

Muscle energy technic is a manual technique used by osteopaths and which was developed in 1948 by Fred Mitchell, Sr, DO. The therapist asks the patient to stretch a muscle from a tightly controlled position in a specific direction against specific resistance from the therapist.
MET is based on the concepts of autogenous inhibition and reciprocal inhibition. If a submaximal muscle contraction is followed by a stretch of the same muscle, it is called autogenous MET inhibition, and if a submaximal contraction of one muscle is followed by a stretch of the opposite muscle, then it is called of reciprocal MET inhibition.
Basic concepts
Contractions by the patient in conjunction with the therapist’s efforts result in:
- Isometric contraction
- Therapist Force Applied = Patient Force Applied
- Isotonic contraction
- Eccentric
- Therapist Applied Force> Patient Applied Force
- Concentric
- Therapist’s Applied Force
- Therapist’s Applied Force
- Eccentric
The term post-isometric relaxation (RPI) refers to the effect of the subsequent reduction in tone experienced by a muscle or group of muscles, after brief periods in which an isometric contraction has been performed.
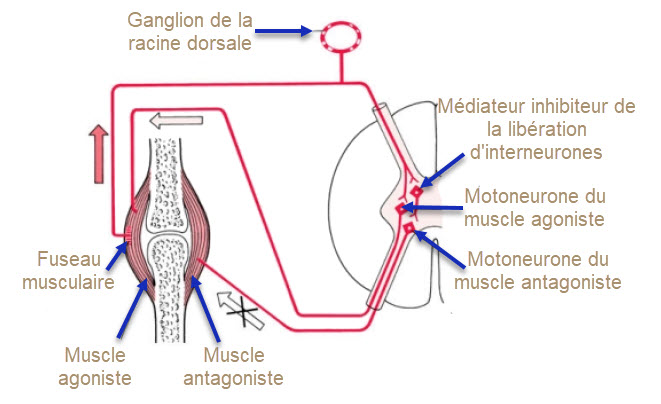
When a muscle is isometrically contracted, its antagonist will be inhibited and show reduced tone immediately after that. Thus, the antagonist of a shortened muscle, or group of muscles, can be contracted isometrically in order to obtain a degree of ease and the potential for additional movement in the shortened tissue.
For the treatment of the joints, it is important that the therapist detects the barriers in the three planes of motion and properly adjusts the joint partner without stretching the muscles to be treated (to avoid the stretch reflex). Here it is essential that they feel the muscle barrier. This is achieved before the joint barrier and before the fascia.
Indication
- Hypertonic inhibitor. Spastic muscles
- Toning of hypotonic and weak muscles
- Stretching of fibrosis, shortening
- Relaxation of muscle adhesions
- Joint dysfunctions
- Stimulation of local venolymphatic circulation
- Positively affecting movements and postural patterns
- Break a painful vicious cycle
Contraindication
- Since this technique requires the participation of the (active) patient, it is important that the latter be able to have the ability to interact with the therapist.
- An unhealed wound
MET Lewit post-isometric relaxation variations
Hypertonic muscle is taken at a length less than pain / resistance
- The patient contracts (10-25%) the muscle for 5-10 seconds while the therapist provides equal force
- The patient relaxes and the muscle is brought to a new range of motion
- From acquired ROM, repeated 2-3 times
Janda’s post-facilitation stretch
The affected muscle is placed in a midline position
- Patient contracts (90-100%) for 5-10 seconds
- Quick stretch to new ROM and hold for 10 seconds
- Relax for 20 seconds and repeat 3-5 times
- Feelings of warmth and weakness may be felt for a short time with this method
Reciprocal inhibition method
- The affected muscle is placed midway
- Patient contracts isometrically or isotonically for 5-10 seconds
- The muscle is passively lengthened
- Repeated 2-3 times













{kind=link}