2 to S5), innervate the pelvic region, the lower limbs, and the organs responsible for controlling the bladder, bowels, and sexual function. When compressed, the consequences can be dramatic: paralysis, saddle anesthesia, urinary and fecal incontinence, and sexual dysfunction . These symptoms indicate profound damage to the peripheral nervous system and require urgent surgical intervention .
A neurosurgical emergency that should not be missed
Cauda equina syndrome is not simply an extension of a classic herniated disc; it is a neurological catastrophe in the making . In most cases, it results from a large lumbar disc herniation , often located between L4 and S1, which protrudes into the spinal canal and compresses the nerve roots. However, other causes exist: tumors, infections (epidural abscess), severe spinal stenosis, vertebral trauma, or post-surgical complications. Whatever the origin, the common denominator remains the acute compression of these fragile nerves within an anatomically confined space.
This compression triggers a cascade of pathophysiological phenomena: inflammation, ischemia, and axonal degeneration. Within hours, nerve signals are interrupted, muscles become paralyzed, and sphincters disconnect. This is why cauda equina syndrome is an absolute surgical emergency . The later the intervention, the more irreversible the damage. Studies show that decompression should ideally be performed within 24 to 48 hours of the onset of the first signs to maximize the chances of neurological recovery.
A diagnosis that is primarily clinical and radiological
When these signs are present, the diagnosis relies first and foremost on carefully listening to the patient’s account . The clinician must know how to ask the right questions:
- How long has the pain been present?
- Is it associated with urinary or digestive problems?
- Does the patient experience numbness in the pelvic region?
- Can he walk or stand?
Once suspicion is established, the diagnosis is confirmed by medical imaging , particularly lumbar MRI , which allows visualization of the nerve compression and determination of its cause. This examination, performed urgently, guides the surgical decision.
MRI often reveals an extruded herniated disc invading the spinal canal, an epidural abscess , or a tumor . Sometimes, the cause is severe degenerative stenosis in elderly patients. Imaging also allows assessment of the severity of the compression and estimation of the likelihood of recovery based on the duration of symptoms.
Time: a decisive factor in avoiding the irreversible
In cauda equina syndrome, time is the primary enemy . Every hour of compression prolongs nerve damage and reduces the chances of reversibility. After 48 hours, the chances of a full recovery decrease drastically.
Even after successful surgery, lasting effects can persist : muscle weakness, incontinence, and chronic neuropathic pain. This is why early recognition of warning signs is key to prognosis. Osteopaths play a crucial role here: they can be the first to detect the symptoms of a neurological emergency and refer the patient without delay.
Between vigilance and interdisciplinary collaboration
The osteopathic approach to the back is based on trust, touch, and a keen awareness of the body. But when faced with cauda equina syndrome, clinical caution must take precedence over all other considerations. The therapist then becomes a link in a chain of vigilance. They don’t cure: they save time , and sometimes lives.
Recognizing this syndrome means understanding that some back pain goes beyond simple mechanics and falls under the category of medical emergency . In a world where lower back pain is often trivialized, knowing how to identify this exception makes the difference between recovery and lifelong disability.
From early descriptions to modern surgery: the history of cauda equina syndrome
The beginnings: the anatomy of the “cauda equina” (16th–19th centuries)
- André Vésale (1543) first described the tapered termination of the spinal cord and the roots that detach from it.
- Charles Bell (1824) clarified the motor and sensory functions of the spinal roots, paving the way for the understanding of their syndromes.
- At the end of the 19th century, the “cauda equina” became a recognized anatomical term to designate the entire lumbar and sacral nerve roots.
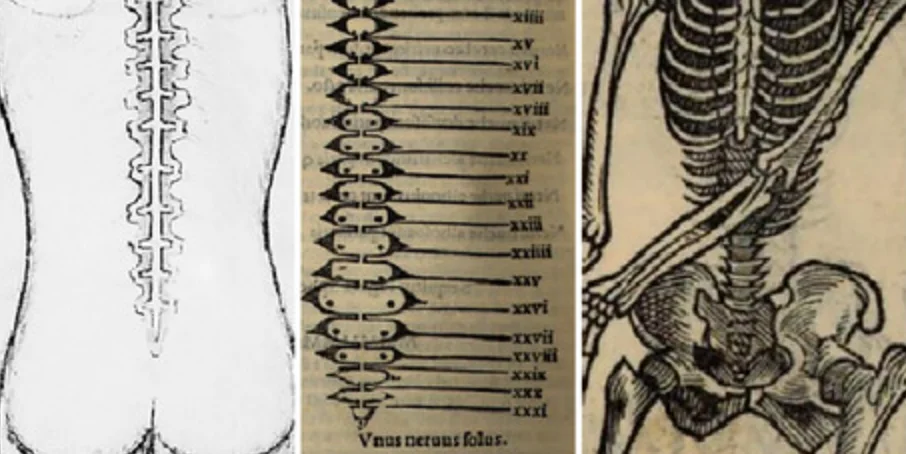
These engravings, inspired by Vesalius and his contemporaries, show the first attempts to represent the spinal cord and its terminal roots, which would later be called cauda equina — the “horse’s tail”.
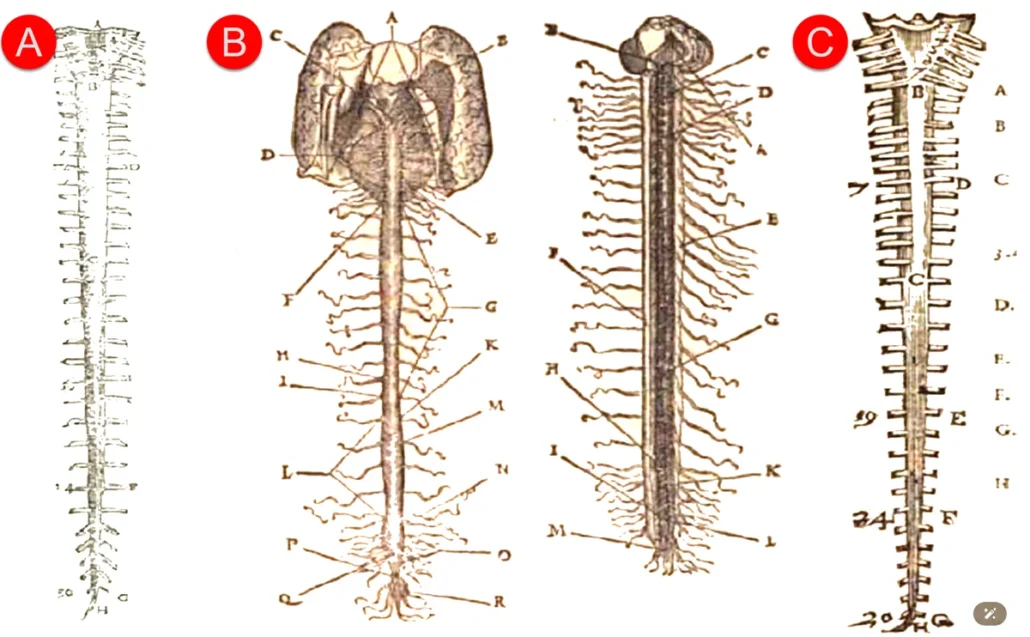
A: Andreas Vesalius. De humani corporis fabrica libri septem. Joannes Oporinus, 1543. BIU Santé, Paris. Public domain.
B: Charles Estienne. La dissection des parties du corps humain, sépare en trois livres. Simon de Colines, 1546. Public domain.
C: Ambroise Paré. Les Œuvres d’Ambroise Paré… sépares en vingt-huit livres avec figures et portraits d’anatomie et d’instruments de chirurgie. Gabriel Buon, 1585. Public domain.
These three engravings, although pioneering, contain inaccuracies: the conus medullaris and the position of the cauda equina are poorly identified. This inaccuracy is explained by the dissection method used at the time, where anatomists accessed the spinal canal through the intervertebral discs rather than via a longitudinal incision.
Estienne’s depiction is considered the most faithful of the three.
The first clinical descriptions (late 19th – early 20th century)
- Horsley (1888) and Gowers (1892) reported the first cases of paralysis of the lower limbs associated with damage to the terminal roots of the spinal cord.
- These observations highlight the distinction between high spinal cord lesions and damage to peripheral roots.
- The term cauda equina syndrome (CES) appeared in British medical literature at the turn of the 20th century.
These two leading figures in British neurology were the first to describe cases of lower limb paralysis associated with damage to the terminal roots of the spinal cord—later known as cauda equina syndrome .
Horsley, a visionary neurosurgeon, dared to operate directly on the spinal cord at a time when such procedures were considered impossible. Gowers, an outstanding neurologist and clinician, translated field observations into precise anatomical knowledge.
Together, they established a link between motor and sphincter symptoms and the topography of the nerve roots, laying the foundations of modern functional neurosurgery .
Their collaboration embodies the convergence of surgical daring and scientific rigor—a historic turning point in the understanding of spinal compression syndromes.
The radiological era: understanding compression (1930–1970)
- The introduction of myelography (Dandy, 1919) , then of scanning (1970s) , finally made it possible to visualize disc and tumor compressions.
- The work of Mixter and Barr (1934) established the direct link between lumbar disc herniation and cauda equina syndrome .
- As a result, the diagnosis became more frequent and better understood, leading to a turning point in spinal neurosurgery.

In 1919, Walter Dandy revolutionized the visualization of the central nervous system by introducing the use of air as a negative contrast agent in radiographic imaging. Thanks to this innovative technique, it became possible for the first time to observe the contours of the brain and spinal canal without resorting to dangerous opaque substances.
This method, called pneumoencephalography , marked the birth of modern myelography , paving the way for neural radiology and functional neurosurgery.
The photograph evokes this era of bold discoveries: Dandy, wearing a lab coat, stands before one of the first medical radiography devices. Air injected into the cerebrospinal fluid made it possible to trace the internal structures of the nervous system — a decisive advance for the diagnosis of tumors, spinal cord compressions, and syndromes such as cauda equina.
The surgical era and the recognized urgency (1970–2000)
- The rise of decompressive laminectomies marks a decisive advance.
- Studies by Shapiro (1993) and Todd (2005) specify that the optimal decompression time is within 24 to 48 hours .
- Cauda equina syndrome is becoming a codified neurosurgical emergency , taught in all medical and manual therapy schools.
The modern era: early diagnosis and interdisciplinarity (2000–2025)
- Lumbar MRI is replacing myelography as the reference tool.
- Research is focused on predictive factors of neurological recovery and interdisciplinary care .
- In osteopathy, clinical vigilance is becoming more refined: the recognition of red flags is now integrated into training.
- Authors such as Shapiro (2021) and Manfredini (2022) update the diagnostic criteria and emphasize the prevention of delays in care.
These stages, from anatomical discovery to modern emergency care, remind us that every advance—scientific or clinical—has been dictated by the need to preserve nerve function. Today, this history illuminates the role of every practitioner: to recognize, guide, and act before nerve failure sets in.
The cascading mechanism: understanding the damage step by step
When lower back pain develops into a neurological emergency, it means an invisible but formidable mechanism is already at work. Cauda equina syndrome illustrates how simple mechanical compression can trigger a cascade of pathophysiological reactions leading to severe, sometimes irreversible, damage. Understanding these successive stages means not only better diagnosis but also better prevention.
The process often begins subtly—a worsening herniated disc, a tightening stenosis, a swelling post-surgical hematoma—then everything accelerates. Within hours, the nerve signals supplying the lower half of the body are constricted. Each compressed fiber becomes a warning pathway to functional chaos.
Step 1 — Nerve compression: the tipping point
It all starts with a mechanical factor . A large herniated disc is the most frequent cause: the gelatinous nucleus of the intervertebral disc escapes through a fissure in the annulus fibrosus and pushes into the spinal canal. This already narrow space cannot tolerate the slightest intrusion.
The lumbar and sacral nerve roots , which are suspended there like electrical wires in an overly constricted conduit, are then compressed. This pressure immediately disrupts the conduction of nerve impulses: the nerves transmit motor and sensory signals poorly or not at all.
This is the tipping point: the patient experiences a sudden, sharp, often bilateral, lower back pain radiating down the legs, sometimes accompanied by a crushing or deep burning sensation. At this stage, the compression may still be reversible—provided action is taken quickly.
Step 2 — Inflammation and radiating pain
Under mechanical stress, the nerve roots become inflamed. Glial cells, guardians of the nervous system, release inflammatory mediators (prostaglandins, cytokines) that amplify the pain and worsen the local edema. This secondary inflammation increases the pressure in the spinal canal, further intensifying the compression: a vicious cycle ensues.
The patient then describes acute, deep, and continuous pain , often accompanied by tingling or numbness in the pelvic region, buttocks, or legs. The sciatica becomes bilateral, sometimes associated with loss of sensation in the so-called “saddle” area—a major sign of the syndrome.
This inflammation is not insignificant: it already signals nerve damage. The motor and sensory fibers, deprived of oxygen, begin to deteriorate.
Step 3 — Nerve ischemia: when the nerves suffocate
Under the combined effect of mechanical compression and edema, intraspinal microcirculation is compromised. The capillaries that nourish the nerve roots can no longer provide a sufficient supply of oxygen and nutrients. This is nerve ischemia .
Nerve cells deprived of oxygen lose their ability to transmit electrical signals. The patient then experiences increasing muscle weakness in the legs, sometimes asymmetrical at first, but quickly becoming bilateral. Walking becomes unsteady, the knees give way, and standing becomes difficult.
Simultaneously, ischemia affects the autonomic nerve fibers responsible for controlling the pelvic organs: the bladder, rectum, and genitals. The first signs appear: urinary retention , loss of fecal control , and sexual dysfunction . At this stage, each additional minute of compression increases the risk of irreversible damage .
Step 4 — Degeneration of nerve fibers
If the compression persists, the nerve fibers suffer structural damage . The myelin sheaths, essential for the rapid conduction of nerve impulses, degrade. This demyelination causes erratic or absent conduction of nerve signals.
The axons themselves, weakened, begin to necrotize. This degenerative process is accompanied by a progressive loss of motor and sensory function: the legs become numb, reflexes disappear, and voluntary control of the sphincters vanishes.
This phase represents the point of no functional return : even decompression surgery performed at this stage will not be able to fully restore lost function. Patients may retain partial paralysis, chronic incontinence, or persistent neuropathic pain.
Step 5 — The absolute emergency: decompress to save your nerves
Cauda equina syndrome is therefore a race against time . As soon as clinical suspicion arises, an urgent lumbar MRI is essential. If compression is confirmed, treatment relies on immediate decompression surgery —often a laminectomy or discectomy —aimed at freeing the trapped nerve roots.
The earlier surgery is performed (ideally within 24 hours), the higher the chances of complete neurological recovery. Beyond this timeframe, damaged nerves may suffer irreversible consequences.
After surgery, functional rehabilitation becomes essential. It aims to restore motor function, improve proprioception, and help the patient regain partial or complete sphincter control. Collaboration between neurosurgeons, physiotherapists, and osteopaths plays a major role in recovery.
A crucial clinical lesson: listen to the waterfall before it sweeps everything away.
For body therapists, understanding this cascade means learning to recognize the critical moment when pain is no longer just musculoskeletal but neurological . This shift from functional to structural pain marks the boundary between osteopathic care and a medical emergency.
Cauda equina syndrome serves as a reminder that the back never lies : it speaks first through tension, then through pain, and finally through the silence of nerves that cease to respond. Intervening before this last stage preserves not only the patient’s mobility but also their dignity.
Unmistakable signs: how the body sounds the alarm
The human body has its own unique warning language. When an imbalance becomes a threat, it doesn’t just whisper: it screams through pain, numbness, and loss of control. In cauda equina syndrome , this bodily alarm reaches its peak. These signals—often mistaken for symptoms of common lower back pain—are actually red flags that every practitioner must recognize immediately. Because here, time is not simply a factor in healing: it determines neurological survival.
The unmistakable lower back pain
It often begins with intense , unusual, sometimes unbearable lower back pain. Unlike typical mechanical pain, this pain is constant, deep, and radiating . It extends to the buttocks, hips, and even both legs. The patient describes it as a burning sensation, an electric shock, an internal pressure that is impossible to relieve.
Often, this pain is accompanied by a marked feeling of tension in the lower back : the back seems “locked,” as if it were refusing any movement. This locking is sometimes mistakenly interpreted as a simple muscle spasm, but it actually reflects a reflexive protection of the nervous system against an internal stressor.
This pain signal is the first manifestation of the conflict between mechanics and neurology . The body seeks to protect the spinal cord and nerve roots—and in this fight, it mobilizes all its defenses. If this pain persists despite rest, stretching, or gentle manipulation, it should immediately raise concern.
Legs giving way: weakness, numbness, bilateral sciatica
The nerve roots in the cauda equina control the muscles and sensation of the lower limbs. When compression occurs, they send erratic signals: burning sensations, tingling, loss of strength, and impaired coordination.
The patient then describes their legs as unresponsive . Walking becomes difficult, getting up from a chair requires excessive effort, and their knees buckle. They may feel as though they are literally “losing their footing.” These neurological signs, often bilateral , differentiate cauda equina syndrome from classic sciatica, which is usually unilateral.
Numbness (or hypoesthesia ) is another key sign. It often begins in the buttocks and travels down the thighs to the calves and feet. Some patients report a loss of sensation in the ground, as if their legs “no longer belong to them.” These symptoms are not simply a postural problem; they indicate active nerve damage .
Anesthesia in the saddle: the major warning sign
If there is one symptom that no therapist should ignore, it is this one: saddle anesthesia .
This term describes the loss of sensation in the perineal region — the area that, when sitting, comes into contact with a horse saddle.
This anesthesia can be partial or total. The patient loses sensation in the buttocks, inner thighs, perineum, or genitals. This sign indicates direct damage to the sacral sensory fibers (S2 to S5) and is a key diagnostic criterion for cauda equina syndrome.
At this stage, the situation is no longer a simple backache: it’s a neurological emergency.
Failing to recognize this anesthesia risks the patient permanently losing pelvic function. A simple question from the practitioner— “Do you feel any numbness between your legs or in your buttocks?” —can make all the difference between prevention and irreversible damage.

Saddle anesthesia occurs due to the compression of the nerve roots in the cauda equina, located at the base of the spinal cord. This nerve compression disrupts sensory signals to these areas, causing numbness, tingling, or a complete loss of sensation. Patients experiencing this symptom may also report difficulties with bladder or bowel control, as these nerves are involved in the autonomic regulation of these functions.
Saddle anesthesia is a medical emergency, as it indicates severe nerve compression, which can lead to permanent damage if not treated promptly. Immediate medical evaluation, typically with MRI, and emergency surgery to decompress the affected nerves are essential to prevent lasting complications such as paralysis or chronic incontinence.
When the body loses control: bladder and bowels in distress
Sphincter dysfunction is the most alarming sign of this condition. It occurs when nerve compression affects the autonomic fibers responsible for controlling the bladder and rectum.
Two scenarios are possible:
- Urinary retention : the patient is unable to urinate, despite a strong urge. The bladder fills, but no flow begins.
- Incontinence : Conversely, some lose all control and urinate without realizing it.
These symptoms are often accompanied by a feeling of pelvic fullness or lower abdominal pain related to bladder distension. At the same time, bowel problems may occur: severe constipation or fecal incontinence.
These symptoms are the direct result of an interruption in the parasympathetic nervous pathways that control these organs. When these signs appear, every minute counts: the patient must be taken to the emergency room immediately .
Sexual disorders: the revealing taboo
Often kept secret out of modesty, sexual disorders nevertheless represent a valuable diagnostic clue. In men, they manifest as difficulty achieving an erection , loss of genital sensation , or even an inability to achieve orgasm. In women, they may include decreased lubrication , vaginal numbness , or a loss of sexual pleasure .
These signs, linked to damage to the sacral nerve roots, may precede or accompany sphincter dysfunction. Their early recognition is crucial: they indicate damage to the erectile and pudendal nerves .
A knowledgeable practitioner, attentive and non-judgmental, will be able to detect this symptom before it becomes irreversible.
Absent reflexes and loss of coordination: the silent signal
Neurologically, tendon reflexes become diminished or even absent, particularly in the patellar and Achilles tendons. The patient may also exhibit a loss of motor coordination , an unsteady gait , or foot drop . These elements, while more subtle, complete the clinical picture of a rapidly progressing syndrome.
They indicate a loss of communication between the peripheral nerves and the spinal cord. At this stage, the body no longer obeys its own commands.
The hierarchy of signals: three levels of urgency
To guide clinical assessment, it is helpful to classify symptoms according to their degree of urgency:
- 🔴 Absolute emergency : saddle anesthesia, incontinence, urinary retention, bilateral weakness.
- 🟠 Relative emergency : bilateral sciatica, progressive numbness, persistent severe lower back pain.
- 🟡 Early warning signs : isolated tingling, leg fatigue, subtle sensory disturbances.
A patient presenting with a single symptom in the red category must be evacuated immediately to a hospital ward .
Listen before it’s too late
These signs are neither trivial nor rare for those who know how to recognize them. Cauda equina syndrome teaches us a fundamental truth: behind certain back pains lies a silent neurological emergency. The osteopath, physiotherapist, or primary care physician is often the first to witness this transformation of lower back pain into a neurogenic crisis.
Knowing how to listen to these signals means preserving more than just mobility: it means preserving dignity and the continuity of bodily life. In this attentive listening to the body, vigilance becomes a form of care in its own right.
What is the source of this emergency? The causes of cauda equina syndrome
Cauda equina syndrome never occurs by chance. Behind this neurosurgical emergency lies a specific structural cause that invades an already very narrow anatomical space: the lumbar spinal canal. Understanding these causes allows for better identification of at-risk patients, refines clinical triage in practice, and avoids dismissing certain symptoms with the reassuring label of “simple back pain.”
Even though the clinical picture is often sudden, its genesis can be slow and silent. A degenerating disc, a narrowing canal, a growing tumor, a developing infection: all these processes can one day cross a critical threshold and trigger a neurological catastrophe.
Large lumbar disc herniation: the most frequent cause
In most cases, cauda equina syndrome is linked to a massive lumbar disc herniation .
Over time, the intervertebral discs crack, dehydrate, and lose their elasticity. Under the effect of exertion, a sudden movement, or sometimes without any obvious trigger, the gelatinous nucleus of the disc can protrude backward and suddenly invade the spinal canal .
When this herniation is central and large , it compresses not just a single nerve root (as in classic sciatica), but an entire bundle of roots : those of the cauda equina. This is what transforms a “simple” radiculopathy into a neurological emergency.
The levels most often affected are between L3 and S1 , where mechanical stresses are significant. In some patients, an episode of chronic lower back pain may precede this for weeks or months, before the situation deteriorates within hours into the dramatic presentation of cauda equina syndrome.
Spinal tumors: a silently growing threat
Tumors of the spine , whether benign (meningiomas, neurinomas) or malignant (metastases, lymphomas), can also cause cauda equina syndrome when they progressively occupy the lumbar canal .
Unlike a herniated disc, the progression is often slower and more insidious . The patient describes atypical lower back pain, sometimes worse at night, with general fatigue, weight loss, or other systemic symptoms. Gradually, radiating pain in the legs, sensory disturbances, and then sphincter dysfunction develop.
In these patients, cauda equina syndrome is often the terminal stage of a neglected or unrecognized compressive process . Hence the importance for clinicians to remain attentive to lumbar pain that is “unusual,” resistant to treatment, and associated with general symptoms.
Epidural infections and abscesses: when inflammation invades the canal
Certain spinal infections can also trigger cauda equina syndrome.
These include:
- epidural abscesses ( purulent collections between the dura mater and the bone),
- spondylodiscitis (infections of the discs and vertebral bodies).
These infections can be of bacterial origin (staphylococcus, tuberculosis, brucellosis, etc.) and sometimes occur in the context of diabetes, immunosuppression, intravenous drug use or after surgery or infiltration.
Inflammation and pus gradually occupy the epidural space, eventually compressing the nerve roots of the cauda equina . The clinical picture then combines intense lumbar pain, possible fever, deterioration of general condition, and rapid onset of neurological signs.
For manual therapists, one element should raise immediate concern: lower back pain accompanied by fever or chills, night sweats, or unexplained fatigue. In this context, any manipulation or mobilization is contraindicated: the priority is urgent imaging .
Severe lumbar stenosis: a canal that closes over time
With age, the lumbar spine undergoes degenerative changes:
- interapophyseal osteoarthritis ,
- hypertrophy of the ligamentum flavum ,
- osteophyte formation ,
- vertebral endplate remodeling .
These changes gradually reduce the diameter of the spinal canal: this is lumbar stenosis .
In most cases, it manifests as neurogenic claudication (pain and heaviness in the legs when walking, relieved by bending or standing still). But when the stenosis is very severe and an intercurrent event occurs—a small herniated disc, a fall, inflammatory edema—the fragile balance is disrupted and the compression becomes acute : cauda equina syndrome can then develop, even in the context of chronic lower back pain.
The danger here is to trivialize this pain in an elderly person, attributing it solely to osteoarthritis, when the canal is already on the verge of saturation.
Trauma and post-surgical complications: when the architecture collapses
Injuries to the lumbar spine (falls from heights, road accidents, crush injuries) can cause:
- fractures,
- dislocations,
- displaced bone fragments,
which invade the spinal canal and directly compress the cauda equina .
In these contexts, the presentation is often sudden, associated with other injuries (polytrauma). But some more “subtle” fractures can go unnoticed and manifest secondarily as a delayed neurological presentation.
Similarly, post-surgical complications (epidural hematoma, significant scar tissue fibrosis, malpositioned osteosynthesis hardware) can lead to secondary nerve root compression. Any appearance of symptoms suggestive of cauda equina syndrome after lumbar surgery should be considered an absolute emergency and not simply postoperative pain.
Field factors and high-risk patients
Certain patient profiles naturally require the therapist to be more vigilant:
- history of severe disc herniation or documented lumbar stenosis ,
- known cancers with a risk of vertebral metastases,
- Immunosuppression , diabetes, drug addiction,
- recent lumbar surgery,
- Recurrent lower back pain with recent sudden worsening.
In these patients, the appearance of new symptoms — perineal numbness, urinary problems, leg weakness — is never a mere detail: it is a major clinical turning point .
Clinical testimony: the decision to go to the emergency room
In someone who suddenly develops cauda equina syndrome (CES), symptoms can worsen rapidly, leaving them with no choice but to seek emergency medical attention. This decision often comes after a harrowing day of intense pain, physical dysfunction, and growing fear about what is happening to their body. Here is a description of how a typical day unfolds, leading up to the crucial decision to go to the emergency room.
Morning: the first signs of a problem
The day begins with an unusual and intense pain in the lower back. For someone who has never experienced such discomfort, this sharp, radiating pain is alarming. As he tries to get out of bed, he notices that the pain isn’t localized: it spreads to the hips and legs, making it difficult to stand or walk. Every movement seems to exacerbate the pain, and what was once a routine morning now feels like an insurmountable challenge.
As they try to go about their usual business, they notice something is wrong. They feel a strange numbness spreading through their buttocks and inner thighs, often described as “saddle numbness.” It’s an odd sensation, and it becomes increasingly difficult to feel the ground beneath their feet. The pain and numbness are bothersome, but it’s still early, and they hope things will improve with some rest.
Midday: Recognizing the seriousness of the symptoms
Around noon, it becomes clear that something serious is happening. The pain in the lower back and legs doesn’t lessen; in fact, it worsens. Even sitting doesn’t seem to bring any relief. The person may try to walk to the kitchen or bathroom, but ends up with weak, wobbly, and unsteady legs. Walking becomes difficult, and sometimes they have to hold onto furniture or walls to stay upright.
Next, bladder symptoms begin. At first, it’s just a slight feeling of not being able to completely empty the bladder. But soon, they find themselves unable to urinate at all, or they may experience the opposite: an uncontrollable urge to urinate, which they can’t stop. The sudden loss of control over bladder function is terrifying because they’ve never experienced anything like it before. They may feel constant pressure, as if they need to go to the toilet, but nothing happens when they try.
At this point, panic begins to set in. Numbness in the legs and groin, sharp back pain, weakness, and now loss of bladder control are not normal symptoms. You realize that something is seriously wrong, and that it’s not something that can be ignored or treated with over-the-counter painkillers.
Afternoon: The decision to seek emergency care
As the afternoon progresses, the situation continues to worsen. The person tries to manage the symptoms on their own, but nothing seems to work. They may try drinking water, lying down, or even taking a hot shower in the hope of easing the pain, but nothing provides relief. The bladder dysfunction worsens, and the person begins to notice that they are also having difficulty controlling their bowels. This loss of control over basic bodily functions is both frightening and humiliating.
The numbness that began in the morning has now spread. The person notices that they can no longer feel certain parts of their lower body, particularly the genitals and inner thighs. Sexual dysfunction may also occur, as sensation in the pelvic region is significantly reduced or even completely absent.
At this point, fear mixes with frustration. The inability to walk without assistance, combined with the alarming loss of bladder and bowel control, clearly indicates that this is not a simple back problem. The symptoms are progressing too rapidly, and the risk of permanent damage weighs heavily on their minds. It is at this moment that they make a crucial decision: it’s time to go to the emergency room.
Evening: Arrival at the Emergency Room
Upon arrival at the emergency room, the person experiences a sense of urgency. The pain is relentless, and the loss of sensation in her lower body is terrifying. At the hospital, she explains the sudden onset of symptoms to the triage nurse: severe lower back pain, numbness, leg weakness, and an inability to control her bladder and bowels. The medical team, recognizing the classic signs of cauda equina syndrome, immediately prioritizes her for evaluation.
An MRI is ordered to assess the extent of nerve compression in the lower spine. The patient is informed that he may need emergency surgery to relieve pressure on the cauda equina nerves. Although this news is upsetting, he feels a slight sense of relief at finally being in the hands of professionals who understand what is happening.
Don’t waste a second: act quickly to avoid the irreversible.
The decision to go to the emergency room can be daunting, but in the case of cauda equina syndrome, it is the most critical decision a person can make. Cauda equina syndrome is a medical emergency, and delayed treatment can lead to permanent damage, including paralysis, chronic pain, and lifelong incontinence. By recognizing symptoms early (severe lower back pain, leg weakness, numbness in the stool, and bladder or bowel dysfunction) and seeking immediate medical help, people with cauda equina syndrome can improve their chances of a full recovery and avoid long-term complications.
Warning to therapists: absolute vigilance required
As a healthcare professional, particularly in osteopathy , physiotherapy, chiropractic, or massage therapy, it is essential to recognize the signs and symptoms of cauda equina syndrome (CES) and understand its severity. CES is a medical emergency that occurs when the bundle of nerves at the base of the spinal cord, called the cauda equina, is compressed. Failure to diagnose or delay treatment of CES can lead to permanent damage, including paralysis, incontinence, and sexual dysfunction.
Therapists are often the first point of contact for patients with lower back pain and other musculoskeletal problems. Recognizing the warning signs associated with cauda equina syndrome and understanding when to refer a patient for immediate medical evaluation is essential to prevent serious and irreversible consequences. Here are the key warnings and guidelines for therapists regarding cauda equina syndrome.
Key symptoms to watch for
CES often presents with symptoms that may initially resemble those of other lower back problems, so it’s essential to be aware of its various warning signs. Be alert to the following symptoms:
- Severe lower back pain : especially when it worsens suddenly or rapidly.
- Bilateral leg weakness or numbness : While sciatica or leg pain is common with lower back problems, CES usually affects both legs and is often accompanied by significant weakness or loss of sensation.
- Saddle anesthesia : loss of sensation in areas that would normally come into contact with the saddle, such as the inner thighs, buttocks, and genital area. This is a characteristic symptom of cauda equina syndrome and should be taken seriously.
- Bladder and bowel dysfunction : patients may experience difficulty urinating, urinary retention, or incontinence. Similarly, loss of bowel control or constipation are warning signs.
- Sexual dysfunction : this can include loss of sensation in the genital area, erectile dysfunction in men, or other forms of sexual deficiency.
Any combination of these symptoms, especially if they appear suddenly, should raise immediate concern about the need for a CES.
When to refer a patient for emergency medical care
If a patient presents with symptoms suggestive of cauda equina syndrome, it is essential to immediately stop any manual or physical therapy intervention and refer the patient for emergency medical care. Cauda equina syndrome requires rapid diagnosis, usually by MRI, and urgent decompression surgery to relieve pressure on the nerves of the cauda equina and prevent permanent damage.
Never attempt to treat the symptoms of cauda equina syndrome in a clinical setting , as this can delay critical medical intervention. Direct referral to the emergency department is warranted, and you should advise the patient not to delay seeking care, even if the symptoms seem manageable at the moment.
High-risk patients
Certain patients may be at higher risk of developing CQS, and therapists should be especially cautious when treating individuals with the following conditions:
- Severe disc herniations : Particularly in the lumbar spine (L4-S1), as large disc herniations can compress the cauda equina.
- Spinal trauma : Patients who have recently experienced a traumatic injury, such as a fall, car accident, or sports injury, may be at risk for SQC due to fractures or dislocations of the vertebrae.
- Patients who have undergone spinal surgery : post-surgical complications, such as hematomas or excessive scar tissue, can lead to SQC.
- Tumors or infections of the spine : Although rare, tumors or infections such as epidural abscesses can compress the cauda equina, resulting in SQC.
If a patient with one of these conditions presents with the warning symptoms of SQC, they should be immediately referred to emergency care.
The dangers of misdiagnosis or delayed treatment
Failing to recognize and respond to the early warning signs of cauda equina syndrome can have devastating and life-altering consequences. If left untreated, cauda equina syndrome can lead to:
- Permanent leg paralysis : Severe compression of the cauda equina can lead to motor dysfunction, resulting in permanent paralysis.
- Chronic bladder and bowel incontinence : damage to the nerves controlling the bladder and bowels can lead to irreversible incontinence, severely affecting the patient’s quality of life.
- Sexual dysfunction : permanent loss of sensation or function in the genital area is a common and irreversible result if CES is not treated promptly.
These consequences can be avoided through early detection and emergency treatment. Therefore, it is essential that therapists prioritize patient safety over manual interventions when a suspected CES (cervical stenosis) is suspected.
What to do if you suspect cauda equina syndrome
- Stop treatment immediately : If you suspect a patient has SQC based on their symptoms, stop all other physical manipulation, stretching, or therapeutic intervention.
- Advise the patient to seek emergency medical attention : instruct the patient to go to the emergency room or contact their doctor immediately. Emphasize the urgency of their condition, as SQC requires prompt medical evaluation and intervention.
- Document the symptoms and your actions : Keep a detailed record of the patient’s symptoms and your response to the situation. This documentation can be essential for healthcare professionals who will assess the patient.
- Follow-up : If possible, follow up with the patient to ensure they have received appropriate medical care and are aware of the seriousness of their condition.
1. Symptoms of a red flag :
- Severe lower back pain .
- Bilateral weakness or numbness of the legs (affecting both legs).
- Saddle anesthesia (loss of sensation in the buttocks, inner thighs or genital area).
- Bladder and bowel dysfunction (urinary retention or incontinence).
- Sexual dysfunction (loss of sensation or erectile dysfunction).
2. Immediate action :
- Stop treatment immediately if symptoms of SQC are suspected.
- Refer the patient to emergency medical care without delay. The SQC requires urgent intervention.
- Inform the patient of the seriousness of their condition and the need for prompt medical evaluation.
3. Causes and risk factors :
- Patients with severe herniated discs, spinal trauma, post-surgical complications, tumors, or infections are at higher risk of SQC.
- Recognize these high-risk patients to remain vigilant.
4. Potential consequences of misdiagnosis or delayed treatment :
- Permanent paralysis.
- Chronic bladder and bowel incontinence.
- Irreversible sexual dysfunction.
Knowing how to distinguish between them leads to better treatment: pathologies not to be confused
- Herniated disc: A herniated disc in the lumbar region may present similar symptoms due to compression of nerve roots, but the severity and extent of the compression may vary.
- Spinal stenosis: Spinal stenosis, a narrowing of the spinal canal, can cause similar symptoms, including lower back pain, leg cramps, and difficulty walking.
- Spinal tumors: Spinal tumors, whether malignant or benign, can compress nerve roots and cause symptoms similar to cauda equina syndrome.
- Spinal infections: Spinal infections, such as epidural abscess, can cause nerve compression and similar symptoms.
- Spinal trauma: Injuries to the spine, such as fractures or dislocations, can lead to compression of nerve roots.
- Peripheral arterial disease: Peripheral arterial disease can cause leg pain when walking, but it is not associated with nerve root compression.
- Spinal restriction syndrome: This is a condition in which the spinal cord is compressed, which can lead to similar symptoms.
- Kidney disease: some kidney disorders can cause lower back pain, although the specific symptoms of cauda equina syndrome are not present.
Lumbar stenosis vs. cauda equina syndrome: two emergencies, one diagnosis to refine
Lower back pain is a common complaint in clinical practice, but not all cases are created equal. Among the serious causes to consider, two conditions stand out due to the severity of their consequences: lumbar spinal stenosis and cauda equina syndrome . Although these two conditions may share some symptoms, they differ significantly in terms of mechanism , urgency of treatment , and prognosis . Being able to distinguish between them quickly can make all the difference in patient management.
Lumbar stenosis: a slow but debilitating progression
Lumbar stenosis is a progressive narrowing of the spinal canal in the lumbar region. This reduction in space available for the spinal cord and nerve roots is usually due to age-related degenerative processes , such as spinal osteoarthritis, hypertrophy of the ligamentum flavum, or osteophytes.
Symptoms develop slowly , often over months or even years, and include chronic lower back pain , neurogenic claudication (fatigue or pain in the legs when walking), tingling, or muscle weakness. Unlike cauda equina syndrome, sphincter dysfunction is rare and late-onset, or even absent.
Treatment for lumbar spinal stenosis is generally progressive , beginning with conservative management: physiotherapy, osteopathic treatment, and anti-inflammatory medication. Decompression surgery may be considered if quality of life is severely impaired.
Cauda equina syndrome: a neurosurgical emergency
In contrast, cauda equina syndrome is an absolute medical emergency . It results from a sudden and severe compression of the nerve roots located in the terminal part of the spinal canal (L2 to S5), forming the bundle known as the “cauda equina.” This compression can be caused by a large herniated disc , a tumor , an infection , trauma , or a post-surgical complication .
Symptoms are often sudden and progressive, developing over hours or days : severe lower back pain, bilateral leg weakness , saddle numbness (in the perineal region), urinary and/or fecal incontinence , and sexual dysfunction . This clinical picture necessitates an urgent MRI , followed by rapid decompression surgery (ideally within 24 to 48 hours) to prevent irreversible damage.
The challenge of differential diagnosis
The difficulty lies in the overlap of certain symptoms : lower back pain, bilateral sciatica, and muscle weakness. However, the rapid onset , the presence of sphincter signs , saddle anesthesia , and the rapid deterioration of the neurological condition lead the clinician to suspect cauda equina syndrome.
A rigorous clinical evaluation, combined with medical imaging (MRI in particular), is essential to quickly distinguish between these two diagnoses. The practitioner must also consider the context : history of trauma, recent surgery, signs of infection or cancer.
Two emergencies, two levels of severity
It is crucial to remember that, although lumbar spinal stenosis may require surgery , it is rarely an immediate emergency. In contrast, cauda equina syndrome requires emergency intervention . A delayed diagnosis can lead to permanent disabilities: paralysis , incontinence , and chronic pain .
The importance of therapeutic vigilance
Healthcare professionals – particularly osteopaths, physiotherapists, and chiropractors – must remain especially vigilant. When faced with a patient presenting with bilateral neurological signs, pelvic numbness, or urinary problems, any manual intervention must be suspended in favor of urgent medical referral.
What imaging reveals: in search of invisible signs
The diagnosis of cauda equina syndrome is usually based on imaging tests such as MRI (magnetic resonance imaging) and CT scans, which allow visualization of the spine and identification of nerve root compression. Specific radiographic signs of cauda equina syndrome may include:
- Major disc herniation: Images may reveal a major disc herniation, where the gelatinous material inside the intervertebral disc is displaced outwards, severely compressing the nerve roots of the cauda equina.
- Nerve root compression: X-rays may show significant compression of the nerve roots at the base of the spine.
- Spinal stenosis: If spinal stenosis is present, radiographic images may indicate narrowing of the spinal canal, contributing to compression of nerve structures.
- Spinal tumors: X-ray images may reveal the presence of tumors along the spine, indicating a possible cause of nerve compression.
- Vertebral displacements or fractures: In cases of trauma or fractures, X-rays may show vertebral displacements or fractures that can compress nerve roots.
It is essential to note that MRI is generally the preferred imaging examination for evaluating cauda equina syndrome, as it allows for more detailed visualization of soft tissues and nerve structures. MRI can accurately show the location, severity, and extent of nerve compression.

In the image on the left, the red circle highlights an area where significant nerve root compression is visible. This compression is likely due to a large herniated disc, a major cause of CES. The disc has bulged into the spinal canal, putting pressure on the nerve bundle known as the cauda equina , which controls lower body motor functions and visceral functions such as bowel and bladder control. The narrowing of the spinal canal is clearly indicated by the compromised space where the nerve roots lie, creating a dangerous situation that requires prompt medical attention.
In the image on the right, the red arrow points to the compressed area of the spine, further illustrating the restricted space within the spinal canal. Such compression can lead to serious neurological symptoms, including leg weakness, saddle numbness, and incontinence.
These MRI scans provide a crucial visual representation of cauda equina syndrome and demonstrate why prompt surgical intervention, usually in the form of decompression surgery, is essential to prevent permanent damage and restore nerve function. Accurate diagnosis and immediate treatment are critical to reducing the risk of long-term disability in patients with this condition. Case study courtesy of Eric F. Greif, Radiopaedia.org . Excerpt from case study rID: 29674
Conclusion
Cauda equina syndrome (CES) is a serious condition requiring immediate medical attention due to its potentially permanent and disabling consequences. The complex pathology of CES, which involves compression of nerve roots at the base of the spine, can lead to severe symptoms affecting both motor and sensory functions, as well as vital autonomic processes such as bladder and bowel control. Prompt intervention, usually in the form of decompression surgery, is essential to prevent long-term nerve damage and maximize the chances of recovery.
Cauda equina syndrome is characterized by the rapid onset of severe symptoms, including intense lower back pain, leg weakness, loss of sensation in the saddle area, and incontinence. These symptoms can worsen rapidly, making early diagnosis with radiographic imaging techniques such as MRI crucial. Cauda equina syndrome must be differentiated from similar conditions such as lumbar spinal stenosis, herniated discs, or spinal tumors, which may present with overlapping symptoms but often have different treatment protocols and prognoses.
Treatment for cauda equina syndrome is not limited to surgery. Postoperative care, including physical therapy and osteopathic interventions, plays a vital role in rehabilitation. These approaches can help restore muscle strength, improve mobility, and address residual pain or dysfunction. Furthermore, osteopathic treatments such as myofascial release and craniosacral therapy can alleviate chronic pain and improve the overall quality of life for patients recovering from cauda equina syndrome.
Living with cauda equina syndrome has a significant impact on daily life. For patients, simple tasks like getting out of bed or walking short distances can become insurmountable challenges. Assistive devices, ergonomic modifications, and ongoing therapy are often necessary to maintain independence and manage the physical limitations of the condition. Furthermore, the psychological burden of cauda equina syndrome, including anxiety, depression, and feelings of helplessness, underscores the need for comprehensive care that addresses both the physical and emotional aspects of the condition. In this context, osteopaths and other healthcare professionals can play a vital role by offering not only physical treatments but also support to improve mental health and quality of life.
Quiz – Cauda Equina Syndrome
Quiz 1
🔹 Part 1 — Multiple Choice
1. What is the most common cause of cauda equina syndrome?
A. Epidural infection
B. Spinal tumor
C. Large lumbar disc herniation
D. Vertebral fracture
E. Congenital malformation
2. From which levels do the nerve roots involved in cauda equina syndrome originate?
A. L1 to S2
B. L2 to S5
C. L3 to S1
D. T12 to L4
E. S1 to S5 only
3. What is the clinical presentation of sacral nerve root involvement (S2 to S5)?
A. Lumbar pain radiating to one limb
B. Saddle anesthesia and sphincter dysfunction
C. Isolated cruralgia
D. Hyperreflexia of the lower limbs
E. Rib pain
4. The optimal time frame for surgical decompression is:
A. 6 hours
B. 12 hours
C. 24 to 48 hours
D. 72 hours
E. 1 week
5. Which statement is correct regarding initial lower back pain?
A. It is always mechanical and intermittent.
B. It disappears with rest.
C. It is bilateral, deep, and often continuous.
D. It only affects the paravertebral muscles.
E. It has no diagnostic value.
6. Which of the following is an absolute red flag ?
A. Bilateral sciatica
B. Plantar numbness
C. Saddle anesthesia
D. Nocturnal lower back pain
E. Increased buttock tenderness
7. Which imaging modality is best to confirm the diagnosis?
A. Plain X-ray
B. Myelography
C. Computed tomography (CT scan)
D. Lumbar MRI
E. Spinal ultrasound
8. In the pathophysiological mechanism, the correct sequence is:
A. Ischemia → inflammation → compression → degeneration
B. Compression → inflammation → ischemia → degeneration
C. Degeneration → inflammation → compression → ischemia
D. Inflammation → compression → degeneration → ischemia
E. Compression → ischemia → inflammation → regeneration
9. Which cause is often gradual rather than sudden?
A. Spinal tumor
B. Central disc herniation
C. Vertebral trauma
D. Epidural hematoma
E. Explosive fracture
10. The role of the manual therapist (osteopath, physiotherapist, chiropractor) in a suspected case is:
A. Attempt gentle manipulation of the pelvis
B. Apply heat to relax the lumbar region
C. Suspend all intervention and immediately refer the patient to the emergency room
D. Prescribe an anti-inflammatory and see the patient again the next day
E. Advise strict rest at home
🔹 Part 2 — True or False
1. Cauda equina syndrome can cause urinary and fecal incontinence.
2. Saddle anesthesia refers to a loss of sensation in the upper limbs.
3. Degenerative lumbar spinal stenosis can sometimes progress to cauda equina syndrome.
4. A normal MRI definitively rules out the diagnosis.
5. The 24- to 48-hour window is critical to avoid permanent neurological sequelae.
6. Spinal infections (abscess, spondylodiscitis) can cause cauda equina syndrome.
7. An osteopath can manipulate the patient if they present with recent bilateral lower back pain without urinary symptoms.
8. Post-surgical rehabilitation can help restore motor function and sphincter control.
9. Cauda equina syndrome primarily affects young children.
10. Delayed diagnosis increases the risk of paralysis and chronic neuropathic pain.
✅ Answers
Multiple choice
- C – Large lumbar disc herniation
- B – L2 to S5
- B – Saddle anesthesia and sphincter disorders
- C – 24 to 48 hours
- C – Bilateral, deep, and continuous pain
- C – Saddle anesthesia
- D – Lumbar MRI
- B – Compression → inflammation → ischemia → degeneration
- A – Spinal tumor
- C – Suspend all intervention and refer the patient
True or False
✅ True
✅ True
❌ False (it concerns the perineal region)
✅ True
❌ False (early false negatives may occur)
✅ True
✅ True
❌ False (red flags must be assessed first)
✅ True
❌ False (mainly adults 30–60 years old)
Quiz 2
🔹 Part 1 — Multiple Choice
1. Which sign most clearly distinguishes cauda equina syndrome from simple bilateral sciatica?
A. Lower back pain
B. Numbness in the legs
C. Saddle anesthesia
D. Lower back stiffness
E. Nocturnal cramps
2. Which area of the spinal canal is directly affected by the syndrome?
A. Mid-cervical
B. Upper thoracic
C. Lower lumbar
D. Posterior sacral
E. Cervicodorsal
3. Which complication is most feared if treatment is delayed?
A. Persistent fever
B. Chronic sciatica
C. Paralysis of the lower limbs and incontinence
D. Isolated muscle pain
E. Spinal stiffness
4. The pathophysiology of the syndrome primarily involves:
A. Reflex muscle involvement
B. Vascular and ischemic compression of nerve roots
C. Sympathetic hyperactivity
D. Systemic infection
E. Lumbar ligament tear
5. What is the approximate proportion of syndromes caused by lumbar disc herniations?
A. 10%
B. 25%
C. 45%
D. 60%
E. 80%
6. Which symptom is not typical of cauda equina syndrome?
A. Loss of urinary control
B. Decreased vaginal lubrication
C. Loss of sensation in the buttocks
D. Frontal headaches
E. Erectile dysfunction
7. What is the best course of action when an osteopath suspects cauda equina syndrome?
A. Gentle lumbar manipulation to relieve pressure
B. Application of a local heat pack
C. Immediately refer the patient to the hospital emergency department
D. Prescribe anti-inflammatory medication
E. Schedule an MRI in 2 weeks
8. What type of radiological lesion is often visible on MRI?
A. Cervical spinal cord displacement
B. Extruded central disc herniation
C. Isolated ligamentum flavum tear
D. Posterior synovial cyst
E. Transverse sacral tear
9. Which patient category is at the highest risk?
A. Growing children
B. Adults aged 30 to 60 with a herniated disc or spinal stenosis
C. Elderly people with no prior medical history
D. Athletic adolescents
E. Pregnant women in their third trimester
10. Functional recovery after surgery depends primarily on:
A. The type of anesthesia used
B. The time between the onset of symptoms and decompression
C. Initial muscle strength
D. The patient’s weight
E. Post-operative sleeping position
🔹 Part 2 — True or False
1. Cauda equina syndrome results from damage to the spinal cord itself.
2. Saddle anesthesia refers to a loss of sensation in the perineal region.
3. MRI can identify the cause and severity of nerve compression.
4. A lateralized herniated disc never causes cauda equina syndrome.
5. The syndrome can be caused by an infection of the spinal canal.
6. Diagnosis is based primarily on the patient’s history and physical examination.
7. Decompression surgery is optional if the symptoms subside.
8. Spinal tumors can cause slow and insidious compression.
9. Severe lumbar stenosis can progress to an acute syndrome.
10. Lower back pain of simple mechanical origin is not accompanied by sphincter dysfunction.
✅ Answers
Multiple choice
- C – Saddle anesthesia
- C – Lower lumbar
- C – Paralysis + incontinence
- B – Vascular and ischemic compression
- C – 45 %
- D – Frontal headaches
- C – Refer the patient immediately
- B – Extruded central disc herniation
- B – Adults aged 30–60 years with herniated disc / stenosis
- B – Time between symptoms and decompression
True or False
✅ True
❌ False – It affects the nerve roots, not the spinal cord.
✅ True
✅ True
❌ False – A large median or lateral hernia can cause it.
✅ True
✅ True
❌ False – It is urgent and mandatory.
✅ True
✅ True
Quiz 3
🔹 Part 1 — Multiple Choice
1. Cauda equina syndrome should be suspected first in the presence of:
A. Lower back pain that increases with extension
B. Bilateral sciatica with perineal anesthesia
C. Isolated mechanical lower back pain
D. Pain referred to the chest
E. Unilateral psoas muscle contracture
2. In osteopathy, the standard response to suspected neurological compression is to:
A. Apply a lumbar HVLA technique
B. Reassess the patient after 48 hours
C. Refer immediately to an emergency medical service
D. Perform a muscle-relaxing massage
E. Prescribe breathing exercises
3. What is the essential difference between severe lumbar spinal stenosis and cauda equina syndrome?
A. The vertebral level affected
B. The speed of onset of symptoms
C. The type of pain experienced
D. The presence of a herniated disc
E. The laterality of the involvement
4. Which anatomical structure is directly compressed in the syndrome?
A. The lumbar vertebral bodies
B. The thoracic spinal cord
C. The lumbar and sacral nerve roots (L2–S5)
D. The paravertebral muscles
E. The ligamentum flavum
5. Which of the following symptoms requires immediate discontinuation of osteopathic treatment ?
A. Mechanical lower back pain with fatigue
B. Bilateral buttock numbness
C. Morning stiffness
D. Unilateral pain with movement
E. Sensation of pulling in the lower back
6. Acute urinary retention associated with bilateral sciatica suggests:
A. Simple sciatic nerve irritation
B. Common lower back pain
C. Cauda equina syndrome
D. Facet joint osteoarthritis
E. Myofascial syndrome
7. During clinical examination, loss of sensation in the saddle position indicates:
A. Femoral nerve involvement
B. S2–S5 nerve root involvement
C. Obturator nerve involvement
D. Brachial plexus involvement
E. Sciatic nerve involvement
8. If the practitioner delays referring the patient, the possible consequences are:
A. Transient muscle pain
B. Persistent paralysis, incontinence, and sexual dysfunction
C. Moderate lumbar stiffness
D. Referred neck pain
E. Chronic fatigue
9. In a preventative role, the osteopath must primarily:
A. Decompress the nerve through manipulation
B. Monitor the evolution of the patellar reflex
C. Identify red flags and refer the patient early
D. Massage the pelvic region to stimulate circulation
E. Recommend the routine use of a lumbar support belt
10. In case of diagnostic uncertainty, the absolute priority is:
A. Perform gentle stretches
B. Test sacral mobility
C. Inform the patient and refer them for an urgent MRI
D. Reschedule the session in 3 days
E. Perform a forced straight leg raise test
🔹 Part 2 — True or False
1. Cauda equina syndrome can be confused with simple chronic lower back pain.
2. The rapid onset of urinary or bowel problems is an absolute red flag.
3. Lumbar spinal stenosis usually develops over several years.
4. Bilateral pain with perineal numbness is never an emergency.
5. A normal MRI completely rules out the diagnosis.
6. The manual therapist’s role is primarily to recognize warning signs.
7. Prolonged compression can lead to irreversible nerve fiber degeneration.
8. After surgery, osteopathy can contribute to functional recovery.
9. Saddle anesthesia is often the last sign to appear.
10. Referral to the emergency department is necessary even if symptoms are intermittent.
✅ Answers
Multiple choice
- B – Bilateral sciatica + perineal anesthesia
- C – Immediate referral to the emergency room
- B – Speed of installation
- C – Nerve roots L2–S5
- B – Bilateral buttock numbness
- C – Cauda equina syndrome
- B – Sacred Roots S2–S5
- B – Paralysis, incontinence, sexual disorders
- C – Identify the red flags and orient
- C – Inform the patient and request an urgent MRI
True or False
✅ True
✅ True
✅ True
✅ True
❌ Faux
❌ False (some compressions are intermittent or partial)
✅ True
✅ True
✅ True
❌ False (often early, even inaugural)
References
1. Introduction / Anatomy / Emergency
Sections :
- When your back sounds the alarm…
- Description of the cauda equina, roots L2–S5
- A neurosurgical emergency that should not be missed
References to be inserted here:
- Shapiro, S. (2021). Cauda Equina Syndrome: A Review. Neurosurgery Clinics of North America, 32(3), 383–391.
- Todd, NV (2020). Research on cauda equina syndrome (reviews and management standards).
2. Clinical diagnosis, MRI and the time factor
Sections :
- A diagnosis that is primarily clinical and radiological
- Time: a decisive factor in avoiding the irreversible
- Between vigilance and interdisciplinary collaboration
References:
- Shapiro, S. (2021). Cauda Equina Syndrome: A Review
- Todd, N.V. (2020).
- Manfredini, L., Sassi, M., Mastri, G. et al. (2022). Delayed cauda equina syndrome from spinal trauma: A diagnostic challenge. Spine Surgery and Related Research. (to illustrate the impact of the delay in prise en charge)
3. Pathophysiology / “cascade mechanism”
Sections :
- The cascading mechanism: understanding the damage step by step
- Infographic caption: The cascade mechanism of cauda equina syndrome
References:
- Shapiro, S. (2021). (pathophysiology, ischemia, degeneration, prognosis)
- Todd, NV (2020). (Evolution, clinical and pathophysiological phases)
4. Clinical signs, red flags, hierarchy of signals
Sections :
- Unmistakable signs: how the body sounds the alarm
- Lower back pain, bilateral sciatica, saddle anesthesia
- Sphincter and sexual dysfunction, absent reflexes
- The hierarchy of signals: three levels of urgency
References:
- Shapiro, S. (2021). (Cardinal signs: pain, saddle anesthesia, retention/incontinence, bilateral weakness)
- Todd, NV (2020). (Clarification on the “red flags” of CES)
5. Causes and risk factors
Sections :
- What is the source of this emergency? The causes of cauda equina syndrome
- Distribution of causes (herniated disc, tumors, trauma, infections, stenosis, post-op, etc.)
- Subsections: herniated disc, tumors, infections, stenosis, trauma, post-surgical complications, predisposing factors
References:
- Shapiro, S. (2021). (Epidemiology and major causes of CES)
- Manfredini, L. et al. (2022). (post-traumatic forms, diagnostic delay)
- Zouaoui, K., Loukil, S., Abbes, M., Rahmouni, S. et al. (2024). Profile of disc-vertebral infections over the last four years: a study of 50 cases. Revue du Rhumatisme. (section infections / spondylodiscitis)
- Saad, A., Fakhfakh, R., Khalifa, D., El Amri, N. et al. (2024). Comparative study of brucellar and tuberculous spondylodiscitis. Revue du Rhumatisme. (specific tuberculous/brucellar infections)
6. Prolonged clinical picture / patient narrative
Section :
- Clinical testimony: the decision to go to the emergency room
It’s primarily an educational story, but you can link it to:
- Shapiro, S. (2021). (Description of the typical clinical presentation and progressive symptoms)
- Manfredini, L. et al. (2022). (Illustration of delayed and misleading presentations after trauma)
7. Warning to therapists / guidelines
Sections :
- Warning to therapists: absolute vigilance required
- Lists: “1. Red flag symptoms”, “2. Immediate action”, “3. Causes and risk factors”, “4. Potential consequences…”
References:
- Shapiro, S. (2021). (Standards of care and emergency decompression)
- Todd, NV (2020). (Time, prognosis, standards of care for CES)
8. Differential diagnosis (hernia, stenosis, tumors, etc.)
Sections :
- Knowing how to distinguish in order to treat better: pathologies not to be confused
- Lumbar stenosis vs. cauda equina syndrome: two emergencies, one diagnosis to refine
References:
- Shapiro, S. (2021). (Differential diagnosis of CES)
- Manfredini, L. et al. (2022). (differential with other post-traumatic/radicular lesions)
9. Imaging (MRI, CT scan, image examples)
Section :
- What imaging reveals: in search of invisible signs
- Comments on MRI scans and explanation of the illustrated case (Radiopaedia)
References:
- Shapiro, S. (2021). (MRI as the examination of choice and radiological criteria)
- Case study Radiopaedia.org, Eric F. Greif, rID 29674.
10. Conclusion / Life with CES / Rehabilitation
Section :
- Conclusion (severity, possible sequelae, rehabilitation, role of physio/osteopathy, impact on daily life)
References:
Goetz-Fu, M. (2023). The short history of an old problem – History of the management of myelomeningocele. (This should be used primarily to provide historical context on neuro-orthopedic/spinal cord management, if you include a historical reference.)
Shapiro, S. (2021). (prognosis, sequelae, rehabilitation)
Manfredini, L.


















{kind=link}