



Introduction
Radiculopathy, also known as “pinched nerve,” is a painful condition that occurs when one of the spinal nerve roots is compressed or irritated where it emerges from the spinal canal. This compression can lead to a range of symptoms, including pain, numbness, tingling and muscle weakness in the corresponding region of the body.
The main cause of radiculopathy is compression of the nerve roots due to various factors. Common causes include herniated discs, bone spurs, spinal stenoses, inflammation from conditions such as arthritis, and spinal trauma. These factors contribute to pressure on the nerve root, causing disruption in the transmission of nerve signals and generating painful symptoms.

Irritated spinal cord: Irritation or inflammation of the spinal cord may occur due to compression by surrounding structures, leading to symptoms such as pain, tingling, or weakness.
Pinched nerve: Nerve compression caused by a herniated disc or osteophytes can result in radiating pain, numbness, or decreased muscle strength in the areas served by the nerve.
Unhealthy disc: Degenerated intervertebral discs lose their ability to absorb shocks, increasing the risk of herniation and nerve compression.
Herniated disc: A protrusion of the nucleus of the intervertebral disc can directly compress spinal nerves, causing local or radiating pain.
Osteophytes: These bony outgrowths, often due to osteoarthritis or aging, reduce the space around spinal nerves, exacerbating compression symptoms.
Radiculopathy can occur at any level of the spine, but when it occurs in the neck, it is referred to as cervical radiculopathy. Cervical nerve roots, originating from the spinal cord in the neck region, are susceptible to compression from conditions such as herniated discs or cervical spondylosis.
Symptoms of cervical radiculopathy can vary depending on the nerve root affected and the severity of the compression. Patients may experience radiating pain down the arm, numbness or tingling in the fingers, and muscle weakness in the neck or shoulder area. Neck movement may also be limited due to pain and stiffness.
Diagnosing cervical radiculopathy usually involves a thorough evaluation of the patient’s medical history, a physical examination, and imaging tests such as X-rays, MRIs, or CT scans. These tests help locate the source of the compression and determine the extent of the damage.
Treatment for cervical radiculopathy aims to relieve pressure on the nerve root, reduce inflammation, and alleviate symptoms. Treatment approaches may include taking anti-inflammatory medications, osteopathy to strengthen neck muscles and improve mobility, and corticosteroid injections to reduce local inflammation.
In more severe cases or when conservative treatments are not effective, surgery may be considered to release pressure on the nerve root. However, surgery is usually only considered after other treatment options have been exhausted and when symptoms persist or worsen.
So, cervical radiculopathy is a painful condition resulting from compression of a nerve root in the neck region. Management of this condition requires an individualized approach, often combining medications, physical therapy, and in some cases, surgical procedures. Early diagnosis and a proper treatment plan are essential to minimize symptoms and improve the quality of life of those affected by this condition.
Example of spinal cord compression (red letter)
The C6 and C7 nerve roots are most commonly affected. Patients younger than 55 years are more likely to experience radiculopathy resulting from acute disc herniation, while those older than 55 years are more likely to experience symptoms resulting from degenerative foramen stenosis.
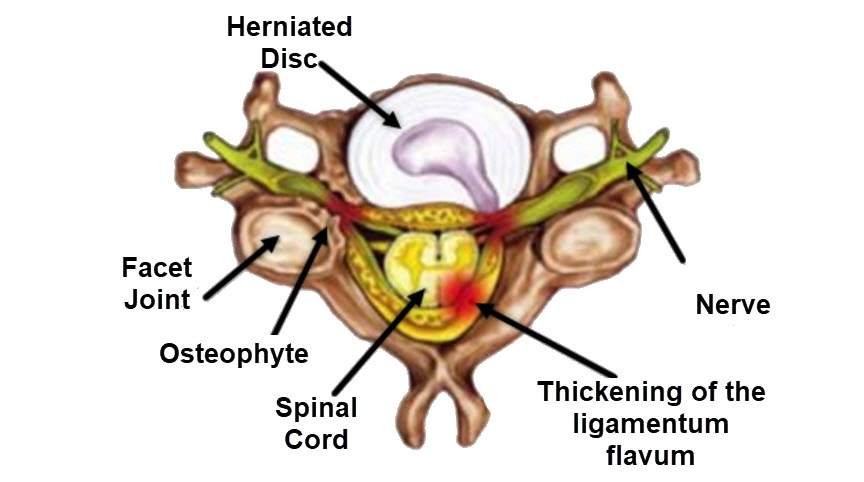
Herniated Disc (Hernie discale): A protrusion of disc material that can compress nearby spinal nerves, often resulting in pain, tingling, or numbness radiating into the arms.
Facet Joint (Articulation facettaire): Degeneration or dysfunction in these stabilizing joints may contribute to nerve irritation and spinal stiffness.
Osteophyte: Bone spurs that develop as a result of degenerative changes in the spine can narrow the spaces where nerves exit the spinal column, exacerbating nerve compression.
Spinal Cord (Moelle épinière): Central to transmitting signals between the brain and the body, it remains protected within the spinal canal but can be indirectly affected by structural changes.
Nerve (Nerf): Compression or irritation of the spinal nerve roots can lead to the characteristic symptoms of cervical radiculopathy, including pain, weakness, or sensory disturbances.
Thickening of the Ligamentum Flavum (Épaississement du ligament jaune): Hypertrophy of this ligament contributes to spinal canal narrowing (stenosis), which can aggravate nerve compression.
WARNING: The information on this blog is for educational purposes only and not a substitute for professional medical advice. Do not attempt any maneuvers, exercises, or treatments described here without consulting a qualified healthcare professional. Improper application may lead to injury or complications. Always seek professional guidance for your specific health needs.
Causes of cervical radiculopathy
The causes of cervical radiculopathy can vary, and their significance may depend on several factors. Here are some of the common causes of cervical radiculopathy, presented in descending order of frequency:
- Cervical disc herniation: A herniated disc in the cervical region, where the intervertebral disc puts pressure on the nerve roots, is a common cause of cervical radiculopathy.
- Cervical osteoarthritis (spondylosis): Osteoarthritis, or wear and tear of the joints, can cause the formation of small bony growths (osteophytes) that compress nerve roots.
- Bone spur (osteophyte): Abnormal bone growth can put pressure on nerve roots, causing radiculopathy.
- Cervical Stenosis: Stenosis, a narrowing of the spinal canal in the cervical spine, can compress nerve roots and cause symptoms of radiculopathy.
- Traumatic cervical injuries: Injuries, such as sprains, dislocations, or fractures of the cervical spine, can result in compression of the nerve roots.
- Tumors: Tumors of the cervical spine can compress nerve roots and cause radiculopathy, although this is less common.
- Infections: Infections of the spine or intervertebral discs can lead to inflammation and compression of nerve roots.
- Birth defects: Some people may have birth defects of the cervical spine that increase the risk of radiculopathy.
It is important to note that several of these factors may coexist in an individual, and the severity of radiculopathy may vary depending on the underlying cause.
Symptoms of cervical radiculopathy
Symptoms of cervical radiculopathy may vary depending on the severity of the compression or irritation of the nerve roots in the cervical region of the spine. Here is a list of symptoms commonly associated with cervical radiculopathy, presented in decreasing order of frequency:
- Radicular pain: Pain is often the most predominant symptom. It can radiate from the neck to the arm, shoulder, or even the fingers. The pain usually follows the path of a specific nerve root.
- Tingling or numbness: Sensations of tingling, numbness, or tingling may be felt in the neck, shoulder, arm, or fingers. These sensations are often linked to nerve compression.
- Muscle weakness: Compression of nerve roots can lead to muscle weakness in the arm or hand corresponding to the affected root.
- Decreased sensitivity: Decreased sensitivity, sometimes described as loss of sensation, may occur in the area innervated by the compressed nerve root.
- Neck Pain: Pain can also be felt in the neck area itself, especially near the spine.
- Decreased reflexes: Compression of nerve roots can cause decreased reflexes in the affected area.
- Difficulty performing certain activities: Symptoms may be exacerbated during certain activities, such as raising your arm or turning your head.
- Neck Stiffness: Stiffness in the neck may be experienced, particularly if radiculopathy is associated with other cervical spine problems, such as osteoarthritis.
It is important to note that symptoms can vary from person to person, and not all symptoms are present in every individual with cervical radiculopathy.
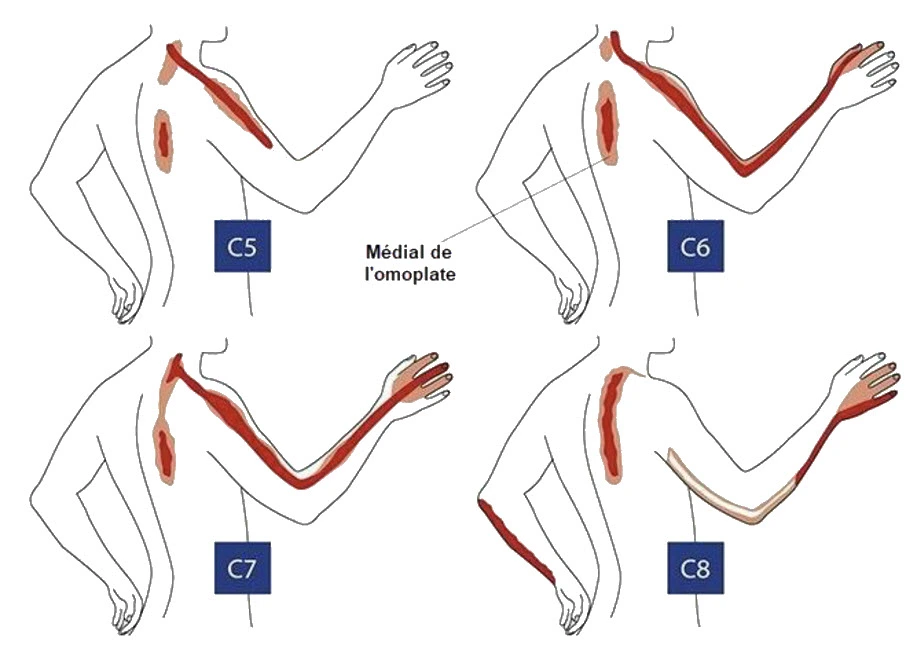
C5 Dermatome: The sensory region includes the lateral shoulder and upper arm, often linked to the deltoid area. This corresponds to sensations mediated by the C5 nerve root.
C6 Dermatome: Extends from the lateral forearm to the thumb and index finger. Pain or numbness in this area may indicate C6 nerve root compression or dysfunction.
C7 Dermatome: Covers the middle finger and extends up the posterior forearm. Symptoms here often suggest issues with the C7 nerve root, commonly associated with cervical radiculopathy.
C8 Dermatome: Encompasses the medial forearm and the ring and little fingers. Dysfunction in the C8 nerve root can manifest as sensory changes or weakness in this region.
The highlighted regions aid in diagnosing nerve compression or irritation, often guiding healthcare professionals in identifying cervical spine disorders. Understanding these patterns is crucial for tailored therapeutic interventions.
Diagnosis of Cervical Radiculopathy
Diagnosing cervical radiculopathy is a critical step in managing this condition effectively. Accurate diagnosis relies on a combination of a thorough medical history, physical examination, and imaging techniques such as X-rays, MRI, and CT scans. Each component provides valuable insights into identifying the root cause of symptoms and formulating an appropriate treatment plan.
Medical History and Physical Examination
The diagnostic process begins with a detailed evaluation of the patient’s medical history. This involves understanding the onset, duration, and progression of symptoms such as pain, numbness, tingling, and muscle weakness. Patients are often asked about activities or movements that exacerbate or relieve their symptoms, as well as any prior injuries, surgeries, or pre-existing spinal conditions.
During the physical examination, healthcare providers assess the following:
- Neurological Symptoms
The provider evaluates areas of pain, numbness, and tingling. These symptoms are often mapped to specific dermatomes—areas of skin innervated by individual nerve roots. For instance:- C5 radiculopathy affects the shoulder and upper arm.
- C6 radiculopathy involves the thumb and index finger.
- C7 radiculopathy impacts the middle finger and posterior forearm.
- C8 radiculopathy affects the medial forearm and ring/little fingers.
- Muscle Strength
The examination includes testing the strength of muscles corresponding to affected nerve roots. Weakness in specific muscle groups, such as the deltoid (C5) or triceps (C7), can help localize the nerve compression. - Reflex Testing
Reflexes, such as the biceps (C5-C6) and triceps (C7), are checked for abnormalities. A diminished or absent reflex indicates potential nerve root dysfunction. - Range of Motion and Provocative Tests
- The provider assesses neck mobility and observes if certain movements reproduce or alleviate symptoms.
- Special tests, such as the Spurling Test, involve tilting the head toward the symptomatic side while applying gentle pressure to the top of the head. Pain radiating to the arm during this test suggests nerve root compression.
- Postural and Functional Analysis
Observation of the patient’s posture and head positioning may reveal compensatory changes, such as the “hand-on-head” posture often adopted by those with C7 radiculopathy.
Imaging Techniques
When the clinical evaluation suggests cervical radiculopathy, imaging studies are used to confirm the diagnosis, identify the underlying cause, and evaluate the extent of structural damage.
1. X-rays
X-rays provide a first-line imaging modality to assess the cervical spine. While they do not show soft tissues such as nerves or discs, they are valuable for identifying:
- Bone Spurs (Osteophytes): Abnormal growths that may compress nerve roots.
- Spinal Alignment: Changes such as scoliosis or vertebral instability.
- Degenerative Changes: Narrowing of intervertebral disc spaces indicative of spondylosis or osteoarthritis.
Lateral and oblique views are particularly useful for assessing foraminal narrowing and vertebral alignment.
2. Magnetic Resonance Imaging (MRI)
MRI is the gold standard for diagnosing cervical radiculopathy because it provides detailed visualization of soft tissues, including nerves, discs, and ligaments. MRI can reveal:
- Herniated Discs: Protrusion or extrusion of disc material compressing nerve roots.
- Spinal Stenosis: Narrowing of the spinal canal and foramina.
- Inflammatory Changes: Swelling around compressed nerve roots.
- Ligament Thickening: Hypertrophy of the ligamentum flavum, contributing to stenosis.
Additionally, MRI is non-invasive and does not expose patients to radiation, making it a preferred option for evaluating complex cases.
3. Computed Tomography (CT) Scans
CT scans offer excellent detail of bony structures and are particularly useful when MRI is contraindicated (e.g., for patients with pacemakers). CT myelography, a specialized form of CT, involves injecting contrast dye into the spinal canal to highlight nerve root compression. It is often used to detect:
- Foraminal Stenosis: Narrowing of the passageways through which nerves exit the spine.
- Bone Abnormalities: Fractures, bone spurs, or vertebral deformities.
Instinctive Postures in C7 Radiculopathy: Understanding the Hand-on-Head Gesture
Patients suffering from C7 radiculopathy often adopt a distinctive posture to alleviate their symptoms. This frequently involves placing the hand of the affected limb on the head in an attempt to ease the pain. This specific gesture, placing the hand on the head, is a natural response to the discomfort and pain associated with C7 radiculopathy.
C7 radiculopathy refers to the compression or irritation of the C7 nerve root, located in the cervical (neck) region of the spine. This nerve root is part of the brachial plexus, a network of nerves that extends from the neck to the arm. When this nerve root is affected, it can cause radiating pain, weakness, or numbness along the nerve’s pathway, often reaching the arm and hand.
Placing the hand on the head is a postural strategy that patients instinctively adopt to reduce pressure on the affected nerve and relieve discomfort. By doing so, individuals may unintentionally ease tension on the nerve roots and experience temporary relief from their symptoms. This gesture reflects the body’s natural tendency to find a position that minimizes stress on the affected nerves.
However, it is important to note that while this posture may provide momentary relief, it does not address the underlying cause of C7 radiculopathy. Consulting a healthcare professional for a proper evaluation and diagnosis is crucial. Understanding the root cause of the condition is key to determining an appropriate treatment plan. Therapeutic options may include physical therapy, medication, and, in some cases, surgical intervention, depending on the severity and nature of the condition.

Differential diagnostics
- Thoracic outlet syndrome: This condition results from compression of blood vessels or nerves in the thoracic outlet area, leading to symptoms such as pain and numbness in the arm.
- Cervical Osteoarthritis: Osteoarthritis of the cervical joints can cause neck pain and radiation into the arms, which can be confused with the symptoms of cervical radiculopathy.
- Cauda Equina Syndrome: Although more common in the lumbar region, cauda equina syndrome can cause compression of nerve roots in the cervical region, resulting in symptoms similar to radiculopathy.
- Cervical meningitis: Inflammation of the membranes surrounding the spinal cord can cause symptoms similar to cervical radiculopathy, such as headaches, neck stiffness, and radiating pain.
- Cervical tumors: Tumors of the spine or surrounding tissues can compress cervical nerve roots, causing symptoms similar to radiculopathy.
- Herniated cervical disc: A herniated disc can put pressure on the cervical nerve roots, causing pain and numbness in the arms.
Pathophysiology
The main pathophysiological mechanisms of cervical radiculopathy include:
- Nerve Root Compression: The root cause of cervical radiculopathy is nerve root compression. This compression can result from a variety of conditions, including herniated discs, bone spurs, spinal stenoses, arthritis-related inflammation, or spinal trauma. Compression causes disruption in the transmission of nerve signals.
- Herniated disc: When an intervertebral disc, which acts as a cushion between the vertebrae, herniates or moves from its normal position, it can put pressure on the cervical nerve roots. This can cause inflammation and irritation of the nerves.
- Bone spurs (osteophytes): Abnormal growth of bone, in the form of bone spurs, can occur as a result of normal wear and tear of joints (osteoarthritis). These bone spurs can compress nerve roots and contribute to the symptoms of radiculopathy.
- Spinal Stenosis: A reduction in the space in the spinal canal, called spinal stenosis, can lead to compression of the cervical nerve roots. This condition can result from osteoarthritis, thickening of ligaments or abnormal bone growth.
- Inflammation: Inflammatory conditions, such as arthritis, can lead to inflammation of the structures around nerve roots. Inflammation contributes to compression and irritation of the nerves.
- Spinal Trauma: Injuries, such as car accidents or falls, can cause damage to spinal structures, leading to compression of nerve roots.
Acute disc herniation (spondylosis)
Cervical spondylosis begins with drying out of the disc. The avascular disc loses water due to a decrease in proteoglycan content in the nucleus pulposus, which leads to a decrease in water content from 90% at birth to 74% during the eighth decade of life. This change leads to loss of disc height, microinstability and consequent osteophyte formation, facet hypertrophy, and buckling and hypertrophy of the ligamentum flavum. Spinal degeneration, or spondylosis, can lead to neuroforaminal stenosis and potentially spinal canal stenosis.
Therapeutic recommendations
It is important to note that the effectiveness of osteopathy can vary from person to person, and its use often depends on the underlying cause of the radiculopathy and the individual response to treatment. Here are recommendations, including osteopathy, for cervical radiculopathy:
- Pain management:
- Use nonsteroidal anti-inflammatory drugs (NSAIDs) or other pain relievers as recommended by your healthcare professional.
- Osteopathy:
- Consult a qualified osteopath for specific manual manipulations aimed at restoring neck mobility, relieving pressure on nerve roots and improving overall function.
- Lifestyle changes:
- Practice good posture at work and at home.
- Avoid positions and activities that make symptoms worse.
- Cervical orthoses:
- In some cases, wearing a cervical collar may be recommended to limit neck movement and allow nerve roots to heal.
Osteopathic Approaches to Cervical Radiculopathy
Cervical osteopathy involves the use of manual techniques to address dysfunctions in the cervical spine (neck region) that may cause pain, stiffness, or other systemic issues. These techniques are performed by trained osteopaths, focusing on restoring mobility, reducing pain, and improving overall function.
Key Techniques in Cervical Osteopathy
- Soft Tissue Manipulation
This technique involves the application of gentle pressure and stretching to the muscles and soft tissues surrounding the cervical spine. It aims to reduce muscle tension, improve circulation, and prepare the area for further manipulation.- Procedure: The osteopath uses their hands to knead, stretch, or compress the soft tissues around the neck and shoulders.
- Benefits: Enhances local blood flow, reduces muscular tightness, and alleviates discomfort.
- Articulatory Techniques
Articulatory techniques involve moving the neck joints through their natural range of motion to improve mobility and reduce stiffness. This is a low-velocity, rhythmic approach that is particularly useful for patients with restricted movement.- Procedure: The osteopath gently mobilizes the cervical joints by moving the neck in specific directions within a comfortable range.
- Benefits: Increases joint range of motion, decreases pain, and promotes functional recovery.
- High-Velocity, Low-Amplitude (HVLA) Thrusts
HVLA thrusts are precise, controlled movements used to address joint restrictions. These are commonly referred to as “neck adjustments” and are performed with extreme care.- Procedure: The osteopath identifies the specific joint causing dysfunction and applies a quick, gentle thrust to release the restriction.
- Benefits: Restores joint alignment, reduces pain, and improves nerve function.
- Cranial Osteopathy
Cranial techniques focus on the subtle movements of the cranial and cervical bones. These are particularly helpful for patients with stress-induced neck pain or tension-related headaches.- Procedure: Gentle hand placements and minute manipulations are performed to release tension in the cranial and upper cervical structures.
- Benefits: Alleviates tension headaches, reduces stress, and promotes relaxation.
Top Scientific Studies on Osteopathic Treatments for Cervical Radiculopathy
1. “The Effects of Osteopathic Treatment on Non-Specific Chronic Neck Pain and Disability” (2013)
Summary: Explores how osteopathy reduces perceived disability and pain in patients with chronic neck pain, highlighting its relevance for cervical radiculopathy.
Read Study (PDF)
2. “Balance Chiropractic Therapy for Cervical Spondylotic Radiculopathy: A Randomized Controlled Trial” (2024)
Summary: This trial evaluates balance chiropractic and osteopathic therapies for cervical radiculopathy, reporting improved pain and functionality.
Read Study
3. “Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review” (2021)
Summary: Reviews various manual therapies, including osteopathy, in managing radiculopathy and their effectiveness in reducing pain and improving mobility.
Read Study (PDF
4. “Cervical Traction Combined with Neural Mobilization for Patients with Cervical Radiculopathy: A Randomized Controlled Trial” (2021)
Summary: Examines the efficacy of combining cervical traction and osteopathic mobilization in improving cervical radiculopathy symptoms.
Read Study
5. “Osteopathic Manipulative Treatment Combined with Exercise Improves Pain and Disability” (2020)
Summary: Shows significant benefits of combining osteopathic treatments with exercise in alleviating neck pain and disability, which are key in radiculopathy management.
Read Study
6. “The Somatic Connection: Manual Therapy Is Beneficial for Cervical Radiculopathy” (2013)
Summary: Highlights how osteopathic manual therapy alleviates symptoms of cervical radiculopathy, focusing on its somatic benefits.
Read Study
7. “Efficacy Comparison of Osteopathic Techniques and Cervical Mobilization in Cervical Spondylosis” (2024)
Summary: Compares the effectiveness of osteopathic muscle energy techniques and cervical mobilization in improving pain and disability.
Read Study (PDF)
8. “Effectiveness of Neuromobilization in Patients with Cervical Radiculopathy” (2022)
Summary: Systematic review showing how osteopathic neuromobilization techniques reduce pain and improve functionality in cervical radiculopathy.
Read Study
9. “Spinal Manipulation in Patients with Disc Herniation: A Critical Review” (2006)
Summary: Evaluates the safety and effectiveness of spinal manipulation, including osteopathy, in managing cervical radiculopathy linked to herniated discs.
Read Study
10. “Manual Therapy for Cervical Radiculopathy: A Review” (2016)
Summary: Reviews manual therapy approaches for cervical radiculopathy, highlighting osteopathy’s role in symptom alleviation and functional recovery.
Read Study (PDF)
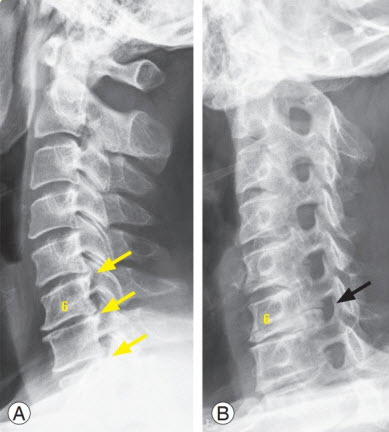
Radiographic signs
Radiographic signs of cervical radiculopathy can be seen through different medical imaging tests, such as x-rays, MRI (magnetic resonance imaging) or CT scans. These signs can indicate changes in the cervical spine and offer clues to the presence of nerve compression. Here are some of the radiographic signs that healthcare professionals can look for when evaluating cervical radiculopathy:
- Narrowing of the spinal canal: Narrowing of the cervical spinal canal may be seen on x-rays, indicating cervical stenosis, which may contribute to nerve root compression.
- Herniated disc: A herniated cervical disc can be seen on an MRI. It manifests itself by a protrusion or protrusion of the intervertebral disc into the space occupied by the nerve roots.
- Osteophytes (many called “bone spurs”): Bony growths can develop along the edges of the vertebrae, often resulting from osteoarthritis. These osteophytes can put pressure on nerve roots.
- Enlargement of the foramen: The foramen, through which nerve roots exit the spine, may show signs of enlargement due to nerve compression.
- Vertebral displacement or instability: Instability or abnormal displacement of the vertebrae may be visible on x-rays.
- Subchondral sclerosis: Thickening or densification of the bone beneath the cartilage (subchondral sclerosis) may indicate degenerative changes.
- Alterations in Cervical Lordosis: Changes in the natural curvature of the cervical spine, such as loss of cervical lordosis, may be noted.
It is important to note that radiographic signs may vary depending on the stage of cervical radiculopathy and the severity of structural changes.
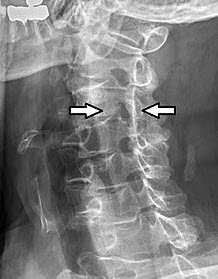
Cervical radiculopathy occurs when nerve roots in the cervical spine are compressed, often due to structural abnormalities such as osteophytes, herniated discs, or degenerative changes. In this case, the stenosis of the intervertebral foramen is likely contributing to the patient’s symptoms, which may include pain radiating to the arm, tingling, numbness, or even muscle weakness in the affected area.
Radiographic imaging is an essential diagnostic tool for identifying the underlying causes of nerve compression. This lateral projection provides a clear view of the vertebral alignment, intervertebral disc spaces, and bony structures, enabling clinicians to pinpoint the site of pathology. Understanding the precise location of the nerve compression helps guide treatment options, which may range from conservative therapies like physical therapy and medication to surgical interventions for severe cases.
Conclusion
In conclusion, cervical radiculopathy, or “pinched nerve” in the neck, represents a potentially disabling condition resulting from compression of a nerve root emerging from the spinal canal. Various symptoms, such as pain, numbness and muscle weakness, can significantly impair the quality of life of affected individuals.
The causes of cervical radiculopathy are diverse, ranging from herniated discs to bone spurs to spinal stenoses. These compression factors contribute to the disruption of nerve signals, thereby generating a range of symptoms specific to the cervical region.
Diagnosis of this condition is based on a thorough clinical assessment, supported by imaging tests such as x-rays and MRIs. Once diagnosed, management of cervical radiculopathy often involves a stepwise approach, starting with conservative treatments such as anti-inflammatory medications, physical therapy, and corticosteroid injections.
However, in cases that are more complex or resistant to non-surgical treatments, surgery may be considered to release the compressed nerve root. This highlights the importance of close collaboration between the patient and the medical team to determine the best therapeutic approach suited to each case.
Cervical radiculopathy highlights the importance of increased awareness of symptoms and seeking early medical evaluation for persistent pain in the neck, shoulders, or arms. Developing a personalized treatment plan, taking into account the severity of symptoms and underlying causes, is crucial to minimizing the impact of this condition on daily life.
Ultimately, an integrated approach, combining medical, physiotherapeutic and sometimes surgical interventions, offers promising prospects in the management of cervical radiculopathy. Improving understanding of this condition and access to appropriate care play a crucial role in improving the quality of life of individuals facing this medical challenge.
References
- Peolsson A, Peterson G, Hermansen A, Ludvigsson ML, Dedering Å, Löfgren H. Physiotherapy after anterior cervical spine surgery for cervical disc disease: study protocol of a prospective randomised study to compare internet-based neck-specific exercise with prescribed physical activity. BMJ Open. 2019 Feb 19;9(2):e027387. [PMC free article] [PubMed]2.
- Hassan KZ, Sherman AL. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 17, 2023. Epidural Steroids. [PubMed]3.
- Doughty CT, Bowley MP. Entrapment Neuropathies of the Upper Extremity. Med Clin North Am. 2019 Mar;103(2):357-370. [PubMed]4.
- Ament JD, Karnati T, Kulubya E, Kim KD, Johnson JP. Treatment of cervical radiculopathy: A review of the evolution and economics. Surg Neurol Int. 2018;9:35. [PMC free article] [PubMed]5.
- Lukies MW, Teoh WW, Clements W. Safety of CT-guided cervical nerve root corticosteroid injections. J Med Imaging Radiat Oncol. 2019 Jun;63(3):300-306. [PubMed]6.
- Miyoshi K. [Dissociation of Anatomical (Neurological) Diagnosis and Imaging Diagnosis]. Brain Nerve. 2019 Mar;71(3):249-256. [PubMed]7.
- Jenkins HJ, Downie AS, Moore CS, French SD. Current evidence for spinal X-ray use in the chiropractic profession: a narrative review. Chiropr Man Therap. 2018;26:48. [PMC free article] [PubMed]8.
- Bise S, Pesquer L, Feldis M, Bou Antoun M, Silvestre A, Hocquelet A, Dallaudière B. Comparison of three CT-guided epidural steroid injection approaches in 104 patients with cervical radicular pain: transforaminal anterolateral, posterolateral, and transfacet indirect. Skeletal Radiol. 2018 Dec;47(12):1625-1633. [PubMed]9.
- Nordin M, Randhawa K, Torres P, Yu H, Haldeman S, Brady O, Côté P, Torres C, Modic M, Mullerpatan R, Cedraschi C, Chou R, Acaroğlu E, Hurwitz EL, Lemeunier N, Dudler J, Taylor-Vaisey A, Sönmez E. The Global Spine Care Initiative: a systematic review for the assessment of spine-related complaints in populations with limited resources and in low- and middle-income communities. Eur Spine J. 2018 Sep;27(Suppl 6):816-827. [PubMed]10.
- Fehlings MG, Tetreault LA, Riew KD, Middleton JW, Aarabi B, Arnold PM, Brodke DS, Burns AS, Carette S, Chen R, Chiba K, Dettori JR, Furlan JC, Harrop JS, Holly LT, Kalsi-Ryan S, Kotter M, Kwon BK, Martin AR, Milligan J, Nakashima H, Nagoshi N, Rhee J, Singh A, Skelly AC, Sodhi S, Wilson JR, Yee A, Wang JC. A Clinical Practice Guideline for the Management of Patients With Degenerative Cervical Myelopathy: Recommendations for Patients With Mild, Moderate, and Severe Disease and Nonmyelopathic Patients With Evidence of Cord Compression. Global Spine J. 2017 Sep;7(3 Suppl):70S-83S. [PMC free article] [PubMed]11.
- Guan Q, Xing F, Long Y, Xiang Z. Cervical intradural disc herniation: A systematic review. J Clin Neurosci. 2018 Feb;48:1-6. [PubMed]12.
- Mattozzi I. [Conservative treatment of cervical radiculopathy with 5% lidocaine medicated plaster]. Minerva Med. 2015 Feb;106(1):1-7. [PubMed]13.
- Carlesso LC, Macdermid JC, Gross AR, Walton DM, Santaguida PL. Treatment preferences amongst physical therapists and chiropractors for the management of neck pain: results of an international survey. Chiropr Man Therap. 2014 Mar 24;22(1):11. [PMC free article] [PubMed]14.
- Kuligowski T, Skrzek A, Cieślik B. Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health. 2021 Jun 07;18(11) [PMC free article] [PubMed]15.
- Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS J. 2011 Oct;7(3):265-72. [PMC free article] [PubMed]16.
- Bukhari SR, Shakil-Ur-Rehman S, Ahmad S, Naeem A. Comparison between effectiveness of Mechanical and Manual Traction combined with mobilization and exercise therapy in Patients with Cervical Radiculopathy. Pak J Med Sci. 2016 Jan-Feb;32(1):31-4. [PMC free article] [PubMed]17.
- Ramirez MM, Brennan GP. Using the value-based care paradigm to compare physical therapy access to care models in cervical spine radiculopathy: a case report. Physiother Theory Pract. 2020 Dec;36(12):1476-1484. [PubMed]18.
- Cerier E, Jain N, Lenobel S, Niedermeier SR, Stammen K, Yu E. Smoking is Associated With 1-year Suboptimal Patient-reported Outcomes After 2-level Anterior Cer

























{kind=link}