

Introduction: Typical runner’s pain
Iliotibial band syndrome (or windshield wiper syndrome) is one of the most common causes of lateral knee pain, particularly among long-distance runners, cyclists, and hikers. It is insidious, often beginning as a diffuse discomfort before developing into sharp, debilitating pain. It is sometimes misunderstood, confused with other knee pathologies, and can be difficult to treat without a comprehensive, individualized approach.
This syndrome highlights a frequent paradox in musculoskeletal pathology: it is not the most obvious structure that suffers, but the one that compensates , that absorbs imbalances in posture, gestures or terrain. This is where osteopathy offers a valuable reading, by placing this pain in a broader biomechanical, functional and even emotional context .
What is iliotibial band syndrome?
The iliotibial band, also called the iliotibial tract or fascia lata, is a fibrous structure stretched between the iliac crest (at the pelvis) and the tibia, via the external lateral condyle. It is reinforced by the muscular insertions of the tensor fascia latae (TFL) and the gluteus maximus, two key muscles in locomotion and postural control.
Its main function is to stabilize the knee laterally when walking, running or jumping . It acts as a strap that limits excessive lateral movements, especially during the stance phase.
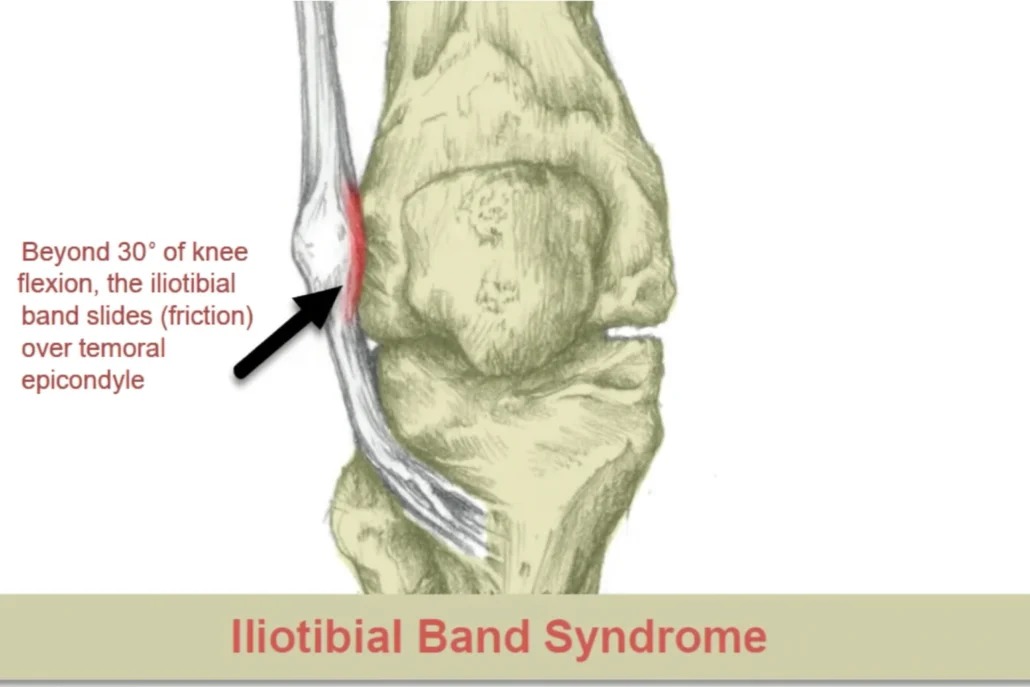
In the syndrome, the band repeatedly rubs on the lateral condyle of the femur during knee flexion/extension, causing local soft tissue inflammation and pinpoint pain, often described as burning or stinging on the outer side of the knee , aggravated by exertion.
Unlike classic tendinitis, this is a friction conflict rather than simple muscular overuse . But as is often the case with functional pathologies, this friction is the result of a more global imbalance : hip dysfunction, poor femoral rotation, collapse of the plantar arch, weakness of the pelvic stabilizers, etc.
Why does it particularly affect athletes?
Iliotibial band syndrome is emblematic of what are called overuse syndromes , common among regular athletes or overly enthusiastic beginners. The repetition of movements – typical of running – exposes this anatomical structure to cumulative mechanical stress, particularly when running downhill, where the gluteal muscles and the TFL work more eccentrically to stabilize the knee.
Several factors promote this syndrome in athletes:
- Too rapid an increase in training intensity or volume , without progressive adaptation.
- Inclined or uneven terrain , such as slopes or inclines, which accentuate pelvic tilt and dynamic knee valgus.
- Poor biomechanical alignment , often ignored: foot collapse, internal rotation of the femur, pelvic asymmetry.
- Improper or worn footwear , altering the way forces are absorbed by the lower kinetic chain.
- Muscle fatigue : Deep stabilizing muscles (especially the gluteus medius) can lose effectiveness over the kilometers, leaving the band to compensate excessively.
This syndrome is therefore often the symptom of a series of poorly integrated compensations in the sporting movement. What makes it so particular in athletes is that it is not caused by trauma, but by a silent accumulation of micro-imbalances.
In osteopathy, this dynamic and systemic reading is essential: it is not just a question of relaxing the band, but of understanding why it is working too much , what it is trying to compensate for, and how to reintegrate its action into a more harmonious body schema.
Roles and Functions of the Iliotibial Band
Functional Anatomy of the Iliotibial Band
The iliotibial band is much more than just a lateral tendon. It plays a vital role in lower limb dynamics, connecting the actions of the pelvis, hip, knee, and even the foot. To fully understand its role in lateral knee pain, it is crucial to explore its structure, muscle interactions, and biomechanical functions.
Origin and path of the strip
The iliotibial band, or iliotibial tract, is a lateral thickening of the fascia lata , a fibrous covering that covers the thigh muscles. It originates at the iliac crest, where it is influenced by two key muscles:
- The gluteus maximus , which is partially inserted into the band and transmits its power to it,
- The tensor fascia latae (TFL) , a small muscle located on the anterolateral aspect of the hip, which participates in locking the knee in extension.
The strip then runs down the lateral side of the thigh and inserts onto the lateral condyle of the tibia, at the level of Gerdy’s tubercle. This longitudinal path positions it ideally to stabilize the knee laterally during dynamic activities.
It is also in contact with the knee joint capsule, the lateral collateral ligament, and the underlying bursa, which explains its sensitivity to frictional conflicts .
Its role in knee and hip stability
The primary function of the iliotibial band is to maintain lateral stability of the knee during locomotion, particularly during the single-leg stance phase of walking or running. When one foot is on the ground, the entire body weight rests on one leg, and the band acts as a natural stay that prevents the knee from collapsing into varus or valgus.
It also plays a postural role at the hip. In coordination with the TFL and the gluteal muscles, it contributes to:
- Limit excessive thigh adduction movements ,
- Check internal rotation of the femur , which is common in cases of weakness of the gluteus medius,
- Maintain constant tension on the lateral compartment of the knee , essential in propulsion movements.
In other words, the band is a biomechanical interface between the upper and lower body. It responds to the stabilization demands imposed by movement, but it is also vulnerable to any disruption of the overall motor pattern.
Tensions, asymmetries and compensation
When posture is altered—for example, by pelvic tilt, leg length discrepancy, or trunk instability—the iliotibial band may become under constant tension . This makes it more prone to friction on bony structures, particularly the lateral condyle of the femur.
In runners, insufficient medial foot support or weakness of the lateral hip rotators (such as the gluteus medius) promote excessive internal rotation of the femur . This deviant biomechanics increases stress on the band.
From an osteopathic point of view, we observe that the band is rarely the only cause . It is part of a chain system, where muscular hypertonia, tense fascia, joint fixations (sacroiliac, knee, talus) and the respiratory pattern can contribute to the problem.
In addition to its role at the knee, the iliotibial band contributes significantly to the stabilization of the hip joint. It helps control hip abduction, i.e., the movement of the thigh away from the body. This role in hip stabilization is fundamental for maintaining balance and coordination during various physical activities.
- Knee Stabilization: When the knee flexes and extends during walking or other movements, the iliotibial band helps stabilize the knee by acting like a tendon. It helps maintain proper knee alignment and prevent excessive movement.
- Hip Extension Assistance: The iliotibial band plays a role in hip extension, which is important in activities such as walking, running, and stair climbing. It acts as an extension of the fascia lata, which is a larger connective tissue covering the thigh muscles.
- Friction Reduction: The iliotibial band can act as a friction-reducing mechanism between nearby muscles and bony structures, particularly at the knee. It slides over the lateral portion of the femur, reducing friction during movement.
- Pelvic Stability Support: By helping stabilize the knee and aiding in hip extension, the iliotibial band can also influence pelvic stability during walking and other activities.
The Mystery of Elastic Function: Key Studies by Carolyn Eng
Research by Carolyn Eng and colleagues sheds light on the intriguing mystery of the iliotibial band (ITB) fascia and its role in human locomotion. The ITB, a large piece of elastic connective tissue that runs along the outer thigh, has long been associated with injury and pain in many people. However, Eng’s studies challenge the conventional wisdom that the IT fascia functions primarily to stabilize the hip during walking. Instead, they suggest that the IT fascia acts as an elastic structure that stores and releases energy to improve walking and running efficiency.
Research has revealed that in humans, the iliotibial band fascia has a remarkable capacity to store 15 to 20 times more elastic energy per body mass than its less developed structure in chimpanzees. This increased energy storage capacity is particularly pronounced during running, a more bouncy gait compared to walking. The researchers suggest that the role of the IT fascia in locomotion, particularly running, may involve recycling stored elastic energy, thereby contributing to energy savings during movement.
Carolyn Eng and her colleagues have conducted extensive research on the iliotibial band (ITB) and its role in human locomotion. Their studies suggest that the ITB acts as an elastic structure that stores and releases energy to improve walking and running efficiency, challenging the conventional wisdom that it primarily serves to stabilize the hip.
One of the key articles on this topic is titled “ The human iliotibial band is specialized for elastic energy storage compared with the chimp fascia lata“, published in 2015 in the Journal of Experimental Biology . In this study, Eng and colleagues compared the ability of the human ITB to store elastic energy versus the chimpanzee fascia lata, demonstrating that the human ITB is specialized for elastic energy storage, which contributes to the economy of bipedal locomotion.
Another relevant article is “ The capacity of the human iliotibial band to store elastic energy during running“, published in 2015 in the Journal of Biomechanics . This study evaluated the ability of the ITB to store and release elastic energy during running, using a musculoskeletal model to estimate ITB forces and deformations during running at different speeds.
For a more accessible presentation of this research, the article ” Understanding the IT band » published by the Harvard Gazette in 2015 provides a summary of Carolyn Eng’s findings on the function of the ITB in human locomotion.
These studies provide valuable insights into the function of the iliotibial band, highlighting its critical role in improving the energy efficiency of walking and running in humans.

Unlike traditional perspectives that focus on the role of this fascia in stabilizing the hip during walking, the researchers approached their study from an evolutionary perspective. They compared this fascia in humans to its counterpart in chimpanzees, emphasizing the importance of considering adaptations for both walking and running in human evolution.
To understand the function of the IT fascia, the researchers developed a computational model to estimate its stretch and energy storage during walking and running. The model was based on measurements obtained by manipulating cadaveric limbs through various movements. The findings have implications for both basic science and clinical studies, potentially influencing athletic training programs and gait rehabilitation.
In the future, the researchers plan to expand their investigation to include other primate species adapted to running. Additionally, they plan to explore how a better understanding of the IT fascia could help prevent or treat injuries, particularly IT fascia syndrome, a common overuse injury among runners and cyclists. Using the computer models developed in this study, the researchers aim to estimate the force transmitted through the IT fascia in individuals with and without IT fascia pain, thereby providing a scientific basis for treating athletes with such injuries.
To uncover the role of the iliotibial (IT) band in human movement, researchers, led by Carolyn Eng, developed a sophisticated computer model to estimate how much the IT band stretches during walking and running — and consequently, how much energy it stores. The findings revealed that one section of the IT band stretches as the leg swings backward, storing elastic energy, which is then released as the leg moves forward, potentially reducing the energy cost of locomotion.
“It’s like recycling energy,” Eng explained. “Using these passive rubber bands instead of relying entirely on muscle activity makes movement more economical. The IT band stands out among human anatomical features as a potential key to improving the efficiency of running and even walking.”
Building the model was no simple task, as detailed descriptions of the IT band’s connections to muscles and bones were limited. To address this, Eng and her team turned to cadaver studies. Using a custom-built frame, they manipulated the hip and knee joints of five human and five chimpanzee cadaver limbs, measuring the changes in IT band length relative to joint angles.
These measurements helped calculate the IT band’s moment arm — the position relative to the hip and knee joints — which determines how much the IT band stretches and the torque it transmits during locomotion. The data provided insights into the IT band’s role in elastic energy storage, contributing to a more economical stride, and underscoring its importance as an adaptation for bipedal locomotion.
Credit: Carolyn Eng
Reference: The studies, co-authored with Daniel Lieberman, Edwin M. Lerner II Professor of Biological Sciences and chair of the Department of Human Evolutionary Biology; Andrew Biewener, Charles P. Lyman Professor of Biology; and Allison Arnold-Rife, a research associate in Biewener’s lab, are described in new articles in the Journal of Experimental Biology and the Journal of Biomechanics.
Pathophysiology: When the Iliotibial Band Goes Out of Adjustment
The pathophysiology of the iliotibial band (ITB) is crucial for understanding disorders related to this anatomical structure. The iliotibial band is a thick band of connective tissue stretched along the outer side of the thigh, extending from the iliac bone to the outer side of the tibia, thus crossing the knee joint. Its primary role is to stabilize the knee during movement, particularly during flexion and extension. However, disorders can occur when the ITB is subjected to excessive stress or repeated friction.
One of the common pathologies associated with the iliotibial band is iliotibial band syndrome, also known as windshield wiper syndrome. This syndrome typically occurs in runners and athletes involved in activities with repetitive knee movements. The pathophysiology of this syndrome often involves inflammation of the ITB as a result of excessive friction on the lateral condyle of the femur, causing considerable pain and discomfort.
The inflammatory process can be triggered by a combination of factors, including overuse, biomechanical abnormalities, improper footwear, or muscle weakness in the pelvic and thigh region. When the iliotibial band repeatedly rubs against the femoral condyle, microtrauma can occur, leading to a local inflammatory response. This inflammation can cause thickening of the iliotibial band, thereby worsening friction and pain.
An important aspect of the pathophysiology of iliotibial band syndrome is excessive tension on the band itself. Biomechanical changes, such as excessive knee rotation or foot pronation, can increase tension on the ITB. These factors contribute to repeated compression of the band against the femur, thus exacerbating the symptoms of the syndrome.
- Repetitive friction: ITBS is often associated with repetitive knee movements, such as running or cycling. During these activities, the iliotibial band, a thick tendon located on the side of the thigh, can experience repeated friction against the lateral condyle of the femur.
- Compression and Friction: When the knee flexes and extends, the iliotibial band passes over the lateral condyle of the femur. Due to the anatomy of this region, the iliotibial band can be compressed against the bone, causing excessive friction.
- Inflammation and irritation: Repeated friction can lead to irritation of the iliotibial band and surrounding tissues. This initial irritation can trigger an inflammatory response.
- Thickening of the iliotibial band: In response to inflammation, the iliotibial band may thicken, increasing friction during knee movements.
- Compression syndrome: Irritation and thickening of the iliotibial band can lead to true compression syndrome, causing lateral knee pain. This pain may be felt during physical activity, particularly when flexing and extending the knee.
Causes and Predisposing Factors
Iliotibial band syndrome does not appear by chance. It is the result of a set of biomechanical, postural, environmental and behavioral factors which, when put together, gradually overload a normally resistant structure . For the osteopath, identifying these causes is not a simple classification exercise, but an essential key to personalizing treatment and avoiding relapses .
Mechanical overload and repetitive movements
This is the most obvious and common cause. Athletes—especially runners, cyclists, and hikers—use the band tens of thousands of times per session. During each knee flexion/extension, it slides over the lateral femoral condyle. Over the long term, this back-and-forth motion creates frictional conflict , particularly around 30 degrees of flexion.
The higher the cadence, the more the friction surface is stressed. This friction can cause:
- Inflammation of the underlying bursa,
- Irritation of the fascia,
- Reflex hypertonia of the muscles involved (TFL, gluteus maximus).
The problem is therefore not the race itself, but often an excessive load that has been poorly anticipated : training that is too intense, returning to work after injury without adaptation, or poor recovery management.
Postural imbalances and muscle weakness
Another major factor is muscular imbalance , particularly in the pelvis and hip stabilizing muscles:
- The gluteus medius , often underactive, allows the pelvis to sag laterally, which increases the tension on the band.
- The poorly coordinated gluteus maximus transfers unregulated force to the iliotibial tract.
- The TFL , over-stressed, becomes hypertonic and maintains continuous traction.
Added to this is sometimes poor proprioception , a motor pattern disorder, or a postural adaptation secondary to an old sprain, chronic lower back pain or asymmetry of the lower limb.
In osteopathy, these imbalances often manifest as sacroiliac fixations, dysfunctions of the thoracolumbar hinge, or a loss of mobility of the coxofemoral joint.
Influence of terrain and shoes
The ground on which the activity takes place plays an underestimated role. Running on:
- sloping ground requires asymmetrical work between the legs (the one upstream works more in adduction),
- a hard surface , such as asphalt, increases the impact with each stride,
- inclined surfaces (banked roads) alter the biomechanics of the pelvis and knee.
In addition, worn or unsuitable shoes (too flexible, too rigid or without correction of a pronated foot) can accentuate internal rotation of the knee or collapse of the plantar arch, two elements which indirectly pull on the band.
Running technique and cadence
Too long a stride, excessive heel strike or too low a cadence (less than 160 steps/minute) increases ground contact time and knee flexion, exposing the band to friction for longer . More experienced athletes naturally adjust their cadence and posture, but beginners often adopt ineffective patterns that prove harmful in the medium term.
The osteopath, if he works with sports patients, can integrate into his clinical reasoning:
- analysis of the sporting gesture,
- dynamic posture,
- compensation chains throughout the lower limb.
Other aggravating factors
- Poor hydration and nutrition , affecting the quality of fascial tissues.
- Chronic stress , which can promote muscle hypertonia via constant activation of the sympathetic nervous system.
- Joint hypermobility , where passive stabilization structures such as the band take over from the muscles.

Symptoms: What to Recognize and Watch For
Clinical Symptoms and Diagnosis
Iliotibial band syndrome presents in a fairly characteristic way, which often makes it easy to spot. However, to avoid confusion with other knee pathologies, a rigorous and differentiated clinical assessment is essential . In osteopathy, the diagnosis is broadened to include overall body dynamics, which allows for effective treatment guidance.
External knee pain: a telltale sign
The main symptom is pain located on the outer side of the knee , often described as:
- Burning, sharp or acute ,
- Occurring during or after exercise, particularly when going downhill or running for long periods ,
- Exacerbated at 30° knee flexion , where the band rubs the most on the femoral condyle.
In some patients, the pain stops abruptly when the activity stops , while in others it persists for several days. It may also radiate slightly to the thigh or shin , without crossing the midline of the knee.
Note: no swelling or joint instability is generally present – which already allows it to be differentiated from other intra-articular pathologies.
Specific functional tests
Several clinical tests are used to confirm the diagnosis:
- Noble test : In the supine position, the therapist applies pressure to the lateral femoral condyle during knee flexion-extension. Pain at 30° of flexion is suggestive of the syndrome.
- Reindeer test : when supporting one leg on the painful leg, pain reproduced at the lateral level of the knee indicates overloading of the band.
- Tender palpation of the iliotibial tract : Palpation often reveals a tense and painful fibrous cord , sometimes associated with tenderness of the TFL.
In osteopathy, the examination will be completed by a global assessment of posture, walking, lumbopelvic mobility and plantar statics .
Differential diagnosis: what to rule out
Despite the clinical clarity of the syndrome, other pathologies can mimic its symptoms:
- Biceps femoris tendinopathy (more posterolateral pain),
- Patellofemoral syndrome (pain more anteriorly, around the kneecap),
- External meniscal injury (locking or catching of the knee),
- Neuropathy of the lateral femoral cutaneous nerve (diffuse lateral paresthesias),
- Projected lumbar injury , particularly L5, which can cause radiating pain.
An imaging assessment is rarely necessary but may be requested to rule out intra-articular pathology or in the event of treatment failure.
Osteopathy and global diagnosis
The osteopath does not just make a localized diagnosis. He will look for:
- Sacroiliac hypomobility which increases the tension on the TFL,
- An asymmetrical motor pattern anchored from an old sprain,
- A rising chain linked to foot instability or pelvic tilt,
- Generalized hypertonia , sometimes triggered by chronic stress.
It is this systemic reading of the symptom which allows lasting effectiveness in osteopathic treatment.
List of symptoms
Recommendations: Managing and Preventing SBIT
- Rest and Ice: Give your body time to recover by avoiding activities that exacerbate pain. Apply ice to the affected area to reduce inflammation.
- Stretching: Regular stretching can help relieve tension in the iliotibial band. Stretching the fascia lata and surrounding muscles can be particularly helpful.
- Muscle Strengthening: Strengthening the core muscles (abdominals, pelvic muscles) and hip muscles can help stabilize the area and reduce stress on the iliotibial band.
- Change of Activity: If pain persists despite conservative measures, consider reducing the intensity or frequency of your exercise activities.
- Proper Equipment: Make sure you have appropriate, fitted footwear for your activity, as poor support can contribute to the development of SBIT.
Associated Myofascial Syndrome: When Points Ruin Everything
Myofascial trigger points, also known as iliotibial band syndrome (ITBS), can sometimes be associated with myofascial trigger points. Myofascial trigger points are areas of localized muscle tension, often associated with palpable nodules in the muscles. In the context of ITBS, certain muscles may develop trigger points that may contribute to symptoms. Here’s how myofascial trigger points may be associated with ITBS:
- Muscle tension: Due to the repetition of certain movements or muscle imbalances, excessive muscle tension can develop in the surrounding muscles, including the hip, thigh, and knee muscles.
- Trigger points: Myofascial trigger points can form in these tight muscles. These points can be hyperirritable areas in the muscles, often palpable as nodules.
- Pain Reference: Trigger points can radiate pain to other areas of the body. In the case of ITBS, pain can be felt along the iliotibial band, knee, and even into the thigh.
- Altered biomechanics: Muscle tension and trigger points can influence normal movement biomechanics, contributing to ITBS symptoms.
- Influence on the iliotibial band: Muscles associated with myofascial release, such as the tensor fasciae latae (TFL) and gluteus medius, are directly related to the iliotibial band. Tension or trigger points in these muscles can influence the tension placed on the iliotibial band.
Frequently Asked Questions (FAQ) about SBIT
- What is Iliotibial Band Syndrome (ITBS)?
- TBI is a painful condition caused by repeated rubbing of the iliotibial band on the outer condyle of the femur, causing inflammation.
- What are the characteristic symptoms of SBIT?
- Symptoms include pain on the outer side of the knee, often during physical activity, swelling, and sometimes a rubbing sensation.
- What activities can trigger or worsen SBIT?
- Activities such as running, prolonged walking, descending stairs, or any action involving repeated flexion and extension of the knee can aggravate TBI.
- How is Iliotibial Band Syndrome diagnosed?
- Diagnosis is based on clinical examination, medical history, and sometimes imaging tests such as MRI to rule out other causes.
- What treatments are available for SBIT?
- Treatments include rest, ice, stretching, osteopathy, the use of compression bandages, and in some cases, surgery.
- How long does it take to recover from SBIT?
- Recovery depends on the severity of the condition and response to treatment. It can take from a few weeks to several months.
- Can I continue to exercise with the SBIT?
- Low-impact activities may be allowed, but it is essential to follow the recommendations of your healthcare professional and avoid those that aggravate symptoms.
- What stretching techniques are beneficial for SBIT?
- Targeted stretches of the iliotibial tract may be recommended, including stretching of the iliotibial band and adjacent muscles.
- Is wearing compression bandages helpful in treating SBIT?
- Yes, compression bands can help reduce pressure on the iliotibial band, thereby relieving symptoms.
- Is SBIT preventable?
- Preventive measures include proper warm-up, progressive training, proper footwear, and correction of biomechanical defects. If pain persists, consult a healthcare professional.
Psychological Aspects and Pain Management
Iliotibial band syndrome (ITB) isn’t just a physical symptom; it can also have a significant impact on the mental and emotional well-being of sufferers. Chronic pain, especially when it prevents people from enjoying physical activities like running, can lead to feelings of frustration, stress, and sometimes even depression. Understanding and managing these psychological aspects is crucial for a complete and lasting recovery.
The psychological impact of chronic pain
Pain is a subjective experience that can be influenced by various psychological factors. When pain becomes chronic, it can lead to a range of emotional reactions, including anxiety and depression. IT band syndrome, which often affects athletes, can be particularly disruptive for those who consider sport an essential part of their lives and identities. The inability to train or compete can affect not only physical fitness, but also self-esteem and motivation.
Approaches to the psychological management of pain
It is important to recognize that pain management is not limited to physical interventions. Psychological approaches can play a key role in reducing pain perception and improving patients’ quality of life. Some of the most commonly used techniques include cognitive behavioral therapy (CBT), mindfulness meditation, and relaxation techniques.
CBT, for example, helps patients identify and change negative thoughts that can exacerbate pain perception. By rewiring their thinking, patients can develop a more positive and resilient attitude toward their condition. Mindfulness exercises, which involve paying conscious attention to the present moment without judgment, can also be effective in reducing stress and improving pain management.
The role of social support and motivation
Another often overlooked aspect of managing IT band syndrome is the importance of social support. Having a support network, whether it’s family, friends, or a fitness community, can make a big difference in how a person copes with pain. Social support not only provides moral encouragement but can also serve as a reminder that you are not alone in facing this challenge.
Motivation also plays a crucial role. For athletes, setting realistic and progressive goals, even if these must be modified due to the injury, can help maintain a sense of purpose and accomplishment. By working with an osteopath or coach, patients can develop a rehabilitation plan that integrates physical and psychological aspects, promoting a more complete recovery.
Daily coping strategies
In addition to formal psychological techniques, there are many coping strategies that patients can incorporate into their daily lives. For example, keeping a pain journal helps track symptoms and identify potential triggers. Adopting regular relaxation practices, such as yoga or deep breathing, can also help manage the muscular and mental tension associated with chronic pain.
Finally, it is essential that patients learn to accept their situation without resigning themselves to it. Acceptance does not mean giving up hope of recovery, but rather recognizing current limitations while continuing to seek ways to improve and live fully despite the pain.
Reindeer Test: Detecting TFL Tension
The athlete stands with one knee bent at 20 degrees.
The positive TFL tension response occurs when pain is felt at the lateral femoral condyle. Apply pressure to the insertion of the TFL to verify the location of the pain.

Osteopathic Approach: Techniques and Prevention
Iliotibial band syndrome, also known as iliotibial band syndrome, is a common cause of knee pain, particularly among runners. While conventional treatments often focus on pain management and rehabilitation, osteopathy offers a complementary perspective worth exploring. This holistic approach not only treats symptoms but also seeks to identify and correct underlying bodily imbalances that may contribute to the recurrence of this condition.
Understanding the osteopathic approach
Osteopathy, a practice based on the principle that the body has an inherent ability to heal itself, offers long-term solutions for IT band syndrome. Unlike conventional treatments that may focus solely on the painful area, osteopaths examine the body as a whole to detect dysfunctions that may be causing the problem. For example, an imbalance in posture or muscle asymmetry can put excessive pressure on the IT band, triggering inflammation.
An osteopathic consultation begins with a comprehensive patient assessment, which includes a postural analysis, joint mobility examination, and muscle tension assessment. The osteopath looks for mobility restrictions that may affect the biomechanics of the knee and, by extension, the iliotibial band. Treatment techniques may include gentle joint manipulation, muscle stretching, and myofascial release techniques aimed at releasing tissue tension.
Prevention by correcting imbalances
One of the most powerful aspects of the osteopathic approach is prevention. Once imbalances have been identified and addressed, the osteopath can suggest personalized exercises to strengthen weak muscles, improve tissue flexibility, and correct posture. These recommendations are tailored to the patient’s lifestyle and activities, whether running or other sports.
For example, specific stretches of the iliotibial band, combined with strengthening of the hip stabilizing muscles, can help prevent the syndrome from recurring. The osteopath may also recommend changes in running technique or the adjustment of equipment, such as shoes, to reduce overload on the iliotibial band.
The role of proprioception and coordination
Another essential aspect of osteopathic prevention is improving proprioception and coordination. Working on proprioception helps improve the perception of the body’s position and movement in space, which is crucial for athletes. Exercises that stimulate proprioception may include the use of balance boards or other tools that strengthen joint and muscle stability.
By integrating these elements into a rehabilitation and prevention program, osteopathy not only treats the symptoms of iliotibial band syndrome, but also aims to reduce the risk of recurrence by correcting the underlying causes.
Osteopathic Approach to the Syndrome
When dealing with iliotibial band syndrome, the osteopath does not limit himself to treating pain localized to the knee. He seeks to understand the patient’s body history , to identify deep compensations and to restore a harmonious dynamic between the different structures. This systemic approach distinguishes osteopathy from strictly symptomatic interventions.
Treatment of fascial and muscular tensions
The iliotibial band is not a muscle strictly speaking, but a fascial structure stretched by the TFL and the gluteus maximus . Its relaxation therefore requires overall work on:
- TFL : release of myofascial tension, reflex inhibition if hypertonic.
- The gluteus maximus : regulation of its activity by myotensive techniques.
- Fascia lata : decompression techniques, passive stretching or fascial gliding (for example in a lateral position with support on the superficial tissues).
- The strip itself : gentle release, without excessive direct pressure, to avoid exacerbating irritation.
The osteopath here favors respectful maneuvers , often slow, deep and attentive to tissue relaxation.
Overall rebalancing of the lower limb and pelvis
Beyond the symptomatic area, the osteopath assesses:
- The pelvis : presence of a posterior or anterior iliac, a tilt or sacroiliac instability.
- The hip : dysfunction of the coxofemoral joint or limitation of internal/external rotation.
- The knee : possible restriction of anteroposterior or rotational mobility.
- The foot : weight-bearing disorder, collapse of the plantar arch, asymmetry of pronation/supination.
These imbalances influence the mechanical chain and create ascending or descending tensions which overload the band . The osteopath thus works to restore the functional axis of the lower limb as a whole.
Integration of sporting gesture and posture
In a preventive and sustainable logic, it is essential to correct the gestural habits at the origin of the imbalance :
- Analysis of stride or pedaling ,
- Observation of the postural pattern standing or in movement ,
- Assessment of the sporting gesture if the patient practices a specific discipline (crossfit, trail, cycling, etc.).
Osteopathic treatment can integrate postural reprogramming , proprioception , or targeted mobility exercises at home.
Cranial approach and autonomic nervous system
In some patients, the neurovegetative component is strongly involved: stress, bodily hypervigilance, sleep disorders, etc. An overload of the sympathetic nervous system can increase basic muscle tone, including at the level of the TFL or lumbar paravertebral muscles.
Cranial relaxation techniques, vagal regulation or thoracic release (particularly of the diaphragm) can reduce this background hypertonia and accelerate recovery.
Individualized support
Each patient presents a unique picture. The osteopath therefore adapts his techniques according to:
- Tissue tolerance (acute vs chronic),
- Sports practice (quick recovery or necessary stop),
- The emotional context (injury experienced as a failure or a signal).
This relational and perceptive dimension of care is often what creates a therapeutic trigger, where mechanical treatments alone fail.
Targeted Exercises and Stretches: Relieving the Iliotibial Band
1. Standing iliotibial band stretch:
- Standing, cross the leg to be stretched behind the other.
- Tilt your upper body to the side opposite the crossed leg, keeping the stretched leg slightly bent.
- You should feel the stretch on the side of your thigh. Hold for 15 to 30 seconds and repeat on the other side.

2. Foam rolling:
- Lie on your side, placing the foam roller under the hip of the leg to be treated.
- Use your arms to support your weight and slowly roll from the top of your hip to your knee.
- Focus on areas that are tense and painful, using back and forth movements.
- Do this for 1 to 2 minutes on each side.

3. IT strip on the side :
- Stand sideways, approximately 30 cm from a wall, with your affected side closest to the wall.
- Extend your arm toward the wall for support.
- Cross your unaffected leg in front of your affected leg, keeping the foot of your affected leg flat on the floor.
- Lean against the wall with your hip and hold this position for 15 seconds.
- Repeat three times.
4. Seated iliotibial band stretch:
- Sit on the floor with your legs extended in front of you.
- Cross the leg to be stretched over the other leg.
- Gently rotate your torso toward the side of the crossed leg, using your opposite elbow to apply gentle pressure to the knee.
- Hold the position for 15 to 30 seconds and repeat on the other side.

5. Hamstrings with a towel, lying on your back:
- Lie on your back, wrap a towel around the back of one thigh and support the thigh by holding each end of the towel.
- Keep the other leg flat on the floor.
- Slowly straighten your knee until you feel a stretch in the back of your thigh, trying to make the bottom of your foot parallel to the ceiling.
- Never straighten your leg or straighten your knee until the stretch is comfortable.
- Hold the position for 10 seconds at first, then gradually increase to 30 seconds.

6. Standing quadriceps:
- When standing, hold onto a counter or the back of a chair to help you maintain balance.
- Bend your knee back, grabbing your ankle with one hand.
- Help bend your knee back as far as possible.
- Hold the position for 30 seconds.
- Return to standing position.
- Repeat the exercise 3 to 5 times with each leg.

7. Strengthening the abductor muscles:
- Exercises such as lateral leg raises, lateral squats, and resistance band exercises can strengthen the abductor muscles and help stabilize the iliotibial band.
8. Quadriceps and hip flexor stretch:
- The quadriceps muscles and hip flexors can also influence tension in the iliotibial band. Be sure to include stretches for these muscle groups in your routine.
It is important to consult a healthcare professional or physiotherapist before beginning any exercise program, especially if you have persistent pain. They will be able to provide you with personalized advice based on your specific situation.
Prevention and Personalized Advice
Once the pain is under control, the crucial step of prevention begins. Since IT band syndrome is an overuse condition, preventive strategies should aim to reduce tissue load , optimize movement and maintain a sustainable functional balance . The osteopath plays a key role here in education, correction and long-term support.
Adapted stretching: flexibility without stress
Contrary to popular belief, the iliotibial band should not be stretched directly , as it is a fibrous tissue with limited elasticity. However, it can be effectively worked:
- The TFL : crossing the affected leg behind the other, then leaning laterally towards the opposite side.
- The gluteus maximus : via stretches in the piriformis or yoga position (“pigeon” type).
- Adjacent muscles ( quadriceps, hamstrings) which can alter the overall stress on the knee.
Short sessions (30 seconds x 3, 1 to 2 times a day) are often more beneficial than a long weekly stretch.
Targeted strengthening: stabilizing the pelvic chain
Pelvic motor control deficits are common in patients with band syndrome. Therefore, it is necessary to strengthen:
- The gluteus medius : clam shell type exercises, stepping, side bridge abduction.
- The transverse abdominis : dynamic sheathing with activation of the pelvic floor.
- The knee stabilizing muscles (VMO, short hamstrings) to correct joint trajectories.
A trained physiotherapist or coach can design a progressive plan tailored to the patient’s profile.
Gradual resumption of physical activity
Resuming too soon or too intensely encourages relapses. It is recommended:
- To wait a week without pain during exertion , even minimal.
- To resume with short sessions , with a gradual warm-up and a prolonged return to calm.
- Avoid hard surfaces, drops or sudden changes in direction.
Wearing corrective insoles or suitable shoes (under podiatric assessment) can also relieve mechanical tension.
Posture and lifestyle habits
The osteopath will be able to observe and correct aggravating habits:
- Prolonged sitting posture in external rotation of the hip (tension on the TFL),
- Crossing legs while sitting,
- Carrying heavy side bags , causing pelvic imbalance,
- Prolonged sedentary lifestyle , which promotes fascial tension.
Incorporating conscious micro-movements into your day (mobilizations, breathing, light stretching) can make a difference in the long term.
Regular osteopathic support
Preventive osteopathic consultations can be useful every 3 to 6 months for:
- Maintain good joint mobility ,
- Correct emerging imbalances ,
- Adapt the treatment to the level of stress or physical fatigue at the time.
This monitoring contributes to better knowledge of the patient’s body and autonomy in managing their bodily signals.
Conclusion: Listen to the Body to Go Further
Iliotibial band syndrome, while often viewed as a simple mechanical overload, actually reveals the complexity of the body in motion . Sometimes, localized knee pain hides a broader imbalance—poor coordination, inappropriate posture, or unexpressed stress.
Osteopathy, through its comprehensive approach, does not only seek to silence the symptom. It invites us to listen to what the body is expressing , to trace the causes, to restore the lost balance. It helps us understand how each gesture, each tension, each posture participates in a silent dialogue that the patient maintains with himself.
But care doesn’t stop at the consulting table. It extends into daily habits, the quality of self-care, and the choices made to respect one’s own rhythm. Preventing a recurrence means relearning how to walk mindfully, how to train with kindness, and how to move without brutality.
Each pain then becomes a starting point towards greater harmony , an opportunity for bodily and inner growth. And perhaps this is the true role of the osteopath: not to repair, but to awaken the body’s ability to find its axis, its breath and its correct movement.
References
- Nguyen US, Zhang Y, Zhu Y, Niu J, Zhang B, Felson DT. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. Ann Intern Med. 2011 Dec 06;155(11):725-32. [PMC free article] [PubMed]
- Falvey EC, Clark RA, Franklyn-Miller A, Bryant AL, Briggs C, McCrory PR. Iliotibial band syndrome: an examination of the evidence behind a number of treatment options. Scand J Med Sci Sports. 2010 Aug;20(4):580-7. [PubMed]
- Strauss EJ, Kim S, Calcei JG, Park D. Iliotibial band syndrome: evaluation and management. J Am Acad Orthop Surg. 2011 Dec;19(12):728-36. [PubMed]
- Ferber R, Noehren B, Hamill J, Davis IS. Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. J Orthop Sports Phys Ther. 2010 Feb;40(2):52-8. [PubMed]
- Fairclough J, Hayashi K, Toumi H, Lyons K, Bydder G, Phillips N, Best TM, Benjamin M. Is iliotibial band syndrome really a friction syndrome? J Sci Med Sport. 2007 Apr;10(2):74-6; discussion 77-8. [PubMed]
- Fredericson M, Weir A. Practical management of iliotibial band friction syndrome in runners. Clin J Sport Med. 2006 May;16(3):261-8. [PubMed]
- Sharma J, Greeves JP, Byers M, Bennett AN, Spears IR. Musculoskeletal injuries in British Army recruits: a prospective study of diagnosis-specific incidence and rehabilitation times. BMC Musculoskelet Disord. 2015 May 04;16:106. [PMC free article] [PubMed]
- Jensen AE, Laird M, Jameson JT, Kelly KR. Prevalence of Musculoskeletal Injuries Sustained During Marine Corps Recruit Training. Mil Med. 2019 Mar 01;184(Suppl 1):511-520. [PubMed]
- Holmes JC, Pruitt AL, Whalen NJ. Iliotibial band syndrome in cyclists. Am J Sports Med. 1993 May-Jun;21(3):419-24. [PubMed]
- Gunter P, Schwellnus MP. Local corticosteroid injection in iliotibial band friction syndrome in runners: a randomised controlled trial. Br J Sports Med. 2004 Jun;38(3):269-72; discussion 272. [PMC free article] [PubMed]
- Noble CA. Iliotibial band friction syndrome in runners. Am J Sports Med. 1980 Jul-Aug;8(4):232-4. [PubMed]
- Creation in part: Andrew Hadeed; David C. Tapscott.



 Weakness: Causes, Implications, and Solutions")











 of the knee")


{kind=link}