

Introduction
Lumbar disc herniation is a feared spinal condition that can cause severe pain and significantly impair quality of life. To better understand this condition, let’s explore the complex anatomy of the lumbar spine, the underlying mechanisms of herniated disc, potential causes, associated symptoms, management recommendations, research advances, and the role of osteopathy in this adventure.
The lumbar spine is made up of five vertebrae (L1 to L5) located in the lower part of the back, between the thoracic spine and the sacrum. These vertebrae support the body’s weight and allow a range of motion, but they are also prone to various conditions, including herniated discs.
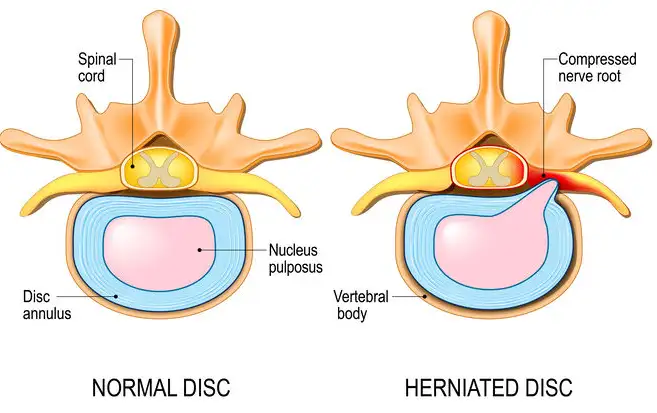
Disc herniation occurs when the gelatinous core of the intervertebral disc extends beyond its outer structure, putting pressure on adjacent nerves. Causes may include aging, genetics, trauma, or overuse of the spine.
Symptoms of a herniated disc vary, but can include severe lower back pain, numbness, tingling, and weakness in the legs. Treatment may include medications, physical therapy, lifestyle changes, and in some cases, surgery.
Research is continually exploring new approaches to treating herniated discs, such as gene therapy or the use of stem cells. Osteopathy, a holistic approach, can play a role in managing symptoms by improving the body’s mobility and balance.
X-ray images, such as MRI or CT, are used to diagnose a herniated disc by visualizing the structure of the spine. In conclusion, lumbar disc herniation requires a multidisciplinary approach for effective management, with continued advances providing new perspectives to provide relief to patients affected by this debilitating spinal condition.
The Historical Evolution of Understanding Lumbar Hernia
Antiquity: The Foundations of Knowledge about the Spine
The earliest recorded explorations of spinal anatomy date back to ancient Egypt and Greece. Egyptian medical papyri, such as the Edwin Smith Papyrus (c. 1600 BCE), suggest an understanding of spinal trauma and its potential to cause paralysis. However, these writings focused primarily on traumatic injuries rather than degenerative conditions such as lumbar herniation.
The Greek physician Hippocrates (460–370 BC), often considered the “Father of Medicine,” contributed significantly to early knowledge of the spine. He documented various spinal deformities and introduced rudimentary methods of traction to treat spinal injuries. Despite these advances, the concept of intervertebral discs and their role in lumbar herniation remained unknown.
The Middle Ages: Stagnation and Survival
During the Middle Ages, which spanned the 5th to the 15th century, medical knowledge in Europe was marked by a notable stagnation. This period, dominated by socio-political instability and a strong influence of religious doctrines, limited scientific advances. Diseases and conditions, particularly those related to the spine, were often interpreted through the prism of supernatural beliefs or as divine punishments, relegating anatomical or physiological explanations to the background.
In the Islamic world, however, a different dynamic developed. As Europe went through a phase of withdrawal, Islamic scholars undertook a vital task: the preservation, translation, and enrichment of medical knowledge inherited from the Greeks and Romans. Eminent figures such as Avicenna (980–1037 CE), a physician, philosopher, and scholar, played a central role in this effort. His monumental work, The Canon of Medicine , was a major reference for centuries. In it, he addressed various disorders, including those related to the spine, laying the foundations for a rational and methodical approach. However, some specific structures such as intervertebral discs or herniated discs were not mentioned in his writings, reflecting the limitations of knowledge at the time, even in the enlightened context of the Islamic world.
Thus, if medieval Europe was marked by a delay in the medical field, the legacy of Islamic scholars made it possible to preserve and transmit the bases of future advances, creating a bridge between Antiquity and the Renaissance.
The Renaissance: The Renaissance of Anatomical Exploration
The Renaissance, which spanned the 14th to the 17th century, marked a turning point in the history of science and medicine. This period was characterized by a revival of scientific investigation, anatomical exploration, and the questioning of dogmas inherited from the Middle Ages. Advances in human dissection, previously prohibited or limited, provided a more precise understanding of the human body and its complex structures, including the spinal column.
Among the leading figures of this era, Andreas Vesalius (1514–1564) stood out as a pioneer of modern anatomy. In 1543, he published De Humani Corporis Fabrica , a groundbreaking treatise that combined a rigorous scientific approach with remarkably precise illustrations. These drawings, made with the help of talented artists, offered a detailed representation of the human spine, from the individual vertebrae to the surrounding structures, including ligaments and muscles.
Although Vesalius did not explicitly describe lumbar herniations or the role of intervertebral discs, his work established an essential foundation for future anatomical and clinical explorations. He broke with the outdated ideas of Galen, whose descriptions were largely based on animal dissections, by asserting the importance of direct observation on human cadavers. His revolutionary approach paved the way for a deeper understanding of spinal pathologies, contributing to the gradual evolution toward modern medicine.
The Renaissance was therefore a pivotal period when art, science and anatomy met, laying the foundations for major medical discoveries that transformed our understanding of the human body.
The 19th Century: The Birth of Modern Spinal Medicine
The 19th century was a transformative period for medical science, marked by significant advances in the understanding of the anatomy and physiology of the spine. The identification and in-depth study of the intervertebral discs was a key step in this progression.
In 1857, German anatomist Rudolf Virchow, considered one of the fathers of modern pathology, accurately described the structure of the intervertebral discs. He highlighted their essential role as shock absorbers, distributing and absorbing mechanical stresses on the spine. This revolutionary discovery laid the foundation for the biomechanical understanding of the spine and sparked a growing interest in disc-related pathologies.
In the decades that followed, researchers expanded on this work, establishing links between degeneration of the intervertebral discs and clinical symptoms such as low back pain. Around 1880, the concept of a herniated disc appeared in the medical literature. Surgeons began reporting cases of sciatica that they attributed to “displaced tissue” in the spine, a description that fit what is now known as protrusion or extrusion of the intervertebral discs.
These pioneering observations laid the foundation for understanding the relationship between disc pathology and conditions such as low back pain and radiculopathies. Although modern diagnostic techniques, such as magnetic resonance imaging (MRI), were still lacking at the time, these early clinical descriptions were crucial in guiding medical research and the development of appropriate treatments.
Thus, the 19th century marked the beginning of a new era in the study of spinal disorders, with discoveries that continue to shape the management of spinal conditions to this day.
The Beginning of the 20th Century: The Discovery of the Herniated Disc
The early 20th century marked a turning point in the understanding and management of lumbar herniation, with scientific and clinical advances that laid the foundations of modern spinal medicine. In 1934, American neurologists William Jason Mixter and Joseph Barr published a groundbreaking study that formally identified intervertebral disc herniation as a major cause of sciatica.

Their work was based on careful surgical observations and demonstrated that displaced disc material could compress nerve roots in the spine, leading to symptoms such as severe pain, numbness, muscle weakness, and other neurological deficits. Prior to this publication, understanding of sciatica and associated low back pain remained fragmentary, often attributed to “rheumatism” or poorly defined causes.
This discovery transformed the medical landscape by establishing a direct link between intervertebral disc pathologies and neurological disorders. It also revolutionized clinical and surgical practices. Among the most significant innovations was laminectomy, a surgical procedure designed to remove herniated disc material and relieve nerve compression. This procedure quickly became the standard treatment for severe cases of lumbar herniation, providing significant relief to many patients previously disabled by their condition.
Mixter and Barr’s study was not only a technical breakthrough, but also a cornerstone in the evolution of spinal medicine. It inspired decades of research and innovation, contributing to the development of less invasive surgical techniques and improved strategies for managing disc pathologies. Even today, their work is cited as a major historical reference in the field of spinal disorders, testifying to the importance of their contribution to modern medicine.
The Mid-20th Century: Advances in Imaging and Treatment
The mid-20th century was marked by technological innovations that improved the diagnosis and management of lumbar disc herniation. The introduction of myelography, followed by computed tomography (CT) and magnetic resonance imaging (MRI), allowed precise visualization of spinal structures. These imaging techniques revolutionized the ability to diagnose disc herniations noninvasively.
At the same time, advances in surgical techniques improved outcomes for patients with lumbar hernias. Microdiscectomy, introduced in the 1970s, reduced tissue damage and recovery times compared with traditional open surgeries. Nonsurgical treatments, such as physical therapy and epidural steroid injections, also gained importance, providing alternatives for managing less severe cases.
The End of the 20th and the Beginning of the 21st Century: A Multidisciplinary Approach
As understanding of lumbar herniation deepened, the late 20th and early 21st centuries saw a shift toward multidisciplinary care. Researchers emphasized the importance of addressing biomechanical and psychosocial factors in the treatment of low back pain and lumbar herniation. This holistic approach integrated osteopathy, chiropractic, physical therapy, and behavioral interventions.
Additionally, minimally invasive surgical techniques, such as endoscopic discectomy and laser-assisted procedures, became increasingly popular. These methods aimed to reduce recovery times and complications, making surgery more accessible and less feared by patients.
Current Perspectives: Personalized and Regenerative Medicine
Today, the understanding of lumbar herniation continues to evolve, driven by advances in personalized and regenerative medicine. Stem cell therapies and biologic treatments aim to restore disc integrity and function, offering hope for nonsurgical solutions. Artificial disc replacement and other innovative surgical techniques are also expanding the options available to patients.
In addition, ongoing research highlights the importance of early diagnosis and prevention. Ergonomics, core strengthening exercises and lifestyle modifications play a crucial role in reducing the risk of lumbar hernia and its recurrence.
Anatomy of the Lumbar Spine
The intervertebral discs, located between the vertebrae of the spine, play a crucial role as cushions providing the flexibility and strength necessary for this complex structure. The spine consists of twenty-four movable vertebrae, while five of them fuse together to form the sacrum. Discs, subject to injury, must combine sufficient flexibility to allow movement and robustness capable of withstanding considerable stress. The lower lumbar discs, in supporting the weight of the upper body, are particularly vulnerable and frequently subject to injury.
The structure of a disc consists of a rigid outer layer called the “annulus fibrosus” surrounding a gelatinous center called the “nucleus pulposus.” With aging, the nucleus pulposus gradually loses its hydration level, thus reducing its effectiveness as a cushion. A herniated disc occurs when the nucleus pulposus escapes through the outer annulus fibrosus, causing the center of the disc, also known as a herniated or ruptured disc, to move through a crack in the outer layer. Terms such as disc herniation, rupture, protrusion, and extrusion all describe this injury, although with subtle nuances. They refer to a tear in the outer ring allowing part of the inner core to escape.
The majority of herniated discs occur in the lower two discs of the lumbar spine. A lumbar disc herniation can put pressure on the nerves in the spine, leading to symptoms such as pain, numbness, tingling, or weakness in the leg, commonly known as “sciatica.” Sciatica affects approximately 1 to 2% of the population, mainly between the ages of 30 and 50.
Pathophysiology of Lumbar Disc Herniation
Here are the stages of the pathophysiology of lumbar disc herniation in a clear and precise manner:
- Trauma or Wear:
- A herniated disc can result from acute trauma, such as improper lifting of heavy objects, or from gradual wear and tear due to aging and natural wear and tear of the intervertebral discs.
- Disc Degradation:
- The intervertebral disc undergoes degenerative changes over time. Dehydration of the nucleus pulposus and loss of elasticity of the annulus fibrosus make the disc more vulnerable to cracking.
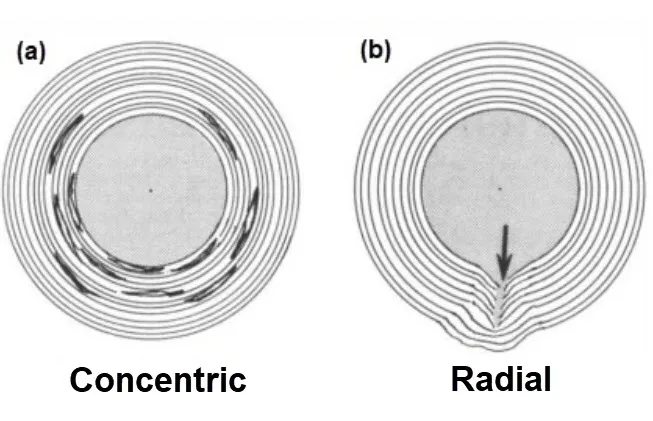
- Fibrosus Ring Cracking:
- Due to wear and tear, the annulus fibrosus may develop cracks or tears. These cracks can allow the nucleus pulposus to move out of its normal position.
- Protrusion of the nucleus pulposus:
- The nucleus pulposus, or part of it, may protrude through the crack in the annulus fibrosus. This forms a protrusion or protrusion of the disc, sometimes called a herniation.
- Nerve Root Compression:
- Disc protrusion can put pressure on nerve roots that emerge from the nearby spinal cord. This can lead to irritation of the nerves and cause symptoms such as pain, numbness or muscle weakness in the lumbar region, buttocks, legs and sometimes even the feet.
- Inflammatory Response:
- Compression of nerve roots triggers a local inflammatory response, contributing to the intensification of symptoms. The inflammation can also irritate surrounding nerves.
- Muscular and Postural Reaction:
- To protect the spine and compensate for pain, surrounding muscles may contract involuntarily, leading to altered posture and sometimes muscle spasms.
- Clinical Symptoms:
- Symptoms of lumbar disc herniation can vary depending on the location of the protrusion and the affected nerve root. These symptoms include lower back pain, sciatica (pain along the sciatic nerve), numbness, muscle weakness, and possibly problems with bladder or bowel control.
Narrowing of the posterior longitudinal ligament
The posterior longitudinal ligament (PLL) is a fibrous structure found at the back of the spine, within the spinal canal. It extends along the posterior surface of the vertebrae and helps hold the intervertebral discs in place. When there is narrowing of the posterior longitudinal ligament, it can lead to symptoms that are often related to compression of the spinal cord or nerve roots in the spinal canal.
When there is narrowing of the posterior longitudinal ligament in association with a lumbar disc herniation, this can worsen symptoms by increasing compression of the nerve structures in the spinal canal. Symptoms may include lower back pain, pain radiating down the buttocks and legs, muscle weakness, numbness and tingling.
Causes of Lumbar Disc Herniation
- Aging: The natural aging process causes changes in the intervertebral discs. Over time, discs lose their elasticity and ability to absorb shock, making them more prone to herniation.
- Wear and Tear: Repetitive movements or overuse of the spine, often associated with certain jobs or activities, can cause wear and tear of the intervertebral discs.
- Poor Body Mechanics: Adopting poor posture, lifting heavy objects incorrectly, or making sudden movements without using supporting muscles can increase the risk of a herniated disc.
- Obesity: Excessive weight can put additional pressure on the intervertebral discs, increasing the risk of disc herniation.
- Genetics: Some individuals may be genetically predisposed to developing intervertebral disc problems, increasing their susceptibility to herniations.
- Sedentary Lifestyle: Low physical activity and lack of exercise can contribute to weakness in the supporting muscles of the spine, increasing the risk of herniated discs.
- Trauma: Trauma, such as a car accident, a fall, or a direct blow to the spine, can lead to a herniated disc.
- Genetic Factors: Genetic factors may play a role in predisposing to conditions such as disc degeneration, thereby increasing the risk of disc herniation.
What levels do lumbar disc herniation occur most often?
L4-5 > L5-S1 > L3-4 > L2-3 > L1-2
Symptoms of Lumbar Herniation
Lumbar herniation, also known as a herniated disc in the lower back, occurs when the soft inner material of an intervertebral disc (nucleus pulposus) protrudes through a tear or weakness in its outer layer (annulus fibrosus). This condition can compress nearby spinal nerves, leading to a range of symptoms. These symptoms vary in severity depending on the location and extent of the herniation, as well as the specific nerve roots affected. Below are the common symptoms associated with lumbar herniation:
1. Lower Back Pain
- One of the earliest and most common symptoms of lumbar herniation is localized pain in the lower back. This pain is often described as dull, aching, or sharp, depending on the severity of the condition. It may worsen with activities that increase spinal pressure, such as bending, lifting, or prolonged sitting.
2. Radicular Pain (Sciatica)
- A hallmark symptom of lumbar herniation is radiating pain that travels from the lower back down one or both legs, following the path of the affected nerve root. This condition is commonly referred to as sciatica. The pain may extend into the buttocks, thighs, calves, or feet and is often described as sharp, burning, or electric-like. It is typically unilateral but can affect both sides if the herniation is central and large.

3. Numbness and Tingling
- Compression or irritation of spinal nerves can lead to sensory changes in the lower extremities. Patients may experience numbness, tingling, or a “pins and needles” sensation, particularly in the areas served by the affected nerve. For example, a herniation at the L5 level may cause numbness along the outer side of the leg and into the foot.
4. Muscle Weakness
- Lumbar herniation can interfere with the motor signals traveling to the muscles. This may result in weakness in the legs, making it difficult to perform specific movements, such as lifting the foot (foot drop) or standing on tiptoes. Muscle weakness is a concerning symptom and may indicate significant nerve compression.
5. Loss of Reflexes
- In some cases, lumbar herniation affects the reflexes controlled by the compressed nerve roots. Reflexes, such as the knee-jerk or ankle-jerk reflex, may be diminished or absent upon clinical examination.
6. Worsening Pain with Movement
- Certain activities or positions, such as coughing, sneezing, or sitting for extended periods, can exacerbate symptoms. This occurs because these actions increase pressure within the spinal column, worsening nerve compression.
7. Changes in Posture
- To avoid pain, individuals with lumbar herniation may adopt abnormal postures or movement patterns, such as leaning to one side or walking with a limp.
8. Cauda Equina Syndrome (Emergency Symptom)
- In rare and severe cases, a large herniation may compress the cauda equina, a bundle of nerves at the lower end of the spinal cord. This can lead to symptoms such as loss of bladder or bowel control, severe weakness in both legs, and numbness in the saddle area (inner thighs, buttocks). This is a medical emergency requiring immediate treatment.
Diagnostic Methods
Clinical and Neurological Evaluation in Osteopathy
Osteopaths begin their diagnostic process by performing a detailed clinical evaluation, which includes obtaining a thorough patient history and conducting a physical and neurological examination. This process allows the practitioner to identify key symptoms, assess their severity, and pinpoint the areas of dysfunction.
- Patient History
The osteopath begins by collecting detailed information about the patient’s symptoms, lifestyle, and medical history. Questions may include:- When did the pain start, and what triggered it?
- Is the pain localized or radiating to other areas, such as the legs or feet?
- Are there specific activities or postures that worsen or alleviate the pain?
- Has the patient experienced numbness, tingling, or muscle weakness? Gathering this information helps the osteopath understand the nature of the condition and potential contributing factors, such as poor posture, repetitive stress, or trauma.
- Physical Examination
The physical examination involves assessing the patient’s posture, range of motion, and areas of tenderness. The osteopath palpates the lumbar spine and surrounding tissues to detect signs of muscle tension, inflammation, or misalignment. - Neurological Assessment
A detailed neurological evaluation is crucial for identifying nerve root involvement, which is common in lumbar disc herniation. This may include:- Reflex Testing: Assessing reflexes such as the patellar (knee) and Achilles reflex to determine nerve function.
- Sensory Testing: Evaluating areas of numbness or tingling to identify affected nerve pathways.
- Motor Strength Testing: Examining muscle strength, particularly in the lower extremities, to detect weakness caused by nerve compression.
- Straight Leg Raise Test: This specific test helps identify sciatic nerve involvement. The patient lies on their back while the osteopath gently raises one leg. Pain or discomfort in the lower back or along the sciatic nerve pathway can indicate nerve root irritation.
Through this evaluation, the osteopath identifies the location and severity of the herniation, as well as potential compensatory patterns that may contribute to the patient’s discomfort.
Medical Imaging: MRI and CT Scans
In many cases, medical imaging is necessary to confirm the diagnosis of a lumbar disc herniation and evaluate its impact on surrounding structures. MRI and CT scans are the most commonly used imaging modalities for this purpose.
- Magnetic Resonance Imaging (MRI)
MRI is the gold standard for diagnosing lumbar disc herniation. This imaging technique uses magnetic fields and radio waves to produce detailed images of soft tissues, including:- Intervertebral Discs: Visualizing the extent of the herniation and detecting tears in the annulus fibrosus or protrusion of the nucleus pulposus.
- Nerve Roots and Spinal Cord: Identifying compression or inflammation caused by the herniation.
- Surrounding Structures: Detecting secondary issues, such as ligament thickening or muscle spasms. MRI provides a comprehensive view of the affected area, allowing practitioners to assess the severity of the herniation and guide treatment decisions.

- Computed Tomography (CT) Scans
CT scans are another valuable tool for diagnosing lumbar disc herniation, particularly when MRI is unavailable or contraindicated. CT uses X-rays to create cross-sectional images of the spine, providing detailed information about:- Bone structures, such as vertebrae and facet joints.
- Calcifications or bony growths (osteophytes) that may exacerbate nerve compression.
- Disc abnormalities, though less detailed than MRI for soft tissues.
- Additional Imaging Techniques
- X-Rays: Although less informative for soft tissues, X-rays can reveal structural changes like reduced disc height or spinal misalignment.
- Myelography: In some cases, contrast-enhanced imaging is used to assess nerve compression within the spinal canal.
The Role of Imaging in Osteopathic Diagnosis
While osteopaths rely heavily on hands-on evaluations, imaging results are invaluable for confirming diagnoses and ruling out other conditions. They use imaging findings to complement their manual assessments, tailoring treatment plans that address both the structural and functional aspects of the condition.
Exercise and Prevention for Lumbar Disc Herniation
Exercise and prevention are crucial components in managing lumbar disc herniation and reducing the risk of recurrence. A targeted approach involving stretches, core strengthening, ergonomic practices, and lifestyle adjustments can help alleviate symptoms, enhance mobility, and maintain spinal health. These strategies promote resilience against future injury and empower individuals to take control of their recovery and well-being.
Stretches, Core Strengthening, and Ergonomic Practices
Engaging in regular exercise tailored to support spinal health plays a pivotal role in preventing the progression of lumbar disc herniation and promoting recovery.
- Stretches to Improve Flexibility and Relieve Tension
Stretching helps release tension in the muscles surrounding the lumbar spine and improves overall flexibility. Key stretches include:- Child’s Pose: A gentle yoga stretch that elongates the spine and relieves lower back tension.
How to do it: Start on hands and knees, lower your hips back toward your heels, and extend your arms forward. Hold for 20–30 seconds. - Hamstring Stretch: Tight hamstrings can contribute to lower back strain. Stretching them reduces stress on the lumbar spine.
How to do it: Lie on your back, extend one leg upward, and gently pull it toward you using a towel or strap. Hold for 20–30 seconds on each leg. - Cat-Cow Stretch: Improves spinal mobility and reduces stiffness.
How to do it: On hands and knees, alternate between arching your back (cat) and dipping your belly while lifting your head and hips (cow). Repeat 10 times.
- Child’s Pose: A gentle yoga stretch that elongates the spine and relieves lower back tension.
- Core Strengthening to Stabilize the Spine
A strong core provides stability and reduces the strain on intervertebral discs. Focus on exercises that engage the deep core muscles without causing excessive spinal load:- Pelvic Tilts: Strengthen the abdominal muscles while promoting spinal flexibility.
How to do it: Lie on your back with knees bent, flatten your back against the floor by tightening your abs, and hold for 5 seconds. Repeat 10 times. - Modified Planks: Build core strength without overloading the lower back.
How to do it: Start on your forearms and knees, keeping your back straight. Hold the position for 10–20 seconds and gradually increase the duration. - Bridges: Activate the glutes and lower back muscles to support spinal alignment.
How to do it: Lie on your back with knees bent, lift your hips to create a straight line from shoulders to knees, hold for 5 seconds, and lower back down.
- Pelvic Tilts: Strengthen the abdominal muscles while promoting spinal flexibility.
- Ergonomic Practices to Protect the Spine
Proper ergonomics minimizes strain on the lumbar region during daily activities.- Use chairs with lumbar support that encourage a neutral spine position.
- Adjust your workstation so the computer screen is at eye level, and your feet rest flat on the floor.
- Avoid prolonged sitting; stand and stretch every 30–60 minutes.
- Practice safe lifting techniques: bend at the knees, keep the load close to your body, and avoid twisting movements.
Tips for Preventing Recurrence
Preventing the recurrence of lumbar disc herniation involves making consistent, healthy lifestyle choices to support spinal health.
- Maintain Regular Physical Activity
Engage in low-impact activities like walking, swimming, or cycling to strengthen muscles and improve circulation. Regular movement keeps the discs hydrated and reduces stiffness. - Adopt a Balanced Diet
A nutrient-rich diet supports spinal health by providing essential vitamins and minerals. Focus on:- Calcium and Vitamin D for bone strength.
- Omega-3 fatty acids to reduce inflammation.
- Adequate hydration to maintain disc elasticity.
- Prioritize Posture
Poor posture increases strain on the lumbar spine.- Keep your back straight and shoulders relaxed when sitting or standing.
- Avoid slouching or prolonged positions that compress the spine.
- Manage Body Weight
Excess weight puts additional pressure on the intervertebral discs. Maintaining a healthy weight through proper nutrition and exercise reduces stress on the spine. - Reduce Repetitive Strain
Avoid repetitive bending, twisting, or heavy lifting. Use tools or equipment to assist with demanding tasks. - Stress Management
Chronic stress can cause muscle tension, increasing strain on the back. Incorporate relaxation techniques such as meditation, deep breathing, or yoga to reduce tension.
It is crucial to remember that each person responds differently to exercises, and it is essential to proceed with caution.
Therapeutic Advances: Innovations in Cell-Based and Genetic Therapies and the Role of Osteopathy
The treatment landscape for lumbar disc herniation has seen remarkable advancements, particularly with the advent of cell-based and genetic therapies that target the root causes of disc degeneration. These innovations, paired with the integrative role of osteopathy, represent a holistic approach to managing this complex condition. This dual focus not only addresses the structural issues of the spine but also supports the body’s natural healing processes, offering new hope for long-term recovery.
Innovations in Cell-Based and Genetic Therapies
1. Stem Cell Therapy
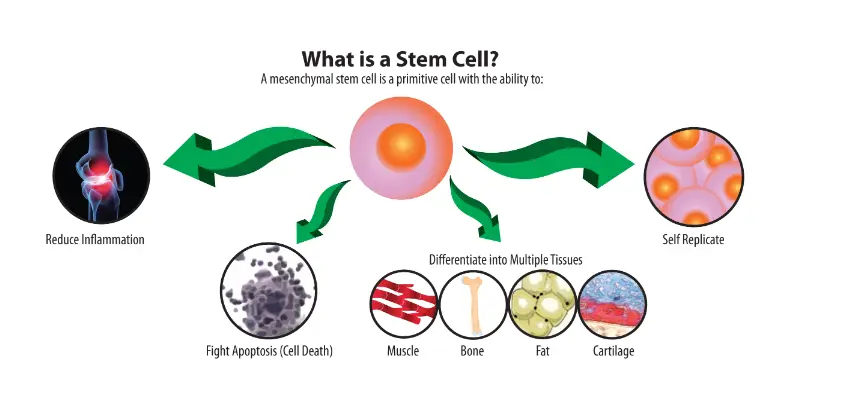
Gene therapy represents an innovative and promising approach to addressing disc degeneration by directly targeting the molecular mechanisms underlying this condition. This technique involves modifying or introducing specific genes into the intervertebral discs to achieve precise and lasting therapeutic effects. The primary objectives of gene therapy in this context include:
- Stimulating the synthesis of essential structural proteins, such as collagen, which is crucial for maintaining the strength and resilience of the intervertebral disc.
- Inhibiting tissue-degrading enzymes, particularly matrix metalloproteinases (MMPs), which play a significant role in the breakdown of the extracellular matrix.
- Activating anti-inflammatory pathways to reduce chronic inflammation often associated with disc degeneration, alleviating pain and protecting surrounding tissues from further damage.
In France, significant progress is being made in the development of viral vectors and nanoparticles, which are essential tools for delivering therapeutic genes with precision. These advancements not only enhance the efficacy of treatments but also improve their safety by minimizing the risk of side effects. For instance, modified viral vectors designed to specifically target intervertebral disc cells reduce interactions with other tissues. Similarly, biodegradable nanoparticles provide a non-viral alternative that is often better tolerated by the body.
These innovations pave the way for exciting possibilities in the treatment of disc degeneration, a condition that remains challenging to manage with traditional methods. However, while gene therapy is advancing rapidly, it faces several hurdles, including regulatory challenges for clinical application, high development costs, and the need to assess long-term outcomes. Clinical trials are currently underway to refine these strategies and evaluate their safety and efficacy in broader patient populations.
2. Gene Therapy
Gene therapy represents an innovative and promising approach to addressing disc degeneration by directly targeting the molecular mechanisms underlying this condition. This technique involves modifying or introducing specific genes into the intervertebral discs to achieve precise and lasting therapeutic effects. The primary objectives of gene therapy in this context include:
- Stimulating the synthesis of essential structural proteins, such as collagen, which is crucial for maintaining the strength and resilience of the intervertebral disc.
- Inhibiting tissue-degrading enzymes, particularly matrix metalloproteinases (MMPs), which play a significant role in the breakdown of the extracellular matrix.
- Activating anti-inflammatory pathways to reduce chronic inflammation often associated with disc degeneration, alleviating pain and protecting surrounding tissues from further damage.
In France, significant progress is being made in the development of viral vectors and nanoparticles, which are essential tools for delivering therapeutic genes with precision. These advancements not only enhance the efficacy of treatments but also improve their safety by minimizing the risk of side effects. For instance, modified viral vectors designed to specifically target intervertebral disc cells reduce interactions with other tissues. Similarly, biodegradable nanoparticles provide a non-viral alternative that is often better tolerated by the body.
These innovations pave the way for exciting possibilities in the treatment of disc degeneration, a condition that remains challenging to manage with traditional methods. However, while gene therapy is advancing rapidly, it faces several hurdles, including regulatory challenges for clinical application, high development costs, and the need to assess long-term outcomes. Clinical trials are currently underway to refine these strategies and evaluate their safety and efficacy in broader patient populations.
3. Growth Factors and Biomaterials
The use of growth factors, such as transforming growth factor-beta (TGF-β) and platelet-derived growth factor (PDGF), represents a groundbreaking area of research aimed at stimulating the repair and regeneration of intervertebral discs. These biologically active molecules play a critical role in modulating cellular activity, promoting the proliferation and differentiation of cells necessary for tissue repair. Specifically, TGF-β has been shown to enhance the synthesis of extracellular matrix components, such as collagen and proteoglycans, which are essential for maintaining the structural integrity and biomechanical properties of the disc. Similarly, PDGF promotes cell growth and angiogenesis, supporting the overall regeneration process.
To optimize the delivery and efficacy of these growth factors, researchers are exploring their combination with advanced biomaterials, such as hydrogels. Hydrogels, due to their biocompatibility and ability to mimic the natural extracellular matrix, provide an ideal scaffold for tissue regeneration. These materials not only support the physical structure of the damaged disc but also serve as reservoirs for sustained and localized delivery of therapeutic agents. This controlled release mechanism ensures that growth factors are delivered at optimal concentrations over extended periods, enhancing their therapeutic effects and reducing the need for repeated interventions.
Moreover, hydrogels can be engineered to respond to specific environmental triggers, such as changes in pH or temperature, further refining the precision of drug delivery. By creating a microenvironment conducive to cell adhesion, migration, and proliferation, this approach facilitates the natural healing process of the intervertebral disc while minimizing the risk of adverse effects associated with systemic administration of growth factors.
In addition to their direct regenerative benefits, growth factor-based therapies hold promise for mitigating inflammation and reducing pain associated with disc degeneration. By modulating inflammatory pathways, these treatments can protect the disc from further damage and improve the overall health of surrounding tissues. Research in this area is ongoing, with preclinical studies and early-phase clinical trials demonstrating encouraging results in terms of safety and efficacy.
While this approach offers significant potential, challenges remain. These include the cost and complexity of manufacturing growth factors and biomaterials at a scale suitable for widespread clinical use, as well as the need to ensure their long-term stability and functionality. Additionally, individual variations in patient responses and the underlying causes of disc degeneration necessitate the development of personalized treatment strategies to maximize outcomes.
In conclusion, the integration of growth factors like TGF-β and PDGF with biomaterials such as hydrogels represents a promising frontier in regenerative medicine for intervertebral disc repair. This multifaceted approach not only aims to restore the structure and function of damaged discs but also seeks to address the root causes of degeneration, offering hope for improved quality of life for patients suffering from chronic spinal conditions. As research progresses, these therapies have the potential to transform the field of spinal care, shifting the focus from symptom management to true tissue regeneration and repair.
Integrative Role of Osteopathy in Modern Treatment
As these advanced therapies develop, osteopathy remains a cornerstone of holistic care, complementing these innovations with manual techniques and personalized approaches that optimize the body’s healing capacity.
1. Enhancing Structural Alignment
Osteopaths focus on restoring proper alignment of the spine to reduce stress on affected discs. Techniques such as spinal mobilization and soft tissue manipulation:
- Relieve nerve compression.
- Improve spinal mobility and posture.
- Prevent compensatory strain on surrounding areas.
2. Supporting Circulation and Tissue Repair
By enhancing blood flow and lymphatic drainage, osteopathy facilitates the delivery of nutrients and oxygen to damaged tissues. Techniques like myofascial release and craniosacral therapy reduce inflammation, promoting an optimal environment for healing.
3. Managing Pain and Restoring Function
Osteopathic manipulative treatment (OMT) alleviates muscle tension and addresses compensatory patterns caused by disc herniation. This non-invasive approach reduces pain, improves range of motion, and enhances overall quality of life.
4. Complementing Regenerative Therapies
Osteopathy works synergistically with regenerative treatments. By addressing structural imbalances and promoting a healthy musculoskeletal system, osteopathic care enhances the effectiveness of cell-based and genetic therapies, ensuring a comprehensive recovery process.
5. Providing Holistic Guidance
Beyond manual techniques, osteopaths educate patients on lifestyle modifications, including ergonomic practices, exercise regimens, and stress management strategies. This guidance empowers patients to actively participate in their recovery and reduces the risk of recurrence.
Future Directions in Treatment
The combination of regenerative medicine and osteopathy represents a promising future for lumbar disc herniation management. While stem cell and gene therapies address the underlying causes at a molecular level, osteopathy supports the structural and functional aspects of recovery. Together, they provide a multifaceted approach that enhances healing, reduces pain, and prevents recurrence.
References
- Pettine, K., et al. (2015). « Regenerative potential of mesenchymal stem cells for intervertebral disc degeneration. » Spine Journal.
This study highlights the efficacy of mesenchymal stem cells in regenerating intervertebral disc tissue and reducing inflammation.
Link - Liu, G., et al. (2020). « Gene therapy approaches for intervertebral disc degeneration. » Journal of Orthopedic Research.
A comprehensive review of gene therapy techniques targeting molecular pathways involved in disc degeneration.
Link - Mwale, F., et al. (2014). « The role of growth factors and biomaterials in intervertebral disc regeneration. » European Spine Journal.
This paper explores the use of biomaterials and growth factors in promoting disc repair and improving outcomes in degenerative disc disease.
Link - Chaitow, L. (2018). « Osteopathic techniques for managing lumbar disc herniation. » Journal of Manual & Manipulative Therapy.
Discusses osteopathic manipulative techniques that alleviate pain and restore spinal function.
Link - Kumar, V., et al. (2021). « Integrative approaches in regenerative therapies and osteopathic care. » Clinical Rehabilitation Journal.
Examines the synergy between regenerative treatments and osteopathy in improving patient outcomes.
Link
Osteopathic Care for Lumbar Herniation: Evidence-Based Benefits and Therapeutic Insights
- Efficiency of Physical Therapy and Osteopathic Techniques in the Treatment of Operated and Recurrent Lumbar Disc Herniation: A Case Report
- Summary: This study explores the role of osteopathic techniques combined with physical therapy in patients with recurrent lumbar disc herniation. Results indicate reduced symptoms and improved functionality.
- Year: 2025
- Link to Article
- The Passive Straight Leg Raising Test in the Diagnosis and Treatment of Lumbar Disc Herniation: A Survey of UK Osteopathic Opinion and Clinical Practice
- Summary: A survey assessing how UK osteopaths use diagnostic tests like the Straight Leg Raise in treating lumbar disc herniation. It highlights the effectiveness of manipulative approaches.
- Year: 2003
- Link to Article
- Therapeutic Effects of Chinese Osteopathy in Patients with Lumbar Disc Herniation
- Summary: A comparative clinical study demonstrating how Chinese osteopathic manipulation can significantly alleviate symptoms of lumbar disc herniation.
- Year: 2013
- Link to Article
- Rehabilitation with Osteopathic Manipulative Treatment After Lumbar Disc Surgery: A Randomized Controlled Pilot Study
- Summary: The study evaluates osteopathic rehabilitation techniques post-lumbar surgery, showing enhanced recovery, reduced pain, and better mobility.
- Year: 2015
- Link to Article
- An Osteopathic Approach to Patients with Degenerative and Herniated Discs
- Summary: A detailed review of osteopathic interventions for herniated discs, emphasizing spinal mechanics and patient education in daily living strategies.
- Year: 2021
- Link to Article
- An Unexpectedly Progressed Lumbar Herniated Disk
- Summary: Case studies highlighting the role of osteopathic diagnostics in detecting advanced herniated discs and guiding surgical or non-surgical treatments.
- Year: 2013
- Link to Article
- The Change in the Clinic in Lumbar Disc Herniation After Osteopathic Treatment
- Summary: The paper discusses the embryological and anatomical connections in the lumbar spine and their significance in osteopathic care for disc herniation.
- Year: 2006
- PDF Link
- Spinal Manipulation in Patients with Disc Herniation: A Critical Review of Risk and Benefit
- Summary: Reviews the efficacy and risks of spinal manipulation in disc herniation treatment, highlighting its integration with other therapies like exercise and heat therapy.
- Year: 2006
- Link to Article
- Work Recovery in Response to Osteopathic Treatment After Hemilaminectomy for Lumbar Disc Herniation
- Summary: A study evaluating the long-term benefits of osteopathy in post-operative rehabilitation, showcasing improved work recovery and reduced pain.
- Year: 1995
- PDF Link
- Osteopathic Manipulative Treatment for the Management of Adjacent Segment Pathology
- Summary: Discusses the conservative management of lumbar disc pathology using osteopathic techniques, focusing on maintaining spinal integrity.
- Year: 2017
- PDF Link
Living with Lumbar Disc Herniation: A Day in my Life
Living with lumbar disc herniation presents a daily challenge that requires both physical and mental resilience. Lumbar disc herniation occurs when the intervertebral discs, which act as cushions between the vertebrae, become damaged and protrude, pressing on the spinal nerves. This condition can cause significant pain and discomfort, affecting a person’s ability to perform everyday tasks. Here’s a glimpse into a typical day for someone living with this condition.
Morning Routine
The day begins with the challenge of getting out of bed. Mornings can be particularly tough due to stiffness and pain that often peak after a night of inactivity. A gentle stretching routine is crucial to loosen up the muscles and reduce stiffness. Exercises like pelvic tilts, knee-to-chest stretches, and gentle yoga poses can help. Taking a warm shower also aids in relieving some of the morning discomfort by increasing blood flow and relaxing the muscles.
Preparing for the Day
After managing to get out of bed, dressing up can be another difficult task. Simple activities like bending down to put on socks or shoes can trigger intense pain. Using aids like a long-handled shoehorn or a sock aid can make this process easier. Choosing clothes that are easy to put on and take off can also reduce strain on the back.
Working with Lumbar Disc Herniation
For those who work, the type of job they have significantly affects their day. Office workers need to ensure their workspace is ergonomically friendly. Using an adjustable chair with proper lumbar support, positioning the computer screen at eye level, and taking regular breaks to stand up and stretch can help manage the pain. For those with physically demanding jobs, modifications might be necessary. This could include avoiding heavy lifting, using support belts, or seeking alternative tasks that are less strenuous on the back.
Daily Activities
Throughout the day, maintaining good posture is critical. Whether sitting, standing, or walking, keeping the spine in a neutral position helps reduce the strain on the herniated disc. Activities like cooking, cleaning, or even simple tasks like reaching for items on a shelf need to be done with caution. Bending at the knees rather than the waist, avoiding twisting motions, and using tools designed to reduce the need for bending can be beneficial.
Pain Management
Pain management is an ongoing task. Over-the-counter pain relievers like ibuprofen or acetaminophen can provide temporary relief. For more severe pain, prescription medications or corticosteroid injections might be necessary. Non-pharmacological approaches like heat or ice therapy, physical therapy, and alternative treatments such as acupuncture or chiropractic care can also play a significant role in managing pain and improving mobility.
Exercise and Physical Therapy
Regular exercise tailored to their condition is vital for those with lumbar disc herniation. Engaging in low-impact activities like walking, swimming, or using a stationary bike helps maintain overall fitness without placing undue stress on the back. Physical therapy sessions are essential as they provide specific exercises aimed at strengthening the core muscles, improving flexibility, and promoting proper posture.
Evening and Nighttime Routine
As the day winds down, unwinding with gentle stretches or relaxation techniques can help reduce the day’s accumulated tension. Using a lumbar support pillow while sitting and a proper mattress while sleeping ensures that the spine remains aligned. Finding a comfortable sleeping position, often on the back with a pillow under the knees or on the side with a pillow between the knees, is crucial for a good night’s rest.
Mental Health and Support
Living with chronic pain can take a toll on mental health. It’s important to address the emotional aspect of dealing with lumbar disc herniation. Joining support groups, talking to a therapist, or practicing mindfulness and relaxation techniques can help manage stress and anxiety. Staying connected with friends and family and communicating openly about the challenges can also provide emotional support and understanding.
Radiographic Signs of Lumbar Disc Herniation
Radiographic signs of a lumbar disc herniation can be seen on imaging tests such as x-rays, CT scans (computed tomography scans), or MRI scans (magnetic resonance imaging). However, it is important to note that radiographic signs do not always perfectly match clinical symptoms, and some people may experience herniated discs without experiencing significant symptoms. Here are some radiographic signs healthcare professionals can look for:
- Loss of Disc Height: A herniated disc can cause a decrease in the height of the affected intervertebral disc.
- Osteophytes (Bone Spurs): Osteophytes, or bone spurs, can form around the intervertebral discs in response to a herniated disc.
- Displacement of Surrounding Structures: A herniated disc can cause displacement of surrounding structures, including compression of nerve roots or spinal cord.
- Foramen Enlargement: The intervertebral foramen is the opening through which nerve roots exit the spine. A herniated disc can cause this opening to widen.
- Widening of the Spinal Canal: In some cases, a herniated disc can contribute to the widening of the spinal canal, leaving less space for the spinal cord.
- Joint Effusion: The presence of fluid around the joints may be an x-ray sign.
- MRI to Visualize Soft Tissues: MRI is particularly useful for visualizing soft tissues, including intervertebral discs, spinal cord, and nerve roots. It can show the precise location of the herniated disc and the impact on surrounding structures.
It is important to emphasize that the diagnosis of herniated disc is often based on a combination of clinical information, imaging studies, and neurological assessments.

Straightening of the lumbar spine with preserved alignment. Irregular margins of end plate L5. Decreased hydration of the L4-5 disc represented by reduced T2 hyperintensity of the disc.
L4-5 disc posterior bulge with central annular tear and protrusion indenting the ventral thecal sac, both obliterating the lateral recess and compressing the two exiting nerve roots.
Posterior L5-S1 disc bulging with left postlateral annular tear and protrusion indenting the ventral thecal sac, obliterating both the lateral cavity and compressing the two exiting nerve roots.
The nerve roots of Conus medullaris and cauda equina are normal. The pre- and paravertebral soft tissues are normal.
Living with Lumbar Disc Herniation
Living with a lumbar disc herniation presents daily challenges that require physical adjustments, mental resilience, and an integrated approach to manage pain and maintain quality of life. This condition, often associated with lower back pain, reduced mobility, and occasional neurological issues, necessitates a multidimensional strategy. Here, we explore strategies for managing daily pain, the importance of emotional and mental support, and testimonials from patients sharing their journeys.
Strategies for Managing Daily Pain
Managing pain from a lumbar disc herniation involves combining physical, medical, and behavioral approaches.
- Adapted Physical Activity
Incorporating specific exercises like back stretches, core strengthening, and gentle activities such as yoga or swimming can reduce spinal pressure and enhance mobility. Regular walking, even in short intervals, promotes circulation and reduces stiffness. - Ergonomic Postures
Adopting correct posture is essential to minimize spinal strain. Using chairs with proper lumbar support, setting up an ergonomic workspace, and avoiding prolonged sitting or standing can prevent additional discomfort. - Pain Management Techniques
Heat or cold therapy, lumbar cushions, and tools like foam rollers can provide localized relief. Medications such as anti-inflammatories or muscle relaxants, coupled with complementary therapies like osteopathy or acupuncture, are integral to managing pain. - Relaxation Practices
Techniques like meditation, deep breathing, or mindfulness can help calm the nervous system, reducing the intensity of pain perception.
Importance of Emotional and Mental Support
Chronic pain profoundly impacts mental health. Feelings of frustration, anxiety, and depression can exacerbate physical symptoms, making emotional balance crucial.
- Psychological Support
Working with a therapist or joining support groups can equip individuals with tools to better manage emotions related to chronic pain. Sharing experiences with others in similar situations helps reduce feelings of isolation. - Cognitive Strategies
Cognitive-behavioral therapy (CBT) helps reframe mental responses to pain and fosters resilience against physical limitations. - Positive Daily Practices
Incorporating gratitude rituals, engaging in enjoyable activities, and maintaining strong social connections improve mood and emotional endurance.
Testimonials and Patient Journeys
Patient testimonials provide valuable insights into the diverse paths toward adapting and finding resilience:
- Marie, 42 years old: “After months of intense pain, osteopathy restored my confidence in my body. Combined with daily exercises, I feel more independent and in control.”
- Paul, 57 years old: “Accepting that my pain wouldn’t fully disappear was life-changing. Meditation and my family’s support have helped me integrate it into my daily life.”
- Sophie, 35 years old: “Joining a support group was a revelation. Realizing I wasn’t alone motivated me to follow a rehabilitation program and take steps toward recovery.”
Conclusion
By diving into the complex anatomy of the lumbar spine and exploring the underlying mechanisms of herniated disc, we have unraveled the mysteries surrounding this dreaded spinal condition. The causes, symptoms and radiographic signs associated with lumbar disc herniation have been demystified, providing an in-depth understanding of this pathology.
The different phases of pathophysiology, from initial trauma to nerve root compression, have been described clearly and precisely. It is essential to note that lumbar disc herniation can be the result of various factors such as aging, wear and tear, repetitive movements, and even genetic predispositions.
The crucial role of the posterior longitudinal ligament in worsening symptoms was also explored, highlighting the importance of considering all of the anatomical structures involved in disc herniation.
In this quest for lasting relief, osteopathy emerges as a natural ally. Soft tissue techniques, cranial manipulations, visceral manipulations, and a holistic approach are all tools that osteopaths use to improve mobility, relieve pain, and restore balance.
Specific exercises and stretches, combined with lifestyle advice, complete the arsenal of osteopathy to help treat and prevent recurrence of lumbar disc herniation. Specific recommendations, such as posterior chain stretching and core strengthening exercises, add to the patient’s toolbox for proactive management of their spinal health.
Finally, radiographic signs were highlighted, emphasizing the importance of imaging examinations such as MRIs to precisely visualize the location of the herniated disc and its impact on surrounding structures.
In summary, this in-depth exploration of lumbar disc herniation offers valuable keys to understanding, managing and treating this complex condition. Through osteopathy and a holistic approach, lasting relief becomes a reality, paving the way to a better quality of life for those facing this spinal health challenge.
Quizz
Questionnaire (1)
1. What is the main cause of lumbar disc herniation according to the text?
a. Poor body mechanics
b. Aging
c. Genetics
d. Obesity
2. What are the common symptoms of lumbar disc herniation?
a. Lower back pain
b. Numbness and tingling
c. Muscle weakness
d. All previous choices
3. What is the main function of the intervertebral discs in the spine?
a. Support body weight
b. Produce stem cells
c. Control digestion
d. Regulate body temperature
4. How can lumbar disc herniation be diagnosed?
has. Radiography
b. MRI
v. Computed tomography (CT)
d. All previous choices
5. What is the gold standard examination method for diagnosing a herniated disc?
a. Radiography
b. MRI
c. Clinical assessment
d. CT
6. What are the possible radiographic signs of a lumbar disc herniation?
a. Loss of disc height
b. Osteophytes (bone spurs)
c. Displacement of surrounding structures
d. All previous choices
7. What is the inflammatory response associated with nerve root compression?
a. Improvement of symptoms
b. Intensification of symptoms
c. No impact
d. Temporary improvement
8. What are the potential benefits of osteopathy in the treatment of lumbar disc herniation?
a. Improved mobility
b. Pain relief
c. Muscle strengthening
d. All previous choices
9. What can make lumbar disc herniation symptoms worse?
a. Complete rest
b. Moderate physical activities
c. Prolonged sitting positions
d. No impact
10. What is the conclusion of the text on lumbar disc herniation?
a. Herniated disc has no effective treatment.
b. Osteopathy is a useless approach.
c. A multidisciplinary approach is necessary for effective management.
d. Traditional treatments are always the best.
Answers:
- b
- d
- a
- d
- b
- d
- b
- d
- c
- c
References
- Sharma SB, Kim JS. A Review of Minimally Invasive Surgical Techniques for the Management of Thoracic Disc Herniations. Neurospin. 2019 Mar;16(1):24-33. [ PMC free article ] [ PubMed ]2.
- Huang R, Meng Z, Cao Y, Yu J, Wang S, Luo C, Yu L, Xu Y, Sun Y, Jiang L. Nonsurgical medical treatment in the management of pain due to lumbar disc prolapse: A network meta-analysis. Semin Arthritis Rheum. 2019 Oct;49(2):303-313. [ PubMed ]3.
- Tang C, Moser FG, Reveille J, Bruckel J, Weisman MH. Cauda Equina Syndrome in Ankylosing Spondylitis: Challenges in Diagnosis, Management, and Pathogenesis. J Rheumatol. 2019 Dec;46(12):1582-1588. [ PubMed ]4.
- Park CH, Park ES, Lee SH, Lee KK, Kwon YK, Kang MS, Lee SY, Shin YH. Risk Factors for Early Recurrence After Transforaminal Endoscopic Lumbar Disc Decompression. Pain Physician. 2019 Mar;22(2):E133-E138. [ PubMed ]5.
- Huang JS, Fan BK, Liu JM. [Overview of risk factors for failed percutaneous transforaminal endoscopic discectomy in lumbar disc herniation]. Zhongguo Gu Shang. 2019 Feb 25;32(2):186-189. [ PubMed ]6.
- Fjeld OR, Grøvle L, Helgeland J, Småstuen MC, Solberg TK, Zwart JA, Grotle M. Complications, reoperations, readmissions, and length of hospital stay in 34,639 surgical cases of lumbar disc herniation. Bone Joint J. 2019 Apr;101-B(4):470-477. [ PubMed ]7.
- Jordan J, Konstantinou K, O’Dowd J. Herniated lumbar disc . BMJ Clin Evid. 2009 Mar 26;2009 [ PMC free article ] [ PubMed ]8.
- Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The prevalence and clinical characteristics of internal disc disruption in patients with chronic low back pain. Spine (Phila Pa 1976). 1995 Sep 01;20(17):1878-83. [ PubMed ]9.
- Dydyk AM, Khan MZ, Singh P. StatPearls [Internet]. Stat Pearls Publishing; Treasure Island (FL): Oct 24, 2022. Radicular Back Pain. [ PubMed ]10.
- M Das J, Nadi M. StatPearls [Internet]. Stat Pearls Publishing; Treasure Island (FL): Mar 27, 2023. Lasegue Sign. [ PubMed ]11.
- Carlson BB, Albert TJ. Lumbar disc herniation: what has the Spine Patient Outcomes Research Trial taught us? Int Orthop. 2019 Apr;43(4):853-859. [ PubMed ]12.
- Hassan KZ, Sherman AL. StatPearls [Internet]. Stat Pearls Publishing; Treasure Island (FL): Jul 17, 2023. Epidural Steroids. [ PubMed ]13.
- Johnson SM, Shah LM. Imaging of Acute Low Back Pain. Radiol Clin North Am. 2019 Mar;57(2):397-413. [ PubMed ]14.
- Brazilian Medical Association. Silvinato A, Simões RS, Buzzini RF, Bernardo WM. Lumbar herniated disc treatment with percutaneous hydrodiscectomy. Rev Assoc Med Bras (1992). 2018 Sep;64(9):778-782. [ PubMed ]15.
- Harper R, Klineberg E. The evidence-based approach for surgical complications in the treatment of lumbar disc herniation. Int Orthop. 2019 Apr;43(4):975-980. [ PubMed ]16.
- Lavi ES, Pal A, Bleicher D, Kang K, Sidani C. Imaging of the Spine: Urgent and Emergent Indications. Semin Ultrasound CT MR. 2018 Dec;39(6):551-569. [ PubMed ]17.
- Alvin MD, Lubelski D, Alam R, Williams SK, Obuchowski NA, Steinmetz MP, Wang JC, Melillo AJ, Pahwa A, Benzel EC, Modic MT, Quencer R, Mroz TE. Spine Surgeon Treatment Variability: The Impact on Costs. Global Spine J. 2018 Aug;8(5):498-506. [ PMC free article ] [ PubMed ]18.
- Qaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of Physicians. Denberg TD, Barry MJ, Boyd C, Chow RD, Fitterman N, Harris RP, Humphrey LL, Vijan S. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017 Apr 04;166(7):514-530. [ PubMed ]19.
- Landau WM, Nelson DA, Armon C, Argoff CE, Samuels J, Backonja MM. Assessment: use of epidural steroid injections to treat radicular lumbosacral pain: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2007 Aug 07;69(6):614; author reply 614-5. [ PubMed ]20.
- Chou R, Hashimoto R, Friedly J, Fu R, Bougatsos C, Dana T, Sullivan SD, Jarvik J. Epidural Corticosteroid Injections for Radiculopathy and Spinal Stenosis: A Systematic Review and Meta-analysis. Ann Intern Med. 2015 Sep 01;163(5):373-81. [ PubMed ]21.
- Chou R, Loeser JD, Owens DK, Rosenquist RW, Atlas SJ, Baisden J, Carragee EJ, Grabois M, Murphy DR, Resnick DK, Stanos SP, Shaffer WO, Wall EM., American Pain Society Low Back Pain Guideline Panel. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: an evidence-based clinical practice guideline from the American Pain Society. Spine (Phila Pa 1976). 2009 May 01;34(10):1066-77. [ PubMed ]22.
- Amlie E, Weber H, Holme I. Treatment of acute low-back pain with piroxicam: results of a double-blind placebo-controlled trial. Spine (Phila Pa 1976). 1987 Jun;12(5):473-6. [ PubMed ]23.
- Schoenfeld AJ, Weiner BK. Treatment of lumbar disc herniation: Evidence-based practice. Int J Gen Med. 2010 Jul 21;3:209-14. [ PMC free article ] [ PubMed ]24.
- Buttermann GR. Treatment of lumbar disc herniation: epidural steroid injection compared with discectomy. A prospective, randomized study. J Bone Joint Surg Am. 2004 Apr;86(4):670-9. [ PubMed ]


















{kind=link}