

Introduction: When everything revolves around you
Vertigo is a sensation of instability or spinning, often disconcerting, which can have a major impact on quality of life. Among the most common types of vertigo is benign paroxysmal positional vertigo (BPPV) , a common yet little-known condition. While conventional medical treatments often provide rapid relief, osteopathy offers a complementary, comprehensive, and long-lasting approach.
This article offers a comprehensive exploration of BPPV, a comparison with other types of vertigo, tools for recognizing it, effective maneuvers, and the specific contribution of osteopathy in its treatment.
Otoliths on the Move: Understanding the Cause of BPPV
BPPV occurs when tiny crystals, called otoliths (or calcium carbonate crystals), break away from the utricle and migrate into the semicircular canals of the inner ear.
These canals contain a fluid whose movement informs the brain about head rotations. The abnormal presence of otoliths disrupts this fluid, generates false sensory information and causes sudden, brief but intense dizziness , often triggered by a change of position (getting up, lying down, turning the head).
The signs that don’t lie: the typical symptoms of BPPV
The main symptom of BPPV is intense rotational vertigo triggered by a change in head position. It can occur when getting up, lying down, turning in bed, or even when looking up or looking down. This vertigo usually lasts less than a minute , but it can be very unsettling.
Besides dizziness, patients may experience:
- nausea (sometimes accompanied by vomiting) ,
- postural instability ,
- apprehension during rapid head movements .
It is important to note that BPPV is not associated with hearing loss or tinnitus , which often helps distinguish it from other vestibular pathologies.
Trigger movements: the most common causes
Benign paroxysmal positional vertigo (BPPV) typically occurs during specific head movements. These simple, everyday actions can be enough to trigger a brief, intense vertigo attack. Identifying these triggers is essential for guiding diagnosis and tailoring treatment.
Among the most frequently involved movements, we find:
- To lie down or get up suddenly from bed
- Turn to one side while lying down
- Tilting the head backward (e.g. looking up at the ceiling)
- Lean forward (to pick up an object, tie your shoes, etc.)
- Turning the head quickly when moving the neck or changing direction
These triggers correspond to positional changes that move the otoliths in the semicircular canals, thus disrupting the vestibular information transmitted to the brain.
👉 Note : Vertigo often occurs with a slight delay of a few seconds after the movement, and may be accompanied by nausea, temporary imbalance and sometimes nystagmus (rapid and involuntary movement of the eyes), visible to an experienced observer.
Do not confuse: BPPV and other vertigo
There are several causes of vertigo, here is a summary comparison:
| Type of vertigo | Duration | Associated symptoms | Main cause | Specificity |
|---|---|---|---|---|
| VPPB | A few seconds | Nausea, triggered by a movement of the head | Displaced otoliths | Positive response to canalithic maneuvers |
| Meniere’s disease | Minutes to hours | Tinnitus, hearing loss, fullness in the ear | Endolymphatic fluid dysregulation | Unpredictable dizziness |
| Vestibular neuritis | Hours to days | Severe isolated vertigo, no auditory symptoms | Viral infection of the vestibular nerve | Often following a cold or flu |
| Cervical vertigo | Variable | Neck pain, stiffness, visual disturbances | Cervical mechanical dysfunction | Related to neck movements |
Exploring Our Internal Compass: The Vestibular System and the Sense of Movement
To fully understand vertigo and its management, it is essential to understand how the vestibular system works , the sensory system located in the inner ear that allows the brain to know where the head is in space , even with the eyes closed. This system works closely with the eyes , proprioceptive receptors , and the brain to maintain balance and coordinate movement.
The Anatomy of the Vestibular System: A Biological Gyroscope
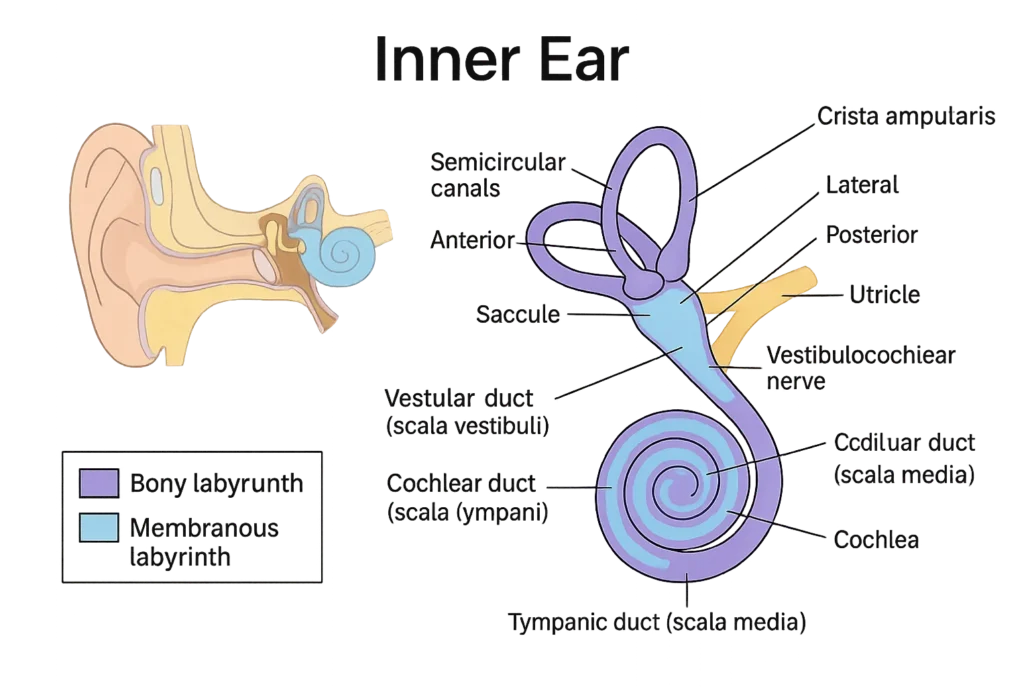
The vestibular system is located in each inner ear and consists of two major parts:
- The semicircular canals (posterior, superior, and horizontal): they detect rotations of the head.
- The otolithic organs (utricle and saccule): they detect linear movements (acceleration, inclination) and gravity .
Each semicircular canal is filled with fluid (endolymph) and contains a sensory receptor called a cupula , located in an enlarged area called the ampulla . When the head is turned, the inertia of the fluid causes pressure on the cupula, which bends and stimulates the sensory hair cells .
These cells send signals to the vestibular nerve , a branch of the auditory nerve (vestibulocochlear nerve – VIII) , which transmits this information to the brain to adjust posture, gaze and spatial perception.
Head movements and spatial perception
Each semicircular canal is oriented in a specific plane:
- The posterior canal detects movements of the head backward or to the side (such as lying down in bed).
- The superior (or anterior) channel detects forward flexions of the head (bending forward).
- The horizontal channel detects lateral rotations (turning the head to say “no”).
When otoliths (small calcium carbonate crystals) move abnormally in these canals, they disrupt the flow of fluid and send false information to the brain, causing vertigo.
Diagnostic tests for BPPV: Observe to better guide
Before considering a repositioning maneuver, it is essential to make an accurate diagnosis . Several clinical tests can identify the presence of benign paroxysmal positional vertigo (BPPV) and, importantly, locate the affected semicircular canal . These tests intentionally provoke symptoms in order to observe the reactions of the vestibular system—particularly through involuntary eye movements called nystagmus .
The Dix-Hallpike Test: Key to the Posterior Canal
The Dix-Hallpike test is most commonly used to diagnose BPPV affecting the posterior canal , the most frequently involved. It is performed as follows:
- The patient sits with their head turned 45° towards the tested side.
- The practitioner quickly lays the patient back, head tilted 20° below the horizontal (exceeding the edge of the table).
- The practitioner observes the patient’s eyes for 30 to 60 seconds.
Vertical rotatory nystagmus ( upward and torsional) and the onset of intense but brief vertigo usually confirm posterior canal involvement. The onset of nystagmus after a delay of a few seconds, followed by spontaneous resolution, is typical of BPPV.
The test is then repeated on the other side to compare the response. The side where the symptoms are most marked is the one usually affected.
The Roll Test (or lateral rotation test): for the horizontal channel
The Roll Test is used to assess the horizontal canal , the second most common location of BPPV. It is performed as follows:
- The patient is in a lying position, head in a neutral position.
- The practitioner turns the head 90° to one side, then to the other, while observing eye movements.
A horizontal (purely lateral) nystagmus then appears. Two forms can be distinguished:
- Geotropic (toward the ground) nystagmus : indicates a canalithic form.
- Apogeotropic nystagmus (towards the ceiling): suggests a cupulolithic shape.
The intensity of the nystagmus and vertigo allows the most affected side to be identified .
Importance of nystagmus direction
The type of nystagmus observed is a key diagnostic indicator:
- Rotatory and vertical upwards : posterior canal.
- Rotatory and vertical downwards : anterior canal (rare).
- Pure horizontal : horizontal channel (geotropic or apogeotropic shape).
These involuntary eye movements reflect abnormal activation of the vestibular system and allow the canal involved to be precisely located , an essential condition for applying the appropriate therapeutic maneuver.
Move to Heal: Otolith Repositioning Maneuvers
To treat BPPV, several canalithic maneuvers aim to put the otoliths back in place. Here is the most well-known:
The Epley maneuver (for the posterior canal)
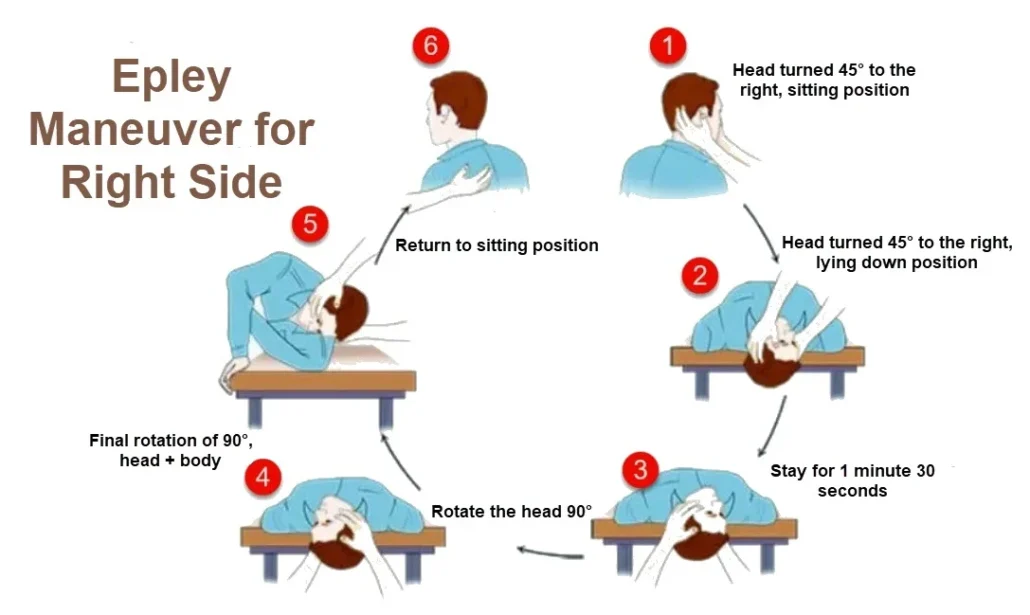
- Sit the patient with the head turned 45° towards the affected side.
- Quickly lay him on his back with his head slightly over the edge of the table.
- Hold the position for 30 seconds.
- Turn your head to the other side (still tilted back), 30 seconds.
- Turn your body to the unaffected side, head facing the floor.
- Wait another 30 seconds before gently straightening.
These movements help guide the otoliths to an area where they will no longer disturb the balance.
Other canalithic maneuvers (Semont, Gufoni, etc.)
While the Epley maneuver is the best known for treating benign paroxysmal positional vertigo (BPPV), it is not the only one. Its effectiveness depends on the semicircular canal involved , usually the posterior canal. However, otoliths can also migrate into the horizontal canal (more rarely, the anterior canal), requiring specific maneuvers adapted to the orientation of the affected canal. For comprehensive and personalized care, it is therefore important to be familiar with other canalith repositioning techniques.
The Semont (or liberatory) maneuver
The Semont maneuver is an alternative to the Epley maneuver for treating posterior canal BPPV . It is sometimes preferred when the patient does not tolerate prolonged head tilts well, or when a more “mechanical” response is desired.

This technique involves quickly moving the patient from a sitting position to a lying position on the affected side, then on the opposite side, in order to cause a sudden release of the otoliths. It is called “liberating” because it relies on centrifugal force to detach the debris from the cups. However, its execution requires more caution, as it is more abrupt and can temporarily intensify symptoms.
The Gufoni maneuver
Indicated in cases of BPPV of the horizontal canal , the Gufoni maneuver allows the otoliths to be repositioned in the utricle via lateral movements. It is particularly useful when dizziness occurs when turning the head in a lying position (a common sign of horizontal BPPV).

The patient is seated and then quickly laid down on the side opposite the affected canal, then their head is turned downward. After maintaining this position, they are gently straightened. This maneuver is well tolerated, relatively simple to perform, and often effective in one or two sessions.
The Lempert maneuver (or barbecue roll)
Another solution for BPPV of the horizontal canal , this technique consists of having the patient perform a series of successive 90° rotations, in a lying position, until returning to the supine position after a complete rotation of the body on a horizontal axis – hence its nickname “barbecue roll”.
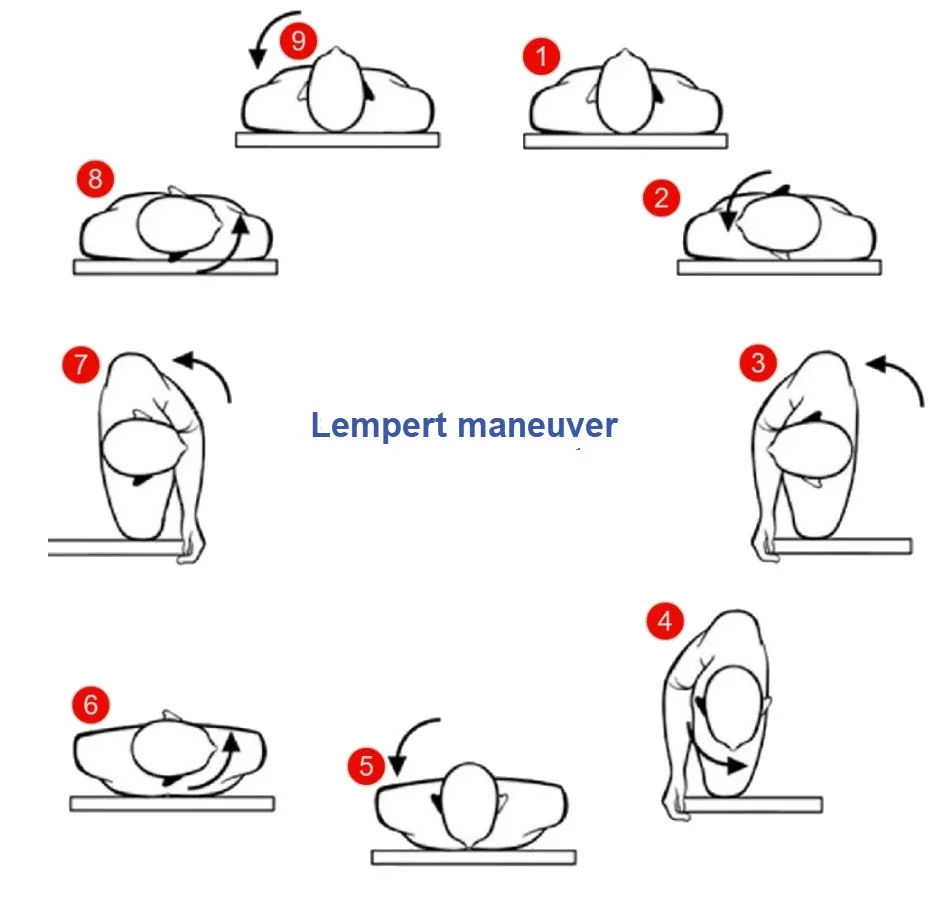
It allows the otoliths to be circulated along the entire length of the horizontal canal to bring them back to the utricle. Although longer, this maneuver is particularly useful in cases of refractory or recurrent forms.
And what about the anterior canal?
Anterior canal BPPV is rarer but can cause atypical vertigo. In this case, certain adaptations of the Epley maneuver, or the Yacovino maneuver (specific to the anterior canal), can be used. However, these techniques are less documented and should be applied by experienced professionals.
Choosing the right maneuver: a question of precise diagnosis
The choice of maneuver is based on the identification of the affected canal, often using specific tests such as the Dix-Hallpike (posterior canal) or the Roll Test (horizontal canal). The direction of the nystagmus, its lateralization, and the response to head movements are valuable indicators to guide the intervention.
👉 In osteopathic practice , it is essential to know these maneuvers to know when to direct the patient, adapt the treatment or integrate certain steps safely into an overall treatment. The objective remains the same: to promote the return to balance , minimize functional discomfort and prevent recurrences.
Osteopathy to the rescue: A holistic approach to vertigo
When faced with benign paroxysmal positional vertigo (BPPV), osteopathy offers much more than simple symptomatic relief. It offers a holistic reading of the body, seeking to identify and treat functional imbalances that can maintain or aggravate episodes of vertigo. Rather than limiting themselves to specific maneuvers to reposition otoliths, osteopaths explore the multiple interconnections between the musculoskeletal, nervous, cranial, and visceral systems. Here’s how this approach works in practice.
1. Cervical spine: regain mobility and proprioception
The cervical spine, particularly its upper portion (C0 to C3), plays a fundamental role in controlling balance. Sensory receptors in the cervical muscles and joints constantly send information to the brain to adjust posture and orient the head in space.
A restriction of mobility at the level of the cervical vertebrae can create a sensory conflict between visual, vestibular and proprioceptive data. This accentuates the sensation of imbalance, or even triggers or prolongs episodes of vertigo. The osteopath, through gentle techniques of joint mobilization , decompression or muscle relaxation , seeks to restore the fluidity of cervical movement and to soothe the reflex tensions which disrupt the perception of the body’s axis.
2. Cranial system and inner ear: subtle listening to movement
The inner ear, the seat of the vestibular system, lies at the heart of the temporal bone. Any tension, compression or imbalance in the latter can disrupt the labyrinthine function. The osteopath, using precise cranial techniques , assesses and treats the micro-mobilities of the bones of the skull, in particular the temporal , the sphenoid , but also the mandible , the tensions of which can have an impact on the cranio-cervical axis.
This work is often subtle, focusing on reharmonizing the intracranial membranes , releasing sutures, and improving the vascularization of the inner ear. In some cases, it may involve removing the after-effects of an old head trauma or emotional shock that may have affected the area.
3. Visceral and diaphragmatic regulation: calming the terrain
Vertigo is not just a mental issue. The autonomic nervous system , responsible for the balance between tension and relaxation in the body, is often compromised in people suffering from BPPV. Chronic stress , digestive or respiratory disorders can create a terrain of heightened reactivity , promoting episodes of vertigo or amplifying the symptoms (nausea, palpitations, fatigue).
The osteopath then explores the state of the visceral organs (liver, stomach, colon) as well as the mobility of the diaphragm , because any restriction in these areas can alter postural tone and the quality of breathing, two key elements in managing balance. Visceral and diaphragmatic work helps to restart exchanges, relieve internal tensions , and promote a return to a more stable body dynamic.
4. Postural advice and healthy lifestyle: prolonging the benefits of life
Osteopathic intervention isn’t limited to the treatment table. The osteopath also guides the patient in actively understanding their body and its habits. Personalized advice on sleep posture, gentle cervical mobility exercises, and stress management through breathing can help prevent recurrence.
For example, avoiding sudden movements upon waking, practicing regular stretching, or adopting suitable bedding are all simple but effective measures. Lifestyle, diet, and listening to your body also play a significant role in restoring overall balance.
How long until results? Patience and precision
The effects of an osteopathy session can be felt very quickly , sometimes within the first 24 to 48 hours. In the case of BPPV, a significant improvement can be observed in 1 to 3 sessions depending on the case. If symptoms persist beyond this, a referral to an ENT or neurologist may be necessary.
Osteopathic support acts as much on the symptoms as on the conditions that favor their appearance.
When to consult? Signs not to ignore
It is important to consult quickly if:
- Dizziness is recurrent or disabling.
- You have hearing loss, tinnitus or visual disturbances.
- Symptoms appear after head or neck trauma.
The Importance of Multidisciplinary Care
When faced with persistent, complex vertigo, or vertigo accompanied by atypical signs (hearing, visual, or neurological disorders, etc.), it is essential to adopt a collaborative approach between healthcare professionals. Osteopathy can play a complementary role, but it is never a substitute for a rigorous medical assessment when necessary.
Optimal management of vertigo often relies on consultation between several disciplines, including:
General practitioners: for an initial assessment and appropriate guidance.
ENT: for specific examinations of the inner ear and vestibular system.
Neurologists: in case of suspicion of central origin or underlying neurological pathology.
Physiotherapists in vestibular rehabilitation: to support functional recovery.
Psychologists or mental health professionals: when dizziness is associated with chronic anxiety or post-traumatic stress.
👉 The osteopath acts as a complement, never as a replacement, by providing a global reading of the body and working on mechanical, somatic or emotional imbalances that can influence the symptoms.
This multidisciplinary approach ensures safe, personalized and long-term patient care.
Signs of improvement after treatment
Improvement in BPPV following osteopathic treatment or canalithic maneuver is manifested by signs that are often clear and progressive. Here are the main ones:
- Disappearance or clear reduction of dizziness during triggering movements (lying down, getting up, turning the head).
- Reduction of the feeling of instability or floating in daily life.
- Reduction of nausea associated with dizzy episodes.
- Better postural anchoring and confidence in head or trunk movements.
- Improvement in the quality of sleep , often disturbed by the apprehension of triggering positions.
- Reduction or disappearance of nystagmus observed during certain tests (Dix-Hallpike, Roll test).
It is also common for patients to report emotional relief , related to the reduction of anticipatory anxiety about dizziness. Although some residual symptoms may persist for a few days (such as mild unsteadiness), their frequency and intensity tend to diminish quickly.
👉 To monitor : if dizziness persists without significant improvement after several sessions or maneuvers, a clinical reassessment and specialist referral (ENT, neurologist) are recommended.
Osteopathy for vertigo: a promising complementary approach in the treatment of BPPV
1. Contribution of structural osteopathy in the management of benign paroxysmal positional vertigo
Summary & Conclusion:
This thesis by Jonathan Donguy explores the osteopathic management of BPPV through structural techniques. The author points out that BPPV is caused by otolithic debris in the semicircular canals of the inner ear. Conventional medical treatment relies on canalithic maneuvers (such as Epley’s), but the study highlights the complementary value of osteopathy. Indeed, an osteopathic approach can reduce the frequency and intensity of vertigo episodes by rebalancing cervical, temporal, and occipital tensions. Work on the craniocervical junction and the proprioceptive system also improves the patient’s overall condition. The conclusion emphasizes that osteopathy, although not a substitute for conventional treatments, offers an effective complement to improve recovery and reduce recurrences.
2. Short-term impact of osteopathic treatment on concussion symptoms
Summary & Conclusion:
Although the study primarily addresses concussion, it addresses related symptoms such as dizziness and presents an osteopathic approach focused on the dura mater and corpus callosum. It demonstrates that cranial and myofascial manipulation can rapidly improve balance disorders and sensations of dizziness, even outside the purely vestibular context. The interest here is to explore how harmonization of intracranial tensions can indirectly influence the vestibular system and spatial perception. The author concludes that osteopathy, in a holistic approach, acts favorably on dizziness associated with post-traumatic disorders and could be considered as a broader therapeutic strategy in addition to the treatment of BPPV.
3. Accuracy of Dix-Hallpike test for the diagnosis of benign paroxysmal positional vertigo in adult patients
Summary & Conclusion:
This study, although focused on the diagnosis of BPPV via the Dix-Hallpike test, also indirectly addresses the effectiveness of the treatment. The author notes that osteopathy is rarely used, although it could complement the diagnosis by addressing cervical mechanical dysfunctions. The Dix-Hallpike test is considered very reliable for diagnosis, but patients often suffer from associated disorders (neck pain, headaches, etc.) that can be addressed by osteopathy. In conclusion, the study calls for interdisciplinary collaboration between ENT doctors and osteopaths to optimize the management of patients with vertigo, emphasizing that osteopathy can improve patient comfort by acting on associated mechanical factors.
4. Contribution of structural osteopathy in the management of benign paroxysmal positional vertigo
Summary & Conclusion:
This thesis by Jonathan Donguy explores the osteopathic management of BPPV through structural techniques. The author points out that BPPV is caused by otolithic debris in the semicircular canals of the inner ear. Conventional medical treatment relies on canalithic maneuvers (such as Epley’s), but the study highlights the complementary value of osteopathy. Indeed, an osteopathic approach can reduce the frequency and intensity of vertigo episodes by rebalancing cervical, temporal, and occipital tensions. Work on the craniocervical junction and the proprioceptive system also improves the patient’s overall condition. The conclusion emphasizes that osteopathy, although not a substitute for conventional treatments, offers an effective complement to improve recovery and reduce recurrences.
5. Short-term impact of osteopathic treatment on concussion symptoms
Summary & Conclusion:
Although the study primarily addresses concussion, it addresses related symptoms such as dizziness and presents an osteopathic approach focused on the dura mater and corpus callosum. It demonstrates that cranial and myofascial manipulation can rapidly improve balance disorders and sensations of dizziness, even outside the purely vestibular context. The interest here is to explore how harmonization of intracranial tensions can indirectly influence the vestibular system and spatial perception. The author concludes that osteopathy, in a holistic approach, acts favorably on dizziness associated with post-traumatic disorders and could be considered as a broader therapeutic strategy in addition to the treatment of BPPV.
6. Accuracy of Dix-Hallpike test for the diagnosis of benign paroxysmal positional vertigo in adult patients
Summary & Conclusion:
This study, although focused on the diagnosis of BPPV via the Dix-Hallpike test, also indirectly addresses the effectiveness of the treatment. The author notes that osteopathy is rarely used, although it could complement the diagnosis by addressing cervical mechanical dysfunctions. The Dix-Hallpike test is considered very reliable for diagnosis, but patients often suffer from associated disorders (neck pain, headaches, etc.) that can be addressed by osteopathy. In conclusion, the study calls for interdisciplinary collaboration between ENT doctors and osteopaths to optimize the management of patients with vertigo, emphasizing that osteopathy can improve patient comfort by acting on associated mechanical factors.
Conclusion
Vertigo, particularly that associated with benign paroxysmal positional vertigo (BPPV), can be profoundly destabilizing. Although rarely physically serious, it has a significant impact on quality of life: anxiety, loss of confidence, fear of movement, social isolation, and even a feeling of loss of control. Every movement becomes a source of anticipation, heightened vigilance, and sometimes even fear.
Fortunately, targeted and integrated care can transform this disabling experience into an opportunity for refocusing. Well-performed canalithic maneuvers —Epley, Semont, Gufoni, or others—often provide rapid relief by returning the otoliths to a position where they no longer interfere with balance.
But beyond this technical gesture, osteopathy offers a holistic view : it doesn’t stop at the inner ear, but examines the interconnections between systems. The skull, the cervical vertebrae, posture, the diaphragm, the autonomic nervous system, even emotions—everything is perceived as a living and coherent whole. Because the head doesn’t float alone in space: it is guided, supported, and balanced by its surroundings.
The osteopath then explores the mechanical, functional, and contextual factors that promote or maintain vestibular disorders. A cervical blockage, diaphragmatic tension, postural imbalance, chronic unexpressed stress… all of these elements can contribute to maintaining a breeding ground for vertigo. The treatment then becomes an invitation to reharmonize internal and external movements.
Dizziness may not just be disrupted signals from the inner ear. It’s sometimes the body’s silent language as it tries to regain some form of stability—physical, emotional, mental. It’s the body’s way of saying, “I’m losing my bearings, help me refocus.”
Osteopathy therefore doesn’t just aim to relieve a symptom. It seeks to restore balance in all its dimensions : biomechanical, neurological, energetic, and psychological. It offers a framework for listening, observation, and understanding—a space in which the patient can not only regain their sense of support, but also their autonomy.
References
Scientific and medical references (anatomy, diagnosis, treatment)
- Bhattacharyya N, et al. (2017). Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update).
Otolaryngology–Head and Neck Surgery , 156(3_suppl), S1–S47.
👉 Official recommendations from the American Academy of Otolaryngology. - von Brevern M, Bertholon P, Brandt T, Fife T, Imai T, Nuti D, Newman-Toker DE. (2015). Benign paroxysmal positional vertigo: Diagnostic criteria.
Journal of Vestibular Research , 25(3-4), 105-117. - Furman JM, Cass SP. (2003). Benign paroxysmal positional vertigo.
New England Journal of Medicine , 349(10), 938–944.
👉 Reference article for general public + professionals. - Hilton MP, Pinder DK. (2014). The Epley (canalith repositioning) maneuver for benign paroxysmal positional vertigo.
Cochrane Database of Systematic Reviews , Issue 12.
👉 Systematic review on the effectiveness of the Epley maneuver. - Mandala M, Santoro GP, Asprella Libonati G, Casani AP. (2013). Double-blind randomized trial on efficacy of Semont’s maneuver for posterior canal BPPV.
Neurology , 80(12), 1205–1211. - Hain TC, Helminski JO. (2007). Update on benign paroxysmal positional vertigo.
Current Opinion in Neurology , 20(1), 40–46.
Neuroscience / Vestibular Physiology Resources
- Guyton & Hall (2020). Medical Physiology , 14th ed.
👉 Chapter on balance, inner ear, and vestibular function. - Baloh RW, Honrubia V. (2001). Clinical Neurophysiology of the Vestibular System , 3rd edition.
Oxford University Press.
👉 Reference for functional anatomy and clinical testing.
Osteopathic and complementary references
- Chaitow L, DeLany J. (2011). Clinical Application of Neuromuscular Techniques, Volume 2: The Lower Body , 2nd edition.
👉 Myofascial, visceral and integrative approach in vertigo. - Barral JP, Croibier A. (2010). Osteopathy and the Treatment of Vertigo.
Thieme Medical Publishers.
👉 Specific to the osteopathic approach to vestibular disorders. - Vleeming A et al. (2007). Osteopathy: Models for Diagnosis, Treatment, and Practice.
👉 A global and interdisciplinary vision of osteopathic treatment.
Additional clinical sites and resources
- VEDA (Vestibular Disorders Association)
https://vestibular.org
👉 Patient and professional information, test and maneuver information sheets. - NHS UK – Benign Paroxysmal Positional Vertigo (BPPV)
https://www.nhs.uk/conditions/benign-paroxysmal-positional-vertigo-bppv/
👉 Simplified and clear explanation.













{kind=link}