
Introduction
Calcific tendinitis, although it can affect different parts of the body, most commonly occurs in the rotator cuff of the shoulder. The rotator cuff is a group of muscles and tendons crucial for the strength and stability of the upper arm and shoulder. This condition is especially common among people between the ages of 30 and 50, and women are more likely to suffer from it than men.
The rotator cuff of the shoulder encompasses various disorders, among which calcific tendinopathy (TC) is common. TC is characterized by the presence of calcifications at the insertion of the rotator cuff tendons and in the synovial tissues, including the subacromial bursa. These calcifications form in the crystalline or amorphous form of calcium hydroxyapatite. Common symptoms of TBI include severe pain associated with repetitive activities, increased sensitivity, localized swelling, and varying degrees of functional impairment.
Although in many cases calcific tendinitis may resolve spontaneously, a significant number of patients remain symptomatic despite the passage of time. Persistence of symptoms can lead to worsening quality of life and reduced shoulder functionality, often requiring medical intervention.
The calcification process in TC can lead to local inflammation, thereby causing the pain and swelling associated with this condition. Repetitive activities can make the situation worse, intensifying the patient’s suffering. Increased sensitivity in the shoulder is also a common feature, making movements and daily activities often painful and limited.
Although some people may experience spontaneous resolution of calcific tendinitis, others may require medical interventions to relieve persistent symptoms. Treatment options may include physiotherapy to strengthen the rotator cuff muscles, anti-inflammatories to relieve pain, corticosteroid injections to reduce inflammation, or in some more serious cases, surgery may be considered. to eliminate calcifications.
In summary, calcific tendinitis, particularly common in the rotator cuff of the shoulder, is a painful condition that can affect individuals’ quality of life. Although some cases may resolve naturally, others require medical intervention to relieve persistent symptoms and restore functionality to the shoulder. A personalized treatment approach, tailored to the severity of the condition and the specific needs of the patient, is essential for effective management of calcific tendinitis.
Causes
- Age: Calcific tendinopathy tends to occur more frequently in middle- and older-aged people.
- Gender: Women seem to be affected more often than men.
- Genetic factors: Some individuals may have a genetic predisposition to developing calcium deposits in the tendons.
- Repetitive Strain Injuries: Repetitive movements or microtrauma to a tendon can contribute to irritation and inflammation, eventually leading to the formation of calcium deposits.
- Metabolic disorders: Metabolic conditions, such as disorders of calcium metabolism, can promote the formation of calcium deposits in soft tissues, including tendons.
- Rotator Cuff Dysfunction: Calcific tendinopathy is commonly seen in the rotator cuff tendons of the shoulder. Structural or functional problems of the rotator cuff may contribute to the development of this condition.
- Vascular factors: Some researchers suggest that vascular problems in the tendon area may play a role in the formation of calcium deposits.
Symptoms
- Pain: Pain is the most common symptom. It can be localized to the shoulder, generally on the external side, and worsens with certain movements of the arm or shoulder. The pain may be intermittent or constant.
- Stiffness: People with calcific tendinopathy may experience stiffness in the shoulder, limiting range of motion.
- Tingling or numbness: Some individuals may experience tingling or numbness sensations in the affected area.
- Muscle weakness: The presence of calcium deposits in the tendons can lead to muscle weakness in the affected area.
- Nighttime pain: The pain may be more intense during the night, disrupting the affected person’s sleep.
- Worsening with certain activities: Specific movements, especially those that involve raising the arm, can make the pain worse.
- Tenderness to touch: The affected area may be tender to touch, and direct pressure on the calcified tendon may cause pain.
Pathophysiology
The pathophysiology of calcific tendinopathy is not completely understood, but several mechanisms are generally considered to contribute to the development of this condition. Calcific tendinopathy involves the formation of calcified deposits in the tendons, primarily in the context of the rotator cuff of the shoulder. Here are some key elements of the pathophysiology associated with this condition:
- Tendon Degeneration Process: Calcific tendinopathy often begins with a process of tendon degeneration. Repetitive microtrauma, excessive loading or degenerative factors can lead to changes in the structure of the tendon, making it more susceptible to calcified deposits.
- Calcium crystal formation: Factors such as chronic irritation, inflammation and microtrauma can induce the release of calcium from tendon cells or surrounding synovial fluid. The calcium then precipitates in the form of calcium phosphate crystals inside the tendon.
- Inflammatory reaction: The presence of calcified deposits in the tendon triggers a local inflammatory reaction. This inflammation can contribute to pain and other symptoms associated with calcific tendinopathy.
- Evolutionary phases:
- Formation stage (precrystalline): Molecular and cellular changes occur, but no calcified deposits are yet visible.
- Calcification (crystalline) stage: Calcium crystals begin to form in the tendon, becoming visible on x-ray images.
- Resorption stage (postcrystalline): Calcified deposits can be resorbed by immune cells and macrophages, leading to an increased inflammatory response.
- Repair stage: The tendon begins to repair and regenerate after resorption of calcified deposits.
- Risk factors: Certain risk factors, such as age, gender (more common in women), metabolic abnormalities and genetic factors, may also influence predisposition to calcific tendinopathy.
Importantly, the precise understanding of the pathophysiology of calcific tendinopathy is still evolving, and additional research is needed to clarify the specific mechanisms underlying each phase of the disease. The complexity of calcific tendinopathy suggests a complex interplay between degenerative, metabolic, and inflammatory factors in its development.
Stages of calcific tendinopathy
Calcific tendinopathy typically goes through different stages, each characterized by specific changes in disease progression. These stages are often identified using imaging tests such as x-ray or ultrasound. Here is a general description of the stages of calcific tendinopathy:
- Calcium formation stage (pre-crystalline): In this initial phase, molecular and cellular changes occur in the tendon. However, there are no calcified deposits visible on the x-ray images yet. Symptoms may be absent or minimal at this stage.
- Calcification (crystalline) stage: At this stage, calcium crystals begin to form in the tendon. Calcified deposits become visible on x-rays. Patients may begin to experience symptoms such as pain and stiffness.
- Resorption (post-crystalline) stage: In this phase, calcified deposits can begin to be resorbed or broken down by the body. This process can lead to increased pain and other symptoms. At this point, x-rays may show a clear area instead of calcified deposits.
- Repair stage: Once the resorption of calcified deposits is complete, the tendon begins to repair itself. The pain usually subsides at this point, although repair may take time.
It is important to note that not all patients will necessarily experience all of these stages, and the progression of the disease can vary from person to person. Some patients may remain asymptomatic or only experience mild pain, while others may experience more severe symptoms at each stage.
What are the cuff tissues affected by calcific tendinopathy.
- Supraspinous: 80%
- Infraspinatus: 15%
- Subscapularis: 5
- Periarticular soft tissues in addition to tendons
- Ligaments
- Capsule
- Bursae
Prevention recommendations
- Maintaining Good Posture: Adopting proper posture during daily and work activities can reduce strain on the shoulder tendons. Avoid staying in uncomfortable positions for long periods of time.
- Warm-up before exercise: Before any strenuous physical activity, be sure to do a proper warm-up to prepare the muscles and tendons for the effort. Dynamic warm-up exercises and specific stretches may be beneficial.
- Balanced Muscle Strengthening: A targeted muscle strengthening program, particularly for the rotator cuff muscles, can help maintain shoulder stability. It is essential to maintain muscular balance between antagonistic muscles to avoid imbalances that could increase stress on the tendons.
- Avoid excessive repetitive movements: Avoid activities that involve intense repetitive movements of the shoulder, especially when associated with overload. If your job or activities involve repetitive movements, try to take regular breaks to allow your muscles and tendons to rest.
- Proper Lifting Techniques: When lifting heavy objects, use proper techniques to minimize stress on the shoulders. Lift with your legs rather than your back and avoid lifting excessive loads.
- Moderation in intense physical activities: If you engage in intensive sports or fitness activities, make sure you progress gradually and avoid excessive overloads that could lead to repetitive strain injuries.
- Regular Stretching: Incorporate regular stretching exercises into your routine to maintain flexibility in the shoulder muscles and tendons.
- Stress management: Stress can contribute to muscle tension. Managing stress through techniques such as meditation, yoga or deep breathing can be beneficial.
- Medical consultation: If you experience persistent pain, weakness or stiffness in your shoulder, consult a healthcare professional. Early assessment can help prevent more serious problems from developing.
Treatment for those with calcific tendinopathy
Treatment for calcific tendinopathy depends on the stage of the disease, severity of symptoms, and patient preference. Here are some treatment approaches that may be considered:
- Conservative treatment:
- Rest: Avoid activities that exacerbate pain.
- Ice: Applying ice to the painful area can help reduce inflammation.
- Nonsteroidal anti-inflammatory drugs (NSAIDs): Medications such as ibuprofen can relieve pain and reduce inflammation.
- Physical Therapy: Specific exercises and physical therapy modalities can help improve mobility and strength while reducing pain.
- Suction of calcified deposits (washing):
- A procedure called washing may be performed to vacuum out calcified deposits in the tendon. This can relieve pain and improve function.
- Corticosteroid infiltrations:
- Corticosteroid injections into the affected area can reduce inflammation and relieve pain. However, their long-term use may have side effects, and they are generally not recommended frequently.
- Extracorporeal shock waves (ESWT):
- ESWT is a procedure in which shock waves are applied to the affected area to stimulate healing. This may be considered in certain cases of calcific tendinopathy.
- Ultrasound therapy:
- The use of ultrasound may be considered to help break down calcified deposits.
- Surgery :
- If conservative treatments fail, surgery may be considered to remove calcified deposits or repair damaged tendons.
Radiographic signs
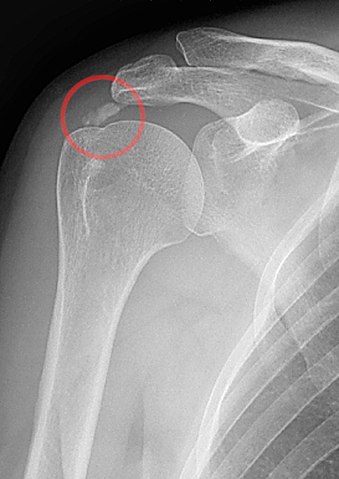
Radiographic signs of calcific tendinopathy may vary depending on the stage of the disease. Calcified deposits in tendons can be visualized on plain x-rays, but certain features can help identify calcific tendinopathy. Here are some common radiographic signs associated with calcific tendinopathy:
- Radiopaque opacities: X- rays may reveal opacities or areas of opacity in the rotator cuff tendon region, indicating the presence of calcified deposits.
- Shape and size of deposits: Calcified deposits can have different shapes and sizes. They may appear as plaques, clumps or more diffuse calcifications.
- Location: Calcific tendinopathy, particularly in the context of the rotator cuff, can often be localized to the supraspinatus muscle tendon. However, it can also affect other rotator cuff tendons.
- Phases of the disease:
- Formation stage (precrystalline): No visible calcification.
- Calcification stage (crystalline): Presence of calcified deposits visible on x-rays.
- Resorption stage (postcrystalline): A clear area may appear in place of calcified deposits, indicating resorption in progress.
- Time course: Successive radiographs can show the progression of calcific tendinopathy, including formation, calcification, resorption and repair.

Conclusion
In conclusion, calcific tendinitis, a condition often localized to the rotator cuff of the shoulder, represents a significant clinical challenge. Although some individuals may experience spontaneous resolution of their symptoms, a substantial number of patients remain symptomatic, requiring appropriate medical management.
Calcium hydroxyapatite calcifications, characteristic of calcific tendinopathy, can lead to local inflammation, thereby causing severe pain, increased sensitivity, swelling and impaired function of the shoulder. Daily activities can become difficult, affecting the quality of life of affected individuals.
Treatment approaches vary depending on the severity of symptoms and patient preferences. Physiotherapy, aimed at strengthening the rotator cuff muscles, is often used to improve functionality. Anti-inflammatories may be prescribed to relieve pain, while corticosteroid injections may be considered to reduce inflammation. In more severe or persistent cases, surgery may be recommended to remove the calcifications.
Successful management of calcific tendinitis requires a personalized approach, taking into account the severity of symptoms, the patient’s tolerance to various interventions, and the individual response to treatment. It is essential that patients consult qualified healthcare professionals to assess their specific situation and determine an appropriate treatment plan.
In short, calcific tendinitis is a condition that can have a significant impact on an individual’s quality of life. Understanding the complexity of this condition and adopting a multidisciplinary approach, involving health specialists such as physiotherapists and doctors, is essential for effective and personalized management of calcific tendinitis.
References
- Depalma AF, Kruper JS. Long-term study of shoulder joints afflicted with and treated for calcific tendinitis. Clin Orthop. 1961;20:61–72. [PubMed] [Google Scholar]
- Loew M, Jurgowski W, Mau HC, Thomsen M. Treatment of calcifying tendinitis of rotator cuff by extracorporeal shock waves: a preliminary report. J Shoulder Elbow Surg. 1995;4:101–6. [PubMed] [Google Scholar]
- Jim YF, Hsu HC, Chang CY, Wu JJ, Chang T. Coexistence of calcific tendinitis and rotator cuff tear: an arthrographic study. Skeletal Radiol. 1993;22:183–5. [PubMed] [Google Scholar]
- Codman EA, Akerson IB. The pathology associated with rupture of the supraspinatus tendon. Ann Surg. 1931;93:348–59. [PMC free article] [PubMed] [Google Scholar]
- Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997;5:183–91. [PubMed] [Google Scholar]
- Bosworth DM. Diagnosis and treatment of lesions of the shoulder. R I Med J. 1953;36:512–5. [PubMed] [Google Scholar]
- Neer CS II. Less frequent procedures. In: Neer CS II, editor. Shoulder reconstruction. Philadelphia, PA: WB Saunders; 1990. pp. 421–85. [Google Scholar]
- Molé D, Kempf JF, Gleyze P, Rio B, Bonnomet F, Walch G. Results of endoscopic treatment of non-broken tendinopathies of the rotator cuff. 2. Calcifications of the rotator cuff. Rev Chir Orthop Reparatrice Appar Mot. 1993;79:532–41. [PubMed] [Google Scholar]
- Loew M, Sabo D, Wehrle M, Mau H. Relationship between calcifying tendinitis and subacromial impingement: a prospective radiography and magnetic resonance imaging study. J Shoulder Elbow Surg. 1996;5:314–9. [PubMed] [Google Scholar]
- Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med. 1999;340:1582–4. [PubMed] [Google Scholar]
- Rompe JD, Zoellner J, Nafe B. Shock wave therapy versus conventional surgery in the treatment of calcifying tendinitis of the shoulder. Clin Orthop Relat Res. 2001;(387):72–82. [PubMed] [Google Scholar]
- Cho NS, Lee BG, Rhee YG. Radiologic course of the calcific deposits in calcific tendinitis of the shoulder: does the initial radiologic aspect affect the final results. J Shoulder Elbow Surg. 2010;19:267–72. [PubMed] [Google Scholar]
- Farin PU, Räsänen H, Jaroma H, Harju A. Rotator cuff calcifications: treatment with ultrasound-guided percutaneous needle aspiration and lavage. Skeletal Radiol. 1996;25:551–4. [PubMed] [Google Scholar]
- Ebenbichler GR, Erdogmus CB, Resch KL, et al. Ultrasound therapy for calcific tendinitis of the shoulder. N Engl J Med. 1999;340:1533–8. [PubMed] [Google Scholar]
- Daecke W, Kusnierczak D, Loew M. Long-term effects of extracorporeal shockwave therapy in chronic calcific tendinitis of the shoulder. J Shoulder Elbow Surg. 2002;11:476–80. [PubMed] [Google Scholar]
- Ioppolo F, Tattoli M, Di Sante L, et al. Clinical improvement and resorption of calcifications in calcific tendinitis of the shoulder after shock wave therapy at 6 months’ follow-up: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2013;94:1699–706. [PubMed] [Google Scholar]
- Bannuru RR, Flavin NE, Vaysbrot E, Harvey W, McAlindon T. High-energy extracorporeal shock-wave therapy for treating chronic calcific tendinitis of the shoulder: a systematic review. Ann Intern Med. 2014;160:542–9. [PubMed] [Google Scholar]
- Rochwerger A, Franceschi JP, Viton JM, Roux H, Mattei JP. Surgical management of calcific tendinitis of the shoulder: an analysis of 26 cases. Clin Rheumatol. 1999;18:313–6. [PubMed] [Google Scholar]
- Ark JW, Flock TJ, Flatow EL, Bigliani LU. Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy. 1992;8:183–8. [PubMed] [Google Scholar]
- Jerosch J, Strauss JM, Schmiel S. Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg. 1998;7:30–7. [PubMed] [Google Scholar]

















