

Introduction: Unraveling a Silent Burden
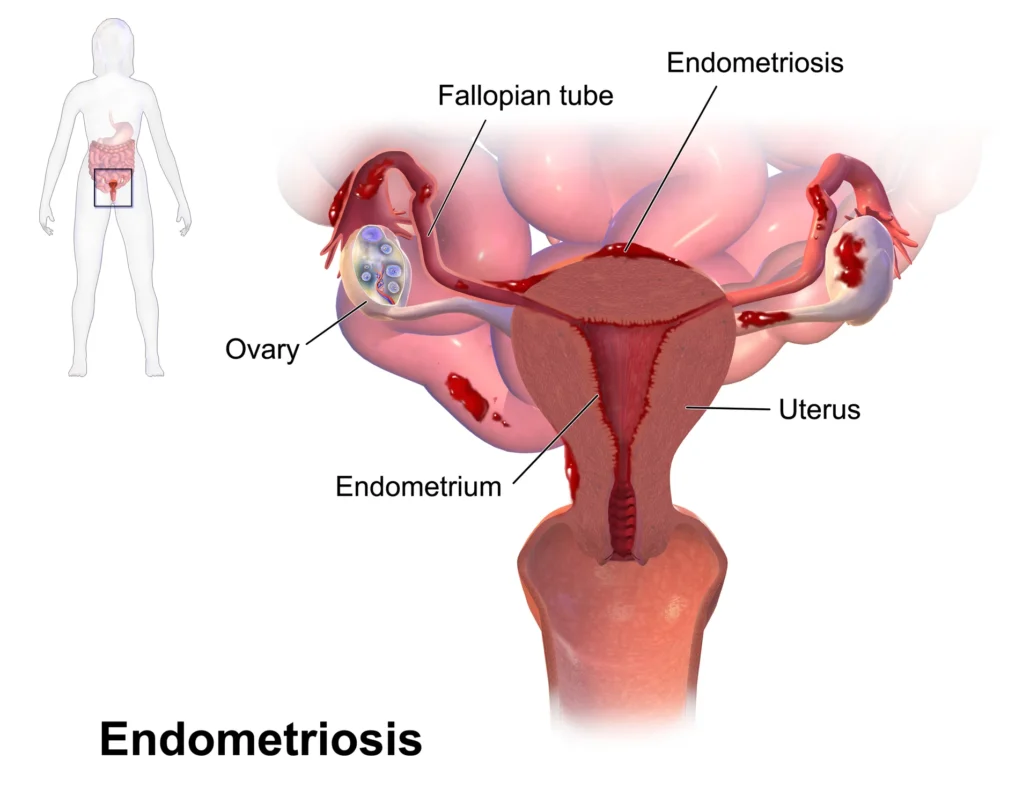
Endometriosis is a condition as enigmatic as it is debilitating. Affecting an estimated 1 in 10 women of reproductive age, it is a chronic inflammatory disease characterized by the presence of endometrial-like tissue outside the uterine cavity—most commonly on the ovaries, pelvic peritoneum, or bowel. Despite its prevalence, it remains woefully underdiagnosed and misunderstood, often dismissed as “bad periods” or generalized pelvic pain. For many, the road to diagnosis can span years, marked by frustration, emotional distress, and a sense of invisibility within the healthcare system.
4o
The burden of endometriosis is not limited to menstruation. Beyond the cyclical pain, many individuals suffer from chronic pelvic discomfort, digestive issues, fatigue, pain during intercourse (dyspareunia), and infertility. The symptoms can be multifaceted and systemic, often fluctuating in severity and impacting day-to-day activities, work performance, mental health, and intimate relationships. The resulting psychosocial strain can be profound, making endometriosis not just a gynecological condition but a whole-person challenge.
Part of the difficulty in addressing endometriosis lies in its complexity. Its causes remain poorly understood, with theories ranging from retrograde menstruation and coelomic metaplasia to immune dysfunction and genetic predisposition. This ambiguity, combined with its variable symptomatology, has led to a fragmented approach in conventional care. While hormonal treatments and laparoscopic surgery are often prescribed, these solutions can bring only partial relief—or worse, new side effects. For many patients, the feeling persists that something deeper is being missed: a persistent tension, a visceral discomfort, a sense that the body is not fully cooperating.
In this therapeutic void, complementary approaches like osteopathy have begun to gain interest—not as replacements for conventional treatment, but as integrative tools that address the broader picture of somatic dysfunction and nervous system imbalance. Osteopathy, with its hands-on, holistic philosophy, views the body as a unified whole where structure and function are intimately connected. In the case of endometriosis, this perspective opens new doors: What if the pain is not just from lesions, but also from fascial restrictions, pelvic misalignment, impaired lymphatic drainage, or heightened autonomic tone? What if the body is trying to adapt, but gets stuck in protective patterns?
Manual osteopathic techniques can offer a unique therapeutic response. By gently releasing restrictions in the abdominal and pelvic fascia, mobilizing the viscera, balancing the sacroiliac joints, and calming the autonomic nervous system, the osteopath works to restore motion and ease throughout the body’s core. Patients often report not only a reduction in pain, but a greater sense of grounding, better digestion, improved posture, and even emotional release. While osteopathy does not claim to cure endometriosis, it can help to relieve many of the secondary effects that perpetuate suffering.
Moreover, the osteopathic approach fosters a different therapeutic relationship—one built on listening, presence, and trust. For patients who have long felt unheard or reduced to their symptoms, this can be a profoundly healing shift. The body is no longer a battleground to be managed, but a living system to be supported.
As awareness of endometriosis continues to grow, so too does the recognition that a singular approach is rarely sufficient. We need care models that embrace complexity, that see the interconnectedness of anatomy, physiology, and emotion. Osteopathy, with its foundational belief in the body’s self-healing capacity, offers such a model. It invites us to consider not just where it hurts, but why the body holds tension there—and how we might gently help it let go.
This article will explore how osteopathy can be integrated into the care of individuals living with endometriosis, from understanding its anatomical underpinnings to applying specific manual techniques. We will also examine case examples, clinical observations, and the broader implications for holistic pelvic care. In doing so, we aim to shed light on a path of relief that is not often visible—but deeply needed.
What Is Endometriosis? A Complex and Painful Condition
Endometriosis is not simply a reproductive disorder—it is a systemic, multifactorial, and often misunderstood condition that challenges both medical science and patient resilience. Defined by the presence of endometrial-like tissue outside the uterus, this condition creates a cascade of chronic inflammation, fibrosis, and nerve sensitization. Although these ectopic tissues resemble the uterine lining, they behave differently: they don’t shed through menstruation, leading instead to internal bleeding, adhesions, and persistent irritation of surrounding structures.
Definition and Pathophysiology
The core mechanism of endometriosis remains elusive. Retrograde menstruation—the backflow of menstrual blood through the fallopian tubes into the pelvic cavity—is a widely accepted theory, but it doesn’t explain all cases, particularly those affecting areas distant from the pelvis. Other hypotheses include metaplastic transformation of coelomic cells, immune dysregulation, lymphatic or hematogenous dissemination, and even environmental or epigenetic influences.
Once established, endometriotic lesions often lead to a localized inflammatory response. This inflammation stimulates angiogenesis (the formation of new blood vessels), fibrotic tissue growth, and an increased presence of pro-inflammatory cytokines. These processes can entrap nerve fibers or stimulate the formation of new ones, which helps explain the chronic, sometimes excruciating pain reported by patients—even when lesion size is small. Pain severity does not always correlate with the extent of visible disease, further complicating diagnosis and treatment.
Symptoms Beyond Menstruation
While the most commonly recognized symptom is dysmenorrhea (painful periods), endometriosis affects the body far beyond menstruation. Chronic pelvic pain may persist throughout the cycle, radiating into the lower back, hips, thighs, or perineum. Pain during intercourse, particularly deep penetration, is a hallmark symptom known as dyspareunia, often reflecting involvement of the uterosacral ligaments or rectovaginal septum.
Gastrointestinal and urinary symptoms are also common. Patients may report bloating, constipation, diarrhea, nausea, or pain during bowel movements, especially during menstruation. In cases where the bladder is involved, symptoms might mimic interstitial cystitis or recurrent urinary tract infections. Because of these overlapping presentations, misdiagnosis is common—many patients are first told they have irritable bowel syndrome, pelvic floor dysfunction, or psychosomatic disorders.
This wide constellation of symptoms points toward a more systemic phenomenon, where endometriosis interacts with the nervous, hormonal, and immune systems in a complex web. Central sensitization, where the nervous system becomes hyper-reactive to stimuli, is often present and may amplify pain perception long after the original lesion is addressed. For some, this leads to the development of secondary conditions such as fibromyalgia, chronic fatigue syndrome, or anxiety and depression.
Emotional and Systemic Impact
Living with endometriosis can be profoundly isolating. The invisibility of the condition, combined with its unpredictable nature, disrupts work, relationships, and daily functioning. Repeated encounters with skeptical healthcare providers or ineffective treatments can erode trust and lead to emotional exhaustion. Many individuals report feeling dismissed or labeled as “hysterical” or “overly sensitive,” which compounds the psychological burden.
In addition to emotional strain, the physiological toll is significant. Chronic pain alters breathing patterns, posture, and muscular tone. Over time, compensatory mechanisms in the pelvis and spine may create somatic dysfunctions—tightness in the iliopsoas, restricted sacroiliac joints, diaphragm tension, and fascial adhesions across the abdomen. These secondary effects can perpetuate pain even when hormonal therapy suppresses the primary lesions.
From an osteopathic standpoint, this interplay between the physical and emotional realms is central. The body responds to pain and inflammation by tightening, protecting, and adapting—often at the expense of mobility and fluidity. These protective patterns, though initially adaptive, can become rigid and self-perpetuating, contributing to the chronicity of symptoms.
Understanding endometriosis, therefore, requires a lens that goes beyond lesion size or hormonal status. It calls for a biopsychosocial model that acknowledges the body’s attempts to cope, the nervous system’s sensitivity, and the individual’s lived experience. Osteopathy, with its integrative and manual approach, is particularly well-suited to work within this complexity.
In the next section, we will explore the limitations of conventional treatment pathways and the growing demand for complementary options that address the body’s structural and functional imbalances.
Conventional Approaches and Their Limitations
For many individuals with endometriosis, the medical journey is long and fraught with frustration. Conventional treatment methods—while sometimes effective—often provide only partial relief, fail to address the root of recurring symptoms, or come with side effects that burden the patient’s quality of life. While science has made strides in identifying and managing the disease, there remains a significant therapeutic gap between clinical objectives and patient experience.
Medical and Surgical Options
First-line medical treatments typically aim to suppress the hormonal cycle that fuels the growth of endometriotic lesions. These include:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce pain and inflammation;
- Hormonal contraceptives (combined or progestin-only) to regulate or suppress menstruation;
- GnRH agonists or antagonists, which induce a pseudo-menopause by drastically lowering estrogen levels.
While hormonal treatments can reduce lesion activity and menstrual pain, they are not curative. Moreover, their systemic effects—hot flashes, mood swings, decreased libido, bone density loss—can make long-term use difficult. For individuals seeking to conceive, these medications also pose a major barrier due to their ovulation-suppressing nature.
When symptoms persist despite medical management, surgery is often proposed. Laparoscopic excision of endometriotic lesions remains the gold standard. It allows both diagnosis and treatment, and can significantly reduce pain and restore fertility in selected cases. However, surgery is not without risks: adhesions can form post-operatively, some lesions are difficult to access, and recurrence rates remain high (up to 50% within five years). Repeated surgeries may yield diminishing returns and increase the risk of complications, particularly when surrounding organs such as the bowel or bladder are involved.
For deep infiltrating endometriosis, particularly cases involving the rectovaginal septum or bowel, more extensive procedures may be required, including bowel resection or ureterolysis. These interventions, while sometimes necessary, carry the weight of long recovery periods, potential nerve damage, and emotional trauma. Many patients are left wondering if the relief justifies the cost to their overall wellbeing.
Why Many Patients Seek Complementary Therapies
Faced with these limitations, a growing number of individuals are turning to complementary or integrative care options. Not because they reject medicine, but because they are seeking a more complete response—one that considers not only lesion removal or hormone suppression, but also pain modulation, body awareness, emotional support, and functional restoration.
In many cases, pain continues even when lesions are removed or suppressed. This is due to the central sensitization of the nervous system, fascial restrictions, myofascial trigger points, and altered biomechanics in the pelvis and lumbar spine. These secondary effects are often invisible in imaging and overlooked in consultations focused on gynecological findings.
Additionally, the psychological toll of endometriosis—years of chronic pain, invalidation, and fear—creates a state of heightened stress reactivity. The autonomic nervous system becomes dysregulated, further contributing to muscle tension, poor sleep, digestive dysfunction, and emotional fatigue.
It’s in this context that manual therapies, such as osteopathy, can play a pivotal role. They offer an embodied experience of care—not just intellectual explanations, but hands-on interventions that meet the body where it is. Osteopathy in particular aligns with the need for integrative solutions by addressing the mechanical, visceral, vascular, neural, and emotional dimensions of chronic pelvic pain.
This doesn’t mean dismissing conventional care—it means complementing it. A patient recovering from laparoscopy may still struggle with postural adaptations and fascial tension. A person on hormonal treatment might still carry years of compensatory patterns in the pelvis and abdomen. The goal is not to replace one model with another, but to build bridges—between disciplines, between systems of care, and between the patient’s symptoms and their body’s deeper patterns.
Endometriosis is a complex and deeply personal condition. No single approach will address every layer of it. But when conventional treatments are integrated with manual therapies and patient-centered listening, new avenues of relief become possible.
In the following section, we will explore how osteopathy conceptualizes pelvic dysfunction in the context of endometriosis—and how its techniques can help restore a sense of coherence, motion, and vitality.
Osteopathic Perspective: A Whole-Body Approach to Pelvic Health
Endometriosis does not merely disrupt the uterus—it impacts the entire pelvic environment, the surrounding structures, and often the global equilibrium of the body. From an osteopathic standpoint, this condition is not only a gynecological challenge but a multisystem dysfunction that affects visceral mobility, fascial continuity, postural dynamics, and nervous system balance. Osteopathy’s holistic lens offers a way to understand and relieve the complex patterns of restriction, compensation, and pain that often accompany endometriosis.
Fascia, Viscera, and Chronic Pain
One of the cornerstones of osteopathic reasoning lies in the interconnectedness of the fascial system. Fascia envelops every organ, muscle, nerve, and vessel. In the pelvis, the fascial planes linking the uterus, bladder, rectum, sacrum, and abdominal viscera form a tightly integrated network. When endometriosis lesions develop and provoke inflammation, this often leads to adhesions, thickening, and loss of glide between these structures.
Even small lesions can create significant discomfort if they restrict fascial mobility or disturb the relationship between organs. For instance, tension in the uterosacral ligaments or pelvic floor fascia can pull on the sacrum, disturb sacroiliac joint dynamics, or alter lumbar lordosis—contributing to both pelvic pain and low back pain. These dysfunctions may persist even after hormonal suppression or surgery, creating a cycle of pain unrelated to active disease.
Moreover, fascial strain patterns are not limited to the pelvis. They can propagate throughout the body, particularly along myofascial chains that connect the pelvis to the diaphragm, thorax, and even the cranium. A uterine fixation can thus contribute to respiratory limitation, tension headaches, or thoracolumbar stiffness, especially if the body compensates asymmetrically over time.
Pelvic Congestion and Somatic Dysfunction
In endometriosis, venous and lymphatic stasis is a frequently overlooked component of pain. Inflammatory processes within the pelvic cavity can impede proper drainage, particularly in the broad ligament, uterine plexus, and iliac vessels. This leads to a sensation of heaviness, congestion, or fullness, especially premenstrually.
Osteopaths pay close attention to venous return and lymphatic circulation, using gentle techniques to restore mobility in the diaphragm, thoracic inlet, and pelvic floor. Mobilizing the inguinal canal, iliopsoas, or sacral base can relieve local congestion and improve systemic fluid dynamics. This helps reduce inflammatory load, improve immune modulation, and restore more balanced internal pressure systems.
Somatic dysfunctions—altered position, mobility, or tone of anatomical structures—are often found in patients with endometriosis. Common patterns include:
- Restricted sacroiliac joint motion
- Hypertonicity of the piriformis or obturator internus
- Fixations in the lumbar spine or thoracolumbar junction
- Diaphragmatic tension from chronic guarding or shallow breathing
These dysfunctions are not merely epiphenomena; they play an active role in perpetuating pain, reducing pelvic mobility, and maintaining an inflammatory state.
Interplay Between Autonomic Nervous System and Visceral Tension
The autonomic nervous system (ANS) governs the visceral organs, regulating uterine contractility, gut motility, blood flow, and pain perception. In endometriosis, the sympathetic system is often hyperactive, maintaining a state of chronic vigilance and muscular bracing. This can manifest as pelvic floor overactivity, reduced peristalsis, or poor vascular supply.
Osteopathic treatment addresses this imbalance through craniosacral therapy, rib cage mobilization, subdiaphragmatic release, and sacral base balancing, all of which act on key autonomic centers. For example, the superior mesenteric ganglion, sacral parasympathetics, and vagus nerve can all be influenced through gentle palpation and indirect techniques.
By down-regulating sympathetic overdrive and supporting parasympathetic tone, the osteopath facilitates a more regulated internal environment. This, in turn, promotes tissue healing, better visceral function, and reduced pain sensitivity.
Osteopathy doesn’t treat endometriosis in the conventional sense—it doesn’t remove lesions or modulate hormones directly. But it addresses what the body does in response to the disease: how it protects, adapts, compresses, and compensates. Through touch, the practitioner helps to free what is stuck, to soften what is tense, and to listen to what the body remembers.
In the next section, we will explore the manual techniques commonly used in osteopathic practice to support individuals with endometriosis—and how they are tailored to the unique anatomy and needs of each patient.
Manual Techniques to Relieve Endometriosis-Related Pain
Osteopathic treatment for endometriosis is not standardized—it is individualized, nuanced, and deeply responsive to each patient’s unique anatomical and emotional landscape. Manual therapy aims to release tissue restrictions, restore physiological mobility, modulate pain pathways, and create space where the body has been compressed by years of inflammation, bracing, and dysfunction. This section explores some of the most commonly used techniques, with attention to therapeutic goals and practical positioning.
Myofascial Release in the Pelvic Region
Purpose: To reduce fascial densification and restore mobility between pelvic structures (uterus, bladder, rectum, ovaries).
Patient position: Supine, knees flexed (hook-lying position) or with a support under the knees to relax abdominal tension.
Technique: The osteopath places one hand gently over the lower abdomen, the other under the sacrum. With very slow, sustained pressure, the practitioner engages the superficial and deep fascia, following the natural direction of tissue glide—or waiting for the tissue to “melt” in areas of restriction. There is no forcing, only an invitation for the body to soften.
Clinical effect: This technique is particularly helpful in reducing restrictions around the broad ligament, uterosacral ligaments, and pelvic floor fascia. Patients often report a decrease in the sense of internal pressure or congestion after treatment.
Visceral Manipulation: Uterus and Surrounding Organs
Purpose: To enhance mobility and motility of the uterus and its visceral relationships, especially with the bladder, sigmoid colon, and sacrum.
Patient position: Supine, hips in slight flexion. A bolster under the knees or a semi-recumbent position can help reduce lumbar tension.
Technique: Using a light but focused palpation, the osteopath locates the uterus (just above the pubic bone). Gentle traction or mobilization is performed along different vectors: superior-inferior (toward/away from umbilicus), lateral (toward iliac crests), and posterior (toward sacral base). If the uterus is retroverted or adherent, the technique is even slower and indirect, allowing time for micro-movement responses.
Clinical effect: These techniques aim to release fascial fixations, restore uterine mobility, and decrease mechanical strain on adjacent organs. This often helps with menstrual pain and premenstrual bloating.
Sacral Balancing and SI Joint Mobilization
Purpose: To restore sacroiliac joint mobility and reduce mechanical tension between the sacrum and uterus, which are linked via the uterosacral ligaments.
Patient position: Prone or side-lying depending on comfort. In some cases, seated mobilization is used for better awareness and feedback.
Technique:
- Prone: The osteopath places one hand over the sacral base and the other over the apex. With gentle pressure and respiratory syncing, the sacrum is encouraged to follow its natural craniosacral rhythm.
- Side-lying: The upper leg is supported in hip and knee flexion. The practitioner contacts the sacrum and ilium to perform rhythmic mobilizations or soft articulatory movements.
Clinical effect: Mobilizing the sacrum helps reduce tethering of the pelvic fascia, decreases low back and pelvic floor discomfort, and may influence autonomic balance through the sacral parasympathetics (S2–S4).
Diaphragmatic Release and Respiratory Mobilization
Purpose: To reduce upper abdominal pressure, improve lymphatic and venous return, and promote parasympathetic activity via the phrenic nerve and vagus.
Patient position: Supine, head and neck in neutral. Pillow under the knees optional.
Technique: The osteopath gently contacts the inferior border of the rib cage bilaterally, following the motion of the diaphragm during breathing. If restrictions are noted (often in the right crura or costal attachments), the practitioner may use direct or indirect release. Emphasis is placed on matching the patient’s breath rather than imposing force.
Clinical effect: A freer diaphragm enhances organ mobility and fluid circulation in the abdomen and pelvis. It also helps regulate the autonomic nervous system, which is frequently dysregulated in chronic pain syndromes.
Intra-Pelvic Techniques (Pelvic Floor and Coccyx)
Purpose: To release hypertonic pelvic floor musculature, rebalance the coccyx, and relieve tension in the levator ani and obturator internus.
Patient position: Side-lying or supine with knees flexed. If intra-vaginal techniques are used, consent and explanation are essential, and gloves are worn.
Technique:
- External: The osteopath may work on the perineum, coccyx, or ischial tuberosities to influence muscle tone and ligamentous attachments.
- Internal: With one finger inserted (if appropriate and permitted), the practitioner may palpate the tension patterns in the pelvic floor and use subtle pressure or unwinding techniques to reduce spasm or asymmetry.
Clinical effect: These techniques can dramatically reduce dyspareunia, improve bowel and bladder function, and restore pelvic floor balance. When done with gentleness and presence, they also help re-establish a sense of safety and embodiment.
Cranial-Sacral Integration
Purpose: To address the global tensions of the craniosacral system, reduce nervous system arousal, and restore fluid rhythm throughout the axial body.
Patient position: Supine, fully relaxed.
Technique: The practitioner may work with the occiput, sacrum, temporal bones, or dural membranes, following the cranial rhythmic impulse (CRI) and releasing restrictions along the central line.
Clinical effect: Calms hyperactive sympathetic tone, reduces systemic tension, and can improve menstrual rhythm, digestion, and emotional regulation.
Manual therapy for endometriosis is not about “fixing” the condition—it’s about listening to how the body has adapted and helping it let go. Through gentle, precise, and deeply respectful techniques, the osteopath offers a space for change where tension, inflammation, and suffering have long dominated. It is in these subtle layers that many patients rediscover a sense of coherence and relief—sometimes for the first time in years.
Clinical Observations and Case Examples
Endometriosis is not just a textbook pathology—it is a lived experience that varies greatly from one individual to another. In clinical osteopathic practice, what often stands out is not only the diversity of symptom presentations, but also the ways in which the body attempts to adapt and compensate. Observing and understanding these patterns is essential for offering truly individualized care. Below are common clinical observations, followed by a few illustrative case examples that highlight the relevance and impact of osteopathic intervention.
Patterns Commonly Observed in Osteopathic Practice
Patients with endometriosis often present with a constellation of somatic dysfunctions that extend beyond the pelvic cavity. These include:
- Pelvic asymmetry, often involving a rotated or side-bent sacrum and restricted sacroiliac joints;
- Abdominal fascial tension, particularly around the lower quadrants and umbilical region;
- Diaphragmatic restriction, manifesting as shallow breathing or tension in the costal margins;
- Lumbar or thoracolumbar fixations, related to protective muscle guarding;
- Hypertonic pelvic floor, often associated with pain during intercourse or bowel movements;
- Coccygeal or sacrococcygeal dysfunctions, particularly in cases with a history of falls or trauma.
Many patients also exhibit signs of autonomic nervous system dysregulation, such as cold extremities, poor digestion, and heightened startle response. These observations often reflect a chronic state of sympathetic dominance—a common finding in those who live with persistent pain.
Case Example 1: Chronic Pelvic Pain and Emotional Release
A 32-year-old patient presented with chronic pelvic pain, fatigue, and a history of three laparoscopies. Despite hormonal treatment, she continued to experience deep pelvic discomfort, especially premenstrually. Osteopathic assessment revealed restricted mobility of the uterus, a left-rotated sacrum, and tension in the right iliopsoas.
Treatment focused on myofascial release of the lower abdomen, mobilization of the uterus and sigmoid colon, and indirect balancing of the sacrum. After three sessions, the patient reported decreased premenstrual bloating, softer abdominal tone, and greater emotional stability. In one session, she experienced a spontaneous release of tears—later described as a “letting go of something stuck in her belly.” The connection between physical tension and emotional holding became a therapeutic pivot in her care.
Case Example 2: Dyspareunia and Postural Adaptations
A 28-year-old dancer sought help for pain during intercourse and right-sided hip tightness. Imaging had shown mild endometriosis, but she felt dismissed by previous providers. Palpation revealed fascial drag from the right ovary toward the pelvic floor, a tight obturator internus, and coccygeal tenderness.
Techniques included intra-pelvic balancing, sacral release, and mobilization of the right ilium. Post-treatment, she noted reduced pelvic tension and, for the first time in years, pain-free intimacy. She also reported greater flexibility in her hip and a newfound awareness of how her posture was subtly protecting the pelvis—something she had never consciously perceived.
Case Example 3: Fertility Challenges and Visceral Restrictions
A 35-year-old patient with unexplained infertility and a known diagnosis of endometriosis consulted osteopathy as part of a broader fertility strategy. She had a history of bowel irregularities, painful ovulation, and emotional burnout.
Osteopathic work focused on the uterus, ovaries, colon, and diaphragm. Special attention was given to the mesenteric attachments and the mobility of the ovaries relative to the iliac vessels. As sessions progressed, her menstrual cycle became more regular, and she described a “softening” in her lower abdomen. After six months of integrative care (including medical, nutritional, and osteopathic support), she successfully conceived.
Integrating Clinical Intuition with Structure
Each case highlights how osteopathy can play a meaningful role—not in isolation, but as part of a multidisciplinary approach. What is particularly powerful is the listening quality of osteopathic touch, which helps patients feel seen, held, and respected in their entirety.
While results vary, the common denominator is that manual therapy helps restore a sense of coherence in bodies that have long felt fragmented by pain, interventions, and misunderstanding. This subtle, whole-body perspective may not “treat” endometriosis in the traditional sense, but it can offer something equally valuable: relief, integration, and a renewed relationship with one’s own body.
Precautions and Contraindications
While osteopathic care offers valuable support for individuals living with endometriosis, it is essential to recognize the importance of clinical judgment, respectful communication, and careful adaptation of techniques. The complex and sometimes unpredictable nature of this condition means that practitioners must be attuned not only to the physical state of the tissues, but also to the emotional and systemic context of the patient.
When to Refer and Collaborate
Purpose: To ensure safety, comprehensive care, and appropriate medical oversight.
Although osteopathy can play a powerful role in pain reduction and functional support, it should never replace essential medical evaluation and treatment. Practitioners must remain vigilant for red flags or signs that require referral, including:
- Sudden, unexplained weight loss
- Persistent gastrointestinal bleeding
- Acute or rapidly worsening pelvic pain
- Signs of infection (fever, purulent discharge)
- Suspicion of malignancy
- Suspected bowel or bladder involvement with obstruction
In such cases, collaboration with gynecologists, gastroenterologists, or pelvic surgeons is vital. Osteopaths should work in parallel, contributing to the broader picture of care. This interdisciplinary dialogue respects the limits of each modality and reinforces patient safety.
Additionally, in cases of fertility treatment, it is crucial to coordinate with reproductive endocrinologists, especially when procedures such as in vitro fertilization (IVF) are underway. Manual therapy should be timed appropriately within the menstrual cycle and in harmony with medical protocols.
Safety in Manual Therapy During Flare-Ups or Post-Surgery
Purpose: To avoid aggravating symptoms or interfering with tissue healing.
Endometriosis symptoms can fluctuate considerably throughout the menstrual cycle. During active flare-ups—particularly around ovulation or menstruation—patients may be more sensitive to touch, emotionally reactive, or fatigued. In these moments, the osteopath should:
- Use lighter techniques such as indirect fascial release, fluidic touch, or cranial-sacral work
- Avoid deep intrapelvic or abdominal work, which may increase pain or lead to a defensive reaction
- Prioritize grounding techniques to support the nervous system rather than target the primary lesion zones
Post-surgical cases also require careful timing and adaptation. In the weeks following a laparoscopy or excision procedure, it is best to avoid direct mobilization of the abdomen or deep visceral techniques. Instead, treatment may focus on:
- Supporting respiratory motion and thoracic outlet drainage
- Addressing compensatory postural patterns
- Mobilizing distant areas (e.g., diaphragm, feet, cervical spine) to gently re-integrate mobility without stressing the healing site
After 6–8 weeks, and with medical clearance, more targeted pelvic and visceral work can be reintroduced progressively, always respecting the tissue quality and the patient’s comfort.
Trauma History and Emotional Considerations
Purpose: To recognize and respect the body’s protective responses in patients with a history of trauma or medical vulnerability.
A significant number of individuals with endometriosis have experienced past trauma, including medical trauma, emotional neglect, or sexual abuse. Invasive examinations, surgical interventions, and repeated dismissal by healthcare professionals may further compound a sense of vulnerability.
Osteopaths must be especially careful when working near intimate areas. Even external palpation of the lower abdomen, iliac crests, or pelvic floor can trigger emotional responses. To ensure safe and ethical practice:
- Always obtain informed consent, explaining the purpose and boundaries of each technique
- Give patients control, allowing them to stop or adjust the session at any time
- Use verbal feedback, asking “Is this pressure okay?” or “Would you prefer a different position?”
- Offer grounding touch at the feet or occiput if deeper work is not appropriate that day
In some cases, the therapeutic goal is not to release a restriction, but simply to establish safety in sensation—to be present with the body without triggering a protective response. This alone can be a powerful step toward healing.
Conclusion: A Gentle Ally in a Complex Journey
Living with endometriosis is often a journey through uncertainty, pain, and persistent search for answers. It affects the body in layered, sometimes contradictory ways—producing not only localized inflammation and pain, but also global dysfunctions, emotional exhaustion, and a sense of disconnection from the self. In this landscape, osteopathy does not offer a cure. But it offers something precious: a therapeutic presence, a listening hand, and a gentle path back toward balance.
Osteopathy sees the body not as a collection of broken parts, but as a coherent system that is always trying to adapt—even under stress, inflammation, or trauma. Every adhesion, every muscle spasm, every shallow breath is understood not as a defect, but as a protective gesture. The goal of osteopathic care is to help the body release what is no longer needed and to support what is still trying to function.
This approach requires time, trust, and an ability to work within complexity. There is no single protocol for treating endometriosis osteopathically. Each patient brings a unique history, set of symptoms, and relationship to their body. Some will need deep fascial work; others will need only stillness and containment. Some will be ready for visceral mobilization, while others will simply need to feel safe enough to breathe again.
The techniques described throughout this article—myofascial release, visceral mobilization, sacral balancing, pelvic floor support, craniosacral integration—are tools, not solutions in themselves. Their effectiveness depends not only on skill, but on the intention behind the touch. When applied with respect, precision, and care, they can reduce pain, restore mobility, and even shift how the patient relates to their own pelvic space.
Beyond hands-on work, the osteopathic approach includes education and empowerment. Helping a patient understand their posture, breath, movement, and emotional responses is part of the healing process. Offering tools they can use between sessions—breathing exercises, gentle stretches, postural cues—reinforces their autonomy and builds trust in their own body.
Importantly, osteopathy does not seek to replace medical care, but to complement it. In the context of endometriosis, collaboration with gynecologists, pain specialists, physical therapists, nutritionists, and mental health professionals is essential. Osteopathy becomes one voice in a therapeutic chorus—often the voice that speaks with the hands, that listens to what is not said, that validates what has long been felt but not seen.
For many, this is the most healing aspect of the work: not just less pain, but less isolation. Not just functional improvement, but the quiet reassurance that their experience is real, and that their body is not broken, but tired—and deserving of care.
In a world that often pushes toward quick fixes and narrow diagnoses, osteopathy offers a slower, wider, more compassionate view. It affirms that the body remembers, that the pelvis holds stories, and that healing is not linear but possible—when space is made for it.
Endometriosis is a complex journey. Osteopathy may not solve every step, but it can walk alongside, gently restoring motion, coherence, and dignity along the way.
References
- Bulun, S. E. (2009). Endometriosis. The New England Journal of Medicine, 360(3), 268–279.
https://doi.org/10.1056/NEJMra0804690 - Missmer, S. A., et al. (2014). Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. American Journal of Epidemiology, 160(8), 784–796.
https://doi.org/10.1093/aje/kwh275 - Bourdel, N., et al. (2019). Pain evaluation in endometriosis: A literature review. Journal of Endometriosis and Pelvic Pain Disorders, 11(4), 147–160.
https://doi.org/10.1177/2284026519889354 - Loving, S., Nordling, J., & Thomsen, T. (2012). Pelvic pain in women: Evaluation and management. BMJ, 345, e5676.
https://doi.org/10.1136/bmj.e5676 - Chaitow, L., Bradley, D., & Gilbert, C. (2012). Multidisciplinary Approaches to Pain Management: The Manual Therapy Contribution. Churchill Livingstone.
- Brun, J. L., et al. (2018). Endometriosis pain explained by central sensitization: A systematic review. Pain Physician, 21(5), 451–462.
https://pubmed.ncbi.nlm.nih.gov/30376845/ - D’Alessandro, G., et al. (2021). Effectiveness of osteopathic treatment in pain and quality of life in women with endometriosis: A randomized controlled trial. Complementary Therapies in Clinical Practice, 42, 101279.
https://doi.org/10.1016/j.ctcp.2021.101279 - FitzGerald, M. P., & Kotarinos, R. (2003). Rehabilitation of the short pelvic floor. II: Treatment of the patient with the short pelvic floor. International Urogynecology Journal, 14(4), 269–275.
https://doi.org/10.1007/s00192-003-1064-8 - Price, R., et al. (2011). The role of physiotherapy in the management of chronic pelvic pain. Current Opinion in Obstetrics and Gynecology, 23(4), 255–260.
https://doi.org/10.1097/GCO.0b013e328348a585







{kind=link}