

What is intercostal neuralgia?
Between chest pain and diagnostic pitfalls
Intercostal neuralgia refers to pain along the path of one or more intercostal nerves, the sensory and motor nerves that run between the ribs, following the costal groove. Although relatively rare in its pure form, this pathology is frequently encountered in manual care practices in mixed or confused forms, where spinal, musculoskeletal, visceral or postural pain come together to form the picture.
A clinical picture not to be underestimated
The cardinal symptom is unilateral, linear pain, following the path of an intercostal space, often located in the thoracic or dorso-lumbar area. The pain can be sharp, burning, stabbing, or like a vice squeezing the rib cage. It is generally amplified by breathing movements, coughing, sneezing, or even certain postures. The patient may report a pulling or electric sensation along the rib, sometimes radiating to the abdomen or back.
This pain may be accompanied by paresthesia (tingling, numbness), cutaneous hyperesthesia (hypersensitivity) along the nerve path, or even a feeling of tension or deep discomfort in the chest, which increases anxiety.
The multiple sources of confusion
The major pitfall of intercostal neuralgia lies in its mimetic potential. It can simulate left-sided cardiac pain, evoke angina pectoris, pericarditis, or even pulmonary pain, particularly in cases of pleural puncture or basal lung disease. On the right side, it can resemble biliary or hepatic pain. In the lower region, it is often confused with abdominal or gynecological pain.
Pain referred from the spine—as in thoracic disc herniation or facet syndromes—can also mimic intercostal neuralgia, particularly if a foramen is narrowed or there is local muscle spasm. Intercostal zoster, in its early stages, can also mimic mechanical intercostal neuralgia, before the characteristic skin blisters appear.
Finally, certain so-called “post-surgical” or “post-traumatic” pains, such as after thoracic surgery, a rib fracture or a blocked rib, can maintain prolonged local nerve irritation.
The importance of a rigorous differential diagnosis
In the face of any chest pain, a medical assessment is essential to exclude serious pathologies (cardiovascular, pulmonary or visceral). Once these causes have been ruled out, it is essential to look for specific clinical signs that could point towards intercostal neuralgia of mechanical, postural or functional origin.
Diagnosis often relies on careful history-taking and palpatory clinical examination, particularly when it reveals a specific painful trigger point along an intercostal space, associated muscle spasm, or loss of rib or spinal mobility.
Disclaimer: The information in this article is provided for educational purposes only. It is not a substitute for professional medical advice or diagnosis. Do not undertake any treatment, exercise, or manipulation described herein without the guidance of a qualified professional.
Functional anatomy of the intercostal nerves
A network sensitive to the slightest imbalance
To understand the origins and mechanisms of intercostal neuralgia, it is essential to delve into the anatomy of the intercostal nerves. These structures, although discreet, play a crucial role in the sensitivity and motor functions of the thorax. Their intimate relationship with the vertebrae, ribs, intercostal muscles, diaphragm, and even the thoracoabdominal viscera makes them a crossroads of mechanical and neurovegetative tensions.
A precise route, an essential mission
Each intercostal nerve arises from the ventral root of a thoracic spinal nerve, from T1 to T12. They emerge from the intervertebral foramen, pass between the intertransverse muscles, and then enter the intercostal space between the corresponding upper and lower ribs. There, they course in the costal groove, accompanied by the intercostal artery and vein, partly protected by the lower margin of the rib.
Along their course, the intercostal nerves emit motor branches for the internal and external intercostal muscles, the upper abdominal muscles (especially from T7 to T12), as well as lateral and anterior cutaneous branches for sensory innervation of the trunk. The subcostal nerve (T12) descends below the 12th rib, with a slightly different configuration.
A vulnerability to multifactorial compression
This relatively long path, confined within narrow anatomical spaces, exposes the intercostal nerves to multiple sources of irritation. Loss of mobility of a thoracic vertebra, costovertebral or costotransverse dysfunction, diaphragmatic tension, muscle spasm, or scar fibrosis can impair nerve gliding, cause a pinching effect, or create hypersensitivity.
Abdominal scars (cesarean sections, appendectomies, laparotomies), chronic myofascial tension, or postural fixations linked to restricted breathing, can cause traction on the terminal cutaneous branches of the intercostal nerves, contributing to persistent localized pain.
A crossroads between somatic and visceral
The intercostal nerves are not isolated from the visceral sphere. Through their connections with the sympathetic nervous system, particularly via the communicating branches, they participate in the neurovegetative regulation of the upper thoracic and abdominal organs. This connection partly explains why intercostal irritation can cause functional digestive disorders, or conversely, why hepatic, gastric, or pancreatic congestion can reflexively irritate an intercostal nerve.
In osteopathy, this interconnection justifies the global assessment of the patient suffering from intercostal neuralgia: chest pain can be the reflection of a local mechanical conflict, but also the expression of a deeper imbalance affecting posture, breathing, or the visceral sphere.
Understanding Intercostal Neuralgia: A Neuropathic Chest Pain
Intercostal neuralgia is a painful condition that occurs when the intercostal nerves, located between the ribs, become irritated, compressed, or inflamed. This neuropathic pain can present in a variety of ways: it is often described as a sharp, throbbing, burning, or stabbing sensation, radiating from the thoracic region to the chest, back, or sometimes the abdomen. Patients frequently report persistent or intermittent pain, sometimes worsened by movements such as deep breathing, coughing, or changes in posture. This pain often appears as a band-like sensation that envelops the chest, following the path of the intercostal nerves, creating a characteristic “girdle” pain.
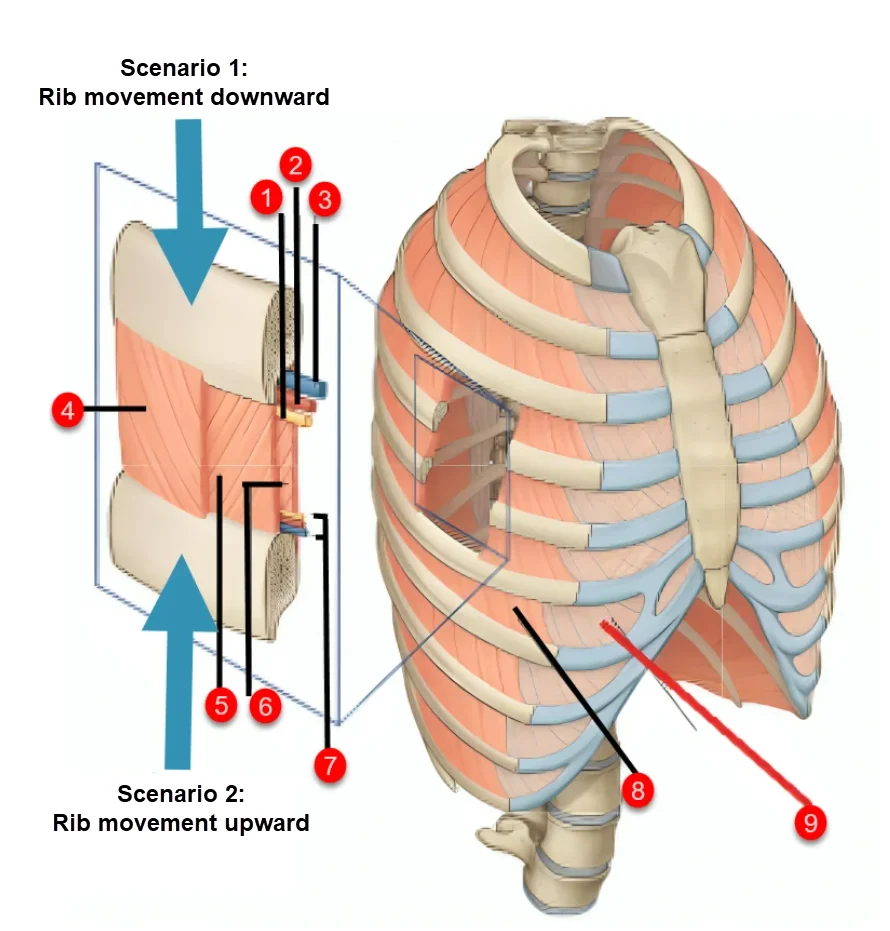
is triggered by compression, irritation, or displacement of the intercostal nerve (1) . This irritation can be caused by various biomechanical imbalances, including downward or upward displacement of the ribs , resulting in nerve compression or stretching of the nerve.
Identification of Structures:
- Intercostal Nerve – Located between the intercostal muscles, it transmits sensory and motor signals. Compression or irritation of this nerve causes intercostal neuralgia .
- Intercostal Artery – Provides blood supply to the intercostal muscles and adjacent structures.
- Intercostal Vein – Drains blood from the intercostal muscles and thoracic tissues.
- External Intercostal Muscles – Located on the outer surface of the ribs, they are involved in inspiration by lifting the rib cage.
- Internal Intercostal Muscles – Located below the external muscles, they participate in forced expiration by lowering the ribs.
- Intimate Intercostal Muscles – Located deeper, they stabilize the ribs and provide biomechanical support to the rib cage.
- Parietal Pleura – Protective membrane covering the inside of the thoracic cage and providing protection to the lungs.
- Thoracic Cage – Bony structure comprising the ribs, vertebrae and sternum, providing protection to vital organs and thoracic mobility.
- Referred Pain in Intercostal Neuralgia – Pain radiating along the course of the intercostal nerve to the chest wall, abdomen, or back.
Scenario 1: Coast Shift Downwards
When the rib moves downward, it compresses the intercostal nerve in the lower intercostal space. This condition can be caused by:
- Chest trauma (fall, direct blow).
- A prolonged posture with thoracic flexion.
- Excessive muscle spasms of the intercostal muscles.
Consequence: This compression causes nerve irritation resulting in intense, stabbing pain, radiating along the nerve’s path.
Scenario 2: Moving the Coast Upwards
When the rib is displaced upward, it stretches or pinches the intercostal nerve at the level of the upper intercostal space. This displacement may be due to:
- A hyperextension of the thoracic spine.
- Excessive traction of the ribs by muscle spasms.
- A misalignment of the costovertebral joints.Consequence: This excessive traction of the nerve creates neuropathic pain, often aggravated by respiratory movements or thoracic rotations.
Consequences of Coastal Shift:
- Nerve Irritation and Inflammation – Prolonged irritation leads to local inflammation which worsens pain.
- Referred Pain – Pain may travel along the nerve pathway, radiating to the chest, back, or abdomen.
- Restricted Thoracic Mobility – Pain prevents deep breathing, limiting chest movement and worsening nerve compression.
Pathophysiological Mechanisms: Why Does Pain Persist?
Intercostal neuralgia, characterized by sharp, persistent pain along the intercostal nerves located between the ribs, is often aggravated by various biomechanical imbalances. These imbalances can result from multiple factors, including nerve compression, poor posture, reduced mobility of the thoracic spine, muscle dysfunction, repetitive activities, and physical trauma. Each of these factors can contribute to persistent pain by placing excessive stress on musculoskeletal structures and exacerbating intercostal nerve irritation. To better understand how the body influences pain, it is essential to thoroughly examine these biomechanical factors in order to adopt appropriate treatment strategies.
Nerve compression is one of the main mechanisms contributing to intercostal neuralgia. It can be caused by a thoracic disc herniation, spinal osteoarthritis, or inflammation due to trauma. When the intercostal nerves are compressed, it generates hypersensitivity in the nerve pathways, causing intense neuropathic pain that radiates along the ribs. This compression can also be linked to a decrease in intervertebral space or excessive muscle tension that puts pressure on the nerves, resulting in persistent and difficult-to-relieve pain.
Poor posture plays a key role in the development and worsening of intercostal neuralgia. Prolonged flexed postures, such as those adopted during prolonged computer or mobile device use, increase pressure on the thoracic spine and limit vertebral mobility. This position creates muscle tension in the intercostal and paravertebral muscles, creating an environment conducive to intercostal nerve irritation. Chronic postural imbalances can also alter the distribution of mechanical loads on the spine, leading to increased nerve compression and exacerbating chest pain.
Reduced mobility of the thoracic spine is another major factor influencing intercostal pain. The thoracic spine, which provides essential mobility for respiratory movements and trunk rotations, can become rigid due to prolonged muscle tension, thoracic spondylosis, or tissue adhesions. Reduced mobility limits normal chest expansion, increasing pressure on the intercostal nerves. This restriction not only leads to neuropathic pain but also to decreased breathing capacity, which can worsen pain and limit daily activities.
Intercostal muscle dysfunction and spasms are also significant contributors to intercostal neuralgia. The intercostal muscles, which play a critical role in stabilizing the rib cage and facilitating respiratory movements, can develop myofascial trigger points. These trigger points, often located in the intercostal muscles or nearby muscles, are hyperirritable areas that cause local and referred pain along the intercostal nerves. When these muscles are subjected to excessive tension, spasms, or involuntary contractions, they compress the intercostal nerves and amplify painful symptoms, thereby increasing pain perception and reducing thoracic mobility.
Repetitive activities and mechanical stress are another key factor in the development and persistence of intercostal neuralgia. Repetitive movements involving excessive rotation or flexion of the trunk, often seen in certain sports such as swimming or tennis, or in occupations that constantly place stress on the thoracic region, can cause microtrauma. These repetitive movements lead to chronic muscle tension, inflammation, and changes in thoracic biomechanics, increasing pressure on the intercostal nerves. In the long term, these excessive mechanical stresses create a biomechanical imbalance, increasing vulnerability to persistent chest pain and irritation of nerve structures.
Finally, physical trauma plays a key role in the onset and worsening of intercostal neuralgia. Direct trauma to the chest, such as a fall, car accident, or sports injury, can cause bruises, fractures, or injuries to the ribs and surrounding structures. These injuries often lead to local inflammation, which, by compressing the intercostal nerves, triggers a cascade of neuropathic pain. In addition, trauma can cause secondary biomechanical imbalances, further limiting thoracic mobility and contributing to persistent pain.
The biomechanical impact on intercostal neuralgia is not limited to these isolated factors. In fact, these elements are often interconnected and act synergistically to exacerbate pain and reduce thoracic functionality. For example, prolonged poor posture can lead to decreased thoracic mobility, causing muscle tension and secondary nerve compression. Similarly, physical trauma can induce muscular and fascial imbalances that increase the vulnerability of thoracic structures to neuropathic pain.
Possible origins of intercostal neuralgia
From mechanical causes to emotional factors
Intercostal neuralgia, often perceived as a simple local nervous conflict, is actually part of a multifactorial framework. Far from being a single entity, it can result from mechanical imbalances, surgical sequelae, visceral disturbances, or even deep-rooted emotional factors. For the osteopath, identifying the origin of the pain means untangling a complex knot where the body expresses, sometimes for a long time, unresolved tension.
1. Vertebral and costovertebral dysfunctions
The most common causes are joint blockages in the thoracic vertebrae or their articulation with the ribs. A loss of mobility of a vertebra (particularly T4 to T9), a fixed rotation or a translation, can create compression or irritation of the intercostal nerve as it exits the intervertebral foramen. The costotransverse joints, when restricted, can also act as areas of friction or localized tension.
This is often associated with a muscle spasm of the paravertebral or intercostal muscles, which increases the pain and creates a vicious circle: pain → contraction → compression → pain.
2. Post-surgical trauma and sequelae
Thoracic trauma (fall, direct impact, rib contusion) or surgery (such as thoracotomy, breast surgery, or low transverse cesarean section) can injure or irritate the intercostal nerves. Even in the absence of frank nerve injury, the formation of fibrosis or tissue adhesions around muscles, fascia, and skin can lead to chronic tension on the cutaneous branches of the nerve.
These pains are often postural, with areas of hypersensitivity or hyperalgesia located near a scar or surgical site.
3. Visceral factors and organ mobility disorders
Intercostal nerve irritation can also be reflexive. An engorged liver, a ptotic stomach, or a spastic colon can disrupt the biomechanics of the diaphragm and lower ribs, causing upward tension on muscle and fascial attachments.
The liver, in particular, whose attachments are close to ribs 7 to 11, can influence the lower intercostal spaces, particularly on the right. These visceral tensions sometimes result in “phantom” or projected pain in the chest wall, without any objective local abnormality.
4. Postural disorders and dysfunctional breathing
Exaggerated kyphotic posture, thoracic scoliosis, or fixation of the diaphragm secondary to chronic stress can also be the cause of intercostal neuralgia. In these cases, it is not so much a specific point of compression that is the cause, but rather an overall loss of flexibility of the rib cage, leading to over-stressing of certain costal or vertebral segments.
Breathing becomes high, rigid, and less mobile, and certain intercostal spaces then become “locked” in a forced dynamic, generating repeated microtraumas.
5. Emotional stress and somatized tensions
Finally, psychological stress plays an insidious but crucial role. The rib cage is a highly symbolic region, the seat of breathing, the heart, and “oppressive” or “squeezing” emotions. Chronic intercostal pain can be the bodily expression of emotional repression, inner conflict, or an old, undigested bodily memory.
In some patients, especially when medical examinations are normal, this psychosomatic dimension emerges as a major avenue. Osteopathic treatment then aims both to restore mobility and to promote a reappropriation of the body and its feelings.
Signs and Symptoms: Recognizing Key Symptoms
- Chest pain: Pain is the main symptom of intercostal neuralgia. It can be sharp, throbbing, or burning and is often described as an electric pricking sensation.
- Pain location: The pain follows the course of the intercostal nerves and is usually located on the side of the torso. It may radiate forward or backward.
- Worse with movement: Movements of the torso, such as coughing, sneezing, twisting the trunk, or even deep breathing, can worsen the pain.
- Skin hypersensitivity: The skin over the affected area may become more sensitive to touch. Tight clothing or direct skin contact may be uncomfortable.
- Belt-like pain: Pain can sometimes surround the chest like a belt, following the course of the intercostal nerves.
- Tingling or Numbness: Some individuals may experience tingling or a feeling of numbness in the affected area.
- Burning sensations: The pain may be accompanied by burning sensations, adding to the discomfort felt by the person.
- Difficulty breathing deeply: Due to the pain associated with breathing movements, some people may avoid breathing deeply, which can lead to shallow breathing.
- Muscle cramps: The intercostal muscles may contract in response to pain, resulting in cramps or spasms.
- Muscle tension: The affected area may exhibit increased muscle tension in response to pain.
Biomechanical Impact: How Does the Body Influence Pain?
Intercostal neuralgia, characterized by intense, stabbing pain along the intercostal nerves, is often influenced by complex biomechanical factors. These include nerve compression, postural imbalances, reduced thoracic spine mobility, muscle dysfunction, repetitive mechanical stress, and physical trauma. Each of these factors contributes to the genesis and maintenance of pain, sometimes complicating its management and requiring a tailored therapeutic approach.
Nerve compression is one of the main causes of intercostal neuralgia. It can result from a thoracic disc herniation, spinal osteoarthritis, or excessive muscle compression in the intercostal spaces. When the intercostal nerves are compressed or irritated, it leads to hypersensitization of the nerve pathways and neuropathic pain that radiates into the thoracic region, sometimes to the abdominal or back wall. This compression can also be aggravated by surrounding muscle tension, which increases pressure on the nerves, intensifying symptoms.
Poor posture plays a major role in the biomechanical imbalances that can trigger or aggravate intercostal neuralgia. Prolonged flexion, such as that adopted during prolonged use of a computer or mobile device, can increase pressure on the thoracic spine, limiting the mobility of the vertebrae and ribs. This prolonged position can also create excessive tension on the intercostal and paravertebral muscles, disrupting musculoskeletal balance and promoting compression of the intercostal nerves. In the long term, these postural imbalances increase the risk of chronic pain and recurrence.
Reduced mobility of the thoracic spine is another key component influencing intercostal pain. The thoracic spine, due to its connection to the ribs and sternum, plays a crucial role in breathing and trunk movement. When this mobility is restricted, whether due to thoracic spondylosis, tissue adhesions, or prolonged muscle tension, it impairs the thorax’s ability to expand and contract properly. A decrease in this range of motion can increase pressure on the intercostal nerves, leading to pain, stiffness, and decreased breathing capacity.
Intercostal muscle dysfunction and spasms are also aggravating factors in intercostal neuralgia. The intercostal muscles, which provide thoracic stability and participate in respiratory movements, can develop myofascial trigger points, contributing to local and referred pain along the intercostal nerves. When these muscles are subjected to repetitive tension, spasms, or involuntary contractions, they can compress the nerves and worsen painful symptoms. This muscle tension can also alter thoracic biomechanics, further limiting mobility and exacerbating pain.
Repetitive activities and mechanical stress are another key factor in the development of intercostal neuralgia. Repetitive movements, such as those seen in certain sports (swimming, tennis) or manual occupations, place excessive strain on the intercostal muscles, rib joints, and thoracic spine. These repeated stresses can cause microtrauma, inflammation, and chronic muscle tension, creating an environment conducive to intercostal nerve compression. Over time, these excessive movements can lead to a biomechanical imbalance, increasing vulnerability to persistent chest pain.
Finally, physical trauma plays a crucial role in the onset and worsening of intercostal neuralgia. A direct blow to the chest, such as a car accident, fall, or sports injury, can result in bruises, fractures, or injuries to the ribs and surrounding structures. These injuries can compress or irritate the intercostal nerves, triggering an inflammatory cascade and increasing the sensitivity of the nerve structures. Furthermore, trauma can lead to secondary biomechanical imbalances, limiting thoracic mobility and contributing to persistent pain.
In summary, biomechanical factors significantly influence the onset and progression of intercostal neuralgia. Understanding these mechanisms allows for a targeted therapeutic approach, including manual techniques to restore mobility, postural corrections to prevent recurrence, and specific exercises to strengthen thoracic stability. By taking these elements into account, practitioners can optimize patient care and improve their quality of life.
Diaphragm and Intercostal Neuralgia: Understanding the Links for Optimal Treatment
Intercostal neuralgia, characterized by sharp, stabbing, or burning pain along the intercostal nerves, can be aggravated by imbalances and tension in the surrounding musculoskeletal structures, particularly the diaphragm. The diaphragm, the primary respiratory muscle, plays a key role not only in breathing but also in thoracoabdominal stability. When tense, dysfunctional, or restricted, it can negatively affect rib cage mobility, cause increased muscle tension, and place additional pressure on the intercostal nerves, contributing to the onset or worsening of intercostal neuralgia. Understanding the interaction between the diaphragm and thoracic structures can improve treatment strategies and achieve more lasting results for patients suffering from this condition.
The Diaphragm: A Key Muscle for Thoracic and Abdominal Mobility
The diaphragm is a dome-shaped muscular structure located between the thoracic and abdominal cavities. It attaches primarily to the lower ribs, lumbar vertebrae, and sternum. During inhalation, the diaphragm contracts and lowers, increasing thoracic volume and allowing air to enter the lungs. During exhalation, it relaxes and returns to its original position, allowing air to escape. This respiratory dynamic is essential for maintaining optimal balance in the rib cage, intercostal muscles, and surrounding fascia.
However, when diaphragmatic dysfunction exists , due to muscle tension, chronic shallow breathing, or visceral adhesions, the normal mobility of the diaphragm is impaired. This restriction can limit the ability to expand the chest and increase mechanical stress on the ribs, intercostal muscles, and intercostal nerves. As a result, pressure on the nerves can increase, leading to irritation, hypersensitivity, and increased neuropathic pain characteristic of intercostal neuralgia.
Influence of the Diaphragm on Intercostal Neuralgia: The Underlying Mechanisms
- Intercostal Nerve Compression
Excessive tension of the diaphragm can alter thoracoabdominal biomechanics, leading to indirect compression of the intercostal nerves. This compression may be due to restricted mobility of the lower ribs, creating an environment conducive to irritation of the nerves that pass through these structures. In addition, when the diaphragm is tense, it exerts increased traction on the surrounding fascia, increasing the pressure on the intercostal nerves. - Reduced Thoracic Mobility
Restricted diaphragmatic mobility also affects the mobility of the ribs and thoracic vertebrae. This limitation leads to decreased chest expansion and respiratory movements, increasing tension on the intercostal muscles. When these muscles become rigid or tight, they can compress the intercostal nerves, exacerbating the neuropathic pain associated with intercostal neuralgia. - Intra-Abdominal Pressure Disruption
The diaphragm also plays a key role in maintaining intra-abdominal pressure. An imbalance in the diaphragm can alter this pressure, creating asymmetrical tensions that influence surrounding structures, including the intercostal muscles and intercostal nerves. This disruption can exacerbate pain, reduce thoracic mobility, and prolong the duration of symptoms.
Osteopathic Techniques to Release the Diaphragm and Treat Intercostal Neuralgia
Osteopathy offers a comprehensive approach to treating intercostal neuralgia by addressing associated diaphragmatic dysfunction. Osteopathic techniques used to release the diaphragm help restore thoracic mobility, reduce muscle tension, and relieve pressure on the intercostal nerves.
- Myofascial Release of the Diaphragm The myofascial release
technique involves applying gentle, sustained pressure to the fascia surrounding the diaphragm. The osteopath places their hands under the lower ribs and gently pulls upward, allowing the diaphragm to gradually release. This technique improves diaphragm mobility, reduces muscle tension, and decreases pressure on the intercostal nerves. - Direct Diaphragmatic Release Techniques
This technique involves gentle mobilization maneuvers to restore diaphragmatic mobility. The osteopath applies gentle pressure under the lower ribs and uses rhythmic movements to promote gradual relaxation. By releasing diaphragmatic tension, this approach improves breathing range, reduces chest strain, and relieves compression of the intercostal nerves. - Visceral Techniques to Release Adhesions
Visceral tension around the liver, stomach, or intestines can also affect diaphragmatic mobility. Osteopaths use visceral techniques to release adhesions and restore harmony between organs and thoracoabdominal structures. This approach improves overall mobility and reduces pressure on surrounding nerve structures. - Postural Rebalancing and Strengthening Exercises
To prevent recurrence, the osteopath may recommend exercises to strengthen the abdominal muscles and diaphragm, as well as postural advice to maintain good thoracoabdominal posture. These exercises help stabilize the thoracic region, prevent excessive muscle tension, and reduce the likelihood of intercostal neuralgia recurring.
Myofascial trigger points and intercostal neuralgia
Myofascial trigger points and intercostal neuralgia are two interconnected concepts in the field of muscle and nerve health. Myofascial trigger points, often referred to as “knot points,” are specific areas of muscle tension and contraction that can cause local or referred pain. Intercostal neuralgia, on the other hand, involves irritation or compression of the intercostal nerves located between the ribs.
In the context of intercostal neuralgia, myofascial trigger points can play a significant role. These tender points in the intercostal muscles or surrounding muscles can contribute to irritation of the intercostal nerves. When activated, these trigger points can cause local pain as well as referred pain along the intercostal nerves, thus exacerbating the symptoms of intercostal neuralgia.
Treating myofascial trigger points can be an important component of managing intercostal neuralgia. Treatment approaches may include manual techniques, such as myofascial release and trigger point release, as well as strengthening and stretching exercises targeting the involved muscles.
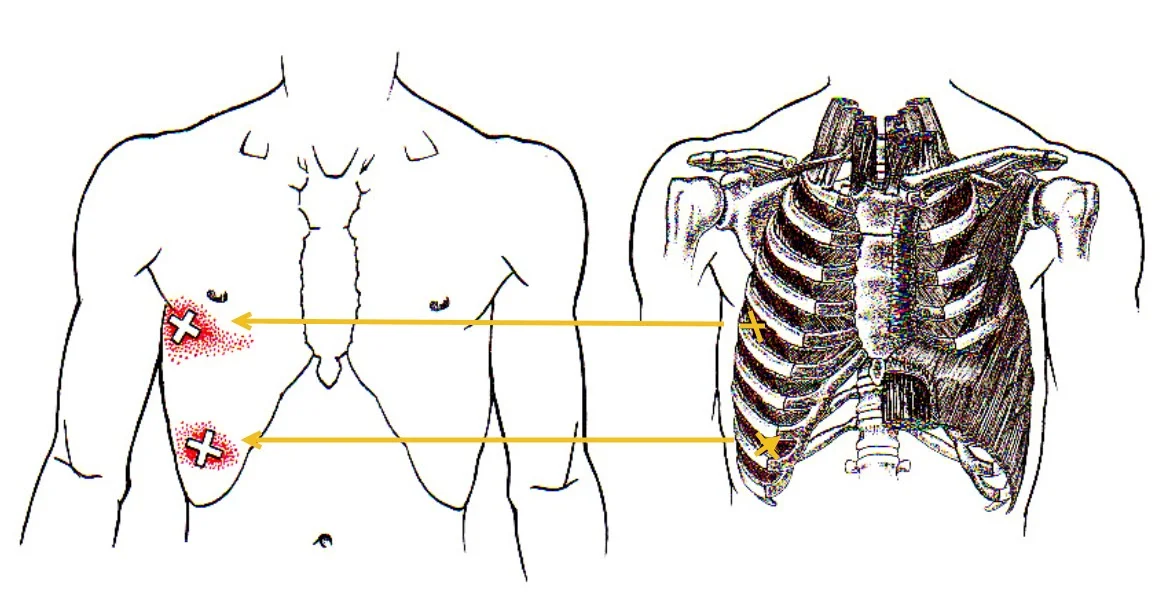
This image illustrates the connection between myofascial trigger points located in the intercostal muscles and referred pain areas felt on the anterior chest wall. The arrows indicate how tender points, often located in the intercostal or oblique muscles, can cause referred pain that follows the course of the intercostal nerves. This correlation explains why some patients experience persistent chest pain despite the absence of obvious organic pathology, highlighting the importance of treating these trigger points to relieve symptoms.
Osteopathic assessment: the art of touch and feeling
Locate the tension, listen to the pain
Before any therapeutic intervention, the osteopath uses their listening and hands-on skills to understand, perceive, and decode the body’s imbalances. In the context of intercostal neuralgia, manual assessment plays a central role: it not only allows the origin of the nervous conflict to be located, but also reveals its deeper layers—mechanical, tissue, visceral, or emotional.
The interrogation: capturing warning and resonance signals
The treatment begins with a rigorous interview. The therapist explores the nature of the pain (burning, stabbing, a feeling of a bar), its precise location, its mode of onset (gradual or sudden), its triggering factors (movement, breathing, stress), and its possible irradiation.
It also questions the antecedents: thoracic or abdominal surgery, rib trauma, visceral disorders, episodes of shingles, posture at work or at rest, anxiety disorders. This collection allows the emergence of the main somatic leads, but also the associated psycho-emotional contexts.
Global observation: posture, breathing and defensive attitude
Upon observation, some patients present a protective or avoidance posture: frozen chest, lowered shoulder, homolateral curvature. Breathing is often altered: short, high chest, with a decrease in amplitude on the painful side. This simple ventilation imbalance can already amplify the irritation of the intercostal nerve by limiting the mobility of the ribs.
The osteopath also observes the overall statics of the spine, the flexibility of the anterior and posterior myofascial chains, and the possible presence of a state of bodily hypervigilance or emotional armor.
Segmental palpation: search for the source of irritation
Fine palpation is the heart of the assessment. The practitioner precisely explores:
- Mobility of the thoracic vertebrae, in flexion, extension, rotation and inclination.
- The costovertebral and costotransverse joints, looking for a loss of elasticity.
- The intercostal spaces, looking for a sensitive, tense or retracted space.
- Trigger points or areas of myofascial tension in the intercostal, serratus, paravertebral, or abdominal muscles.
- Skin sensitivity or local temperature variation, which may indicate inflammation or neurovegetative irritation.
When the pain is specific and well-localized, the therapist guides the hand toward a thoracic segment or an involved intercostal space. But in other, more diffuse or chronic cases, the therapist follows the thread of tissue tension to trace its origin—which may be distant.
Global mobility tests and fascial listening
The assessment isn’t limited to the thorax. The pelvis, lumbar region, diaphragm, stomach, or liver may all be involved. The practitioner tests diaphragmatic mobility during breathing, visceral flexibility at the liver or gastric level, and fascial continuity between the anterior and posterior chains.
Through tissue listening , the therapist perceives areas of hypomobility, density, and coiling. This global perception makes it possible to link localized pain to a broader systemic imbalance: a thorax locked by disturbed digestion, chronic stress, or an imbalance of the pelvic floor.
Towards a functional mapping of the thorax
Following this assessment, the osteopath creates a sort of dynamic map of the thorax: areas of blockage, areas of compensation, points of nervous irritation, and altered breathing patterns. This multidimensional reading serves as a compass for the treatment strategy: should a vertebra be released? An intercostal spasm be released? The diaphragm be worked on? Or a silent visceral tension be lifted?
Osteopathy and Intercostal Neuralgia: Techniques and Therapeutic Approaches

Release the knots, restart the breathing
When faced with intercostal neuralgia, osteopathy offers a fine, individualized approach that respects the body’s rhythm. Far from simple targeted manipulation, osteopathic treatment aims to dissolve the tensions that cause nervous irritation , restore thoracic and spinal mobility, and reintegrate breathing as a central living function . This is in-depth work, which mobilizes not only the manual tool, but also listening, intuition, and understanding of anatomical and emotional interrelationships.
1. Release the fixed thoracic vertebrae and ribs
The first therapeutic intention is often to restore mobility to the vertebral or costovertebral segment in question. Depending on the nature of the dysfunction, the therapist may use:
- Gentle joint techniques (rhythmic mobilizations, decoaptations) to restart vertebral or costal micromovements without shocking the system.
- Myotensive techniques (MET) to correct postural asymmetries and release spasm through gentle muscle contraction.
- Targeted structural manipulations (if the patient tolerates them), to remove a specific blockage responsible for compression of the intercostal nerve.
These techniques are applied with precision, often on the vertebrae from T3 to T9, areas frequently involved in intercostal neuralgia of mechanical origin.
2. Relax the intercostal muscles and thoracic fascia
A key aspect of treatment is to relax the soft tissues surrounding the nerve. The intercostal muscles may be in reflex spasm, either in response to local pain or as a form of postural compensation. The osteopath uses:
- Slow and deep myofascial release techniques to decongest the area and restore flexibility to the intercostal tissue.
- Inhibitory pressures or Jones points (strain-counterstrain) to release hyperalgesic areas.
- Global fascial techniques , particularly anteroposterior traction of the thorax, to restore respiratory coherence and tension balance.
This work is often accompanied by support for the patient’s breathing, who learns to breathe in the painful area to reintegrate it into his proprioception.
3. Release the diaphragm and associated visceral tensions
The diaphragm, the central muscle of respiration, is frequently involved. A spasmed or frozen diaphragm pulls on the lower costal insertions, alters thoracic mechanics, and worsens irritation of the lower intercostal nerves (T8 to T12).
The osteopath mobilizes the diaphragm using subcostal relaxation techniques , also rebalancing its relationships with:
- The liver (right), often congested or twisted.
- The stomach and hiatal region (left), sources of ascending tension.
- The psoas and pillars of the diaphragm, if a posterior tensional chain is involved.
These visceral techniques, often ignored in other approaches, are fundamental in osteopathy to address the root cause of pain.
4. Reintegrate the thorax as a whole
The thorax is a crossroads: mechanical, respiratory, emotional. Chronic intercostal neuralgia often reveals a locking of the thorax as a whole . The osteopath then accompanies the patient towards a broader relaxation, through:
- Craniosacral techniques , which harmonize deep tensions and soothe the autonomic nervous system.
- Work on the anterior and posterior fascial chains , particularly if the patient is in a posture of withdrawal, defense or collapse.
- Tissue listening, which allows you to go to the rhythm of the body, without forcing, by following what the tissues “want to tell”.
5. Work on scars, emotional anchors and tissue memories
When the pain follows surgery or old trauma, the scar sometimes becomes the focus of persistent tension . Through specific work of debonding and integration, the osteopath can help the intercostal nerve regain its normal glide and provide lasting pain relief.
In some cases, the therapist perceives that the intercostal pain carries an emotional charge : an undigested shock, an experienced oppression, a repressed anger. In this case, touch becomes support, a space for repair, and can promote a gentle emotional release, sometimes silent, sometimes verbalized by the patient.
Chronic intercostal neuralgia: unraveling tissue memory
When the body retains the trace of trauma
Chronic intercostal pain often goes beyond simple nervous conflict. When it persists beyond the acute phase, it takes root in the tissues, becomes associated with deep bodily adaptations, and becomes entangled in the patient’s somatic memory. Far from being a simple symptom, it then becomes the silent language of a body that has not been able to release , that remains frozen in a form of protection.
Osteopathy, through its sensitivity to tissue sensations and its global approach, offers a path to reintegrating this pain. It is no longer just a matter of “correcting a lesion”, but of freeing a memory , of listening to a story inscribed in the flesh .
1. Persistent pain: the compensation trap
After an acute phase, the body may continue to protect the painful area through reflex muscle tension, avoidant postures, or voluntary respiratory limitation. These defense mechanisms, initially useful, become harmful if they become established: they maintain hypomobility of the thorax , prevent nerve gliding, and fuel a vicious cycle of pain, stiffness, and apprehension.
The patient then lives in anticipation of the next “painful peak,” monitors their movements, and reduces their physical exertion. This hypervigilance of the body promotes the perpetuation of neuralgia, even in the absence of an active lesion.
2. Scars, witnesses of an ancient conflict
A surgical scar (such as a cesarean section, mastectomy, thoracic or digestive surgery) is much more than just a mark on the skin. It can act as a real tissue anchor , disrupting fascial glide, stiffening mobility chains, and capturing undigested traumatic memory.
The intercostal nerve, when it crosses or runs along a scarred area, can become fixed, stretched, or simply irritated during movement. The osteopath, through fine work of desensitization and tissue release, can thus restore freedom to the nerve and the emotional tissue it contains .
3. Intercostal pain and emotional memory
The thorax, the seat of the heart and breathing, is also the seat of “contained,” “repressed,” “silenced” emotions. Many patients describe their chronic intercostal pain as oppression , a vice , or a breathlessness . These words often reflect a deep emotional reality: shock, fear, anger, or unexpressed pain.
The body then becomes the silent receptacle of what words could not say. Intercostal neuralgia becomes a symptom of the unexpressed , an attempt by the body to regulate an emotional excess lodged in the tissues.
Osteopathy does not replace psychotherapeutic speech, but it can be a bodily complement to it. Through respectful touch, through silent listening to frozen areas, it sometimes allows a gentle, non-verbal, but transformative release.
4. The biodynamic approach: supporting reintegration
In the oldest, most subtle cases, it is the biodynamic approach of osteopathy that finds its full relevance. It does not seek to force, but to listen to the deep rhythms of the body , to follow the involuntary movements of internal reorganization. The osteopath then accompanies the patient towards a reintegration of the injured area, without imposing anything.
The tissues speak, relax, sometimes open up to a forgotten memory. The pain, which seemed trapped in an infinite loop, can gradually dissolve into the regained movement , the redeployed breathing, the reinvested body image.
5. When the patient regains his chest… and his breath
As the sessions progress, a striking phenomenon occurs: the patient regains control of his thorax . He straightens up, breathes more fully, and moves without fear. The intercostal nerve, now freed, stops sending warning signals. But even more, it is the experience of the entire body that changes : the thorax is no longer a place of pain, but a living center of breathing, emotion, and movement.
Summary of scientific studies on the benefits of osteopathic treatment
Scientific studies show that osteopathy is an effective method for treating intercostal neuralgia, which manifests as sharp pain along the intercostal nerves. This approach helps relieve pain by working on the musculoskeletal structures and improving thoracic mobility.
The main osteopathic techniques used to treat intercostal neuralgia include:
- Structural manipulations : Correction of costal and vertebral joint restrictions.
- Visceral techniques : Release of diaphragmatic tension and improvement of thoracic mobility.
- Myofascial techniques : Relaxation of the intercostal muscles and associated thoracic structures.
Studies show significant improvement in pain, thoracic mobility and quality of life for patients, often after just a few sessions.
Key study
Title: “Benefits of structural osteopathic treatment in the context of common back pain”
Link: Download the study (PDF)
Abstract: This study led by Guillou Bastien explores the benefits of structural osteopathic treatment for common back pain, including associated intercostal neuralgia. The study concludes that patients with chronic intercostal pain experience significant improvements in their pain and thoracic mobility following a treatment protocol.
Other relevant studies
Evaluation of the effectiveness of the practice of osteopathy
- Auteurs : Caroline Barry, Bruno Falissard
- Publication: INSERM U669, 2012
- Abstract:
This study explores the effectiveness of osteopathic practices in the treatment of musculoskeletal disorders, including chest pain and intercostal neuralgia. The results show significant improvements in pain, mobility, and quality of life after regular osteopathic sessions. - Link: Download the study (PDF)
Doctors and Structural Osteopathy: Analysis of the effects of structural treatments on intercostal disorders
- Author: Clarisse Langevin
- Publication: End of studies dissertation, 2023
- Abstract:
This study analyzes the effects of osteopathic structural techniques on intercostal disorders and chronic chest pain. The results demonstrate that structural techniques targeting rib and vertebral dysfunctions provide significant improvements in pain and mobility. - Link: Download the study (PDF)
Comparative analysis of the main indications for osteopathy mentioned by general practitioners and the three main osteopathy professionals
- Author: G. Humbert
- Publication: University of Lorraine, 2015
- Abstract:
This analysis highlights the main indications for osteopathy identified by general practitioners and osteopaths, including the treatment of chest pain and intercostal neuralgia. The study concludes that osteopathy is perceived as an effective alternative for treating these pathologies. - Link: Download the study (PDF)
Clinical evaluation of the effects of myofascial and structural techniques in the treatment of chest pain
- Author: Aline Mouchet
- Publication: University of Lorraine, 2015
- Abstract:
The study compared the effectiveness of myofascial and structural techniques in relieving mechanical chest pain, including intercostal neuralgia. The results showed rapid improvement in pain in patients treated with a combined approach. - Link: Download the study (PDF)
Place and needs of manual medicine-osteopathy in the practice of general practitioners in the Army Health Service
- Author: Mr. Sahut
- Publication : CORE, 2015
- Abstract:
This study explores the role of osteopathy in the medical practices of the Army Health Service and its effects on chest pain. Osteopathy is perceived as an effective alternative, especially in the treatment of persistent musculoskeletal pain, including intercostal pain. - Link: Download the study (PDF)
Clinical approach and diagnosis in physiotherapy: Contribution of osteopathy in the management of chest pain
- Authors: M. Dufour, S. Tixa, SDV Acedo
- Publication : Elsevier, 2024
- Abstract:
This manual examines the contributions of osteopathy in the treatment of chest pain and intercostal neuralgia. The analysis highlights the positive results achieved through structural and visceral techniques targeting areas of dysfunction. - Link: Access the book
Osteopathy: The foundations, techniques and 100 exercises to practice daily
- Authors : H. Caure, P. Pilate
- Publication: Odile Jacob, 2015
- Summary:
This guide offers a detailed analysis of osteopathic techniques applied to chest pain, including intercostal neuralgia, with positive results demonstrated by clinical studies. - Link: Access the book
The Guide to Osteopathy: 2017 Edition
- Author: G. Mondoloni
- Publication: 2017, Edition Odile Jacob
- Abstract:
This guide highlights the applications of osteopathy for the treatment of musculoskeletal pain, including chest pain associated with intercostal neuralgia. It provides a summary of effective manual techniques validated by clinical studies. - Link: Access the book
Treating yourself with osteopathy
- Author: G. Mondoloni
- Publication: 2006, Odile Jacob
- Summary:
The book analyzes the benefits of osteopathy for the management of chronic pain, with a specific section dedicated to chest pain and intercostal neuralgia. - Link: Access the book
Self-management and prevention advice
Breathe, stretch, reclaim your thorax
Osteopathic support does not stop at the treatment table. To consolidate the effects of the session, prevent recurrences and promote greater patient autonomy, it is essential to offer simple, adapted and body-friendly gestures . These tools allow the patient to regain confidence in their thorax , to regain fluid breathing, and to break out of the pain-protection-inhibition cycle.
1. Relearn to breathe fully
Breathing is often impaired in patients with intercostal neuralgia. It becomes high, shortened, and held. However, free breathing is one of the best natural therapies for the rib cage. Here are some simple exercises:
- Conscious breathing in the supine position: Lying on their back, one hand on their chest and the other on their abdomen, the patient observes their breathing without controlling it, then seeks to release tension as they exhale. This awareness is often the first step toward returning to smooth breathing.
- Targeted lateral breathing: Sitting or standing, the patient places their hands on the lateral ribs. They inhale gently, sending the air towards their hands, as if opening an accordion. This mobilizes the intercostal muscles and restarts rib mechanics.
- 4-beat breathing (inhalation – pause – exhalation – pause): this exercise sets the rhythm of breathing, soothes the nervous system, and promotes relaxation of the diaphragm.
2. Gentle stretches of the chest and intercostal spaces
The intercostal muscles need to regain their elasticity. We will favor slow, progressive movements, without forcing:
- Side bend stretch: Standing or sitting, arm raised, bend your torso to the side opposite the pain, without going all the way to the painful area. Hold for 20 to 30 seconds, breathe into the stretch, release.
- Sphinx pose or gentle chest extension: Lie on your stomach, leaning on your forearms, and gently open your chest. This exercise improves back extension and promotes oxygenation.
- Gentle trunk rotation: In a seated position, with your hands crossed over your shoulders, rotate your upper body from right to left. This promotes thoracic rotational mobility and loosens the rib attachments.
3. Self-massage and gentle myofascial release
Some patients benefit from self-massage with a tennis ball or foam roller along the paraspinal muscles or under the posterior ribs. It’s important to keep this painless and comfortable. This type of self-stimulation improves proprioception and releases local tension.
4. Postural precautions and healthy lifestyle
Some simple tips to avoid recurrences:
- Avoid prolonged thoracic flexion positions (in front of a computer, while driving), without breaks.
- Raise screens to eye level , limit repeated twisting.
- Support the arm on the painful side when carrying loads or performing repetitive movements .
- Favor sleeping in a side position with a pillow under your arm to avoid tension on the rib cage.
5. Stress management and relaxation
Since the thorax is a common area of somatization, incorporating stress management techniques is valuable. Meditation, cardiac coherence, gentle yoga, or sophrology can soothe the nervous system, release tension, and support osteopathic work.
6. When to consult again?
A patient who is aware of their feelings will be able to recognize the signs of recurrence. It is recommended to consult again if:
Significant stress or postural change seems to awaken the sensitive area.
The pain persists despite the exercises after two weeks.
Breathing discomfort or chest blockage reappears.
Clinical cases: from gripping pain to liberation
Stories of locked chests finding their breath again
Clinical cases powerfully illustrate the diversity of causes and expressions of intercostal neuralgia . Each patient brings a unique configuration: posture, life story, history, suppressed emotions or forgotten injuries. Osteopathy, through its individualized approach, allows for the adjustment of care to the body’s experience , beyond the simple symptom. Here are three significant cases.
Case 1: Nathalie, 42 years old – Post-surgical pain and shortness of breath
Nathalie, a teacher, presented with right chest pain that began three months after a cesarean section. She described a pulling sensation under her ribs, as if something had gotten stuck. The pain intensified at the end of the day and made it difficult to breathe deeply.
Assessment:
Low scar adherent to the abdominal wall, limited mobility of the last right ribs, spasmed diaphragm. The right T8-T9 intercostal space is hyperalgesic. The liver is slightly ptotic.
Osteopathic approach:
- Gentle scar release using fascial techniques.
- Mobilization of the diaphragm and lower ribs.
- Hepatic visceral normalization.
- Guided conscious breathing reintegration.
Result:
After three sessions spaced two weeks apart, the pain disappeared. Nathalie happily resumed yoga and reported a “more alive chest.”
Case 2: Karim, 55 years old – False angina and lateralized pain
Karim arrives at the emergency room, concerned about a sudden onset of chest pain in his left chest after lifting a heavy load. Cardiac tests are normal. He then consults an osteopath, still experiencing sharp pain when inhaling.
Assessment:
Left T5 costovertebral block, intercostal spasm, loss of scapular mobility. Pain reproduced on palpation is located in the left intercostal space. Breathing limited by apprehension.
Osteopathic approach:
- Gentle decompression of the affected thoracic segment.
- Targeted muscle inhibition of the intercostals.
- Passive stretching of the thorax in a lateral position.
- Progressive breathing work.
Result:
Immediate relief after the first session. Two additional follow-ups allow for complete recovery of mobility and a reduction in associated anxiety.
Case 3: Chantal, 38 years old – Unexplained chronic pain and emotional stress
Chantal, a nurse, has been suffering from right chest pain for over a year, with no known organic cause. She has seen several specialists and taken anti-inflammatory medications without success. She describes the pain as “squeezing” and “relentless.” The interview reveals a traumatic episode she experienced at work a few months before the pain began.
Assessment:
Rigidity of the entire right hemithorax, blocked breathing, diaphragm spasm. No specific spinal pain, but diffuse tension. Tissue examination reveals deep fascial wrapping.
Osteopathic approach:
- Gentle craniosacral work.
- Global fascial release techniques.
- Minimal verbal support in a security posture.
- Progressive integration of respiratory movement.
Result:
In the third session, Chantal evokes an old, unexpressed fear. A gentle emotional release accompanies the return of her breath. Two sessions later, the pain has almost disappeared. She describes a “general calming” and resumes swimming.
These cases demonstrate that intercostal neuralgia is never just a symptom : it reveals a deeper, often multifactorial imbalance. Osteopathy, through its keen listening, respectful touch, and holistic vision, allows for an approach tailored to each pain pathway.
Conclusion: Behind every intercostal pain, a message to decipher
Intercostal neuralgia, seemingly localized, is in reality a complex signal emitted by a body out of balance. It is one of those pains that confuses both the patient and the caregivers: too clear to be ignored, but too vague to be easily linked to an obvious organic cause. Yet, to those who know how to listen, it reveals much more than nervous irritation. It is the reflection of a tissue, functional, sometimes emotional knot , that osteopathy, in its holistic vision, can gradually unravel.
In osteopathic medicine, we do not seek to “make the pain disappear” as we would turn off an annoying alarm. We seek to understand why the body has sounded this alert, where the imbalance lies, what memory or old tension is replaying itself through this peripheral neurological complaint . The osteopath therefore does not intervene against the pain, but with it – taking it as the starting point for a tissue investigation, sometimes organic, sometimes symbolic.
Each intercostal neuralgia is different. In one, it will be the mechanical consequence of a clear vertebral blockage. In another, it will be rooted in a forgotten scar, chronic unexpressed stress, a posture contracted for years. Chest pain then becomes the mask of an older story , sometimes silent, sometimes buried. In all cases, it questions breathing, the mobility of the heart, the emotional space we give ourselves—or that we deny ourselves.
The osteopathic approach connects these dimensions. Through touch, it restores the mechanical mobility of the ribs, vertebrae, and diaphragm. Through listening, it invites the patient to reintegrate their thorax, often experienced as rigid, closed, and protective. And through silent presence, it opens a therapeutic space in which the body can release what it is holding onto: tension, memory, fear.
When pain settles in the thorax, it is often the breath itself that retracts. The patient is afraid to breathe, to move, to open the injured area. He withdraws into himself, in a form of rigid protection. The osteopath then accompanies a process of reopening , gently, through breathing, the sensory reconquest of the thorax, the re-establishment of movement of the intercostal spaces. He helps to reconnect the patient to this central area of the body – that of the heart, of rhythm, of the inner connection.
But there is no one-size-fits-all solution. Some patients will need a simple joint correction procedure. Others will need time, patience, and more comprehensive support, perhaps including additional psycho-corporal work. The key is to recognize that intercostal pain is not a “problem to be solved,” but a bodily experience to be worked through , a message to be deciphered.
So, osteopathy does not promise immediate healing, but the beginning of a path . A path towards more fluidity, self-awareness, confidence in one’s sensations. And sometimes, when the knot loosens, the breath returns. This breath which circulates again in the thorax, like a silent word from the body which finally says: “I can breathe.”
Scientific Sources to Explore the Subject in More Detail
Scientific and clinical references
- Standring S. (Ed.). Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Elsevier, 2020.
→ Major anatomical reference for the courses of the intercostal nerves, relationships to the ribs, muscles, and thoracic viscera. - Netter FH Atlas of Human Anatomy. Ed. Masson, 7th edition, 2019.
→ Clear visualization of the intercostal structures and myofascial insertions involved. - Busch H. et al. (2019). “Intercostal Neuralgia: A Diagnostic and Therapeutic Challenge.” Pain Physician , 22(6), 551-558.
→ Article on clinical forms of intercostal neuralgia, diagnostic pitfalls, and management strategies. - Dommerholt J., Fernández-de-las-Peñas C. Myofascial Pain and Dysfunction: The Trigger Point Manual. Elsevier, 2013.
→ References on thoracic myofascial pain, intercostal trigger points and their manual treatment. - Chaitow L., DeLany J. Clinical Application of Neuromuscular Techniques: Volume 2 – The Lower Body. Churchill Livingstone, 2008.
→ Osteopathic and integrative approach to neuromuscular pain, including fascial release techniques.
Research and publications in osteopathy
- Thomson OP, Petty NJ, Moore AP (2011). “Osteopaths’ Use of Techniques: A National Survey of United Kingdom Practitioners.” International Journal of Osteopathic Medicine , 14(1), 11–19.
→ Study on the most commonly used osteopathic techniques, particularly in chest pain. - Degenhardt BF, Johnson JC, Fossum C. (2010). “Osteopathic Treatment and Its Relationship to Autonomic Nervous System Activity as Demonstrated by Heart Rate Variability: A Repeated Measures Study.” Journal of Bodywork and Movement Therapies , 14(3), 281–291.
→ Research on the impact of osteopathic treatment on the autonomic nervous system, useful for understanding the effects on thoracic stress. - Licciardone JC (2005). “Osteopathic Manual Treatment in Patients with Chronic Low Back Pain: A Randomized Controlled Trial.” The New England Journal of Medicine , 352(5), 511–519.
→ Although focused on low back pain, this study supports the effectiveness of osteopathy on chronic pain of multifactorial origin. - Henley CE, Ivins D., Mills M., Wen FK, Benjamin BA (2008). “Osteopathic Manipulative Treatment and Its Relationship to Measures of Pain and Function in Patients with Chronic Low Back Pain.” Journal of the American Osteopathic Association , 108(8), 387–393.
→ Data extrapolable to chronic chest pain, within the framework of a whole-tissue approach.
Additional sources on the psychosomatic and tissue dimension
- Scaer RC The Body Bears the Burden: Trauma, Dissociation, and Disease. Routledge, 2nd ed., 2005.
→ Link between past trauma, chronic pain and body memory. - van der Kolk B. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Penguin Books, 2014.
→ Exploration of how stress and emotional trauma imprint themselves on the body, including the chest. - Gehin M., Le Corre A. Osteopathic treatment of the thorax. Éditions Sully, 2016.
→ Essential French-language work for osteopathic reading of the thorax and intercostal pain.





")







")




{kind=link}