

Hip fracture in the elderly is a break located at the femoral head. It is common in older people who suffer from osteoporosis.
Synonym: Femoral neck fracture, fracture of the upper end of the femur
Introduction
Hip fracture in the elderly constitutes a serious medical problem, with significant consequences on the health and quality of life of the individuals concerned. Often triggered by a fall, a common event among older adults due to the loss of stability and decreased bone density associated with aging, this fracture is of particular importance due to its impact on mobility.
The hip joint, essential for walking and balance, has its function impaired during a fracture, leading to a drastic reduction in independence. Affected older adults may experience severe pain, an inability to bear weight on the affected leg, and often, a loss of confidence in their ability to move safely.
Treatment of hip fracture in older adults generally requires a multidisciplinary approach. Although surgery is often essential to stabilize the fracture, fragile patients require special precautions. The postoperative recovery phase proves to be a prolonged and demanding process, involving attentive care, physical rehabilitation, and in many cases, psychological support to overcome the emotional challenges associated with the temporary loss of independence.
Fall prevention is a crucial aspect of the management of hip fractures in older adults. Measures such as improving home lighting, using non-slip mats, and participating in exercise programs aimed at strengthening stability and balance can help reduce the risk of falls and, in turn, consequently, hip fractures.
Factors That May Compromise Balance and Predispose Elderly Patients to Hip Fractures
Hip fractures are a significant concern in the elderly population, often leading to long-term disability, loss of independence, or even death. One of the primary contributors to hip fractures in older adults is compromised balance, which makes them more susceptible to falls. There are numerous factors that can affect balance in the elderly, each playing a role in increasing the risk of falling and thus suffering a hip fracture. Below are the key factors that may compromise balance and contribute to this increased risk in elderly individuals.
Factors that compromise balance in older adults may contribute to an increased risk of falls and, therefore, predispose these individuals to hip fractures. Some of these factors include:
List of Factors
1. Age-Related Muscle Weakness (Sarcopenia)
As people age, they experience a natural loss of muscle mass and strength, a condition known as sarcopenia. This decline in muscle mass is particularly pronounced in the muscles that support posture and balance, such as those in the legs, hips, and core.
- Impact on Balance: Muscle weakness compromises an individual’s ability to maintain stability during standing and walking. Without strong muscles to support the body, elderly individuals are more likely to lose their balance, stumble, or fall, increasing their risk of a hip fracture.
- Outcome: Loss of muscle strength, combined with the natural decline in bone density due to osteoporosis, makes falls more frequent and hip fractures more likely to occur upon impact.
2. Poor Vision
Vision plays a critical role in maintaining balance because it provides spatial awareness and helps the brain assess distance and obstacles in the environment. As people age, they commonly experience vision deterioration due to conditions like cataracts, glaucoma, and macular degeneration.
- Impact on Balance: Reduced vision makes it harder to detect hazards such as uneven surfaces, steps, or obstacles on the ground, leading to an increased risk of trips and falls.
- Outcome: Poor vision combined with other balance-compromising factors increases the risk of falls that can lead to hip fractures. Regular vision exams and corrective measures, such as wearing glasses or undergoing cataract surgery, can help mitigate this risk.
3. Vestibular Dysfunction
The vestibular system in the inner ear is responsible for providing the brain with information about balance and spatial orientation. As people age, the function of the vestibular system may decline, leading to dizziness or vertigo, both of which can compromise balance.
- Impact on Balance: Elderly individuals with vestibular dysfunction may experience frequent episodes of dizziness or unsteadiness, which can lead to falls, especially during transitions, such as standing up or walking after sitting for a long period.
- Outcome: Vestibular dysfunction increases the likelihood of falls that can result in hip fractures. Vestibular rehabilitation or medical management may be necessary to reduce dizziness and improve balance.
4. Neurological Disorders
Conditions like Parkinson’s disease, stroke, multiple sclerosis, and peripheral neuropathy affect the nervous system and can severely impact balance and coordination. In Parkinson’s disease, for example, muscle rigidity and tremors make it difficult to initiate and control movements. Similarly, peripheral neuropathy, often caused by diabetes, affects sensation in the feet, leading to an increased risk of losing balance.
- Impact on Balance: Neurological disorders compromise the ability to sense the ground and move the body smoothly, increasing the risk of falls.
- Outcome: Elderly individuals with neurological disorders are at a higher risk of hip fractures because their reduced coordination and proprioception make falls more likely. Physical therapy and medication management can help improve balance in these individuals.
5. Medications
Certain medications commonly used by the elderly can have side effects that compromise balance. For example, sedatives, antidepressants, blood pressure medications, and sleep aids can cause dizziness, drowsiness, and postural hypotension (a sudden drop in blood pressure when standing), which all contribute to a higher fall risk.
- Impact on Balance: Medications that cause dizziness or drowsiness affect the central nervous system’s ability to coordinate movements, which can lead to stumbling or falling, especially when getting up quickly.
- Outcome: Regular medication reviews by healthcare providers can help reduce the risk of falls. Adjusting dosages or switching to medications with fewer balance-related side effects can make a significant difference in preventing falls and fractures.
6. Environmental Hazards
Environmental factors such as poor lighting, slippery floors, clutter, and uneven surfaces can compromise balance, especially in elderly individuals with impaired mobility or vision. Tripping on loose rugs, stairs without handrails, or slipping in the bathroom are common causes of falls in older adults.
- Impact on Balance: Environmental hazards can quickly turn into fall risks for elderly individuals with compromised balance. Slipping or tripping in the home can lead to falls, which may result in hip fractures.
- Outcome: Home modifications like installing grab bars, non-slip mats, improving lighting, and removing tripping hazards can greatly reduce the risk of falls.
7. Chronic Conditions and Fatigue
Chronic illnesses such as arthritis, heart disease, and chronic obstructive pulmonary disease (COPD) can reduce physical stamina and make it difficult for elderly individuals to maintain balance during activities. Fatigue from chronic conditions can make walking and standing feel more challenging, increasing the risk of falls.
Outcome: Addressing chronic conditions through appropriate medical management, physical therapy, and energy conservation techniques can improve balance and reduce the risk of hip fractures.
Impact on Balance: Individuals with chronic conditions often experience pain, fatigue, and reduced mobility, which weakens their ability to stay balanced, particularly during movement or transitions.
8. Decreased Proprioception
Proprioception is the body’s ability to sense its position in space, and it is crucial for maintaining balance during activities like standing, walking, or shifting weight. As people age, proprioception declines due to changes in the nervous system, and this can significantly affect balance.
- Impact on Balance: When proprioception is impaired, it becomes difficult to make subtle adjustments to body posture. Older adults may not realize they are losing balance until it’s too late to correct it, leading to falls.
- Outcome: Falls caused by decreased proprioception often occur during transitions, such as getting up from a seated position or changing direction while walking. Balance exercises such as tai chi or yoga can help improve proprioception in elderly individuals and reduce the risk of falls and hip fractures.
9. Dehydration
Dehydration is common among the elderly, often due to factors like reduced thirst sensation, certain medications, or chronic illnesses. Dehydration can lead to dizziness, confusion, low blood pressure, and weakness, all of which can compromise balance.
- Impact on Balance: When an elderly person is dehydrated, they are more prone to episodes of lightheadedness, particularly when standing up or moving quickly. This can lead to fainting or staggering, resulting in a fall.
- Outcome: Ensuring that elderly individuals remain adequately hydrated, especially during hot weather or illness, is crucial for preventing dehydration-related falls. Encouraging regular fluid intake and monitoring hydration status can help reduce balance issues and hip fractures caused by dehydration.
10. Foot Problems and Inappropriate Footwear
Foot conditions such as bunions, calluses, arthritis, or neuropathy (nerve damage, often due to diabetes) can alter gait and compromise balance. Additionally, wearing improper footwear, such as high heels, flip-flops, or worn-out shoes, can increase the risk of falls.
- Impact on Balance: Painful or dysfunctional feet can lead to instability when walking, increasing the likelihood of tripping or losing balance. Inappropriate footwear further exacerbates the problem, as it may not provide adequate support, traction, or shock absorption.
- Outcome: Encouraging the use of well-fitting shoes with nonslip soles and sufficient support can significantly reduce the risk of falls. Regular visits to a podiatrist to address foot problems and ensure proper foot care can also help improve balance and prevent hip fractures.
11. Cognitive Impairmen
Cognitive decline or dementia is another significant factor that can compromise balance and coordination in elderly individuals. Conditions like Alzheimer’s disease or vascular dementia may cause confusion, disorientation, and difficulty in judging distances or identifying obstacles in the environment.
- Impact on Balance: Cognitive impairment reduces the ability to navigate spaces safely and make quick adjustments to prevent a fall. Elderly individuals with cognitive decline may not remember to use assistive devices (like canes or walkers), or they may forget safety instructions, increasing their risk of falls.
- Outcome: Environmental modifications and supervision are critical in preventing falls in patients with cognitive impairment. Implementing clear pathways, non-slip flooring, and assistive devices can reduce fall risk, while cognitive training and medication management can further enhance safety.
12. Fear of Falling (Post-Fall Syndrome)
After experiencing a fall, many elderly individuals develop a fear of falling again, which can lead to a vicious cycle of reduced mobility, muscle weakness, and further loss of balance. This fear causes them to avoid physical activities or use cautious, hesitant movements that paradoxically increase the risk of falling.
- Impact on Balance: Fear of falling often leads to immobility, which further reduces muscle strength and balance. The avoidance of physical activities can also lead to social isolation, depression, and loss of confidence in walking or standing, all of which compound the risk of falls.
- Outcome: Fall prevention programs that focus on building confidence through strength training and balance exercises are essential for individuals who are afraid of falling. Physical therapists and occupational therapists can provide strategies to improve mobility and reduce fear, helping to lower the risk of hip fractures.
13. Nutritional Deficiencies
Elderly individuals are at higher risk of nutritional deficiencies, particularly calcium, vitamin D, and protein, all of which are critical for maintaining bone health and muscle strength. Poor nutrition can lead to weak muscles, brittle bones, and compromised coordination.
- Impact on Balance: A lack of adequate nutrition weakens the muscles that help maintain posture and balance. In addition, vitamin D deficiency can contribute to osteomalacia (soft bones), which further compromises bone strength and increases the risk of fractures.
- Outcome: Ensuring a balanced diet with enough calcium, vitamin D, and protein is critical for maintaining muscle and bone health in older adults. In some cases, supplements may be necessary to correct deficiencies and improve overall balance and bone strength, reducing the risk of hip fractures.
14. Postural Hypotension
Postural hypotension, also known as orthostatic hypotension, is a condition where blood pressure drops suddenly when standing up from a seated or lying position. It is common in elderly individuals, especially those taking blood pressure medications or diuretics. This sudden drop in blood pressure can cause dizziness, fainting, or lightheadedness, which can lead to falls.
- Impact on Balance: When blood pressure drops, the brain may not receive enough oxygen, resulting in brief blackouts or dizziness that can cause the individual to lose balance and fall.
- Outcome: Preventing postural hypotension-related falls involves managing medications, ensuring adequate hydration, and advising the individual to rise slowly from seated or lying positions. Physicians may also adjust medications or suggest compression stockings to maintain blood pressure stability.
15. Lack of Physical Activity
Sedentary lifestyles are common among the elderly due to health conditions, fatigue, or fear of falling. However, a lack of physical activity leads to muscle atrophy, joint stiffness, and reduced balance, all of which increase the risk of falls and hip fractures.
- Impact on Balance: Physical inactivity leads to weakened muscles and poor coordination, both of which are necessary for maintaining balance. The longer a person remains sedentary, the more difficult it becomes to regain strength and mobility, which further increases fall risk.
- Outcome: Engaging in regular physical activity, including strength training, balance exercises, and walking, is crucial for maintaining muscle tone and coordination. Programs designed for elderly individuals, such as tai chi, yoga, or water aerobics, are especially beneficial for improving balance and reducing the risk of hip fractures.
16. Reduced Reflexes and Reaction Time
As people age, their reaction time and reflexes tend to slow down, making it harder to quickly respond to situations that might compromise balance, such as tripping over an object or slipping on a wet surface.
- Impact on Balance: With slower reflexes, elderly individuals may not be able to react quickly enough to catch themselves or stabilize their posture when they stumble. The body’s natural ability to make small corrections in posture to maintain balance is diminished.
- Outcome: This delayed reaction increases the likelihood of a fall in unexpected situations. Balance training and exercises that improve agility and reflexes can help elderly individuals maintain quicker reaction times, reducing their risk of falling and suffering from hip fractures.
17. Chronic Pain
Many elderly individuals suffer from chronic pain, which can stem from conditions like arthritis, degenerative joint disease, or previous injuries. Chronic pain can affect mobility, balance, and confidence in walking.
- Impact on Balance: Chronic pain, especially in the hips, knees, or feet, can cause an abnormal gait or hesitation when moving. People with pain may move more slowly or awkwardly, which can compromise their stability and lead to falls.
- Outcome: Pain management strategies, including medications, physical therapy, or even joint replacement surgery, can help improve mobility and balance, thus reducing the risk of falls and hip fractures.
18. Joint Instability
Elderly individuals often experience joint instability due to the weakening of muscles, tendons, and ligaments, particularly around the hips, knees, and ankles. Conditions such as osteoarthritis can cause joint stiffness and instability.
- Impact on Balance: Unstable joints make it difficult to maintain balance, especially during activities that require rapid movements or weight shifts, such as walking on uneven surfaces or climbing stairs. Joint instability in the hips or ankles can make elderly individuals more prone to stumbling and falling.
- Outcome: Physical therapy focused on strengthening the muscles around the joints and improving joint stability can help reduce the risk of falls. In severe cases, bracing or even joint replacement surgery might be necessary to restore stability.
19. Sensory Decline
Aging is often associated with a decline in multiple sensory functions, including hearing, touch, and vision. Sensory inputs are critical for maintaining balance and spatial orientation.
- Impact on Balance: Elderly individuals with reduced sensation in their feet (common in conditions like diabetes or neuropathy) may have difficulty sensing the ground, leading to a loss of balance. Similarly, a decline in hearing can affect balance, as the auditory system also plays a role in spatial orientation.
- Outcome: Addressing sensory deficits through proper footwear, hearing aids, and maintaining a safe, well-lit environment can help compensate for these changes and reduce the risk of falls.
20. Medically Complex Conditions (Comorbidities)
Elderly individuals often suffer from multiple health conditions simultaneously, a situation known as multimorbidity. Conditions such as cardiovascular disease, diabetes, and chronic respiratory conditions can contribute to poor balance and increased fall risk.
- Impact on Balance: Many chronic conditions directly or indirectly compromise balance. For instance, cardiovascular conditions can cause dizziness, while diabetes can lead to neuropathy and impaired proprioception. Additionally, chronic lung diseases like COPD may cause fatigue and shortness of breath, reducing physical endurance and balance.
- Outcome: A holistic management approach is needed for elderly patients with multiple comorbidities. Ensuring proper medical care and addressing each condition comprehensively can help improve overall health and reduce balance-related issues.
21. Overreliance on Assistive Devices
While assistive devices like canes and walkers can help improve mobility, they can also present a risk if not used correctly or if an individual becomes overly reliant on them.
- Impact on Balance: Improper use of assistive devices can lead to loss of balance. For example, if a cane is used incorrectly or a walker isn’t the right size, the individual may trip over the device or fail to support themselves adequately. Additionally, overreliance on these devices can cause muscle weakness and reduce natural balance abilities.
- Outcome: Ensuring that assistive devices are used correctly and that elderly individuals maintain an exercise routine to strengthen muscles and enhance balance is important for preventing falls. Training by a physical therapist on how to properly use these devices can reduce risks.
22. Urinary Urgency and Incontinence
Urinary incontinence or urgency is a common problem among elderly individuals. The urgent need to get to the bathroom quickly can cause them to rush or move too quickly, leading to slips and falls.
- Impact on Balance: Incontinence can create situations where elderly individuals rush to get to the bathroom, especially at night when visibility is low. Hurrying or not paying attention to their surroundings increases the likelihood of tripping, stumbling, or losing balance.
- Outcome: Managing incontinence through bladder training, medications, and environmental modifications, such as installing bathroom grab bars and ensuring adequate lighting, can help reduce the risk of falls and related hip fractures.
23. Lack of Social Interaction and Isolation
Social isolation is a significant issue for many elderly individuals, particularly those who live alone or are homebound due to health conditions. Lack of social interaction can lead to depression, anxiety, and even physical inactivity, all of which can contribute to poor balance.
- Impact on Balance: When elderly individuals are isolated, they may become less active, weakening their muscles and coordination. Additionally, isolation may cause mental health issues like depression, which is associated with fatigue and slower reaction times, further increasing the risk of falls.
- Outcome: Encouraging social interaction and community involvement can improve both mental and physical health. Group exercise classes designed for older adults, such as tai chi or yoga, can help improve balance, reduce fall risk, and alleviate feelings of loneliness.
24. Poor Sleep Quality
Sleep disturbances are common in elderly individuals, often due to chronic pain, anxiety, or other health conditions. Poor sleep quality or insomnia can result in daytime drowsiness, reduced alertness, and impaired balance.
- Impact on Balance: Sleep deprivation affects reaction time, motor coordination, and cognitive function, all of which are essential for maintaining balance. Fatigue increases the risk of missteps and falls, especially during nighttime trips to the bathroom.
- Outcome: Improving sleep quality through sleep hygiene, addressing underlying sleep disorders, and ensuring a safe nighttime environment can help prevent falls and related hip fractures.
Epidemiology of Hip Fractures in Canada
In Canada, hip fractures represent a significant public health concern, particularly among the aging population. By 1990, the global incidence of hip fractures had reached 1.3 million annually, and this number is projected to rise to between 7 and 21 million by 2050. In Canada, the risk of hip fractures doubles with each decade after the age of 50, similar to global trends. Studies show that hip fractures are more common in women, with Canadian women over 50 experiencing a much higher incidence compared to men, following a ratio observed globally.
In Canada, the annual incidence per 100,000 inhabitants for hip fractures ranges from approximately 500 to 600 for women and 200 to 250 for men, closely aligned with international data. The average age of patients experiencing a hip fracture is around 80 years, and these injuries carry significant mortality risks. One in three Canadians aged 50 and above who suffer a hip fracture will die within 12 months of the incident, with the highest risk occurring in the first three months. Older adults have a five to eight times higher chance of mortality after a hip fracture, and this elevated risk persists for up to a decade, making the fracture a severe prognostic indicator.
Furthermore, around one in seven Canadian women will experience a hip fracture in her lifetime, often leading to the need for a hip replacement. Hip fractures not only increase mortality but also contribute to long-term disability, decreased quality of life, and a substantial burden on healthcare systems. Efforts to prevent falls and fractures, alongside early intervention, remain critical to mitigating these risks in the aging population.
Causes of hip fracture in the elderly
Osteoporosis
One of the most common causes of hip fractures is osteoporosis, a condition characterized by the weakening of bones. Osteoporosis makes bones fragile and more prone to fractures even from minor impacts. In particular, the elderly are highly susceptible to this condition due to natural bone density loss that occurs with aging. Women are especially at risk after menopause because of the drop in estrogen levels, which plays a critical role in maintaining bone density.
Key Points:
- Reduced bone density leads to a higher risk of fractures.
- Osteoporosis primarily affects postmenopausal women but can occur in men as well.
- Lack of calcium and vitamin D can exacerbate bone weakness.
Falls
Falls are a leading cause of hip fractures, particularly in older adults. As people age, their balance, coordination, and muscle strength typically decline, making them more prone to falling. When a person with weakened bones falls, especially if they land on their hip, the risk of fracturing the hip is significant.
Key Points:
- Falls are often triggered by poor balance, slippery surfaces, or inadequate footwear.
- Muscle weakness, vision impairments, and neurological conditions contribute to fall risk.
- Most hip fractures occur indoors, often from falls at home.
Age-related Factors
Aging itself is a significant risk factor for hip fractures. As people age, various physiological changes occur that can increase susceptibility to injury. For instance, bones become thinner and weaker, muscles lose mass and strength (sarcopenia), and reflexes slow down. Additionally, aging often comes with impaired vision and cognitive decline, further increasing the likelihood of falls and injuries.
Key Points:
- Bone density decreases with age, leading to frailty.
- Muscle atrophy and slower reflexes increase the chances of falls.
- Elderly individuals may experience slower healing after a fracture.
Physical Inactivity
A sedentary lifestyle can also contribute to the risk of hip fractures. Regular physical activity helps to maintain muscle strength, balance, and bone health. Conversely, lack of exercise leads to muscle weakening, poor coordination, and decreased bone density, all of which increase the likelihood of falls and fractures.
Key Points:
- Inactive individuals have weaker muscles and bones, which leads to an increased risk of fractures.
- Exercises that promote balance and strength can help reduce the risk.
- Weight-bearing activities like walking and light resistance training can strengthen bones.
5. Medical Conditions
Certain medical conditions can increase the risk of hip fractures. Conditions that affect mobility, balance, and bone health are particularly concerning. For example, individuals with Parkinson’s disease, stroke, or arthritis may experience difficulties in walking, increased fall risk, and weakened bones. Additionally, diseases like hyperthyroidism and rheumatoid arthritis can lead to bone loss, while diabetes is linked to poor muscle function and balance.
Key Points:
- Parkinson’s disease, stroke, and arthritis impair mobility and increase fall risk.
- Hyperthyroidism and diabetes may weaken bones and muscles.
- Osteomalacia (softening of bones) can further exacerbate fracture risks.
Medications
Certain medications, particularly those used to treat chronic illnesses, can contribute to hip fracture risk. Medications such as sedatives, antidepressants, and antipsychotics may cause drowsiness, dizziness, or loss of balance, increasing the chances of falling. Long-term use of corticosteroids is also known to cause bone thinning, which weakens the bones and makes fractures more likely.
Key Points:
- Sedatives and antidepressants can cause dizziness or loss of balance.
- Long-term corticosteroid use weakens bones.
- Drug interactions may exacerbate risk factors for falls and fractures.
Environmental Hazards
Environmental factors, particularly at home, play a significant role in causing falls that lead to hip fractures. Hazards such as loose rugs, poor lighting, clutter, and slippery floors can make it easy for older adults to trip or slip. The absence of handrails or grab bars in bathrooms or on stairs can also increase the risk of falls.
Key Points:
- Poor lighting, slippery surfaces, and clutter contribute to fall risks.
- Installing grab bars and using non-slip mats can help prevent falls.
- Ensuring proper footwear and assistive devices can reduce hazards.
Other Contributing Factors
In addition to the factors above, lifestyle choices like poor diet and smoking can also increase the risk of hip fractures. Smoking is known to reduce bone density, while a diet lacking in essential nutrients like calcium and vitamin D can weaken bones. Excessive alcohol consumption can impair balance and coordination, raising the likelihood of falls.
Key Points:
- Smoking reduces bone density, increasing fracture risk.
- Poor nutrition leads to weaker bones and muscles.
- Excessive alcohol use can impair coordination, leading to falls.
Symptoms of hip fracture in the elderly
- Pain: Hip pain is often intense and localized. The person may feel severe pain in the hip or groin. Sometimes the pain may radiate to the thigh, knee, or groin area.
- Inability to bear weight: The person may have difficulty bearing weight on the affected leg and may experience severe pain when trying to stand or walk.
- Difficulty moving the leg: Due to pain and instability, the person may have difficulty moving the affected leg or performing movements of the hip joint.
- Discomfort or swelling: The area around the hip may be swollen, and there may be tenderness or discomfort to the touch.
- Abnormal leg rotation: The affected leg may appear to rotate outward abnormally, especially if the fracture is at the head of the femur.
- Leg length discrepancies: The affected leg may appear shorter than the other due to deformity resulting from the fracture.
- Immobilization: The person may have difficulty moving or turning the affected leg and may prefer to remain still due to the pain.
***Elderly patients with hip pain after a fall should be treated as if they had a hip fracture until proven otherwise.***
Classification (Delbet) of hip fracture
The classification of hip fracture according to Delbet, proposed at the beginning of the 20th century by the French surgeon Pierre Delbet, remains a historical reference in the medical field. This ancient classification categorizes hip fractures into four main types based on the specific location of the fracture.
His work was instrumental in shaping modern orthopedic practices, making him a notable figure in the history of medical science. Delbet’s techniques and research had a profound influence on the treatment of fractures, especially in an era when many of the current surgical standards were still in their formative stages.
The first type of fracture identified by Delbet concerns the cervical region, which is the part of the femur close to the head of the femur. This type of cervical fracture can have significant implications on the vascularization of the femoral head, potentially leading to severe complications.
The second type of fracture is located at the greater trochanter, a bony protuberance at the base of the femoral neck. Fractures of this type can influence the stability of the hip joint and often require surgical attention.
The third category of fractures, according to Delntertrochanteric area, located between the greater trochanter and the cervical part of the femur. These fractures can present particular challenges due to their proximity to critical bony and vascular structures.
Finally, the fourth type of fracture according to this classification is located at the level of the subtrochanter, the region located under the major trochanter. These fractures can affect the mechanical stability of the hip and often require surgery to restore normal function.
Although Delbet’s classification played an important role in the understanding of hip fractures in its time, it is essential to note that more modern classifications are preferred in the medical field today. These more recent classifications take into account different factors, such as the specific nature of the fracture, the type of displacement of the bone fragments, and other important anatomical characteristics.
In conclusion, although the Delbet classification remains a historical reference, medical advances have led to the evolution of more precise classification methods adapted to current needs. Understanding these classifications, ancient and modern, is crucial for healthcare professionals in the diagnosis and management of hip fractures, ensuring appropriate interventions and optimal patient outcomes.
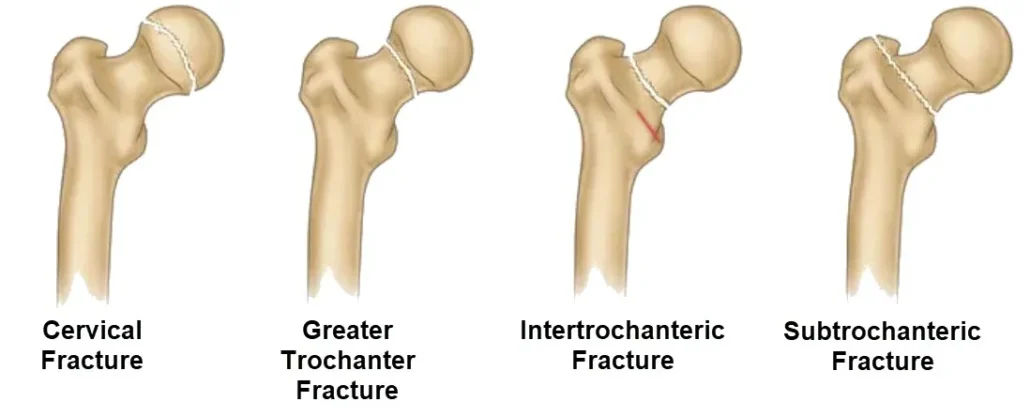
Cervical Fracture: This fracture occurs in the neck of the femur, just below the ball of the hip joint. It is often seen in older adults and is commonly associated with osteoporosis. These fractures can lead to complications in blood supply to the femoral head.
Greater Trochanter Fracture: Located at the bony prominence on the upper side of the femur, this fracture typically results from direct trauma or falls. Although less common, these fractures can cause significant pain and mobility issues.
Intertrochanteric Fracture: Occurs between the greater and lesser trochanter of the femur. This type of fracture is more common in elderly patients and is generally treated with surgery.
Subtrochanteric Fracture: This fracture occurs just below the trochanteric region and can be particularly challenging to treat due to the complex forces acting on this area during movement. It often requires surgical intervention.
- Type I – Cervical Fracture: This category concerns fractures located in the cervical region of the femur, near the head of the femur. Cervical fractures can have severe implications due to their proximity to the blood supply to the femoral head
- Type II – Greater Trochanter Fracture: Fractures in this category occur at the greater trochanter, a bony protrusion at the base of the femoral neck. They can influence the stability of the hip joint.
- Type III – Intertrochanteric Fracture: This category concerns fractures located in the intertrochanteric area, between the greater trochanter and the cervical part of the femur. These fractures can present particular challenges due to their proximity to crucial bony and vascular structures.
- Type IV – Subtrochanteric Fracture: Subtrochanteric fractures are located in the region below the greater trochanter. They can affect the mechanical stability of the hip, often requiring surgery to restore normal function.
Complication of intracapsular hip fracture
- Avascular necrosis of the femoral head: A common complication of intracapsular fractures, particularly those of the femoral neck, is avascular necrosis of the femoral head. This occurs when the blood supply to the femoral head is compromised due to the fracture, which can lead to bone cell death.
- Osteoarthritis: Intracapsular fractures can increase the risk of developing osteoarthritis of the hip, particularly if the fracture is not properly treated and heals poorly.
- Nonunion or delayed union: Some fractures may have difficulty healing properly, which can result in nonunion (lack of healing) or delayed union (slower than normal healing).
- Vascular and nervous complications: In the event of a severe fracture, there is a risk of associated vascular or nerve damage. Injury to surrounding blood vessels or nerves can have serious consequences.
- Infection: Any open fracture (perforation of the skin) exposes the fracture site to the risk of infection. Infections can delay healing and cause other complications.
- Mobility and function problems: Hip fractures can lead to mobility and function problems, especially in older adults. Recovery can be long, and some people may have difficulty returning to their previous level of activity.
- Fat embolism syndrome: In some severe hip fractures, there may be a release of fat particles into the bloodstream, causing fat embolism syndrome. This can lead to pulmonary and neurological complications.
Logical Pathway to Hip Fracture Diagnosis
A logical and systematic approach is essential for accurate diagnosis, appropriate treatment, and optimal patient outcomes. The pathway to diagnosing a hip fracture involves clinical assessment, imaging, and differential diagnosis, all performed with urgency, given the complications that can arise from delayed intervention. Below is the logical pathway to diagnose a hip fracture.
Pathway to diagnosis
1. Clinical History and Presentation
The diagnostic process begins with a thorough clinical history, focusing on the mechanism of injury and patient symptoms. Hip fractures typically result from trauma, most commonly a fall in elderly patients. However, they can also occur due to high-energy impacts, such as in motor vehicle accidents, or pathological conditions that weaken the bone, like cancer or osteoporosis.
The typical patient with a hip fracture presents with:
- Severe pain in the groin or hip area, exacerbated by movement.
- Inability to bear weight on the affected leg.
- Shortened and externally rotated leg, a characteristic sign of femoral neck or intertrochanteric fractures.
In cases of pathological fractures, the patient might have reported chronic pain prior to the acute event due to underlying conditions such as bone metastasis.
2. Physical Examination
During the physical examination, key features confirming a hip fracture include:
- Pain on palpation of the hip or femoral area.
- External rotation and shortening of the affected limb.
- Impaired mobility of the hip joint.
- In cases where the fracture is not displaced, physical signs may be subtle, and the patient may still be able to move the leg, though with pain.
An assessment of overall patient health, comorbid conditions, and prior functional status is important, as these will guide treatment decisions, such as whether surgical or conservative management is more appropriate.
3. Imaging for Diagnosis
Imaging is the cornerstone for confirming a hip fracture diagnosis and classifying the type and severity of the fracture. There are various modalities used to visualize and evaluate the injury:
- X-ray: The first-line imaging modality for diagnosing hip fractures. A standard anteroposterior (AP) view of the pelvis and a lateral view of the hip can help identify fractures, displacement, and alignment issues.
- Intracapsular fractures (such as femoral neck fractures) often appear with a displaced femoral head or a subcapital break.
- Extracapsular fractures (such as intertrochanteric fractures) involve the broader region outside the hip capsule and may show multiple fragments.
- MRI: In cases where the X-ray is inconclusive (e.g., in non-displaced fractures or fractures of osteoporotic bones), an MRI is highly sensitive and can detect fractures not visible on X-rays. MRI is also valuable for diagnosing avascular necrosis (AVN) of the femoral head, as seen by the double line sign.
- CT scan: A CT scan provides detailed three-dimensional images and is particularly useful for evaluating complex fractures or planning surgery.
4. Differential Diagnosis
The diagnosis of a hip fracture can be complicated by other conditions that mimic the symptoms of a fracture. Therefore, it is important to consider the following in the differential diagnosis:
- Osteoarthritis: Can cause chronic hip pain and difficulty walking, but the onset is typically gradual compared to the acute pain of a fracture.
- Bursitis: Inflammation of the bursa in the hip joint can cause pain similar to a fracture, but without associated trauma.
- Muscle strains or contusions: These may present with localized pain after a fall but typically allow for some movement without the intense pain seen in fractures.
5. Classification of Hip Fractures
Once a hip fracture is confirmed, classification of the fracture helps guide treatment:
Extracapsular fractures: These occur outside the joint capsule and include intertrochanteric and subtrochanteric fractures. These tend to heal better due to a better blood supply.
Intracapsular fractures: These occur within the joint capsule and include femoral neck and subcapital fractures. These fractures are at high risk for complications like AVN due to the disruption of blood supply to the femoral head.
A Day in the Life of Someone Suffering from a Hip Fracture
6:00 AM: A Painful Awakening
James, a 68-year-old retired engineer, begins his day with a sharp reminder of his hip fracture. The injury, sustained from a fall, has left him with significant pain and limited mobility. As he slowly wakes up, the discomfort is acute, and moving from a lying to a sitting position requires careful maneuvering. James gingerly uses his walker to sit up, wincing with every shift. Applying an ice pack to his hip helps manage the swelling and soothe some of the pain before he begins his day.
7:00 AM: Morning Routine with Assistance
Getting ready for the day is a slow and deliberate process. James relies on a series of adaptive tools and techniques to manage his hip fracture. He uses a long-handled reacher to pick up clothes and a dressing stick to put on his pants without bending too much. Bathing is done using a shower chair and grab bars, which provide stability and reduce the risk of further injury. Despite these adjustments, the routine is laborious and often exhausting.
8:00 AM: Navigating the Commute
James’s commute to his medical appointment is carefully planned. He has arranged for a ride with a family member or a specialized transport service that accommodates his mobility needs. The car is equipped with a swivel seat to make entry and exit easier. The journey is uncomfortable due to prolonged sitting, and James takes frequent breaks to stretch and relieve pressure on his hip. Every movement is cautious, aiming to avoid exacerbating his injury.
9:00 AM: Medical Consultation
At the clinic, James meets with his orthopedic specialist for a follow-up. The appointment involves assessing his progress, adjusting his treatment plan, and discussing pain management strategies. The consultation is crucial for monitoring his recovery but often involves a lot of waiting and moving around, which can be physically draining. James appreciates the support of his healthcare team, who provide him with strategies to manage his pain and improve his mobility.
12:00 PM: Lunch and Rest
Returning home, James has a light lunch prepared by a caregiver or family member. He focuses on maintaining a balanced diet to support healing and overall health. The meal is often eaten while sitting comfortably in his recliner, which provides better support for his hip. After eating, James spends time resting, elevating his leg to reduce swelling and performing gentle range-of-motion exercises as advised by his therapist.
2:00 PM: Rehabilitation Exercises
In the afternoon, James dedicates time to his physical therapy exercises. These exercises are designed to strengthen the muscles around his hip and improve flexibility. Though sometimes painful, they are essential for his recovery. James follows a structured program, which includes gentle stretching, isometric exercises, and gradually increasing weight-bearing activities. Physical therapy is crucial for regaining mobility and reducing the risk of future complications.
4:00 PM: Engaging in Light Activities
The later part of the afternoon is spent engaging in light activities that don’t strain his hip. James might read, work on a puzzle, or enjoy a television show. He also uses this time to stay connected with friends and family through phone calls or video chats, which helps lift his spirits and provides a sense of normalcy despite his injury.
6:00 PM: Dinner and Evening Routine
Dinner is another opportunity for James to enjoy a nutritious meal while seated comfortably. After eating, he continues with his routine of elevating his leg and applying ice if needed. The evening is a quieter time, allowing James to relax and reflect on his day. He might do some light stretching exercises or practice relaxation techniques to manage pain and stress.
8:00 PM: Preparing for Bed
As bedtime approaches, James prepares for sleep with the help of a supportive sleep position. He uses pillows to keep his hip in a stable position and follows any specific instructions from his healthcare provider regarding sleep posture. The process of getting into bed requires careful movement to avoid discomfort, and James focuses on finding a position that alleviates pressure on his hip.
10:00 PM: Reflecting on the Day
Before falling asleep, James reflects on his day, grateful for the support of his caregivers and the progress he’s making in his recovery. Managing a hip fracture involves a combination of careful planning, pain management, and adherence to a rehabilitation program. Despite the challenges, James remains hopeful for continued improvement and a return to a more active lifestyle.
Differential diagnosis of intracapsular hip fracture
- Muscle sprain or tear: Muscle sprains or tears around the hip can cause pain similar to that of a fracture, but they do not necessarily involve an interruption in bone continuity.
- Hip dislocation: A hip dislocation can cause severe pain and inability to use the leg, but it does not necessarily result from a fracture. However, a hip dislocation can sometimes be associated with a fracture or ligament damage.
- Hip bursitis: Inflammation of the synovial bursae around the hip, called bursitis, can cause pain in the hip area, but it does not cause a fracture.
- Osteoarthritis of the hip: Osteoarthritis of the hip can cause pain similar to that of a fracture, especially in older people. However, osteoarthritis is a degenerative condition of the joints and does not result from an acute fracture.
- Tendonitis: Inflammation of the tendons surrounding the hip can cause local pain, but it does not represent a fracture.
- Deep vein thrombosis (DVT): DVT can cause pain and swelling in the leg, sometimes confused with fracture symptoms. However, DVT does not involve disruption of the bone.
- Fracture of other parts of the femur: It is important to distinguish intracapsular fractures from fractures of other parts of the femur, such as subtrochanteric or diaphyseal fractures.
Diagnosis and treatment of intracapsular hip fracture
Intracapsular hip fracture is a serious injury that occurs within the joint capsule of the hip joint. This capsule surrounds the joint and contains synovial fluid, which lubricates and nourishes the joint. Intracapsular fractures are generally classified into two main types: femoral neck fractures and femoral head fractures.
Diagnostic
- Imaging tests: X-rays are often used to diagnose intracapsular hip fractures. They make it possible to assess the location and severity of the fracture.
- CT scan: In some cases, a CT scan may be performed to obtain more detailed images of the fracture and its surrounding structures.
- Magnetic resonance imaging (MRI): MRI can be used to assess damage to the soft tissues around the hip, providing a more complete perspective of the injury.
Treatment
- Closed reduction: If the bone fragments retain some stability, closed reduction can be attempted. This involves realigning the fragments without resorting to surgery.
- Internal fixation: Most intracapsular fractures require surgery to stabilize the bone fragments. Internal fixation, such as the placement of screws or pins, is often performed to hold the bones in the correct position.
- Hip replacement: In severe cases, especially in older people, hip replacement (arthroplasty) may be recommended. This involves replacing the femoral head and sometimes the femoral neck with artificial implants.
- Rehabilitation: After surgery, rehabilitation is crucial to restore muscle strength, mobility and balance. Exercises are prescribed to promote recovery and minimize the risk of complications.
- Pain Management: Analgesic and anti-inflammatory medications may be prescribed to control postoperative pain and inflammation.
Prompt diagnosis and appropriate treatment of intracapsular hip fracture are essential to minimize complications and promote successful recovery. The choice of treatment depends on various factors, including the severity of the fracture, the patient’s age, and their general health.
Factors that contribute to the high risk of death after femoral neck fracture
Femoral neck fractures, particularly in older adults, are a significant medical issue due to their association with high morbidity and mortality rates. The femoral neck is the region of the thigh bone just below the ball of the hip joint. A fracture in this area, often resulting from a fall or other trauma, can lead to severe complications. Studies show that up to 30% of elderly patients may die within a year following a femoral neck fracture. Understanding the factors that contribute to this elevated risk of death is essential for prevention and effective management.
Age and Frailty
One of the primary factors contributing to the high risk of death following a femoral neck fracture is advanced age. As people age, their bones become more fragile due to a natural decline in bone density and muscle mass. This condition, known as osteoporosis, increases the likelihood of fractures from even minor trauma, such as a simple fall. Moreover, elderly individuals are more likely to suffer from frailty, a condition characterized by diminished strength, endurance, and physiological function. Frailty not only increases the risk of falls but also limits the body’s ability to recover from injuries.
Key Points:
- Elderly individuals often have weaker bones and muscles, making them more prone to fractures.
- Frailty decreases the body’s resilience, leading to complications during recovery.
- As age increases, so does the likelihood of multiple comorbidities that can exacerbate the recovery process.
Comorbidities and Chronic Illnesses
Patients with femoral neck fractures frequently have multiple chronic conditions, such as cardiovascular disease, diabetes, respiratory problems, or kidney disease. These comorbidities significantly affect the patient’s ability to recover from surgery or the injury itself. For example, cardiovascular diseases can increase the risk of complications like blood clots or heart failure, while diabetes can impair wound healing and increase the risk of infections. Respiratory conditions can lead to pneumonia or other breathing problems, which are common in immobile patients.
Key Points:
- Comorbid conditions such as heart disease, diabetes, and respiratory issues complicate recovery.
- Chronic illnesses increase the risk of postoperative complications and infections.
- Poor wound healing, infections, and blood clots are common complications in patients with comorbidities.
Surgical Complications
Surgery is the primary treatment for most femoral neck fractures, particularly in older patients, as non-surgical treatments are rarely effective. However, surgical intervention in elderly patients comes with significant risks. Anesthesia, blood loss, and the stress of surgery can have severe effects on an already compromised cardiovascular or respiratory system. Additionally, patients may suffer from postoperative complications like deep vein thrombosis, pulmonary embolism, or infections, all of which can be life-threatening.
Key Points:
- Surgical intervention is often necessary but carries risks, especially in elderly patients.
- Anesthesia and blood loss during surgery can lead to cardiovascular complications.
- Postoperative complications, such as blood clots and infections, are significant contributors to mortality.
Immobility and Hospitalization
After a femoral neck fracture, patients, especially older adults, often become immobilized during the recovery period. Prolonged immobility can lead to numerous complications, including deep vein thrombosis (DVT), pulmonary embolism, muscle atrophy, and pressure ulcers. Immobility also increases the risk of pneumonia, a serious lung infection that can be fatal, especially in older individuals. Furthermore, long hospital stays increase the risk of hospital-acquired infections such as urinary tract infections, sepsis, or pneumonia.
Key Points:
- Prolonged immobility following a fracture increases the risk of DVT, pulmonary embolism, and pressure ulcers.
- Muscle atrophy and respiratory infections like pneumonia can complicate recovery.
- Hospitalization increases the risk of acquiring infections, such as sepsis or pneumonia.
Malnutrition and Poor Nutritional Status
Many elderly patients suffer from malnutrition or poor nutritional status, which negatively impacts their ability to heal after a femoral neck fracture. Proper nutrition is essential for bone health, wound healing, and overall recovery. A lack of protein, vitamins (particularly vitamin D), and minerals like calcium can weaken the bones, slow healing, and increase the risk of infection. Malnourished patients may also be less resilient to the stress of surgery and recovery, further increasing their risk of mortality.
Key Points:
- Malnutrition leads to delayed wound healing and increases the risk of infections.
- A lack of essential nutrients like protein and calcium weakens the body’s ability to recover.
- Poor nutritional status is associated with higher rates of postoperative complications and mortality.
Mental Health and Cognitive Decline
Mental health and cognitive function play a significant role in the recovery process. Patients with cognitive impairments, such as dementia or Alzheimer’s disease, are at an increased risk of mortality following a femoral neck fracture. These patients often experience delirium after surgery, which can lead to confusion, agitation, and an inability to follow postoperative care instructions. Moreover, cognitive impairments can increase the likelihood of falls, both before and after surgery, further complicating the recovery process. Depression, common in elderly patients after a traumatic injury, can also negatively impact recovery, as it may lead to poor self-care, malnutrition, and a lack of motivation for rehabilitation.
Key Points:
- Cognitive decline increases the risk of postoperative delirium and poor recovery outcomes.
- Dementia and Alzheimer’s patients are more likely to experience complications after surgery.
- Depression and anxiety can lead to poor self-care, reducing the chances of successful recovery.
Delayed Medical Attention
In some cases, a femoral neck fracture may not be immediately diagnosed or treated, particularly if the fall occurs in elderly patients who live alone or in nursing homes. Delayed medical attention can lead to further complications, such as avascular necrosis (death of bone tissue due to lack of blood supply), infection, and increased immobility. This delay can exacerbate the condition and significantly increase the risk of death, particularly if medical intervention is postponed.
Key Points:
- Delayed treatment can worsen the severity of the fracture and lead to complications.
- Lack of immediate care increases the risk of avascular necrosis and infection.
- Early intervention is crucial for improving survival outcomes.
Source
- Advanced Age and Frailty: Elderly individuals, especially those over 80 years of age, are at a greater risk of death following a femoral neck fracture. Frailty significantly impairs recovery due to decreased physiological reserves and resilience, making it harder for these patients to survive surgery and the rehabilitation process(BioMed Central)(BioMed Central).
- Comorbidities: Older adults with multiple chronic conditions, such as cardiovascular disease, diabetes, and chronic obstructive pulmonary disease (COPD), are at a higher risk of mortality following a hip fracture. These conditions not only complicate surgical outcomes but also increase vulnerability to postoperative complications such as infections, delayed wound healing, and cardiovascular events(SpringerOpen).
- Surgical and Postoperative Complications: Surgery is generally required to treat femoral neck fractures, but it carries significant risks for elderly patients. Studies show that delays in surgery—particularly beyond 48 hours—can increase the likelihood of mortality. Additionally, patients with higher preoperative ASA (American Society of Anesthesiologists) scores, indicating poor overall health, are more likely to experience fatal complications(BioMed Central).
- Immobility and Hospitalization Risks: After surgery, patients often face prolonged periods of immobility, which can lead to complications like deep vein thrombosis (DVT), pneumonia, and pressure ulcers. Immobility also exacerbates muscle weakness and increases the risk of further falls and complications(SpringerLink).
- Nutritional Deficiencies: Malnutrition is a prevalent issue among elderly patients with hip fractures. Poor nutritional status, characterized by deficiencies in essential nutrients like protein, calcium, and vitamin D, impairs the body’s ability to heal and fend off infections, increasing the risk of death(BioMed Central).
- Mental Health and Cognitive Decline: Patients suffering from dementia or other cognitive impairments are at greater risk of mortality post-fracture. Cognitive impairments can complicate postoperative care, lead to delirium, and reduce compliance with rehabilitation efforts, thereby worsening outcomes(SpringerOpen).
Radiographic signs of femoral neck fracture
Femoral neck fractures are a critical type of hip fracture, often occurring in elderly individuals and those with underlying bone conditions like osteoporosis. Timely and accurate diagnosis is essential for determining the appropriate treatment plan and avoiding complications. Radiographic imaging is the primary tool used to diagnose femoral neck fractures, as it provides essential details about the fracture’s type, location, and severity. Understanding the key radiographic signs of femoral neck fractures is crucial for healthcare providers to ensure effective treatment and improved outcomes.
List of Radiographic signs of femoral neck fracture
Displacement of the Femoral Head
One of the most significant radiographic signs of a femoral neck fracture is the displacement of the femoral head. This occurs when the fracture causes a misalignment between the head of the femur (ball) and the neck of the femur (connecting portion). Displacement is graded using the Garden classification system, which helps predict the prognosis and guide treatment strategies.
- Garden I: An incomplete or minimally displaced fracture. This type may be difficult to detect, as the alignment of the femoral head and neck appears relatively normal on an X-ray.
- Garden II: A complete but non-displaced fracture. The femoral head remains in its normal position, and there is no visible separation between the bone fragments.
- Garden III: A complete fracture with partial displacement. The femoral head is slightly misaligned but still maintains some contact with the acetabulum (hip socket).
- Garden IV: A fully displaced fracture where the femoral head has completely lost contact with the acetabulum, often requiring surgical intervention for repair.
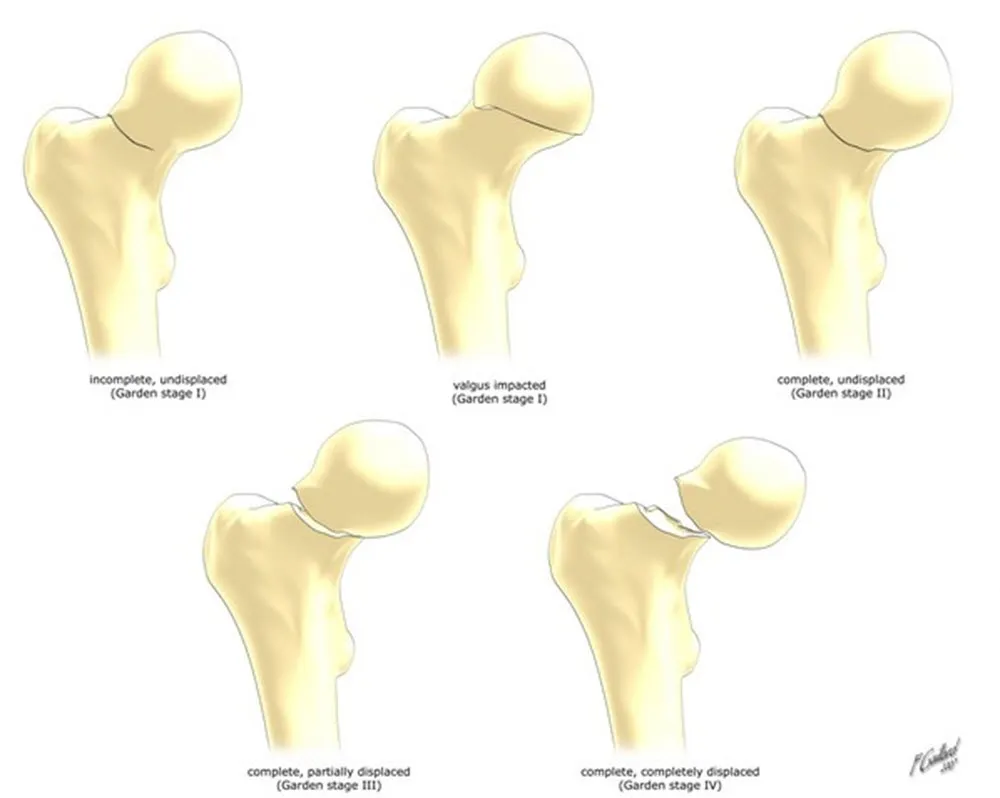
Top left (Garden stage I): Represents an incomplete, undisplaced fracture. The fracture line is subtle, and the bone remains largely intact.
Top middle (Garden stage I, valgus impacted): The fracture is still incomplete but shows a valgus (angled inward) impaction, where the bone is slightly compressed.
Top right (Garden stage II): A complete fracture, yet it remains undisplaced, meaning the bone fragments are still aligned properly.
Bottom left (Garden stage III): This stage shows a complete, partially displaced fracture, where the bone fragments have started to shift but remain in partial contact.
Bottom right (Garden stage IV): Represents a complete and fully displaced fracture, where the femoral head is entirely separated from the shaft.
This classification helps guide treatment decisions for hip fractures, which can range from conservative management to surgical intervention.
The degree of displacement visible on radiographic images is crucial in determining whether the fracture can heal with conservative management or if surgical intervention is necessary. Full displacement (Garden IV) usually requires surgical treatment, as the blood supply to the femoral head is at risk, which can lead to avascular necrosis.
Shortening and Rotation of the Femoral Neck
Radiographs of the hip often reveal shortening or rotation of the femoral neck in cases of femoral neck fractures. Shortening occurs when the femoral neck collapses or compresses due to the fracture, causing the leg to appear shorter on the affected side. Additionally, the femoral neck may rotate abnormally, which is evident in an altered alignment of the femur on an X-ray.
- Shortening: Visible on both anteroposterior (AP) and lateral radiographic views, shortening is an important sign of a displaced or unstable femoral neck fracture.
- Rotation: Internal or external rotation of the femoral neck can also be a critical sign, often visible on the AP view. In particular, external rotation is a typical finding in displaced fractures, where the femoral head moves outward from its normal position.
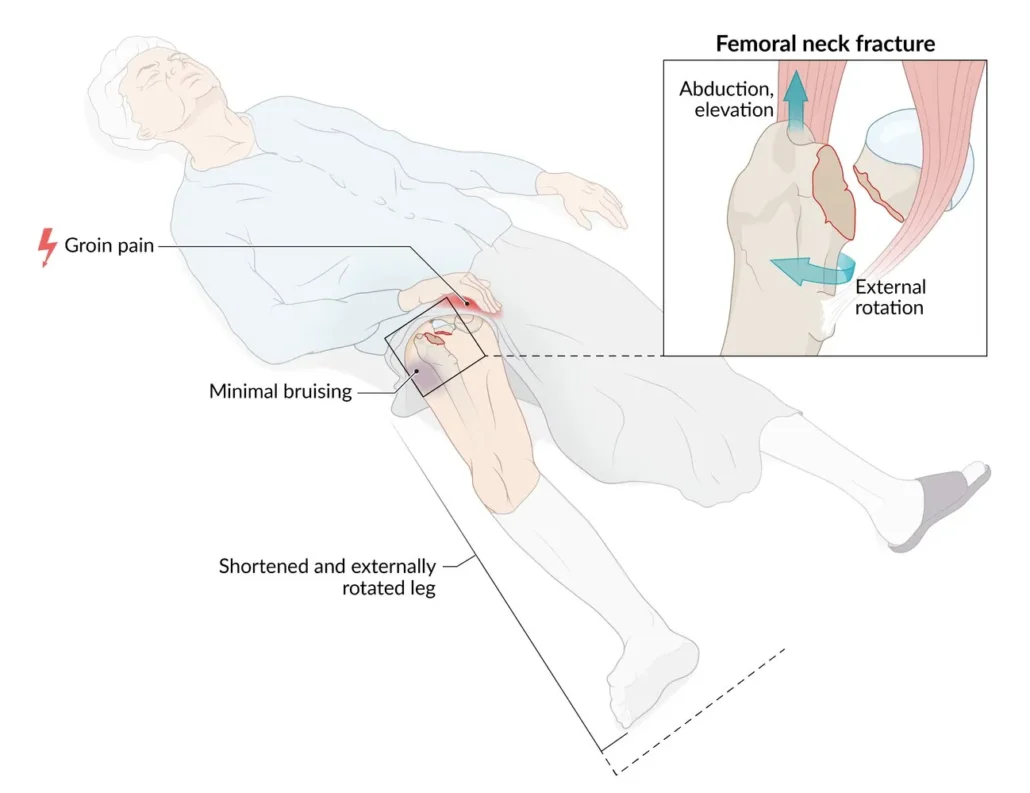
Key clinical indicators include:
Groin pain: The patient reports pain localized to the groin area, which is a hallmark symptom of a femoral neck fracture.
Minimal bruising: Despite the significant injury, external bruising can be minimal due to the deep location of the femur.
Shortened and externally rotated leg: The fractured limb typically appears shorter and rotated outward due to muscle contraction and displacement of the bone fragments.
The inset highlights the abduction, elevation, and external rotation of the affected hip, emphasizing the biomechanical changes caused by the fracture. Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 7823
Cortical Discontinuity
Another key radiographic sign of a femoral neck fracture is the disruption or discontinuity of the cortical bone. The cortex is the outer, dense layer of bone that is clearly visible on radiographic images. When a fracture occurs, the normally smooth and continuous cortical line of the femoral neck will appear broken or irregular.
- Anterior and Posterior Cortical Disruption: Cortical disruption may be more easily visualized in the anterior or posterior aspects of the femoral neck, depending on the angle of the X-ray. The fracture line often appears as a jagged or sharp break in the bone cortex, confirming the presence of a fracture.
In subtle or non-displaced fractures, cortical disruption may be difficult to detect, requiring additional imaging, such as a CT scan or MRI, to provide a clearer view of the fracture and associated soft tissue damage.
Trabecular Pattern Distortion
The trabeculae are the fine, spongy structures inside the bone that provide strength and support. In the femoral neck, the trabecular pattern is usually uniform and well-defined. A femoral neck fracture often causes distortion or disruption of the normal trabecular pattern, which can be visualized on radiographs.
- Loss of Normal Trabecular Alignment: A common radiographic sign of a fracture is the loss of the regular trabecular alignment within the femoral neck. This may present as areas of increased or decreased radiodensity (whiteness or darkness on the X-ray) around the fracture site.
- Compression or Collapse of Trabeculae: In cases of significant compression fractures, the trabeculae may appear crushed or compacted. This is often seen in Garden III and IV fractures, where there is substantial bone displacement.

In the normal femur, several trabecular groups are visible:
Primary compressive group: These trabeculae resist weight-bearing forces and are essential for maintaining the structural integrity of the bone.
Secondary compressive group: Provides additional support and reinforcement, though not as dominant as the primary group.
Primary tensile group: These trabeculae counteract tensile forces generated during movement.
Secondary tensile group: Provides supplementary tensile resistance, particularly in rotational movements.
Ward’s triangle: This is an area of relative paucity of trabeculae, but in normal bones, it is well-defined.
In the osteopenic femur, changes in trabecular architecture become evident:
Accentuated trabeculae: Loss of bone density makes some trabeculae more prominent, but overall, their number and connectivity decrease.
Enlarged and indistinct Ward’s triangle: The triangle becomes larger and less defined, a hallmark of weakened bone structure.
Trabecular thinning: There is a loss of connectivity, weakening the bone and increasing susceptibility to fractures.
These changes reflect the progressive deterioration of bone quality in osteopenia, which can lead to osteoporosis and increase the risk of fractures, especially in weight-bearing bones like the femur.
Lucent Fracture Line
The most straightforward sign of a femoral neck fracture on a radiograph is the presence of a visible fracture line. This appears as a radiolucent (dark) line that cuts across the femoral neck, indicating where the bone has broken. The visibility of the fracture line depends on the degree of displacement, the type of fracture, and the quality of the radiographic image.
- In Non-Displaced Fractures: The fracture line may be faint and difficult to identify, especially in early or incomplete fractures. In these cases, supplementary imaging may be necessary to confirm the diagnosis.
- In Displaced Fractures: The fracture line is usually more prominent, with a clear separation between bone fragments. This is most often seen in Garden III and IV fractures.
Femoral Head Angulation
Radiographic images may also show abnormal angulation of the femoral head relative to the femoral neck. This occurs when the head of the femur tilts or shifts due to the fracture. The angle between the femoral head and neck can provide important information about the severity of the fracture and its potential impact on hip stability and function.
- Coxa Vara Deformity: A common finding in displaced femoral neck fractures is coxa vara, where the angle between the femoral head and neck decreases, leading to an inward tilt of the femoral shaft. This deformity is often associated with poor outcomes and may require surgical correction.

On the left side (labeled as “L”), there is notable irregularity and deformity of the femoral head and neck, which may indicate a femoral neck fracture, common in elderly patients, particularly those with weakened bone structure, such as osteopenia or osteoporosis. The right femur appears to be intact, though further analysis is required for a comprehensive assessment.
The radiograph also shows the lumbar spine, where the alignment of the vertebrae can be observed. There are no immediate signs of dislocation, but any subtle fractures or degenerative changes would need to be closely evaluated.
This type of pelvic X-ray is commonly used to diagnose hip fractures, dislocations, and degenerative bone conditions, and it is critical for planning orthopedic interventions like hip replacement or fixation. Authorization Dr Benoudina Samir, Radiopaedia.org, rID: 47665

The X-ray shows a displaced or partially displaced fracture, which often results in a shortened and externally rotated leg due to muscle pull. The pelvic bones, including the ilium and acetabulum, are also visible, with the right hip appearing aligned and intact.
Femoral neck fractures are typically treated surgically, with options ranging from internal fixation (pins or plates) to hip replacement, depending on the fracture’s severity and the patient’s overall health. The involvement of this critical area raises concerns about potential complications, such as avascular necrosis of the femoral head, making timely intervention essential.
Attribution: Dr. Benoudina Samir, Radiopaedia.org, rID: 22392.


In this lateral view, the fracture is visible with some degree of displacement, which may cause shortening and external rotation of the leg clinically. Subcapital fractures can disrupt blood supply to the femoral head, increasing the risk of avascular necrosis (bone death due to lack of blood flow) if not treated promptly.
Management typically involves surgical intervention, such as internal fixation with screws or a partial or total hip replacement, depending on the patient’s age, health, and fracture severity. Prompt diagnosis and treatment are crucial to restore function and prevent complications.Authorization Assoc Prof Frank Gaillard, Radiopaedia.org, rID: 7952
Varus and Valgus Deformities
Varus and valgus deformities refer to the abnormal inward (varus) or outward (valgus) angulation of the femoral head relative to the shaft. These deformities are best identified on anteroposterior (AP) radiographs.
- Varus Deformity: This occurs when the angle between the femoral neck and the shaft of the femur is reduced, causing the femoral head to tilt inward. Varus deformities are associated with displaced fractures and often indicate poor prognosis, especially when significant displacement occurs.
- Valgus Deformity: Less common than varus deformity, valgus deformity presents as an increased angle between the femoral head and neck, causing an outward tilt of the head. While this type of deformity can also result from femoral neck fractures, it tends to have a better prognosis than varus deformities.
Sclerosis Around the Fracture Site
Sclerosis refers to the hardening or thickening of bone, which appears as an area of increased radiodensity (whiteness) on radiographs. In femoral neck fractures, sclerosis often develops around the fracture site as a natural reaction to the injury. This thickening of the bone can indicate an attempt by the body to stabilize the fracture, but it may also reflect healing in more chronic cases.
- Reactive Sclerosis: This is typically seen in non-displaced or minimally displaced fractures. The body attempts to repair the injury by thickening the bone around the fracture line. However, excessive sclerosis can sometimes indicate poor healing or delayed union.
- Subchondral Sclerosis: In cases where the fracture involves the subchondral bone (the bone just beneath the cartilage), sclerosis may develop in the femoral head or acetabulum. Subchondral sclerosis is a potential sign of ongoing stress at the joint due to malalignment or inadequate fracture healing.
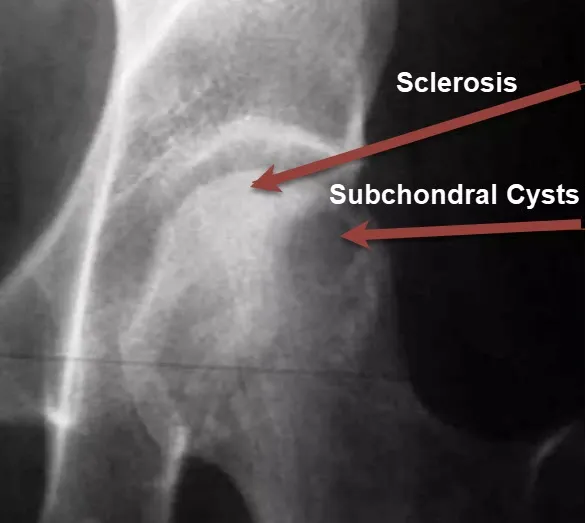
Subchondral cysts are also visible, which can occur as part of the healing process following a fracture. These cysts are small, fluid-filled sacs that form within the bone, often due to stress and microtrauma in the affected area.
The sclerosis and cyst formation are common signs that the bone is trying to heal itself after the injury. The increased density and hardening suggest that the body is laying down new bone in an attempt to stabilize the fractured area and adapt to the mechanical stress caused by the fracture. This reaction is typical in response to chronic or severe injuries.
Increased Femoral Neck-Shaft Angle
In some cases, radiographs may show an abnormal increase in the neck-shaft angle, leading to valgus displacement of the femoral head. This condition is more commonly seen in non-displaced or incomplete fractures and is typically observed in younger patients or those with relatively strong bone density.
- Increased Neck-Shaft Angle: A neck-shaft angle greater than 135 degrees indicates valgus displacement, which often presents in minimally displaced fractures. Though it is less common, this sign can be important in assessing the overall alignment of the femoral head and neck.
Bone Fragmentation
Bone fragmentation is an indication of a comminuted fracture, in which the bone has broken into several small pieces. Comminuted fractures are generally more severe and carry a higher risk of complications, including nonunion and avascular necrosis (bone death). Radiographs will show multiple bone fragments around the fracture site, and the number and size of these fragments can give insights into the severity of the injury.
- Multiple Bone Fragments: When there are more than two fragments visible on radiographs, the fracture is classified as comminuted. This can occur in both intra- and extracapsular fractures, with comminuted femoral neck fractures being particularly challenging to manage.
Signs of Avascular Necrosis
Avascular necrosis (AVN) is one of the most feared complications of femoral neck fractures, as it results from interrupted blood flow to the femoral head. Early signs of AVN may not always be visible on initial radiographs, but certain changes can be seen in follow-up imaging.
- Crescent Sign: This is a subtle radiographic sign that may indicate early-stage AVN. It appears as a subchondral radiolucent line, typically found near the weight-bearing surface of the femoral head. This crescent-shaped line represents bone collapse just beneath the cartilage, suggesting loss of blood supply.
- Flattening of the Femoral Head: As AVN progresses, radiographs may show flattening or collapse of the femoral head, which appears as a loss of the spherical contour of the femoral head. This sign is usually accompanied by progressive joint space narrowing, indicating advanced AVN.
Lipohemarthrosis
Lipohemarthrosis is the presence of fat and blood in the joint space, and it is a radiographic sign suggestive of intra-articular fractures. Though more commonly associated with fractures of the knee, lipohemarthrosis can also be seen in femoral neck fractures, especially if the fracture extends into the joint capsule.
- Fat-Fluid Level: On radiographs, lipohemarthrosis can be visualized as a fat-fluid level within the joint space, typically seen on cross-table lateral views. This finding indicates that both fat and blood from the fracture site have leaked into the joint space, often a sign of a more severe fracture.
Double Line Sign on MRI
While plain radiographs are the initial diagnostic tool, MRI may be used when radiographs do not provide a definitive diagnosis, especially in occult or subtle fractures. One of the most telling signs of a femoral neck fracture on MRI is the “double line sign.”
- Double Line Sign: This sign appears as two parallel lines in the femoral head on T2-weighted MRI images. It indicates a fracture with associated bone edema and is a sensitive marker for identifying femoral neck fractures that may not be visible on X-rays.
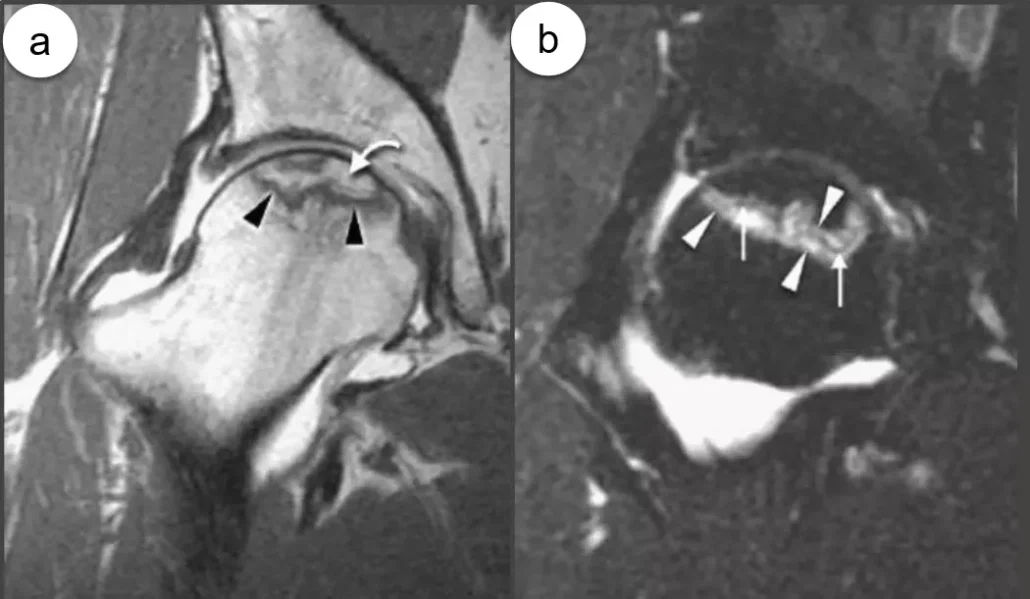
The inner dark line corresponds to the boundary of dead bone (necrosis), while the outer bright line signifies active granulation tissue forming around the necrotic area.
In image (a), on the T1-weighted MRI, a serpiginous low-signal line encircles an area of fatty marrow, indicating the necrotic region within the femoral head.
This double line sign is a critical diagnostic feature in AVN, where the blood supply to the bone is disrupted, leading to bone death and potentially collapse of the femoral head. Early detection with MRI is essential for managing AVN before significant joint damage occurs.
Periosteal Reaction
A periosteal reaction occurs when the bone’s outer layer, or periosteum, reacts to a fracture by forming new bone. This reaction may appear as new bone formation around the fracture site on radiographs and can indicate an ongoing healing process.
Visible Periosteal Reaction: In cases of chronic or healing femoral neck fractures, a periosteal reaction may be visible as a thin, dense line of new bone formation adjacent to the fracture site. This is more common in fractures that have been present for an extended period before treatment.
Quizz
Questionnaire 1
- What is the main cause of hip fracture in older people?
- A) Arthrose
- B) Chutes
- C) Osteoporosis
- D) Hip dislocation
- E) Vitamin D deficiency
- What is the impact of hip fracture on the mobility of older people?
- A) Improved mobility
- B) No impact
- C) Drastic reduction of independence
- D) Increased muscle strength
- E) Stabilization of balance
- What factor contributes to bone fragility and increases the risk of fractures?
- A) Regular exercise
- B) Muscle weakness
- C) Balanced diet
- D) Youth
- E) Adequate hydration
- What complication is associated with intracapsular fractures, particularly those of the femoral neck?
- A) Infection
- B) Arthrose
- C) Avascular necrosis of the femoral head
- D) Deep vein thrombosis
- E) Cognitive impairment
- What is the classification of hip fracture according to Delbet?
- A) Type A – Fracture cervicale
- B) Type B – Fracture trochantérienne
- C) Type C – Subtrochanteric fracture
- D) Type D – Diaphyseal fracture
- E) Type E – Epiphyseal fracture
- What is one of the symptoms of hip fracture in older adults?
- A) Hip burn
- B) Numbness of the feet
- C) Increased flexibility
- D) Normal leg rotation
- E) Inability to bear weight on the affected leg
- What is one factor that contributes to the high risk of death after a femoral neck fracture?
- A) Youth
- B) Delay in surgery
- C) Muscle weakness
- D) Early treatment
- E) Weight loss
- What is the complication that can result from a release of fat particles into the bloodstream after a severe hip fracture?
- A) Pulmonary embolism
- B) High blood pressure
- C) Diabetes
- D) Renal failure
- E) Visual impairment
- What is the main radiographic feature looked for to diagnose a femoral neck fracture?
- A) Bloodshed
- B) Angular displacement
- C) Interrupted fracture line
- D) Signs of osteoarthritis
- E) Cognitive impairment
- What factor is not mentioned as contributing to hip fracture risk?
- A) Sedentary lifestyle
- B) Cognitive impairment
- C) Non-slip mats
- D) High muscle strength
- E) Degraded vision
Answers to multiple choice questions:
- What is the main cause of hip fracture in older people?
- Answer: C) Osteoporosis
- What is the impact of hip fracture on the mobility of older people?
- Answer: C) Drastic reduction in independence
- What factor contributes to bone fragility and increases the risk of fractures?
- Answer: B) Muscle weakness
- What complication is associated with intracapsular fractures, particularly those of the femoral neck?
- Answer: C) Avascular necrosis of the femoral head
- What is the classification of hip fracture according to Delbet?
- Answer: A) Type A – Cervical fracture
- What is one of the symptoms of hip fracture in older adults?
- Answer: E) Inability to bear weight on the affected leg
- What is one factor that contributes to the high risk of death after a femoral neck fracture?
- Answer: B) Delay in surgery
- What is the complication that can result from a release of fat particles into the bloodstream after a severe hip fracture?
- Answer: A) Pulmonary embolism
- What is the main radiographic feature looked for to diagnose a femoral neck fracture?
- Answer: C) Interrupted fracture line
- What factor is not mentioned as contributing to hip fracture risk?
- Answer: D) High muscular strength
Conclusion
Hip fractures in the elderly present a formidable challenge, profoundly affecting the health, mobility, and quality of life of those affected. These fractures, commonly resulting from falls due to age-related factors such as decreased bone density and muscle weakness, necessitate a comprehensive approach to management. The importance of effective prevention strategies cannot be overstated, as they play a crucial role in mitigating the risk of such fractures. By improving home safety, enhancing muscle strength, and addressing factors that compromise balance, the incidence of falls and subsequent hip fractures can be significantly reduced.
The multidisciplinary treatment of hip fractures, which often involves surgical intervention and a thorough rehabilitation process, underscores the complexity of managing these injuries in older adults. The impact of hip fractures extends beyond the physical injury, encompassing emotional and psychological challenges that necessitate supportive care and psychological assistance.
Understanding the classification, complications, and diagnostic approaches associated with hip fractures is essential for providing optimal care. The historical Delbet classification, while valuable, has been largely supplanted by modern methods that offer a more nuanced understanding of fracture types and treatment strategies. Prompt and effective treatment, coupled with diligent postoperative care, is critical in minimizing complications and promoting recovery.
Ultimately, addressing the multifaceted issues surrounding hip fractures in the elderly requires a proactive and holistic approach. By focusing on prevention, timely medical intervention, and comprehensive care, it is possible to improve outcomes and enhance the overall well-being of affected individuals.
Reference
- Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010 Sep;21(5):658-68. [PubMed]
- Parker M, Johansen A. Hip fracture. BMJ. 2006 Jul 01;333(7557):27-30. [PMC free article] [PubMed]
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporosis Int. 1997;7(5):407-13. [ PubMed ]
- Dhanwal DK, Dennison EM, Harvey NC, Cooper C. Epidemiology of hip fracture: Worldwide geographic variation. Indian J Orthop. 2011 Jan;45(1):15-22. [PMC free article] [PubMed]
- Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009 Oct 14;302(14):1573-9. [PMC free article] [PubMed
- Youm T, Koval KJ, Zuckerman JD. The economic impact of geriatric hip fractures. Am J Orthop (Belle Mead NJ). 1999 Jul;28(7):423-8. [PubMed]
- Mosk CA, Mus M, Vroemen JP, van der Ploeg T, Vos DI, Elmans LH, van der Laan L. Dementia and delirium, the outcomes in elderly hip fracture patients. Clin Interv Aging. 2017;12:421-430. [PMC free article] [PubMed]
- Deleanu B, Prejbeanu R, Tsiridis E, Vermesan D, Crisan D, Haragus H, Predescu V, Birsasteanu F. Occult fractures of the proximal femur: imaging diagnosis and management of 82 cases in a regional trauma center. World J Emerg Surg. 2015;10:55. [PMC free article] [PubMed]
- Foex BA, Russell A. BET 2: CT versus MRI for occult hip fractures. Emerg Med J. 2018 Oct;35(10):645-647. [PubMed]
- Bartonícek J. Pauwels’ classification of femoral neck fractures: correct interpretation of the original. J Orthop Trauma. 2001 Jun-Jul;15(5):358-60. [PubMed]
- van Embden D, Roukema GR, Rhemrev SJ, Genelin F, Meylaerts SA. The Pauwels classification for intracapsular hip fractures: is it reliable? Injury. 2011 Nov;42(11):1238-40. [PubMed]
- Kazley JM, Banerjee S, Abousayed MM, Rosenbaum AJ. Classifications in Brief: Garden Classification of Femoral Neck Fractures. Clin Orthop Relat Res. 2018 Feb;476(2):441-445. [PMC free article] [PubMed]
- Credit in part:Benjamin R. Emmerson; Matthew Varacallo; Dominic Inman.


















{kind=link}