

In a SLAP lesion, the upper (superior) portion of the labrum is injured. This upper area is also where the biceps tendon is attached. A SLAP tear occurs both in front (anterior) and behind (posterior) of this attachment point.
Introduction
In the shoulder, the superior labral complex is made up of the biceps tendon and a meniscus-like tissue called the labrum. Together, these components help stabilize the shoulder joint during overhead activities. In the mid-1980s, the labral complex was identified as a possible source of shoulder pain and dysfunction in throwing athletes. Since then, numerous reports have provided a better understanding of this complex structure and helped orthopedic surgeons properly treat these “SLAP” lesions.
SLAP injuries are usually caused by falling onto an outstretched arm, repeated throwing, or traumatic shoulder dislocations. Damaging force, whether all at once or over time, causes this stable anchoring complex to loosen and become painful.
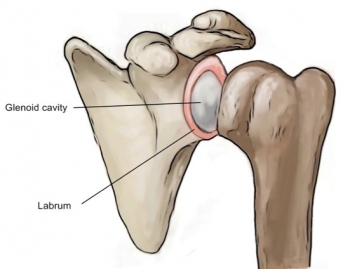
The shoulder joint (humeral head) is like a golf ball placed on a golf tee, which is the glenoid fossa. If the labrum is torn, it is more difficult for the humerus to stay in the socket. The end result is that the shoulder joint becomes unstable and prone to injury.
Because the biceps tendon attaches to the scapula through the labrum, labral tears can occur when you put extra pressure on the biceps muscle, such as when throwing a ball. Tears can also result from pinching or compression of the shoulder joint when the arm is raised above the head.

Causes of a SLAP lesion
SLAP lesions, or lesions of the upper anterior portion of the glenoid labrum, can be caused by a variety of factors. The main causes include acute trauma, repetitive movements, anatomical abnormalities and joint instability.
Acute trauma, such as a direct fall onto the shoulder or violent impact, can result in a tear of the labrum at its junction with the biceps brachii tendon, thereby causing a SLAP injury. These traumatic events can place excessive force on the shoulder joint, damaging the labrum and compromising its stabilizing function.
Sports or work activities that involve repetitive movements of the shoulder, such as throwing in baseball or throwing motions in athletes, may also contribute to the development of a SLAP injury. Repetition of these movements can cause progressive wear of the labrum, increasing the risk of tearing and injury.
Congenital or acquired anatomical abnormalities may also play a role in the development of a SLAP lesion. Some individuals may have anatomical defects, such as an abnormal shape of the glenoid fossa or poor healing of the labrum, that predispose them to this injury. These abnormalities can compromise the stability of the shoulder joint, thereby increasing susceptibility to labrum injuries.
Shoulder joint instability, whether congenital or acquired from previous injuries, is also a common cause of SLAP injury. Chronic joint instability can place additional stress on the labrum, increasing the risk of tearing and injury.
- Acute Trauma: Sudden trauma, such as a direct fall on the shoulder, a sports collision, or an accident, can cause a tear of the upper labrum of the shoulder.
- Repetitive arm movements: Activities that involve repetitive movements of the arm overhead, such as throwing in certain sports like baseball or softball, can contribute to labrum wear and SLAP injury.
- Shoulder Instability: Chronic shoulder instability, where the head of the humerus may move abnormally within the joint, increases the risk of developing a SLAP injury.
- Degenerative processes: Natural aging and degenerative processes can weaken the labrum over time, increasing susceptibility to injury.
- Throwing Sports: Athletes participating in throwing sports, such as baseball, softball, or tennis, are at particular risk for SLAP injury due to the repetitive movements involved in these activities.
- Heavy Lifting Activities: Heavy lifting activities, especially those involving raising the arm above the head with heavy loads, can contribute to wear and tear of the labrum and the development of SLAP injury.
- Anatomical factors: Some individuals may have anatomical factors predisposing to a SLAP injury, such as an abnormal shape of the acromion (part of the shoulder blade) or variations in shoulder structure.
- Poor exercise technique: Poor exercise technique, especially during movements that place heavy strain on the shoulder, can contribute to the occurrence of a SLAP injury.
Symptoms of a SLAP injury
Symptoms of a SLAP injury can vary depending on the severity of the injury and how it affects shoulder function. Here are some of the most common symptoms associated with a SLAP injury:
Pain : Pain is one of the most common symptoms of a SLAP injury. It is usually felt deep in the shoulder and may be described as a dull or stabbing pain. The pain may be exacerbated by certain activities, such as raising your arm above your head or performing rotating movements.
Locking or blocking sensation : People with a SLAP injury may feel a locking or blocking sensation in the shoulder when they try to raise their arm or move it in certain directions. This sensation may be due to joint instability caused by the labrum injury.
Muscle weakness : A SLAP injury can lead to muscle weakness in the affected shoulder, especially during specific movements. The muscles surrounding the shoulder may not function properly due to joint instability or pain, which can limit the shoulder’s range of motion and strength.
Crepitus or clicks : Some people with a SLAP injury may hear or feel crepitus or click sensations when they move their shoulder. This may be due to abnormal friction of the joint surfaces due to instability caused by the labrum injury.
Restriction of mobility : A SLAP injury can cause restriction of shoulder mobility, especially when raising the arm above the head or moving it in certain directions. This mobility limitation may be due to pain, joint instability, or a combination of both.
Shoulder instability : A SLAP injury can also lead to a feeling of shoulder instability, where the person feels like the shoulder is likely to dislocate or dislocate during certain activities. This instability may be accompanied by pain and muscle weakness.
A Day in the Life of Someone Suffering from a SLAP Lesion
6:30 AM: A Painful Start
Lena, a 30-year-old physical therapist, begins her day with a familiar ache in her left shoulder. Diagnosed with a SLAP (Superior Labral Anterior and Posterior) lesion, Lena experiences a persistent, sharp pain that often worsens in the morning. The injury, which affects the labrum, the cartilage that stabilizes the shoulder joint, can make even simple movements challenging. She gently stretches her shoulder and applies a cold pack, hoping to ease the discomfort before starting her day.
7:00 AM: Adjusting the Morning Routine
Lena’s morning routine is carefully adjusted to accommodate her shoulder pain. Dressing requires a cautious approach, as lifting her arm too high can trigger sharp pangs. She opts for loose-fitting clothing that’s easier to manage. Breakfast is prepared with minimal movement; she uses tools and appliances that allow her to operate without extensive shoulder use. Despite these modifications, the morning remains a struggle as Lena copes with the constant ache and limited mobility.
8:00 AM: The Commute
Driving to work is a slow and deliberate process for Lena. She uses an ergonomic seat cushion to reduce strain on her shoulder and adjusts the car’s seat to find a comfortable position. The commute, though brief, is uncomfortable due to the extended periods of holding the steering wheel and operating the gear shift. Lena takes regular breaks to stretch and shift her arm positions, trying to mitigate the pain and stiffness that accumulate during the drive.
9:00 AM: Working with Limitations
At the clinic, Lena’s role as a physical therapist is both a source of pride and a challenge. The demands of her job, which include demonstrating exercises and assisting patients, often exacerbate her shoulder pain. She has to carefully select and modify her treatment techniques to avoid aggravating her SLAP lesion. Lena collaborates with colleagues to delegate tasks that involve heavy lifting or overhead movements, ensuring she can still contribute effectively while managing her own condition.
12:00 PM: Managing Pain During Lunch
Lunchtime offers a brief respite from the demands of her job. Lena uses this time to rest her shoulder and apply a heat pack, which helps to relax the muscles and soothe the pain. She avoids activities that involve lifting or reaching, focusing instead on a light meal and gentle stretches. Conversations with colleagues often turn to her injury, and while their support is appreciated, Lena is conscious of not letting her condition define her interactions.
2:00 PM: Afternoon Fatigue
By the afternoon, Lena finds her shoulder pain increasing. The combination of repetitive movements and sustained postures takes its toll. She takes periodic breaks to perform stretching exercises and consults with a specialist for any adjustments to her rehabilitation plan. Her focus on patient care remains strong, but she must continuously manage her own discomfort, which can be mentally and physically draining.
5:00 PM: Heading Home
The commute home is as challenging as the morning drive. Lena is careful to avoid abrupt movements and takes breaks to stretch her arm and shoulder. Once home, she immediately applies ice to her shoulder to reduce swelling and discomfort. Lena takes time to unwind, focusing on activities that require minimal shoulder engagement, such as reading or watching TV.
7:00 PM: Evening Physical Therapy
In the evening, Lena dedicates time to her own physical therapy exercises. These exercises are crucial for maintaining her shoulder’s range of motion and strength, even though they can be uncomfortable. Lena follows a tailored program designed by her therapist, incorporating gentle stretches and strengthening exercises. This routine helps her manage pain and improve function, offering hope for eventual recovery.
9:00 PM: Relaxing and Reflecting
As bedtime approaches, Lena takes time to relax and reflect on her day. She performs some mindfulness techniques to manage stress and prepare for restful sleep. Arranging her pillows to support her shoulder and adopting a comfortable sleeping position helps alleviate some of the pain. Despite the challenges, Lena remains optimistic about her recovery and is determined to manage her SLAP lesion with resilience and patience.
11:00 PM: Preparing for Tomorrow
Before falling asleep, Lena reviews her day and plans for the next. Managing a SLAP lesion requires constant vigilance and adaptation, but she remains hopeful. Each day is a testament to her strength and determination, and she looks forward to the gradual improvement of her condition, knowing that perseverance and care are key to her recovery.
Pathophysiology of a SLAP lesion
The pathophysiology of a SLAP (Superior Labral Anterior to Posterior) lesion of the shoulder involves an alteration of the labrum, a cartilaginous structure located in the shoulder joint. This injury can result from a variety of factors and cause changes to the shoulder, affecting its stability and causing symptoms. Here is an overview of the pathophysiology associated with SLAP injury:
- Labrum Tear: SLAP injury usually involves a tear of the labrum, the portion of cartilage that surrounds the glenoid socket of the scapula. This tear can occur as a result of acute trauma, overuse, or age-related degenerative processes.
- Traumatic Mechanisms: Acute trauma, such as a fall on the shoulder or a collision, can cause a tear of the labrum. The impact forces the joint into extreme positions, potentially leading to tears.
- Overuse or Repetitive Movements: Repetitive overhead arm movements, often associated with throwing sports like baseball, can contribute to progressive wear and tear of the labrum. This can create cumulative microtrauma leading to the SLAP injury.
- Shoulder Instability: Chronic shoulder instability, where the head of the humerus does not remain securely in the joint, can cause abnormal stress on the labrum, promoting tears.
- Compression and Pinching: Certain specific movements, such as forced abduction of the arm or rotational movements, can compress and pinch the labrum, contributing to its wear and tear.
- Deficient Healing Processes: The labrum has a limited ability to heal itself due to its limited blood supply. Therefore, a labrum tear can persist and lead to chronic problems.
- Abnormal Humeral Head Displacement: When unstable, the head of the humerus may move abnormally within the joint, generating inadequate forces on the labrum and thus contributing to the injury.
- Inflammatory Response and Pain: Tearing the labrum triggers an inflammatory response, causing pain and discomfort. Nerves in the area may be stimulated, causing symptoms such as pain, numbness, or a feeling of blockage.
The mechanism of injury in the case of a SLAP (Superior Labral Anterior to Posterior) lesion of the shoulder is often complex and can vary depending on several factors, including the type of physical activities performed, the movements repetitive stress, trauma and individual anatomical characteristics. Let us explore in detail the main mechanisms involved in the occurrence of SLAP injury.
Mechanism of injury
- Acute Trauma: A common mechanism of SLAP injury is acute trauma, such as a direct fall onto the shoulder or a violent collision. In such incidents, the force applied to the shoulder can cause abnormal movements of the humeral head, thereby putting the superior labrum in a vulnerable position. Tearing may occur as a result of this trauma, compromising the integrity of the labrum.
- Repetitive Throwing Motions: Athletes involved in throwing sports, such as baseball, softball, or tennis, are particularly susceptible to developing a SLAP injury due to repetitive overhead arm movements. Throwing movements exert significant pressure on the shoulder, repeatedly straining the labrum. Over time, these repeated stresses can contribute to wear and tear of the labrum and eventually injury.
- Compression and Pinching: Certain specific movements, such as forced abduction of the arm or rotational movements, can result in compression and pinching of the superior labrum between the humeral head and the glenoid fossa. This mechanism can damage the labrum and lead to a SLAP lesion.
- Shoulder Instability: Chronic shoulder instability, where the head of the humerus has excessive mobility in the joint, can contribute to SLAP injury. This instability may result from previous trauma, ligamentous laxity, or other anatomical abnormalities. An unstable humeral head can exert abnormal forces on the labrum, leading to a tear.
- Deficient Healing Processes: The labrum has limited vascularity, which means it has limited healing capacity. In the event of a tear, the ability of the labrum to regenerate is restricted. Degenerative processes and lack of adequate healing may contribute to the persistence of the SLAP lesion.
- Shoulder Hyperextension: Certain movements, such as shoulder hyperextension, can also contribute to SLAP injury. When the occiput and cervical vertebrae are extended posteriorly, this can place additional pressure on the shoulder structures, including the labrum.
- Improper Exercise Technique: Improper exercise technique, particularly during lifting movements or intensive upper extremity training, can result in inappropriate stresses on the shoulder, contributing to the development of a SLAP injury.
- Anatomical Factors: Some individuals may have anatomical factors predisposing to a SLAP injury, such as an abnormal shape of the acromion or variations in shoulder structure. These anatomical features may increase the vulnerability of the labrum to injury.
Exercice routine
For managing a SLAP (Superior Labral Anterior to Posterior) lesion, focusing on strengthening and stretching specific shoulder muscles can help improve stability, support, and overall function. Here’s a routine for strengthening and stretching the muscles involved:
Strengthening Exercises
- External Rotator Cuff Strengthening
- Exercise: Side-lying external rotation
- How to do it: Lie on your side with your affected shoulder on top. Hold a light dumbbell in the top hand, keeping the elbow bent at 90 degrees. Rotate the arm outward, lifting the dumbbell towards the ceiling, then slowly lower it back down.
- Reps/Sets: 3 sets of 10-15 reps
- Internal Rotator Cuff Strengthening
- Exercise: Internal rotation with resistance band
- How to do it: Attach a resistance band to a fixed point at waist height. Stand with your affected side closest to the band. Hold the band with the elbow bent at 90 degrees and rotate the forearm towards your body. Return to the starting position slowly.
- Reps/Sets: 3 sets of 10-15 reps
- Scapular Stabilization
- Exercise: Scapular push-ups
- How to do it: Get into a plank position with your arms straight. Instead of bending your elbows, focus on moving your shoulder blades together and apart, allowing your chest to sink towards the floor and then pushing away.
- Reps/Sets: 3 sets of 12-15 reps
- Shoulder Abduction
- Exercise: Lateral raises
- How to do it: Stand with feet shoulder-width apart and hold light dumbbells by your sides. Keeping your arms straight, lift the dumbbells out to the sides until shoulder height, then slowly lower them back down.
- Reps/Sets: 3 sets of 10-12 reps
- Rotator Cuff Strengthening
- Exercise: Prone horizontal abduction
- How to do it: Lie face down on a bench or bed with arms hanging off the edge. Hold light dumbbells and lift your arms out to the sides, squeezing your shoulder blades together. Lower the weights back slowly.
- Reps/Sets: 3 sets of 10-12 reps
Stretching Exercises
- Posterior Shoulder Stretch
- How to do it: Sit or stand upright. Cross the affected arm over your chest, using the opposite hand to pull the arm closer to your chest. Hold for 20-30 seconds.
- Reps/Sets: 3 times on each side
- Anterior Shoulder Stretch
- How to do it: Stand in a doorway with your elbow bent at 90 degrees and your forearm against the door frame. Gently lean forward until you feel a stretch in the front of your shoulder. Hold for 20-30 seconds.
- Reps/Sets: 3 times on each side
- Sleeper Stretch
- How to do it: Lie on your side with the affected shoulder down. Use your top hand to gently push your affected arm down towards the floor, feeling a stretch in the back of the shoulder. Hold for 20-30 seconds.
- Reps/Sets: 3 times on each side
- Cross-body Shoulder Stretch
- How to do it: Bring one arm across your chest and use the opposite hand to gently pull the arm closer to your chest. You should feel a stretch across the back of the shoulder. Hold for 20-30 seconds.
- Reps/Sets: 3 times on each side
- Latissimus Dorsi Stretch
- How to do it: Stand with your feet shoulder-width apart and reach one arm overhead, bending slightly to the opposite side. Hold the stretch for 20-30 seconds, feeling the stretch along the side of your torso and shoulder.
- Reps/Sets: 3 times on each side
Routine Overview
- Warm-up: 5-10 minutes of light cardio (e.g., walking or cycling) to get the blood flowing to the shoulder.
- Strengthening Exercises: Perform 3 sets of each strengthening exercise, with 10-15 reps per set.
- Stretching Exercises: Hold each stretch for 20-30 seconds, repeating 3 times on each side.
- Cool-down: Gentle stretching and relaxation exercises to help your muscles recover.
Always consult with a healthcare professional before starting any new exercise routine, especially if you have a SLAP lesion or other shoulder issues. They can provide personalized recommendations and ensure that exercises are performed safely and effectively.
Conclusion
The superior labral complex plays a crucial role in stabilizing the shoulder joint, particularly during overhead activities. As a key component of the shoulder’s anatomical integrity, the labrum, along with the biceps tendon, supports the humeral head within the glenoid fossa, preventing instability and discomfort. The identification of SLAP (Superior Labral Anterior to Posterior) lesions in the mid-1980s has significantly advanced our understanding of shoulder pathologies, especially in athletes who are prone to these injuries due to repetitive strain or acute trauma.
SLAP lesions, which involve tears to this essential cartilage ring, disrupt the delicate balance that maintains joint stability. Whether caused by acute trauma, repetitive overhead movements, or congenital abnormalities, these injuries compromise the shoulder’s ability to function effectively, leading to pain, weakness, and instability. The various mechanisms contributing to SLAP lesions, from direct impacts to chronic overuse, highlight the complex interplay of forces affecting the shoulder joint.
Understanding the pathophysiology of SLAP lesions emphasizes the importance of both prevention and treatment. Addressing contributing factors such as improper technique, anatomical predispositions, and repetitive stress can mitigate the risk of injury. Moreover, advancements in diagnostic techniques and treatment strategies continue to enhance the management of SLAP injuries, enabling better outcomes for affected individuals. As our knowledge of the superior labral complex deepens, we move closer to optimizing care and restoring function to those impacted by this challenging shoulder condition.
References
- Andrews JR, Carson WG, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985 Sep-Oct;13(5):337-41. [ PubMed ]2.
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-9. [ PubMed ]3.
- Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998 Sep;14(6):553-65. [ PubMed ]4.
- Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med. 1995 Jan-Feb;23(1):93-8. [ PubMed ]5.
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20. [ PubMed ]6.
- Kuhn JE, Lindholm SR, Huston LJ, Soslowsky LJ, Blasier RB. Failure of the biceps superior labral complex: a cadaveric biomechanical investigation comparing the late cocking and early deceleration positions of throwing. Arthroscopy. 2003 Apr;19(4):373-9. [ PubMed ]7.
- Clavert P, Bonnomet F, Kempf JF, Boutemy P, Braun M, Kahn JL. Contribution to the study of the pathogenesis of type II superior labrum anterior-posterior lesions: a cadaveric model of a fall on the outstretched hand. J Shoulder Elbow Surg. 2004 Jan-Feb;13(1):45-50. [ PubMed ]8.
- Erickson BJ, Jain A, Abrams GD, Nicholson GP, Cole BJ, Romeo AA, Verma NN. SLAP Lesions: Trends in Treatment. Arthroscopy. 2016 Jun;32(6):976-81. [ PubMed ]9.
- Clavert P. Glenoid labrum pathology. Orthop Traumatol Surg Res. 2015 Feb;101(1 Suppl):S19-24. [ PubMed ]10.
- Kampa RJ, Clasper J. Incidence of SLAP injuries in a military population. JR Army Med Corps. 2005 Sep;151(3):171-5. [ PubMed ]11.
- Waterman BR, Cameron KL, Hsiao M, Langston JR, Clark NJ, Owens BD. Trends in the diagnosis of SLAP lesions in the US military. Knee Surg Sports Traumatol Arthrosc. 2015 May;23(5):1453-1459. [ PubMed ]12.
- Weber SC, Martin DF, Seiler JG, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012 Jul;40(7):1538-43. [ PubMed ]13.
- Rossy W, Sanchez G, Sanchez A, Provencher MT. Superior Labral Anterior-Posterior ( SLAP ) Tears in the Military. Sports Health. 2016 Nov/Dec;8(6):503-506. [ PMC free article ] [ PubMed ]14.
- Waterman BR, Arroyo W, Heida K, Burks R, Pallis M. SLAP Repairs With Combined Procedures Have Lower Failure Rate Than Isolated Repairs in a Military Population: Surgical Outcomes With Minimum 2-Year Follow-up. Orthop J Sports Med. 2015 Aug;3(8):2325967115599154. [ PMC free article ] [ PubMed ]15.
- Zhang AL, Kreulen C, Ngo SS, Hame SL, Wang JC, Gamradt SC. Demographic trends in arthroscopic SLAP repair in the United States. Am J Sports Med. 2012 May;40(5):1144-7. [ PubMed ]16.
- Miniaci A, Mascia AT, Salonen DC, Becker EJ. Magnetic resonance imaging of the shoulder in asymptomatic professional baseball pitchers. Am J Sports Med. 2002 Jan-Feb;30(1):66-73. [ PubMed ]17.
- Connor PM, Banks DM, Tyson AB, Coumas JS, D’Alessandro DF. Magnetic resonance imaging of the asymptomatic shoulder of overhead athletes: a 5-year follow-up study. Am J Sports Med. 2003 Sep-Oct;31(5):724-7. [ PubMed ]18.
- Mathew CJ, Lintner DM. Superior Labral Anterior to Posterior Tear Management in Athletes. Open Orthop J. 2018;12:303-313. [ PMC free article ] [ PubMed ]19.
- Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS, Kwon YW. The rising incidence of arthroscopic superior labrum anterior and posterior ( SLAP ) repairs. J Shoulder Elbow Surg. 2012 Jun;21(6):728-31. [ PubMed ]20.
- Johannsen AM, Costouros JG. A Treatment-Based Algorithm for the Management of Type-II SLAP Tears. Open Orthop J. 2018;12:282-287. [ PMC free article ] [ PubMed ]21.
- Ilahi OA, Labbe MR, Cosculluela P. Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy. 2002 Oct;18(8):882-6. [ PubMed ]22.
- Kim TK, Queale WS, Cosgarea AJ, McFarland EG. Clinical characteristics of the different types of SLAP lesions: an analysis of one hundred and thirty-nine cases. J Bone Joint Surg Am. 2003 Jan;85(1):66-71. [ PubMed ]23.
- Yeh ML, Lintner D, Luo ZP. Stress distribution in the superior labrum during throwing motion. Am J Sports Med. 2005 Mar;33(3):395-401. [ PubMed ]24.
- Vangsness CT, Jorgenson SS, Watson T, Johnson DL. The origin of the long head of the biceps from the scapula and glenoid labrum. An anatomical study of 100 shoulders. J Bone Joint Surg Br. 1994 Nov;76(6):951-4. [ PubMed ]25.
- Tuoheti Y, Itoi E, Minagawa H, Yamamoto N, Saito H, Seki N, Okada K, Shimada Y, Abe H. Attachment types of the long head of the biceps tendon to the glenoid labrum and their relationships with the glenohumeral ligaments. Arthroscopy. 2005 Oct;21(10):1242-9. [ PubMed ]26.
- Fealy S, Rodeo SA, Dicarlo EF, O’Brien SJ. The developmental anatomy of the neonatal glenohumeral joint. J Shoulder Elbow Surg. 2000 May-Jun;9(3):217-22. [ PubMed ]27.
- Kwak SM, Brown RR, Resnick D, Trudell D, Applegate GR, Haghighi P. Anatomy, anatomic variations, and pathology of the 11- to 3-o’clock position of the glenoid labrum: findings on MR arthrography and anatomic sections. AJR Am J Roentgenol. 1998 Jul;171(1):235-8. [ PubMed ]


















{kind=link}